
Abstract
The cognitive skills critical for success have largely been studied in Western populations, despite the fact that children in low- and middle-income countries are at risk to not reach their full developmental potential. Moreover, scientists should leverage recent discovery to explore means of boosting cognition in at-risk populations. This semi-randomized controlled trial examined normative cognitive development and whether it could be enhanced by consumption of a probiotic food in a sample of 251 4- to 7-year-old children in urban schools in Côte d’Ivoire. Participants completed executive functioning measures at baseline (T1) and 5 months later (T2). After T1, children in one school received a probiotic (N = 74) or placebo (N = 79) fermented dairy food every day they were in school for one semester; children in the other school (N = 98) continued their diet as usual. Children improved on all tests across time (Cohen’s d = 0.08–0.30). The effects of probiotic ingestion were inconclusive and are interpreted with caution due to socio-political factors affecting daily administration. Given the general feasibility of the study, we hope that it will serve as an inspiration for future research into child development and sustainable (health-promoting) interventions for school children in developing nations.
Similar content being viewed by others
Introduction
Executive functioning (EF) is an umbrella term for a set of skills including working memory and response inhibition1. EF and numeracy skills at school entry are critical components of academic success and contribute to other beneficial life outcomes. For example, deficits in EF in first graders (4–6 years old) are linked with later writing and mental health difficulties, whereas EF competence is linked with school achievement and social competence2,3,4. Numerical skills at the same age contribute to functional numeracy, or mathematical competence, 6 years later5. In turn, numeracy at later ages is negatively associated with self-reports of poor health and positively associated with higher personal wealth5,6,7. Despite recognition of the importance of these skills, their development is largely studied in white, educated, industrialized, rich, and democratic (WEIRD8) populations, limiting the generalizability of findings to a small subset of the world’s population. The current study examined normative cognitive development, and whether it is enhanced through probiotic supplementation in the form of a locally produced probiotic fermented milk product, in an urban sample of first grade children in Côte d’Ivoire.
Cognition in the developing world
To date, studies examining the development of EF and other cognitive skills in low- and middle-income or LMIC (i.e., non-WEIRD) populations have been limited in both number and scope. Extant studies have tended to focus on very young children prior to school entry, specific populations (e.g., HIV-infected or malnourished children), parenting or academic interventions, and test development (e.g., Refs.9,10,11). Studies that do examine normative school-age cognition in LMICs find it linked with important life outcomes, underscoring the need to study cognition in diverse populations. For example, one study found positive associations between early executive functioning and academic achievement in 1480 4- to 7-year-old Kenyan children; another with 150 South African primary school children showed a correlation between early academic achievement and cognitive test scores and later school retention and survival in a longitudinal investigation12,13.
Despite the paucity of literature, there is growing interest in examining cognitive development in diverse populations, as it is widely recognized that children in LMICs, and particularly those in sub-Saharan Africa, are at risk to not reach their full development potential14. Children in LIMCs often face combined risk factors for suboptimal development, including parasitic infections, malnutrition, exposure to toxins, and food insecurity—all of which are linked with cognitive deficits (e.g., Refs.10,15,16,17,18). Understanding normative cognitive development in LMICs will help identify requirements to counter inequality in underserved communities and provide critical data for governments aiming to intervene when children are failing to reach their potential.
In addition to studying normative cognitive development, scientists should look to recent research and scientific discoveries to develop sustainable, low-cost, and accessible means to improve cognitive outcomes for at-risk populations. The literature points to at least two promising avenues to achieve this aim in developing contexts—nutrition supplementation and the use of probiotics.
Nutrition supplementation
A recent systematic review examining school-based nutrition programs in sub-Saharan Africa found that affordable and practical programs demonstrate positive effects on cognitive performance in a number of domains19. Milk products in particular hold promise: a randomized controlled trial with first grade Kenyan children showed that children who received milk powder-supplemented stew each school day over two years had better end-term test scores than children who received oil-supplemented stew or no stew20. Additionally, a study in Ghana showed that adding milk powder to a school meal for nine months increased children’s executive functioning scores compared to a control group whose school meal was not supplemented21.
Probiotics
Probiotics, defined as “live microorganisms that, when administered in adequate amounts, confer a health benefit on the host”22, may be another promising route to boost cognitive outcomes. Although no research has yet examined probiotic effects on cognition in LMICS, studies have shown health benefits such as reduced absorption of environmental toxins, reduced respiratory infections, and shortened duration of acute diarrhea, a common ailment in the developing world16,23,24,25. The latter two studies utilized Lacticaseibacillus rhamnosus GG, the strain from which a generic variant, Lacticaseibacillus rhamnosus yoba 2012, was developed by Yoba for Life Foundation26, which was used in the present study. It is possible that such documented health benefits would be indirectly linked with cognitive improvements in children by, for example, decreasing school absence.
Another route through which probiotics may induce cognitive improvements is through modulation of the microbiota-gut-brain axis. A recent review indicated that probiotic ingestion was associated with positive gut microbiota changes (e.g., more healthy and fewer unhealthy bacteria) in healthy older adults27, although this has not been replicated in children. However, in very young children, gut microbiota composition is associated with both cognition28 and brain functional connectivity29, indicating that positive alterations to the gut microbiota (i.e., through probiotic supplementation) may also influence cognitive function.
Empirically, the evidence for probiotic effects on cognition is small and somewhat inconsistent. While the animal literature points to positive probiotic effects on learning and memory (e.g., Ref.30), human studies, which generally involve probiotic supplementation for between 3 and 12 weeks, are more equivocal: one recent meta-analysis found evidence suggesting positive probiotic effects on cognition in humans31, whereas another did not32. A recent review reported that 21 out of the 25 studies in adult humans examined found a positive effect of probiotic consumption on cognition. In the same review, however, studies examining very young children tended to find no effects. Importantly, all occurred in children under 2 years of age, a time in which the brain is undergoing rapid development and potentially susceptible to a wide range of external influences33. Similarly, probiotic strains such as Lacticaseibacillus rhamnosus HN001 and Bifidobacterium animalis subsp. lactis HN019 were unassociated with cognitive improvements in infants34. However, a randomized placebo-controlled study of infants showed that L. rhamnosus GG (a strain similar to the one used in the current investigation) could have a benefit against attention deficit hyperactivity disorder and Asperger syndrome35. No studies have yet examined the effects of probiotic ingestion on cognition in school-aged children, which is surprising given that the safety record of this class of products is excellent for children of all ages (e.g., Ref.36). Based on the evidence presented above on outcomes and potential mechanisms, we hypothesize that L. rhamnosus yoba 2012, administered with a nutrient-rich food, may improve cognitive functioning in children from an economically stressed setting.
The current study
This manuscript describes the results of a semi-randomized controlled trial with first grade children in Côte d’Ivoire. The first aim was to examine children’s normative cognitive gains, using free and widely available age-appropriate tests, over one semester at urban, economically-disadvantaged schools. We hypothesized that children would improve on all tests over one semester. The second aim was to determine whether regular intake of a traditional fermented milk-based probiotic product with millet, locally known as dêguê, that was enriched with the probiotic L. rhamnosus yoba 2012 could enhance cognitive scores compared to a non-enriched variant (placebo). We hypothesized that children who consumed the fermented probiotic product for one semester (approximately 16 weeks) would have higher scores at the end of the semester than children who consumed a placebo and children who followed their diet as usual, taking into account baseline scores. Finally, we exploratorily examined whether probiotic dose or regularity of consumption were related to test scores, but advanced no hypotheses about these.
Methods
Study design and participants
This semi-randomized controlled trial had three arms: probiotic, placebo, and diet as usual (DAU). We employed a semi-randomized design due to the ethical concern of giving some children but not others a food supplement in a single school. Accordingly, children in one school (the experimental school) comprised the probiotic and placebo arms randomized within classes, whereas children in the other school (the control school) comprised the DAU arm. A power analysis conducted with G*Power37 determined that 3 groups with at least 89 participants per group would give us 90% power to detect small to medium group mean differences. To plan for participant attrition and to increase power, we aimed to include at least 100 children in each group.
Children were recruited (via flyers sent home in backpacks, word of mouth, and two social events held at the schools) from first grade classes (level CP1 in the French/Ivorian education systems) in two closely-situated public primary schools in a low-income district of Abidjan, Côte d’Ivoire. All first-grade children were West-African and eligible for inclusion. In the experimental school, all available (i.e., currently enrolled in first grade) children were recruited (Nprobiotic = 87, Nplacebo = 82, NDAU = 1). Given that schools were assigned by the government, we were unable to recruit additional children from nearby schools or switch to a school with more available children. In the control school, the first 100 children whose caregivers consented were recruited (NDAU = 100), resulting in a total sample of 270 children.
Caregivers provided written informed consent for themselves and their children to take part in the study; children provided verbal assent prior to each round of testing. Caregivers who were able to read could take the consent form to read at their leisure and return at any time to sign up. Caregivers who were illiterate (the majority) had the consent form verbally explained page-by-page by a member of the research team. All caregivers were given the opportunity to pose questions before signing (or providing a thumbprint if unable to sign).
The study was approved by the “Comité National d'Ethique des Sciences de la Vie et de la Santé” (National Committee of Ethics of Life Sciences and Health) in Côte d’Ivoire and the ethics committee of the Social Science faculty of Radboud University in The Netherlands (project number: ECSW-2018-085R1). All methods were performed in accordance with the guidelines and regulations set forth by both committees, and approved procedures were not deviated from. The study was registered: AsPredicted #32143 (10/15/2019). To this registration we added a general question about changes in cognition over time. Additionally, not all variables mentioned in the registration were able to be used and analytic techniques were adapted due to missing data. In addition, we registered the trial with the Pan African Clinical Trials Registry: PACTR202207495830367. This registration was completed on June 18, 2022 and accurately reflects our work.
Procedure
Caregivers (N = 231) completed a 20 to 30-min interview on family demographics and child characteristics either immediately after consenting or 1–4 months later via telephone. All efforts were made to ensure that the respondent was the primary caregiver of the child, but in some instances, this was not possible, and it was completed by someone else close to the child.
At baseline (T1) prior to randomization and at outcome (T2; 3–5 months later; mean = 4.89 months; standard deviation = 19.39 days), children completed cognitive measures and provided biological measures (height and weight, saliva and fecal samples) that are not part of the current study.
After most T1 testing was complete, experimental school children were randomized into probiotic and placebo groups stratified by class. Children were assigned numbers; a random number generator determined groups. Children enrolled after randomization (N = 11) were assigned on an alternating basis. For one semester, randomized children were given a probiotic or a placebo product each day they were in class. No child consumed the product prior to completing T1 testing. Children in the control school received no dietary intervention. Medical care was available at no cost to all participants during the study period.
Dietary intervention
Probiotic and placebo dêguê (a well-known West African fermented milk product containing sugar and millet) were produced for this study by a local dêguê-producing company using standard hygiene practices including gloves and hair and shoe coverings. The company adapted their recipe to create a healthier product with 40% less sugar than their usual commercial product. Probiotic dêguê was fermented using L. rhamnosus yoba 2012 and Streptococcus thermophilus C106; placebo dêguê was fermented using only S. thermophilus C106. We chose L. rhamnosus yoba 2012 as it is a well-documented probiotic strain that has been shown to confer health benefits (e.g., Refs.24,26,38), whereas S. thermophilus alone, common in yogurt production worldwide, has not been examined specifically for its probiotic properties in humans (although it is often paired with other probiotics, due to its synergistic effects26). Ferments were provided to the company in labelled sachets provided by the Yoba-for-Life Foundation. Tests performed in the Netherlands confirmed that the sachets contained the expected bacteria. The local dêguê producer was trained on how to use the Yoba starter culture for the production of probiotic fermented dêguê. Final cell counts are expected to vary between 2-9E7 cfu/mL for L. rhamnosus yoba 2012 and 0.8-2E9 cfu/mL for S. thermophilus C106 (Ref.26, and see Ref.39 for the bacterial profile of L. rhamnosus yoba 2012 in a similar fermented dish). In-country tests of the product confirmed that it was safe for consumption. Adult consumers reported that the products were similar, but that the probiotic dêguê was slightly more sour.
Dêguê was served in locally purchased 125 mL cups with snap-on lids. Probiotic and placebo cups were indistinguishable other than a small label with a nearly-identical series of numbers on the side of the cup. Dêguê was delivered to schools in coolers on ice and distributed in classrooms. Children were monitored to ensure they only consumed their own dêguê.
Measures
Child age and gender
Caregivers reported their child’s gender. Schools and caregivers provided birthdays. When reporters disagreed or provided incomplete data (e.g., a month and year but no day), a series of decisions was used to estimate ages (see Supplementary Material Section S1). Ages are presented as age in days at December 1, 2018.
Socioeconomic status (SES)
Caregivers endorsed which of 20 household items they owned, a common procedure for estimating SES in low-income contexts (e.g., Ref.40). The list of items was created in consultation with local researchers. Scores are the number of items endorsed; higher scores reflect higher SES.
Milliliters of product consumed
Each day, researchers recorded when children were present and consumed 125 mL of dêguê (which weighed 125 g). If a child did not finish a serving, their cup was weighed; the amount remaining was subtracted from 125 g to approximate how much they had eaten. Scores reflect the approximate total milliliters of dêguê consumed prior to T2 testing.
Regularity of product consumption
Children were defined as regular consumers when they consumed some dêguê on at least 2 days in nearly every week it was offered prior to testing.
Pen and paper cognitive tests
All cognitive tests were administered by trained Ivorian researchers in a semi-private area at the child’s school. Tests were administered in the same manner to all participants; parallel forms were used for the second administration of each. The Numeracy task was added to the end of the battery in T2 after researchers became aware of it at a conference. Children used a large marker to complete pen and paper tasks.
Cancellation task
A cancellation task was used to measure selective attention and processing speed (e.g., Ref.41). Children had 60 s to cross out as many target items (e.g., t-shirts) they could find out of 35 among a field of approximately 250 distractor items (e.g., other types of clothing). Scores are the number of correctly crossed items minus the number of incorrectly crossed items.
Numeracy task
To assess numerical magnitude understanding, children completed the Numeracy Screener42 at T2. The screener consists of two sections, a non-symbolic (dots) and a symbolic (numbers) section, completed in an identical manner. In the task, children saw pairs of dot clusters or numbers and were instructed to mark the larger of the two. Children completed a practice round with feedback and then had 60 s to complete as many items as they could out of 56. Children have two scores reflecting the number of correctly completed items for the dot and number sections, respectively.
Computerized cognitive tests
All computer tasks were adapted from the NIH EXAMINER battery43. Adaptations were completed in consultation with local partners after pilot testing and included French translation, simplification of language, removal of written instructions, addition of hand gestures, and increasing the size of the arrow keys using laminated arrows. The tasks were unchanged.
Children could only complete a computer task if they demonstrated proficiency in a practice trial. Children had three opportunities to pass the practice trial for each task before it was skipped. Further details about the measures and score generation can be found in Ref.43.
Flanker task
In this measure of response inhibition, children saw a horizontal line of five fish and were instructed to press the arrow key corresponding to the direction the middle fish was facing, which could be congruent or incongruent with the other fish (e.g., Ref.44). Children had to correctly respond to 6 out of 8 practice items to pass to the task.
The task consisted of 48 trials: 24 congruent and 24 incongruent. Automatically generated scores are on a 0–10 scale and reflect the speed and accuracy of children’s responses in incongruent trials. Higher scores indicate better performance.
Set shifting
In this task measuring cognitive flexibility, children were asked to match a colored shape (e.g., red rectangle) in the middle of the screen to one of two colored shapes (e.g., a blue rectangle and a red triangle) on the bottom of the screen using either a shape rule or a color rule (e.g., Ref.45). Children had to correctly respond to 12 out of 16 practice items to pass to the task.
The task consisted of 104 trials. In the first and second blocks of 20 trials each, children applied a single rule (e.g., shape or color) that changed from block one to block two. In the final 64 trials, the rule shifted from trial to trial. Automatically generated scores are on a 0–10 scale and reflect the speed and accuracy of children’s responses in shifting trials. Higher scores indicate better performance.
Go/no go
In the Continuous Performance Task, a Go/no go (GNG) task that measures sustained and selective attention and response inhibition, children pressed a button when they saw a target image displayed in a series of distractor images (e.g., Ref.46). Children had to correctly respond to 16 out of 20 practice items to pass to the task.
The task consisted of 104 trials. Automatically generated scores reflect the total number of times the child correctly pressed or did not press the button; higher scores indicate better performance.
Analysis plan
Main and exploratory analyses
To examine whether children improved across time on cognitive tests (except Numeracy), we ran paired samples t-tests comparing T1 and T2 scores. To examine whether consumption of a fermented probiotic food product influenced cognition, we performed ANCOVA analyses predicting T2 cognitive performance using group as a predictor and T1 scores as a covariate. In addition, due to a disruption in probiotic administration (see “Results”), we also did exploratory dose–response and regularity analyses to examine whether higher doses or regular administration (as intended) were associated with cognitive outcomes. In the probiotic and placebo groups only, we used multiple regression to see if the amount of dêguê consumed or regularity of consumption influenced T2 scores, controlling for T1 scores and including the group × mL consumed/regularity interaction. Missingness was handled using complete case analysis, as is recommended for trials with large amounts of missing data47.
Sensitivity analyses
We performed two types of sensitivity analysis. First, we a priori decided to include child gender, age, and SES as covariates and reran all analyses accordingly using complete case analysis. Second, for all tasks but the Numeracy task (whose missing data was negligible) we ran sensitivity analyses appropriate to their missing data. For the Cancellation task, we used multiple imputation to replace missing task and covariate values and reran analyses with and without covariates. For all computer tasks, given that data were missing not at random, we performed worst-case scenario analyses with and without covariates in which we calculated mean scores by group and replaced missing values with a value two standard deviations below the mean47.
Results
Preliminary analyses
Between December 2018 and February 2019, 270 children enrolled in the study (Nprobiotic = 87, Nplacebo = 82, NDAU = 101) from two schools in the Koumassi district of Abidjan. Current analyses exclude 16 children outside the target age range, two who enrolled but did not participate, and one in the experimental school who was placed in the DAU group due to medical issues, leaving a final sample of 251 4- to 7-year-old children (Nprobiotic = 74, Nplacebo = 79, NDAU = 98). Six children left the study prior to outcome data collection (Nplacebo = 2, NDAU = 4) but are included in analyses (Fig. 1). Demographic differences between the experimental and control schools revealed that control school caregivers reported higher SES than experimental school caregivers (Table 1).

Consort participant flow diagram. Participants who were lost to follow-up are included in analyses. *One child in the experimental school was excluded because he was in the Diet as Usual group due to dietary issues. His experience was substantially different than all other Diet as Usual participants.
Probiotic and placebo dêguê were provided to experimental school participants every Monday through Friday from January 14, 2019 to May 15, 2019 except 20 days due to production issues, national holidays, and school exams. In the remaining 68 days, children could receive between 53 and 68 portions prior to T2 testing, depending on when they were tested (provision of dêguê continued until the end of testing). Thirty-three of these possible days coincided with a nationwide teacher strike in which schools were closed but the research team was present and attempted contact to encourage caregivers to bring children to school for the consumption of dêguê. The mean number of days children consumed dêguê was 33.65 (SD = 10.97) and equal between groups (Mprobiotic = 33.64, SD = 10.31; Mplacebo = 33.66, SD = 11.69). Experimental groups consumed similar quantities of dêguê over the study period (t = − 0.03; p = 0.979) and had a statistically equivalent number of “regular” consumers (χ2 = 1.87, p = 0.172; Table 1). More than 95% of cups given were finished and no adverse health effects of the product were reported.
Missing data were rare for paper tasks but common for computer tasks as many children did not pass the practice trials (Table 2). For this reason, computer task analyses are considered exploratory and are not representative of the sample as a whole.
Main analyses
Analyses were conducted in SPSS Version 25. Sensitivity analyses are mentioned when they differed from main or exploratory analyses.
Improvement across one semester
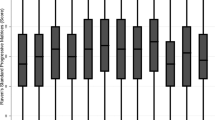
Children improved in all tasks across time (Cohen’s d = 0.08–0.30; Fig. 2; Table 3; Supplemental Materials, Table S1).

Mean cognitive test scores at T1 and T2 by group. Error bars are standard errors.
Probiotic effects
Cancellation
There were no group effects on T2 Cancellation scores (Table 3; Fig. 2). Sensitivity analyses revealed that the placebo group mean was significantly lower than the grand mean; this effect disappeared with the inclusion of imputed covariates (Supplemental Materials, Table S2).
Numeracy
An ANOVA uncovered group effects for dot scores (Table 3, Fig. 2). Fisher’s LSD post-hoc comparison revealed that the placebo group had significantly lower scores than the DAU group (p value). The group effect became nonsignificant with the inclusion of covariates (Supplemental Materials, Table S2). There was no group effect predicting number scores (Table 3; Fig. 2; Supplemental Materials, Table S2).
Computer tasks
There were no group effects predicting T2 Flanker or Set shifting scores in any analysis or for T2 GNG scores in complete case analyses with or without covariates. Worst-case scenario sensitivity analyses revealed that the probiotic group had lower scores than the placebo and DAU groups (Table 3; Fig. 2; Supplemental Materials, Table S3).
Exploratory analyses
Dose response
Cancellation
Milliliters consumed was not significantly associated with T2 Cancellation scores accounting for T1 scores, but its main effect trended toward significance in all analyses (Table 4; Supplemental Materials, Table S4).
Numeracy
Models predicting dot and number scores using milliliters consumed were not significant (Table 4). The model predicting number scores became significant with the inclusion of covariates, but no predictors other than age reached significance (Supplemental Materials, Table S4).
Flanker
Neither group nor milliliters consumed were significant in any models predicting T2 Flanker scores (Table 4; Supplemental Materials, Table S4).
Set shifting
No model predicting T2 Set shifting scores using milliliters consumed were significant except a worst-case scenario sensitivity analysis without covariates in which no predictors other than T1 scores reached significance (Table 4; Supplemental Materials, Table S4).
Go/no go
The model predicting T2 Go/no go scores was not significant (Table 4), but all sensitivity analysis models were (Supplemental Materials; Table S4). Complete case analysis with covariates revealed a significant interaction such that milliliters consumed was negatively associated with Go/no go scores in the probiotic group only. In the worst-case scenario sensitivity analyses, the interaction was not significant, but probiotic group scores were lower than those for the placebo group (Supplemental Materials; Table S4).
Regularity effects
Cancellation
There was a main effect of regularity on T2 scores accounting for T1 scores, with regular consumers having higher scores than non-regular consumers (Table 4). The effect trended toward significance in sensitivity analyses using multiple imputation (Supplemental Materials; Table S5).
Numeracy
Models predicting dot and number scores using regularity classification were not significant (Table 4). Models with covariates were significant, but neither group nor regularity classification effects were (Supplemental Materials; Table S5).
Flanker
There were fewer than 10 regular consumers with Flanker scores, so we ran this only as a worst-case scenario analysis and found no effects (Supplemental Materials; Table S5).
Set shifting
There were fewer than 10 regular consumers with set shifting scores, so we ran this only as a worst-case scenario analysis and found no effects (Supplemental Materials; Table S5).
Go/no go
The model predicating T2 Go/no go scores with regularity classification and group was not significant (Table 4). The models were significant in worst-case scenario sensitivity analyses and in both, group significantly predicted Go/no go scores with probiotic scores being lower than placebo (Supplemental Materials; Table S5).
Discussion
This semi-randomized controlled trial examined cognitive change over time and the effects of a probiotic food intervention on first-graders’ cognitive outcomes. Children improved across one semester in all tasks, showing significantly higher scores and more children able to complete tasks at T2. Examinations of probiotic effects were discrepant between main and sensitivity analyses but largely indicated no effect of the probiotic on cognition in the present sample.
Notably, children showed improvement in all tasks despite a disrupted semester in which schools were closed for 5 weeks (and then closed every Wednesday after courses resumed) due to a nationwide teacher strike. That children improved is consistent with the notion that aspects of executive functioning improve across one semester (e.g., Ref.48) and suggests that such improvements are not entirely dependent on formal schooling. This study provides a first look into normative cognitive development over time in first grade children in Côte d’Ivoire. Future work examining how gains are amplified in an uninterrupted school year will add to the growing body of literature on cognitive development in LMICs. In addition, examining how this population compares with other populations in Abidjan and surrounding areas (e.g., higher SES; more rural) could inform the field on factors contributing to cognitive development in LIMCS.
In the current sample, there were no apparent effects of the probiotic on cognition. This may be in part because the consumption of dêguê was substantially interrupted due to the 5-week teacher strike during which less than 20% of participants came to school to consume dêguê. In addition, analyses must be considered critically as we were unable to reach our target sample of 300 participants, leading to power concerns, particularly in the computer tasks which also had large amounts of missing data. Interestingly, although results did not reach significance, our most consistent analyses point toward possible effects of milliliters consumed and regularity on cancellation scores (in the probiotic and placebo groups only). While these trends could also be explained by unexamined child characteristics, such as agreeableness (e.g., willingness to consume the product and put forth effort on tests), we note that the majority of children consumed all dêguê offered to them, so this seems unlikely. Moreover, we also found a potential (i.e., only apparent in sensitivity analyses) effect in the opposite direction, with children who consumed more (both more mL consumed and more consistently) probiotic having lower Go/no go scores than children in the placebo group. While we considered all computer tasks to be both exploratory and non-representative of the sample as a whole (due to the large amount of missing data), this puzzling finding was consistent across both analyses and deserves consideration in future work. Most important, consistent and prolonged administration will be necessary to draw strong conclusions about probiotic effects on cognitive outcomes. Indeed, such studies are warranted given recent evidence pointing to probiotic effects on attention tasks in Thai children (6–12-year-olds) after prolonged (12 weeks) administration49. Moreover, multiple reviews published since this study was conducted have found evidence for a potential role of probiotics and prebiotics in improved cognitive function in humans50,51,52. Importantly, we note that all studies finding effects engaged in uninterrupted and/or prolonged (12 or more weeks) probiotic administration, underscoring the importance consistent administration will play in future investigations.
This ambitious study was the first of its type in Côte d’Ivoire and provided valuable insight, as did a previous study in Uganda with the same probiotic strains and another in Tanzania using a different probiotic strain38,53. In the current study, children appreciated the dêguê (i.e., 95% consumed the whole portion every time), and the product was easily produced and affordable, costing only 0.39 USD per 125 mL. Approaches using a similar fermented dairy product including the same strains tested here have shown that regular consumption can decrease intestinal infections, upper respiratory tract infections, and angina, and that their administration is feasible on a large scale24,38. Understanding the full range of benefits such probiotics may provide is a worthy goal, given their safety, availability, ease of use, and acceptance in diverse populations. In particular, due to a long tradition of consuming fermented foods in African culture, some scholars suggest that the local production and distribution of affordable probiotics holds promise to both empower women through small enterprises and positively affect the health of probiotic consumers54. Given the equivocal nature of our results (due to probiotic administration disruption and measurement difficulties) researchers should continue to examine whether affordable, locally produced, health-promoting foods can enhance also cognitive development, particularly in at-risk populations.
Despite challenges, this study has strengths. It was a three-armed semi-randomized controlled trial with very low attrition and high compliance. Children participated readily in the cognitive testing sessions and enjoyed the locally produced dêguê. Given large amounts of missing data, two types of sensitivity analyses leant support to the findings. Limitations of the present study are acknowledged as follows: first, as mentioned, it was not possible to deliver the probiotic food intervention 5 days a week during 4 consecutive months as planned. Second, although the study was designed for first grade (CP1) and hence piloted in 6- to 7-year-old children, the mean participant age was 5.5 years, which was unanticipated. This precluded some aspects of data collection (e.g., a test of working memory that required counting; self-reports of health) intended for use in the current investigation.
The breadth of ages in the current sample also brings up some important considerations for future work examining cognition in similar populations. LMIC researchers in schools might prepare for a substantially larger age range than would be expected per grade level and pilot in a wide range of ages to ensure test feasibility beyond what previous research has shown. The EXAMINER manual reports that 96.5% of 3–7-year-olds were able to complete the tasks used in the current study and indeed, much literature indicates that tasks such as the ones used in the present investigation can be used with younger populations. However, given that our majority five-year-old population struggled with the computer (but not the paper) tasks, researchers might also consider using non-digital versions in future work examining similar populations (e.g., Ref.55). Notably, the EXAMINER was normed in populations accustomed to electronic devices43. Evidence using touch screen tablets shows that electronic assessments are feasible for use in school aged children in LMICs, but we found that computerized assessments, where children have to link concepts on a screen to one or two keys on a keyboard, were too complicated for many participants, despite instructional adaptations designed to make them clearer (e.g., Ref.56). This study adds to the work of Willoughby et al.9 addressing the need to develop low cost and accessible ways of testing early cognition in LMICs by noting that computerized assessments (as opposed to tablet based) may prove too complicated for use in certain contexts. In addition, researchers may consider interviewing teachers to ascertain the academic ability of their participants before implementing measures that rely on letter and number recognition.
This study is a promising step in a research agenda aimed at examining cognitive development in LMIC contexts. We add to the literature by demonstrating that economically disadvantaged children improved in multiple domains of executive functioning across one semester, and by discussing some necessary considerations of using computerized cognitive assessments in a single grade level in French-speaking West Africa. These considerations will be valuable for researchers intending to conduct similar work in like settings. We also note that, despite significant study disruption due to socio-political factors, the study was well received by both the participants and the community. Given the general feasibility of the study, we hope that it may serve as an inspiration for future research into child development and into sustainable (health-promoting) interventions for school children in developing nations.
Data availability
Data Sharing: We did not have participant consent to store deidentified data in an online repository. Deidentified participant data underlying the reported results will be available upon publication (no end date) to researchers with a methodologically sound proposal for use. Proposals should be directed to carolina.deweerth@radboudumc.nl.
References
Diamond, A. Executive functions. Annu. Rev. Psychol. 64, 135–168 (2013).
Wang, Y. & Zhou, X. Longitudinal relations between executive function and internalizing problems in grade school: The role of peer difficulty and academic performance. Dev. Psychol. 55(10), 2147–2158 (2019).
Ribner, A. D., Willoughby, M. T., Blair, C. B., Family Life Project Key Investigators. Executive function buffers the association between early math and later academic skills. Front. Psychol. 8, 869 (2017).
Jacobson, L. A., Williford, A. P. & Pianta, R. C. The role of executive function in children’s competent adjustment to middle school. Child. Neuropsychol. J. Norm. Abnorm. Dev. Child. Adolesc. 17(3), 255–280 (2011).
Geary, D. C., Hoard, M. K., Nugent, L. & Bailey, D. H. Adolescents’ functional numeracy is predicted by their school entry number system knowledge. PLoS One 8(1), e54651 (2013).
Rodgers, J., Kakarmath, S., Denis, V., Encinas-Martin, M. & Subramanian, S. V. Association between numeracy and self-rated poor health in 33 high- and upper middle-income countries. Prev. Med. 129, 105872 (2019).
Estrada-Mejia, C., de Vries, M. & Zeelenberg, M. Numeracy and wealth. J. Econ. Psychol. 54, 53–63 (2016).
Henrich, J., Heine, S. J. & Norenzayan, A. The weirdest people in the world?. Behav. Brain Sci. 33(2–3), 61–83 (2010) (discussion 83–135).
Willoughby, M. T., Piper, B., Kwayumba, D. & McCune, M. Measuring executive function skills in young children in Kenya. Child. Neuropsychol. J. Norm. Abnorm. Dev. Child. Adolesc. 25(4), 425–444 (2019).
Abessa, T. G., Bruckers, L., Kolsteren, P. & Granitzer, M. Developmental performance of hospitalized severely acutely malnourished under-six children in low- income setting. BMC Pediatr. 17(1), 197 (2017).
Obradović, J., Yousafzai, A. K., Finch, J. E. & Rasheed, M. A. Maternal scaffolding and home stimulation: Key mediators of early intervention effects on children’s cognitive development. Dev. Psychol. 52(9), 1409–1421 (2016).
Willoughby, M. T., Piper, B., Oyanga, A. & Merseth, K. K. Measuring executive function skills in young children in Kenya: Associations with school readiness. Dev. Sci. 22(5), e12818 (2019).
Liddell, C. & Rae, G. Predicting early grade retention: A longitudinal investigation of primary school progress in a sample of rural South African children. Br. J. Educ. Psychol. 71(Pt 3), 413–428 (2001).
Lu, C., Black, M. M. & Richter, L. M. Risk of poor development in young children in low-income and middle-income countries: An estimation and analysis at the global, regional, and country level. Lancet Glob. Health. 4(12), e916–e922 (2016).
Aurino, E., Wolf, S. & Tsinigo, E. Household food insecurity and early childhood development: Longitudinal evidence from Ghana. PLoS One 15(4), e0230965 (2020).
Wacoo, A. P. et al. Aflatoxins: occurrence, exposure, and binding to Lactobacillus species from the gut microbiota of rural ugandan children. Microorganisms. 8(3), E347 (2020).
Walker, S. P. et al. Child development: Risk factors for adverse outcomes in developing countries. Lancet Lond. Engl. 369(9556), 145–157 (2007).
Ezeamama, A. E. et al. Helminth infection and cognitive impairment among Filipino children. Am. J. Trop. Med. Hyg. 72(5), 540–548 (2005).
Kyere, P., Veerman, J. L., Lee, P. & Stewart, D. E. Effectiveness of school-based nutrition interventions in sub-Saharan Africa: A systematic review. Public Health Nutr. 23(14), 2626–2636 (2020).
Hulett, J. L. et al. Animal source foods have a positive impact on the primary school test scores of Kenyan schoolchildren in a cluster-randomised, controlled feeding intervention trial. Br. J. Nutr. 111(5), 875–886 (2014).
Lee, R. et al. Milk powder added to a school meal increases cognitive test scores in ghanaian children. J. Nutr. 148(7), 1177–1184 (2018).
Hill, C. et al. Expert consensus document. The international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 11(8), 506–514 (2014).
Bisanz, J. E. et al. Randomized open-label pilot study of the influence of probiotics and the gut microbiome on toxic metal levels in Tanzanian pregnant women and school children. MBio 5(5), e01580-e11514 (2014).
Villena, J. et al. Probiotics for everyone! The novel immunobiotic Lactobacillus rhamnosus CRL1505 and the beginning of Social Probiotic Programs in Argentina. Int. J. Biotechnol. Wellness Ind. 1(3), 189–198 (2012).
Basu, S., Paul, D. K., Ganguly, S., Chatterjee, M. & Chandra, P. K. Efficacy of high-dose Lactobacillus rhamnosus GG in controlling acute watery diarrhea in Indian children: A randomized controlled trial. J. Clin. Gastroenterol. 43(3), 208–213 (2009).
Kort, R. et al. A novel consortium of Lactobacillus rhamnosus and Streptococcus thermophilus for increased access to functional fermented foods. Microb. Cell Factories. 8(14), 195 (2015).
Hutchinson, A. N. et al. The effect of probiotics on health outcomes in the elderly: A systematic review of randomized, placebo-controlled studies. Microorganisms. 9(6), 1344 (2021).
Carlson, A. L. et al. Infant gut microbiome associated with cognitive development. Biol. Psychiatry. 83(2), 148–159 (2018).
Gao, W. et al. Gut microbiome and brain functional connectivity in infants-a preliminary study focusing on the amygdala. Psychopharmacology 236(5), 1641–1651 (2019).
O’Hagan, C. et al. Long-term multi-species Lactobacillus and Bifidobacterium dietary supplement enhances memory and changes regional brain metabolites in middle-aged rats. Neurobiol. Learn. Mem. 144, 36–47 (2017).
Lv, T. et al. Probiotics treatment improves cognitive impairment in patients and animals: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 120, 159–172 (2021).
Marx, W. et al. Prebiotics, probiotics, fermented foods and cognitive outcomes: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 118, 472–484 (2020).
Eastwood, J., Walton, G., Van Hemert, S., Williams, C. & Lamport, D. The effect of probiotics on cognitive function across the human lifespan: A systematic review. Neurosci. Biobehav. Rev. 24(128), 311–327 (2021).
Slykerman, R. F. et al. Effect of early probiotic supplementation on childhood cognition, behaviour and mood a randomised, placebo-controlled trial. Acta Paediatr. Oslo Nor. 1992 107(12), 2172–2178 (2018).
Pärtty, A., Kalliomäki, M., Wacklin, P., Salminen, S. & Isolauri, E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: A randomized trial. Pediatr. Res. 77(6), 823–828 (2015).
van den Nieuwboer, M. et al. Safety of probiotics and synbiotics in children under 18 years of age. Benef. Microbes. 6(5), 615–630 (2015).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods. 41(4), 1149–1160 (2009).
Westerik, N., Nelson, A., Wacoo, A. P., Sybesma, W. & Kort, R. A Comparative interrupted times series on the health impact of probiotic yogurt consumption among school children from three to six years old in Southwest Uganda. Front. Nutr. 7, 574792 (2020).
Parker, M. et al. Naturally fermented milk from Northern Senegal: Bacterial community composition and probiotic enrichment with Lactobacillus rhamnosus. Front. Microbiol. 9, 2218 (2018).
Fotso, J.-C. & Kuate-Defo, B. Measuring socioeconomic status in health research in developing countries: Should we be focusing on households, communities or both?. Soc. Indic. Res. 72(2), 189–237 (2005).
Wechsler, D. Wechsler Intelligence Scale for Children, 5th ed. (PsychCorp, 2014).
Nosworthy, N., Bugden, S., Archibald, L., Evans, B. & Ansari, D. A two-minute paper-and-pencil test of symbolic and nonsymbolic numerical magnitude processing explains variability in primary school children’s arithmetic competence. PLoS One 8(7), e67918 (2013).
Kramer, J. H. et al. NIH EXAMINER: Conceptualization and development of an executive function battery. J. Int. Neuropsychol. Soc. JINS. 20(1), 11–19 (2014).
Eriksen, B. A. & Eriksen, C. W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 16(1), 143–149 (1974).
Hooper, S. R., Swartz, C. W., Wakely, M. B., de Kruif, R. E. L. & Montgomery, J. W. Executive functions in elementary school children with and without problems in written expression. J. Learn. Disabil. 35(1), 57–68 (2002).
Kirmizi-Alsan, E. et al. Comparative analysis of event-related potentials during Go/NoGo and CPT: Decomposition of electrophysiological markers of response inhibition and sustained attention. Brain Res. 1104(1), 114–128 (2006).
Jakobsen, J. C., Gluud, C., Wetterslev, J. & Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol. 17(1), 162 (2017).
Shen, Y., Lin, Y., Liu, S., Fang, L. & Liu, G. Sustained effect of music training on the enhancement of executive function in preschool children. Front. Psychol. 10, 1910 (2019).
Fukngoen, P. et al. The influence of Lactobacillus paracasei HII01 supplementation on performance in attention (Go/No-Go) tasks and quinolinic acid and 5-hydroxyindoleacetic acid levels in Thai Children—A preliminary study. Appl. Sci. 12(11), 5658 (2022).
Baldi, S., Mundula, T., Nannini, G. & Amedei, A. Microbiota shaping—The effects of probiotics, prebiotics, and fecal microbiota transplant on cognitive functions: A systematic review. World J. Gastroenterol. 27(39), 6715–6732 (2021).
Basso, M. et al. A systematic review of psychobiotic interventions in children and adolescents to enhance cognitive functioning and emotional behavior. Nutrients 14(3), 614 (2022).
Eastwood, J., Walton, G., Van Hemert, S., Williams, C. & Lamport, D. The effect of probiotics on cognitive function across the human lifespan: A systematic review. Neurosci. Biobehav. Rev. 128, 311–327 (2021).
Dols, J. A. M. et al. The impact of probiotic yogurt on HIV positive women in Tanzania. Int. Dairy J. 21(8), 575–577 (2011).
Reid, G. et al. Empowering women through probiotic fermented food in East Africa. J. Glob. Health. 10(1), 010330 (2020).
Willoughby, M. T., Blair, C. B., Wirth, R. J. & Greenberg, M. The measurement of executive function at age 5: Psychometric properties and relationship to academic achievement. Psychol. Assess. 24(1), 226–239 (2012).
Pitchford, N. J. & Outhwaite, L. A. Can touch screen tablets be used to assess cognitive and motor skills in early years primary school children? A cross-cultural study. Front. Psychol. 7, 1666 (2016).
Acknowledgements
We thank the many contributors who helped make this study happen. We are especially thankful for our local partners, too numerous to name but including: the dêguê production team, the school directors and teachers who helped us facilitate testing and probiotic administration, the government officials who helped us find the families and schools to participate in this study, our partners from the Jacobs Foundation at Transforming Education in Cocoa Communities (TRECC) who helped us navigate the local landscape and gave us a home from which to operate, our esteemed research partners who were integral to keeping the study running even in the face of political turmoil, and the families and children who were kind enough to be a part of the study. We also thank Daniel Ansari for generously providing us with the Numeracy Screener in French and Dr. Nieke Westerik for the yoghurt-production training she provided.
Author information
Authors and Affiliations
Contributions
Authors took on the following CRediT roles: B.E.B.: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing—original draft, review, and editing, visualization; H.O.Y.D.: investigation, methodology, project administration, resources, writing-reviewing and editing; B.K.: investigation, methodology, project administration, resources, writing-reviewing and editing; F.K.K.: investigation, methodology, writing-reviewing and editing; S.E.A.: investigation, methodology, writing-reviewing and editing; K.Y.A.S.Z.: investigation, methodology, writing-reviewing and editing; R.K.: conceptualization, methodology, resources, writing—review and editing; W.S.: conceptualization, methodology, resources, writing—review and editing; G.R.: conceptualization, methodology, writing—review and editing; and C.W.: conceptualization, data curation, funding acquisition, methodology, project administration, resources, supervision, writing—original draft, reviewing and editing.
Corresponding author
Ethics declarations
Competing interests
WS and RK developed the starter culture sachets and founded the Yoba for Life Foundation, a non-profit networking organization aiming to improve health and wealth of people in developing countries by facilitating local production of probiotic fermented food.WS and RK gain no financial benefits from their Yoba for Life activities. BEB, HOYD, BK, FKK, SEA, KYASZ, GR, and CdW have no declarations of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Brett, B.E., Doumbia, H.O.Y., Koko, B.K. et al. Normative cognition and the effects of a probiotic food intervention in first grade children in Côte d’Ivoire. Sci Rep 12, 19491 (2022). https://doi.org/10.1038/s41598-022-23797-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23797-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
