
Abstract
Peer victimization have a negative impact on Health-Related Quality of Life (HRQoL) during adolescence, however some personal skills such a person's resilience could play a significant role in this relationship. In this context, this study aims to analyse if resilience is a moderator of the relation between peer victimization and HRQoL’s psychological dimensions. Sociodemographic data, peer victimization, psychological domains of HRQoL and resilience were measures in a sample of 1428 secondary school students using the following scales: “Adolescent Peer Relations Instrument-Bullying”, “KIDSCREEN-52” and “Brief Resilient Coping Scale. Different multivariate analyses were carried out using linear regression. PROCESS tool was used to examine the moderating role of resilience, with John-Neyman post-hoc approach to quantify moderation. Results suggest that resilience could moderate the association between physical (β = − 0.0021; p = 0.025) and verbal victimization (β = − 0.0018; p = 0.024) and the “Mood and Emotions” dimension of adolescents’ HRQoL. Nevertheless, this regulating influence appears to be faint (∆R2 0.004). Resilience showed no moderating effect between social victimization and psychological dimensions of HRQoL. We concluded that resilience could function as a protective factor that weakly regulates the negative association between physical and verbal victimization and the psychological sphere of adolescents’ HRQoL.
Similar content being viewed by others


Introduction
Peer victimization has been suggested as a type of abuse in which an adolescent or child is frequently the object of aggressive and/or unsolicited behaviour (victim) from one or more schoolmates (bullies)1. It is a societal phenomenon that has become increasingly common and problematic2, representing the most prevalent type of violence during school years3, especially in adolescence4. According to World Health Organization5, one-third of children and teenagers have been bullied by their peers at least once in their lifetime. Specifically, in Spain, the reported lifetime prevalence of peer victimization is even higher6 with a probability of having been harassed by colleagues ranging from 48.8% to 62.2%7,8.
Negative actions within traditional peer victimization can be physical (e.g. punching, pushing, kicking, hitting), verbal (e.g. teasing, threatening, name calling) and social (e.g. rumour spreading, social exclusion)9. In addition, with the incorporation of new technologies into our digital society, recent forms of attack on the Internet– cyberbullying – have recently emerged10, with an increasing time trend11.
The impact of peer victimization on adolescents’ health has been extensively studied during the past decades12,13. This period of life is especially susceptible to victimization effects due to the importance of social relationships, the intensity in the perception of emotions and biological changes 14. Researchers have documented how experiencing victimization by peers, in any of its forms, affects negatively youths’ physical and mental health15,16,17. Health-Related Quality of Life (HRQoL), a multidimensional concept that covers functional status and individual assessment of physical, mental and social health 18, is one of the health correlates related to peer victimization. It is well-recognized that adolescents who are victimized by their peers, and especially those who experience more than one form of victimization 19, have a lower HRQoL compared to youths who are not involved20,21,22. Moreover, recent research has shown that all types of peer victimization negatively affect HRQoL and, in particular, its psychological domains. Of all forms of peer victimization, physical violence appears to be the one that most negatively affects adolescents’ HRQoL23. However, victims can present different psychological and emotional outcomes even if they faced the same type of harassment.
Little data is still known about protective factors that might facilitate better psycho-emotional HRQoL among teens who have suffered from peer victimization. Protective factors are defined as elements that can mitigate the harmful impact of being exposed to risk, in this case, victimization by peers24. Resilience has been emphasized as a widely studied protective factor by several authors25,26,27. It has been conceived as a personal trait, a result or a process of adaptation28 that leads a person to recover from negative emotional experiences or, ultimately, adversity 29. Previous studies have analysed how resilience mediated the relation between peer victimization and negative outcomes on HRQoL 20, subjective well-being 30,31 or youth’s mental health problems27,32,33. All the studies previously mentioned show that resilience plays a role in regulating the harmful impact that peer victimization has on different health’s correlates. However, the extent to which it is able to modulate this impact is controversial. Moreover, little is known about the association between different types of peer victimization, resilience and its effect on specific dimensions of HRQoL.
Accordingly, this study was conducted to examine the association between psychological domains of HRQoL and resilience among adolescents exposed to different forms of peer victimization (physical, verbal and social). Consequently, we analysed if resilience is a moderator of the relation between peer victimization and the “psychological well-being” and “mood and emotions” dimensions of the HRQoL. As a secondary objective, it was also studied whether there were differences in adolescents’ resilience levels according to sociodemographic factors.
Methods
General design and participants
A retrospective cross-sectional study was conducted including secondary school students (12–16 years old) recruited from all academic centres in a city located in south-eastern Spain (n = 1476). Every adolescent meeting the inclusion criteria was invite to take part in the present research. The inclusion criteria were: (a) being a secondary school student, (b) fluency Spanish to understand the questionnaire, (c) having obtained legal tutors’ written consent before joining the study.
Before starting the fieldwork, a letter was sent to the city council’s Department of Education to inform them about the research project and approval was obtained. Department of Education transmitted the information to the participating secondary schools’ heads and, they, to major teachers of each class. Several meetings between the research committee and secondary schools’ heads took place to discuss the protocol to be followed as well as to plan the logistics and data collection methods.
Information was obtained during the last 30 days of the school year from self-completed questionnaires administered by major teachers during class time. Data collection was supervised by qualified staff of the research committee. Adolescents were given one hour to complete the entire questionnaire. All questionnaires were completed anonymously by students. Written consent was obtained from parents via Parents’ Associations in all participating schools before joining the study.
The present study was approved by the Research Ethics Committee of Murcia’s University.
Instruments
Sociodemographic variables were collected by means of a questionnaire designed ad hoc. The variables included were gender, age, family structure (Nuclear, Mononuclear or No parents at home), ethnic origin (parents’ birthplace: both Spanish, one Spanish, Maghreb, Latin-Ecuador or Others which included all other options) and parental educational attainment. Based on the procedure proposed by the Spanish Society of Epidemiology34, information about social class in terms of parents’ employment was also included. For both parental educational attainment and social class, the highest positions of both parents were taken as a reference.
Peer victimization was measured using the validated Spanish version of the “Adolescent Peer Relation Instrument-Bullying (APRI)”, developed by Parada35,36. This scale comprises 18 items and measures three different dimensions of peer victimization: physical (6 items), verbal (6 items) and social (6 items). Each item is rated on a 4-point Likert scale (0 = Never/seldom, 1 = Frequently, 2 = Very often, 3 = Constantly), which indicates the frequency of peer victimization suffered by an adolescent from the beginning to the end of the academic year (9-month retrospective follow-up). The score for each dimension was calculated as the sum of the respective items. The higher the score on each subscale, the stronger the victimization suffered by the teenager.
Adolescents were considered victims of each form of victimization if they reported having suffered “frequently” at least one of the behaviours indicated in the questionnaire during the last academic year.
HRQoL was measured by analysing two out of ten dimensions of the validated and adapted to Spanish version of the KIDSCREEN-52 questionnaire37: Psychological Well-being (6 items) and Mood and Emotions (7 items). Each item is rated on a five-point Likert scale corresponding to feelings of well-being over the previous week (Never = 1, Seldom = 2, Sometimes = 3, Often = 4, or Always = 5). Scores are calculated independently for each dimension as T- values of the Rasch scores corresponding to the sum of the response options 38. The higher the score on each dimension, the higher the quality of life related to that dimension.
Resilience was assessed using the validated and adapted to Spanish version of the “Brief Resilient Coping Scale (BRCS)”39,40. This scale comprises 4 items and measures a person’s ability to cope with stress in a highly adaptative way. Each item is rated on a five-point Likert scale corresponding to the degree of agreement that the person feels about him/herself, ranging from “1 = completely disagree” to “5 = completely agree”. The score for resilience was calculated as the sum of the four items, with higher scores denoting higher resilience levels. Resilience total scores were standardised on a scale from 0 to 100 points in order to ease its interpretation.
Statistical analysis
All descriptive and inferential analyses were performed using the Statistical Package for Social Sciences SPSS – 24.0 and the statistical package Stata, version 16.0. p-values < 0.05 were considered to be statistically significant.
The adolescents’ sociodemographic characteristics were analysed using descriptive analysis calculating frequencies and percentages. The mean scores and standard deviations (SD) of the scale measuring adolescents’ resilience levels were calculated according to sociodemographic characteristics. Any sociodemographic related differences were tested by applying a one-way analysis of variance (ANOVA)41. Welch’s t-test was applied to test the hypothesis of means’ equality between the different categories of the studied variables42. Differences between groups were assessed using Tamhane’s T243 when variances were heterogeneous while Fisher’s Least Significant Difference (LSD) test44 was applied when variances were homogeneous.
Several multivariable linear regressions45 were carried out to study the associations between peer victimization and resilience on psycho-emotional dimensions of HRQoL. To detect whether resilience moderated the association of peer victimization on adolescents’ HRQoL, Hayes PROCESS tool was used to examine the moderating role of resilience 46. To explore moderating effects, post hoc analyses were conducted using the Johnson–Neyman technique with Hayes’s PROCESS. Before carrying out linear regression analyses, assumptions associated with a linear regression model were checked for compliance47. Linearity and homoscedasticity were checked by using scatter plots. Normality was tested by P-P plots. Independence was verified by calculating Durbin-Watson statistics and by checking their values were between 1.5 and 2.5. The absence of multicollinearity was tested by measuring Tolerance (> 0.10) and Variance Inflation Factor (< 5). Each form of peer victimization (physical, social and verbal) was taken as an independent variable. On the other hand, “Psychological well-being” and “Moods and Emotions” were taken as dependent variables. Resilience was introduced as the moderating variable. Gender and age were also inputted as covariates. Gender was handled as a dummy variable, considering as reference category “girl” (girl = 0; boy = 1). Analyses were carried out by calculating β coefficient at a 95% Confidence Interval (CI).
A series of confirmatory factor analysis48 by means of the corresponding Structural Equation Model were used to determine the validity of the scores of the three scales used according the theoretical internal structure of each questionnaire (a first order model consisting of three and two correlated factors for the APRI and KIDSCREEN respectively and a one-dimensional first order model for the BRCS). Therefore, Maximum Likelihood method with Satorra Bentler (SB) correction for non-normality49 was used to estimate parameter and calculated goodness-of-fit indices. In this sense, we estimate the goodness of fit of the scales using the “Root Mean Square Error of Approximation” (RMSEA), the “Comparative Fit Index” (CFI), the Tucker-Lewis index (TLI) and the “Standardized Root Mean Square Residual” (SRMR) using the Satorra-Bentler scaled chi2 statistic in their calculation. RMSEA < 0.05, CFI and TLI > 0.95 and SRMR < 0.05 indicate good fit for model while RMSEA < 0.08, CFI and TLI > 0.90 and SRMR < 0.06 indicate a reasonable fit50. In addition, stability of measurements or consistency of each subscale was measured using the “composite reliability” (CR) coefficient and taking into account the values of the “standardized factors loadings for the indicators” and the “variances of the error for the indicators” obtained in the corresponding CFA51. CR values above 0.7 were found satisfactory52.
Ethics approval
The present study was approved by the Research Ethics Committee of Murcia’s University. All procedures performed in the study were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants (and their parents/legal guardians) included in the study.
Results
Demographic characteristics and prevalence of peer victimization among adolescents
Thirty-five adolescents of the eligible population did not obtain written consent from their legal tutors and 13 teenagers did not obtain written consent. From the remaining students, 1341 of them finally completed the entire questionnaire (effective participation rate = 90.8%). Figure 1 shows the participant flow chart during the study.

Flow chart of the study population.
Participants included 709 boys (52.9%) with a mean age of 14.6 years (SD = 1.2) and an age range of 12 – 18 years. The majority (85.6%) belonged to a nuclear family, in which both parents were Spanish (64.7%). Two–thirds of the main breadwinners worked in semi-skilled or unskilled manual jobs, and less than one fifth had higher education.
One quarter of the participants reported having been victims of at least one form of victimization. (Table 1).
Validity and reliability of the scores of the scales in the study sample
Confirmatory Factor Analysis (CFA) showed a reasonable fit to the sample data for the APRI (95%CI RMSEA = 0.062–0.071; RMSEA(SB) = 0.027; CFI(SB) = 0.964; TLI(SB) = 0.958; SRMR = 0.035), the two KIDSCREEN domains (95%CI RMSEA = 0.070–0.082; RMSEA(SB) = 0.066; CFI(SB) = 0.933; TLI(SB) = 0.918; SRMR = 0.043), and the BRCS questionnaire (95%CI RMSEA = 0.001–0.083; RMSEA(SB) = 0.009; CFI(SB) = 0.999; TLI(SB) = 0.999; SRMR = 0.005). Internal consistency was also adequate for the three used scales (Composite reliability was 0.755 for the BRCS scale, while it ranged between a minimum of 0.855 and a maximum of 0.887 in the three subscales of the APRI and 0.853–0,850 for the “Psychological well-being” and “Mood and emotions” KIDSCREEN domains respectively.
Resilience levels and HRQoL`s psycho-emotional domains according to sociodemographic characteristics
From a 0 to 100 range, the mean resilience levels of participants calculated through the BRCS questionnaire was 61.4 points (SD = 25.3 points). As shown in Table 2, no statistically significant results were found between adolescents’ resilience levels according to sociodemographic characteristics.
Results in Tables 3, 4 and 5 show how HRQoL’s levels decreased as the age of the adolescents increased. This specially occurred for “Moods and Emotions” domain, in particular when adjusted by social victimization (β = − 1.22; CI 95% − 1.63, − 0.80).
A significant relation was also found between gender and HRQoL in “Moods and Emotions” dimension. Women obtained lower scores, with β-values ranging from a minimum of − 2.21 (CI 95% − 3.21, − 1.21) adjusted by verbal victimization to a maximum of − 2.00 (CI 95% − 2.99, − 1.00) adjusted by social victimization.
Resilience as a moderator of relation between peer victimization and psycho-emotional domains of HRQoL
The main objective of this study was to examine adolescents’ resilience as a moderator of the relationship between physical, social and verbal victimization and the psychological domains of adolescents’ HRQoL.
It was observed how resilience levels had a directly proportional linear correlation with psychological well-being and mood levels, with β-values ranging from a minimum of 0.06 (CI 95%0.04, 0.08) adjusted by physical and social victimization to a maximum of 0.09 (CI 95% 0.07, 0.11) adjusted by verbal victimization (see Tables 3, 4 and 5).
Peer victimization was negatively associated with both domains of HRQoL. The negative association of violence was particularly stronger on psychological well-being, with social victimization reaching the highest β-values − 0.20 (CI 95% − 0.30, − 0.10).
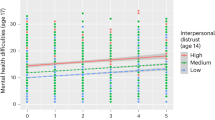
The moderating effect of resilience between the association of peer victimization and HRQoL’s psycho-emotional dimensions was statistically significant between “Mood and Emotions” domain with physical victimization (β = − 0.0021; CI 95% − 0.004, − 0.0003; p = 0.025) and verbal victimization (β = − 0.0018; CI 95% − 0.0034, − 0.0002; p = 0.024), but not in case of social victimization. However, these relations were weak and accounted for only an additional 0.4% of variance in adolescents’ mood in both cases (∆R2 0.004). However, no moderating effect on resilience was found between victimization in any of its forms and psychological well-being.
There were no statistical significance transition points within the moderating effect of resilience using the Johnson-Neyman method in any of the victimizations. (Figs. 2 and 3).

Johnson–Neyman method to study conditional effect of resilience as a moderator of the association between “Mood and Emotions” and Physical victimization. Y-axis represents β-coefficients.

Johnson–Neyman method to study conditional effect of resilience as a moderator of the association between “Mood and Emotions” and Verbal victimization. Y-axis represents β-coefficients.
Discussion
To our knowledge, this is one of the first studies to explore the association between specific types of peer victimization experienced by adolescents, resilience and its possible modulating power on HRQoL’s psychological dimensions. We sought to analyse whether adolescents’ resilience could function as a moderating factor of the relation between physical, social and verbal victimization and the HRQoL’s psychological domains.
This study suggests that resilience could regulate the association between physical and verbal victimization and the “Mood and Emotions” dimension of adolescents’ HRQoL. Nevertheless, this regulating influence appears to be faint since it only represents an additional 0.4% of variance in adolescents’ mood in both cases. On the other hand, no modulating effect of resilience was found related to victimization and HRQoL when it came to social victimization or the “Psychological Well-being” domain of HRQoL.
Although previous studies have considered resilience to be a powerful factor that mediated the relation between peer victimization and different adolescents’ health correlates33, other authors have also demonstrated that this regulating effect is weak30,32. The latter is the case of the present study, in which weak relations or none were found in the analysis of the associations between resilience, specific HRQoL’s dimensions and the most important types of peer victimization (physical, social and verbal).
According to prior literature53,54, the results of this research show that high resilience levels are associated with better psychological HRQoL. Likewise, those adolescents who reported having suffered peer victimization are those with the worst HRQoL in psychological terms20, obtaining the worst results in the case of psychological well-being when suffering social victimization. Therefore, as mentioned above, the results of the present study show that resilience is associated to peer victimization and psychological HRQoL, but no robust moderating effect of resilience was observed between peer victimization and psychological HRQoL. These results support theories proposed by other authors30,31: peer victimization may lead to a depletion or detriment of personal tools for coping with distress relationships or other adverse events, that is, it may lead to a depletion of resilience. In this sense, lower resilience levels in these adolescents mean that their modulatory capacity to avoid adverse effects on their HRQoL’s psychological sphere is reduced. This would explain the reduced regulatory power of resilience in these terms and, therefore, its association with lower levels of HRQoL in victims compared to not victimized adolescents. This hypothesis could lead us to suggest that social victimization negatively affects adolescents’ resilience capacity the most, since this study shows that this victimization is the only one in which resilience does not have any modulatory effect and, therefore, in which the worst levels of psychological HRQoL are observed.
In sum, these findings highlight the need of urgent effort into avoiding peer victimization in any of its forms, since all types of peer violence negatively impact adolescents’ HRQoL related to psychological domains. Previous research have shown that secondary schools are ideal settings for developing prevention programs aimed to reducing violence between peers 55, since they give the opportunity to interact directly with them in a practical way by role-playing, games, or any other activity that allows to work on avoiding violence in a stimulating way. On the other hand, results also suggest the importance of establishing surveillance programmes at schools to early detect teenagers who are experiencing violence. In this way, adolescent victims, whose personal strengths to manage disruptive relationships are exhausted, could be helped to strengthening their resources for better coping with undesirable life situations and, thus, minimize negative outcomes on their health. Previous studies have demonstrated strategies to reinforce personal strengths at secondary schools56.
The results of this study suggest that resilience could function as a protective factor that weakly regulates the negative association between physical and verbal victimization and the “Mood and Emotions” domain of adolescents’ HRQoL, however, we cannot know whether resilience has a stronger protective capacity on other components of the emotional well-being and health of victimized adolescents. For this reason, more research is needed to further investigate resilience trajectories in the context of peer victimization and its potential protective capacity over undesirable adolescents’ health outcomes.
Sociodemographic factors did not play a significant role between adolescents’ resilience levels in this research. Although other authors suggested that resilience may differ according to different cultural contexts29,57, this study is in line with those concluding that resilience is a process of adaptation28 and it is necessary to take into account previously accumulated adverse events to understand it58, being independent from the socio-demographic factors associated with an individual.
Strengths and limitations
Potential limitations should be considered when interpreting the results. First, our findings must be interpreted in a specific socio-cultural context in which the investigation took place, so we cannot generalize the results to other regions. Although one third of the total participants were non-Spanish, further studies would be desirable to collect evidence from other regions or countries since results cannot be generalised to other populations. Second, it is not possible to make causal inferences because of the cross-sectional nature of the study. Future prospective investigations are recommended to clarify resilience behaviour in the context of peer victimization. Furthermore, due to the cross-sectional nature of this research levels of adolescents’ HRQoL could only be analysed at the time of data collection. Therefore, we can’t know how was their quality of life before being victimized. Third, the information was obtained from self-administered questionnaires so the possibility of recall bias cannot be rule out. Cross-checking adolescents' information by different sources would be desirable in future studies. Fourth, the quality of life construct has been partially measured, referring only to two of the KIDSCREEN dimensions (“Psychological Well-being” and “Mood and Emotions), which was considered to be the most relevant in our study. For this reason, we cannot affirm that the dependent variable was the “quality of life” during school age, but rather a partial aspect of it (the psychological components). However, according to the results of CFA these components of the quality of life seems to have its own entity by showing a good fit to the sample data. In addition, Internal consistency of both dimensions was also adequate. Finally, cyberbullying, a type of victimization that is becoming increasingly important, was not analysed. This may explain the lower prevalence of victimization in our study compared to others7,8 which have shown higher rates of this phenomenon. Future investigation should consider studying possible associations between resilience, cyberbullying and HRQoL’s psychological domains in order to compare outcomes with those from research that only focuses on traditional forms of peer victimization.
Notwithstanding these limitations, strengths of this study include the large sample size in conjunction with the significant participation rate (90.8%). The use of widely accepted questionnaires with scores that are valid and reliable in this study sample should also be taken into account. An interesting strength is also the separate analyses of the three most important types of peer victimization rather than the measurement of victimization as a whole.
Conclusions
The results of this study suggest that resilience could function as a protective factor that weakly regulates the negative association between physical and verbal victimization and the “Mood and Emotions” domain of adolescents’ HRQoL. Therefore, future research directions should focus on exploring other protective factors that could stronger minimize the devastating consequences that peer victimization has on the psychological sphere of adolescents’ HRQoL. Thus, specific intervention programmes could be implemented to build and reinforce these strengths in victimized adolescents. Likewise, more research is needed to further investigate resilience trajectories in the context of peer victimization and its potential protective capacity over undesirable adolescents’ health outcomes.
Data availability
ll data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Kochenderfer, B. J. & Ladd, G. W. Peer victimization: Cause or consequence of school maladjustment?. Child Dev. 67, 1305–1317 (1996).
Kowalski, R. M. & Limber, S. P. Psychological, physical, and academic correlates of cyberbullying and traditional bullying. J. Adolesc. Heal. 53, S13–S20 (2013).
Zarate-Garza, P. P. et al. How well do we understand the long-term health implications of childhood bullying?. Harv. Rev. Psychiatry 25, 89–95 (2017).
Kowalski, R. M., Giumetti, G. W., Schroeder, A. N. & Lattanner, M. R. Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychol. Bull. 140, 1073–1137 (2014).
Currie, C. et al. Social determinants of health and well-being among young people : Health Behaviour in School-Aged Children (HBSC) study : International report from the 2009/2010 survey (Health Policy for Children and Adolescents, No. 6). in (ed. WHO Regional Office for Europe) doi:https://doi.org/10.1358/dof.2005.030.10.942816.
García, S. I. & Ochotorena, J. D. P. Lifetime victimization among Spanish adolescents. Psicothema 29, 378–383 (2017).
Pereda, N., Guilera, G. & Abad, J. Victimization and polyvictimization of Spanish children and youth: Results from a community sample. Child Abus. Negl. 38, 640–649 (2014).
Caravaca Sánchez, F. et al. Prevalence and patterns of traditional bullying victimization and cyber-teasing among college population in Spain. BMC Public Health 16, 176 (2016).
Waasdorp, T. E. & Bradshaw, C. P. The overlap between cyberbullying and traditional bullying. J. Adolesc. Heal. 56, 483–488 (2015).
Ferrara, P., Ianniello, F., Villani, A. & Corsello, G. Cyberbullying a modern form of bullying: Let’s talk about this health and social problem. Ital. J. Pediatr. 44, 14 (2018).
Kennedy, R. S. Bullying trends in the United States: A meta-regression. Trauma Violence Abus. 22, 914–927 (2021).
Chen, Y. Y. & Huang, J. H. Precollege and in-college bullying experiences and health-related quality of life among college students. Pediatrics 135, 18–25 (2015).
Juvonen, J. & Graham, S. Bullying in schools: The power of bullies and the plight of victims. Annu. Rev. Psychol. 65, 159–185 (2014).
Pellegrini, A. D., Bartini, M. & Brooks, F. School bullies, victims, and aggressive victims: Factors relating to group affiliation and victimization in early adolescence. J. Educ. Psychol. 91, 216–224 (1999).
Le, H. T. H. et al. Longitudinal associations between bullying and mental health among adolescents in Vietnam. Int. J. Public Health 62, S51–S61 (2017).
Gini, G. & Pozzoli, T. Association between bullying and psychosomatic problems: A meta-analysis. Pediatrics 123, 1059–1065 (2009).
Arslan, G., Allen, K. A. & Tanhan, A. School bullying, mental health, and wellbeing in adolescents: Mediating impact of positive psychological orientations. Child Indic. Res. https://doi.org/10.1007/s12187-020-09780-2 (2020).
Ravens-Sieberer, U., Erhart, M., Wille, N. & Bullinger, M. Health-related quality of life in children and adolescents in Germany: Results of the BELLA study. Eur. Child Adolesc. Psychiatry 17, 148–156 (2008).
González-Cabrera, J., Machimbarrena, J. M., Ortega-Barón, J. & Álvarez-Bardón, A. Joint association of bullying and cyberbullying in health-related quality of life in a sample of adolescents. Qual. Life Res. 29, 941–952 (2020).
Hamby, S., Taylor, E., Mitchell, K., Jones, L. & Newlin, C. Health-related quality of life among adolescents as a function of victimization, other adversities, and strengths. J. Pediatr. Nurs. 50, 46–53 (2020).
Albaladejo-Blázquez, N. et al. Health-related quality of life and mental health of adolescents involved in school bullying and homophobic verbal content bullying. Int. J. Environ. Res. Public Health 16, 2622 (2019).
Kadiroğlu, T., Hendekci, A. & Tosun, Ö. Investigation of the relationship between peer victimization and quality of life in school-age adolescents. Arch. Psychiatr. Nurs. 32, 850–854 (2018).
Martín-Pérez, Á. de L. & Gascón-Cánovas, J. J. The impact of the magnitude of the group of bullies on health-related quality of life and academic performance among adolescents. Child Psychiatry Hum. Dev. (2021) https://doi.org/10.1007/s10578-021-01290-8.
Rutter, M. Resilience as a dynamic concept. Dev. Psychopathol. 24, 335–344 (2012).
Feeney, B. C. & Collins, N. L. New look at social support: A Theoretical perspective on thriving through relationships. Personality Soc. Psychol. Rev. 19 (2015).
Singham, T. et al. Concurrent and longitudinal contribution of exposure to bullying in childhood to mental health: The Role of vulnerability and resilience. JAMA Psychiat. 74, 1112–1119 (2017).
Segura, A., Pereda, N., Guilera, G. & Hamby, S. Resilience and psychopathology among victimized youth in residential care. Child Abus. Negl. 72, 301–311 (2017).
Lee, J. H. et al. Resilience: A meta-analytic approach. J. Couns. Dev. 91, 269–279 (2013).
Masten, A. S. Global perspectives on resilience in children and youth. Child Dev. 85, 6–20 (2014).
Víllora, B., Larrañaga, E., Yubero, S., Alfaro, A. & Navarro, R. Relations among poly-bullying victimization, subjective well-being and resilience in a sample of late adolescents. Int. J. Environ. Res. Public Health 17, 590 (2020).
Brighi, A. et al. Coping with cybervictimization: The role of direct confrontation and resilience on adolescent wellbeing. Int. J. Environ. Res. Public Health 16, 4893 (2019).
Hinduja, S. & Patchin, J. W. Cultivating youth resilience to prevent bullying and cyberbullying victimization. Child Abus. Negl. 73, 51–62 (2017).
Zhou, Z. K., Liu, Q. Q., Niu, G. F., Sun, X. J. & Fan, C. Y. Bullying victimization and depression in Chinese children: A moderated mediation model of resilience and mindfulness. Pers. Individ. Dif. 104, 137–142 (2017).
Domingo-Salvany, A. et al. Propuestas de clase social neoweberiana y neomarxista a partir de la Clasificación Nacional de Ocupaciones 2011. Gac. Sanit. 27, 263–272 (2013).
Hamburger, M. E., Basile, K. C. & Vivolo, A. M. Measuring Bullying Victimization,Perpetration and Bystander Experiences : A Compendium of Assessment Tools. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control (Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, 2011).
Gascón-Cánovas, J. J., Russo de Leon, J. R., Cózar Fernandez, A. & Heredia Calzado, J. M. Cultural adaptation to Spanish and assessment of an adolescent peer relationships tool for detecting school bullying: Preliminary study of the psychometric properties. An. Pediatr. 87, 9–17 (2017).
Ravens-Sieberer, U. et al. The KIDSCREEN-52 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Value Heal. 11, 645–658 (2008).
The KIDSCREEN Group Europe. The KIDSCREEN questionnaires: Quality of life questionnaires for children and adolescents. Pabst Science Publishers (Pabst, 2006). doi:https://doi.org/10.1017/CBO9781107415324.004.
Sinclair, V. G. & Wallston, K. A. The development and psychometric evaluation of the brief resilient coping scale. Assessment 11, 94–101 (2004).
López-Pina, J. A. et al. Measurement properties of the brief resilient coping scale in patients with systemic lupus erythematosus using rasch analysis. Health Qual. Life Outcomes 14, 128 (2016).
Rosner, B. Multisample Inference. Fundam. Biostat. 516–587 (2011).
Ahad, N. A., Soaad, S. & Yahaya, S. Sensitivity analysis of Welch’s t-test. AIP Conf. Proc. 1605, 888–893 (2014).
Lee, S. & Lee, D. K. What is the proper way to apply the multiple comparison test?. Korean J. Anesth. 71, 353–360 (2018).
Williams, L. J. & Abdi, H. Fisher’s Least Significant Difference (LSD) Test. in Encyclopedia of Research Design (ed. Salkind, N. J.) (SAGE, 2010). doi:https://doi.org/10.4135/9781412961288.
Rosner, B. Regression and Correlation Methods. In Fundamentals of biostatistics 427–515 (Brooks/Cole, Cengage Learning, 2011).
Hayes, A. F. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. J. Educ. Meas. 51, 335–337 (2013).
Tranmer, M., Murphy, J., Elliot, M. & Pampaka, M. Multiple Linear Regression (2 nd Edition). Cathie Marsh Inst. Work. Pap. 2020–01 (2020).
Brown, T. A. Confirmatory Factor Analysis for Applied Research. (Guilford Press, 2006).
Satorra, A. & Bentler, P. M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent variables analysis: Applications for developmental research. 399–419 (Sage, Inc, 1994).
Hu, L. & Bentler, P. M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 6, 1–55 (1999).
Viladrich, C., Angulo-Brunet, A. & Doval, E. A journey around alpha and omega to estimate internal consistency reliability. An. Psicol. 33, 755–782 (2017).
Hair, J. F., Sarstedt, M., Ringle, C. M. & Mena, J. A. An assessment of the use of partial least squares structural equation modeling in marketing research. J. Acad. Mark. Sci. 40, 414–433 (2012).
Simón-Saiz, M. J. et al. Influencia de la resiliencia sobre la calidad de vida relacionada con la salud en adolescentes. Enferm. Clin. 28, 283–291 (2018).
Gonzalez-Mendez, R., Ramírez-Santana, G. & Hamby, S. Analyzing Spanish adolescents through the lens of the resilience portfolio model. J. Interpers. Violence https://doi.org/10.1177/0886260518790600 (2018).
Costantino, C. et al. Effects of an intervention to prevent the bullying in first-grade secondary schools of Palermo, Italy: The BIAS study. Ital. J. Pediatr. 45, 65 (2019).
Andermo, S. et al. School-related physical activity interventions and mental health among children: A systematic review and meta-analysis. Sport. Med. Open 6, 25 (2020).
Ungar, M. Resilience, trauma, context, and culture. Trauma Violence Abus. 14, 255–266 (2013).
Grych, J., Hamby, S. & Banyard, V. The resilience portfolio model: Understanding healthy adaptation in victims of violence. Psychol. Violence 5, 343–354 (2015).
Acknowledgements
The authors would like to thank the Department of Health and Secondary Schools from the city of Torre Pacheco which participated in this study. Thanks to Lourdes Sánchez Fernández for having collaborated in the revision of English grammar.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception, design, material preparation, data collection, analysis and writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martín-Pérez, Á., Morán-Sánchez, I. & Gascón-Cánovas, J.J. The impact of resilience as a protective factor on Health-Related Quality of Life’s psychological dimensions among adolescents who experience peer victimization. Sci Rep 12, 18898 (2022). https://doi.org/10.1038/s41598-022-23424-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23424-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
