
Abstract
Diet and lifestyle as modifiable factors play an effective role in muscle strength and muscle endurance. In addition, inflammatory reactions may have an association with the etiology of a a lower muscle strength and muscle endurance. We aimed to investigate the association of dietary and lifestyle inflammation scores (DLIS) with muscle strength and muscle endurance in a sample of Iranian adults. In this cross-sectional study, 270 adults aged 20 to 59 years (55.9% female) were selected. The dietary intakes were collected using a 168-item semi-quantitative food frequency questionnaire. The DLIS was calculated using the dietary inflammatory score (DIS), and lifestyle inflammatory score (LIS). Muscle endurance and muscle strength were measured by a digital-handgrip-dynamometer. Multivariate adjusted means for muscle strength and endurance across quartiles of the DIS, LIS, and DLIS were determined by the ANCOVA test. Multiple linear regression analysis was used to evaluate the association between inflammation scores (i.e., DIS, LIS, and DLIS), and muscle strength, muscle endurance. The DLIS ranged between −2.94 and 3.09. The adjusted P-value of muscle strength of the right hand (MSR) along quartiles of DIS was significantly lower (P = 0.024). MSR (β: −1.19; P-value: 0.020) and mean muscle strength (MMS) (β: −0.95; P-value: 0.047) had significant association with DIS. MSR (β: −0.85; P-value: 0.050) had a marginally significant association with DLIS. Overall, we found that a high adherence to a pro-inflammatory diet might be associated to a lower muscle strength. However, a lifestyle with greater inflammatory potential was not related to any components of muscle endurance. Further studies with prospective designs are needed to confirm the present findings in further details.
Similar content being viewed by others

Introduction
Skeletal muscle mass plays an essential role in the strength, function, and regulation of metabolism1. Muscle strength and endurance are two separate characteristics of muscle mass2. Muscle strength as the ability to produce the most force3 is an important tool for assessing nutritional status and a valid indicator of muscle quality and function4,5. Muscular endurance as a major part of muscle function6 refers to the ability to exert and maintain a continuous force over time2. Reduction of muscle strength and endurance can be associated with chronic diseases such as obstructive pulmonary disease, heart disease7,8,9, insulin resistance10, and metabolic syndrome11. Moreover, assessing muscular endurance along with muscular strength can provide practical information about the ability to perform normal daily activities12.
Numerous factors such as genetics13, lifestyle habits such as physical activity14, alcohol consumption15, abdominal obesity16, smoking17; and dietary patterns18, can affect muscle mass. It is proposed that inflammation may mediate the association between the aforementioned factors and muscle mass status19,20. To determine the inflammatory potential of the total food intake, the Dietary Inflammation Index (DII) has been designed and validated21. However, DII has some limitations and has no indication of the lifestyle21.
In a recent study, the use of dietary and lifestyle inflammation scores (DLIS) was validated and recommended22. The DLIS contains the dietary inflammation score (DIS) including 19 dietary components, and four components forming the lifestyle inflammation score (LIS): cigarette smoking, physical activity, alcohol drinking, and obesity22. Therefore, DLIS can present a relatively comprehensive view of the effects of modifiable factors (diet and lifestyle) on inflammatory status.
Some previous studies have reported that higher dietary and lifestyle inflammatory scores are associated with an increased risk of chronic diseases such as cancer- and cardiovascular disease23,24, metabolic syndrome25, and insulin-related disorders26. However, only a few studies showed that a higher DII score can be associated with reduced muscle mass27, muscle strength and endurance28, and muscle function29. To the best of our knowledge, no prior study has assessed the association between LIS ( with its four components) and muscle strength and endurance. In addition, to the best of our knowledge, no prior work in the Middle East has investigated the relationship between DLIS with muscle strength and muscle endurance. In this study, for the first time, we aimed to investigate the association between DLIS and muscle strength and muscle endurance in Tehranian adults.
Materials and methods
Study population selection
In this cross-sectional study, adults were selected from the residents of Tehran (118 males and 152 females). The sample size based on the correlation coefficient can be calculated as the following:30,31
where, the calculated correlation coefficient between pro-inflammatory diets and muscle strength in previous study has been determined as r = 0.37 (the observed correlation)30,31. We set the error type 1, α = 5%, and the statistical power, 1-β = 95%, resulting in N = 135. However, due to possible decline in the number of participants, 271 subjects were recruited in this study.
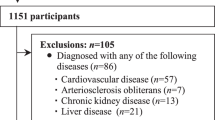
Participants were recruited using advertisements, from February 2018 to July 2019. Inclusion criteria were individuals aged 20 to 59 years old. Exclusion criteria were (i) drug addiction, (ii) having special diets, e.g., weight loss diets and weight gain diets (as they cannot properly represent of the target population), (iii) having acute or chronic diseases which may change the diet routine, (iv) pregnant and lactating women, (v) taking hormone-specific medications, sedatives, supplements, and (vi) any conditions that limit exercise testing (some diseases such as atopy, stroke, asthma, or any other condition that can influence exercise testing). All participants signed informed written consent. The informed consent form and protocol were approved by the ethical standards of the Tehran University of Medical Sciences (ethical number: IR.TUMS.VCR.REC.1397.157).
Exposures and outcomes
Demographic factors
Trained interviewers obtained information about age, gender, education (illiterate, under diploma, diploma, or educated), marriage status (single, married, or divorced), smoking status (never smoker, former smoker, light smoker, or heavy smoker), and occupation (employee, housekeeper, retired, or unemployed). We categorized the smoking status into two groups: “smokers” including current smokers or “non-smokers” including former smokers /never.
Physical activity
We assessed the physical activity through the validated International Physical Activity Questionnaire (IPAQ)32. The obtained data was expressed as a metabolic equivalent minute per week (MET- minute /week)33 and accordingly, participants were categorized into three groups: very low (< 600 MET-minute/week), low (600–3000 MET-minute/week), and moderate and high physical activity (> 3000 MET-minute/week)34.
Dietary assessment and calculating the dietary and lifestyle inflammation scores (DLIS)
Using a semi-quantitative food frequency questionnaire, the average food intake in the past year for each participant was obtained35. This 168-item questionnaire contained a list of groceries with the standard portion size of each food item. The frequency of consumption for each item was recorded for each subject separately. Utilizing household measures, the portion sizes were converted to grams per day. The questionnaire data was entered into Nutritionist IV software based on the Iranian foods-modified version of the US Department of Agriculture food composition database36, and subsequently, we obtained the amount of food intake.
The method introduced by Byrd et al. was used to calculate the DLIS for each participant22. The score includes dietary inflammation score (DIS) and lifestyle inflammation score (LIS). The DIS and LIS were calculated as follows. Subsequently, to calculate the DLIS; DIS and LIS for each participant were summed. A higher DLIS indicates a more pro-inflammatory diet and lifestyle.
Calculating the dietary inflammation score (DIS)
The DIS includes 19 dietary components including leafy greens and cruciferous vegetables, tomatoes, apples and berries, deep yellow or orange vegetables and fruit, other fruits and real fruit juices, other vegetables, legumes, fish, poultry, red and organ meats, processed meats, added sugars, high-fat dairy, low-fat dairy, coffee and tea, nuts and other fats, refined grains and starchy vegetables and supplement score22. Of these, the supplement score was removed due to a lack of relevant information. To calculate the weight of each component in the DIS, each dietary component was treated as a continuous variable (g/d) and then was standardized by gender, to a mean of 0 and SD of 1.0. Next, each dietary component was scored based on the strength of its association with an inflammation biomarker score in the REGARDS case cohort study. Multivariable linear regression was used to estimate the maximum likelihood estimates for the β-coefficients, which represent the average change in the inflammation biomarker score per 1 SD increase in a dietary component. Each dietary component intake was multiplied by the weight (β-coefficient) and then all were summed to calculate the DIS.
Calculating the lifestyle inflammation score (LIS)
The LIS includes four components: smoking status, physical activity, alcohol intake, and obesity. We categorized the smoking status into two groups: “current smoker” or “former smoker /never.” Physical activity was divided into two groups of “high or moderate” or “low or no physical activity”. Obesity was characterized by BMI (kg/m2) [overweight (25–29.99), or obese (≥ 30)]. Alcohol intake was eliminated due to a lack of information regarding alcohol drinking in the Iranian population. For the LIS, dummy variables were created for physical activity and smoking status, and then multivariable linear regression was applied to estimate the β coefficients to represent the average change in the inflammation biomarker score per having a certain lifestyle behavior relative to its referent category. To calculate the DLIS, the DIS and LIS for each participant were summed. Higher DLIS indicates a more pro-inflammatory diet and lifestyle.
Anthropometric measurements
The weight, height, waist (WC), and hip circumference (HP) of the study participants were measured by trained dietitians. Subjects were weighted with slight clothing, by an adult’s digital scale (808Seca, Germany) with 0.1 kg sensitivity. The subject’s height was metered using a wall stadiometer with 0.1 cm precision, barefoot with relaxing shoulders (Seca, Germany). Using an anthropometric tape, WC was measured in the middle between the iliac crest and the lower rib margin. The HC was measured by the static tape in the correct horizontal position at the extreme level from the sidelong facet over light clothing, without any force to the body surface with 0.1 cm accuracy. The BMI was calculated as weight in kg divided by height in meters squared. The waist-to-hip ratio (WHR) was calculated by dividing the WC by HP (in centimeters).
Definition of muscle strength and muscle endurance
Muscle strength and endurance tests were done under the controlled condition: in the laboratory at normal room temperature (23–25 °C), between 8:30–11:30 A.M.37. Measures were obtained with a digital handgrip Dynamometer (Saehan, Model SH5003; Saehan Corporation, Masan, South Korea). The validity and reliability of using this instrument have been confirmed38. Muscle strength was measured in a standing position while their arms dangling normally on the side of the body and the angle of the elbow was near 180°, subjects were asked to press the handle of the dynamometer as much as possible for measuring the extreme strength for each hand. This method was repeated three times for each hand, entirely six times muscle strength was determined; then in data analysis, a mean of three measurements was applied39. For determining muscle endurance participants were asked to continue 1/3rd of maximal deliberate contraction on the condition that he/she could while using a halt watch, the time was recorded40.
Statistical methods
We performed the statistical analyses using the Statistical Package for the Social Sciences (SPSS version 25; SPSS Inc). P-value < 0.05 was considered as a statistical significance level. Participants were evaluated in quartiles of the DLIS. Quantitative variables were reported as mean and standard deviation (SD) and qualitative variables as frequency (percent). The Chi-square test was applied to compare the frequency of qualitative variables across the DLIS quartiles and the Analysis of Variance (ANOVA) was used to compare the means of quantitative variables. Values of daily food consumption across the DLIS quartiles were adjusted for age, sex, energy intake, marriage status, occupation, and education using an analysis of covariance (ANCOVA). Multivariate adjusted means for muscle strength and endurance across quartile of the dietary and lifestyle inflammation scores for the participants were determined through the ANCOVA test, which was adjusted for sex, age, energy intake, marriage status, occupation, and education status. Multiple linear regression analysis was used to evaluate the association between DIS, LIS, DLIS and muscle strength and endurance. We performed this association analysis before and after adjustment for age, sex, energy intake, marriage status, occupation, and education status. For the association of DIS and outcomes, further adjustments for body mass index, physical activity, and smoking status were done.
Ethical approval and consent to participate
The ethical committee approved the present study of Tehran University of Medical Sciences (ethical number: IR.TUMS.VCR.REC.1397.157). All participants filled out informed consent at the beginning of the study.
Human and animal rights
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the ethics committee of Tehran University of Medical Sciences. Written informed consent was obtained from all subjects/patients.
Results
Of the initial 271 participants enrolled in the study, eight participants were removed due to insufficient data for one of the variables, which yielded 263 participants (55.9% female) for the present study. The mean ± SD of age and BMI of participants were 36.8 ± 13.2 years and 25.6 ± 4.6 kg/m2, respectively. The inflammatory scores: DIS, LIS, and DLIS were ranged from −3.02 to 1.55 (mean ± SD: −0.50 ± 0.90), −0.41 to 2.07 (mean ± SD: −0.43 ± 0.64), and −2.94 to 3.09 (mean ± SD: −0.08 ± 1.11), respectively. The mean ± SD of mean muscle strength and mean muscle endurance of subjects was 30.9 ± 11.7 kg and 123 ± 67.0 s, respectively. Characteristics of the study participants across quartiles of the DLIS are presented in Table 1. The proportion of married persons increased significantly in the top quartile of the DLIS compared with the lowest quartile, but the percentage of university-graduated persons decreased significantly across the quartiles of the DLIS. Values of age, weight, BMI, WC, WHR, body fat, FM, and FFM increased in the top quartile of the DLIS compared with the lowest quartile.
The dietary intakes of participants according to quartiles of the DLIS are indicated in Table 2. By the ANCOVA test, energy intake is adjusted for age and sex, and all other values for age, sex, and energy intake are adjusted. The intake of added sugar, and refined grains increased significantly along with an increase in the DLIS. In contrast, intakes of fiber, tomatoes, apples and berries, deep yellow or orange vegetables and fruit, other fruits and real fruit juices, other vegetables, and nuts decreased proportionally across quartiles of the DLIS.
Multivariate adjusted means for muscle strength and endurance across quartiles of the DIS, LIS, and DLIS for the participants, separately, are presented in Table 3. By the ANCOVA test, potential confounders including age, sex, energy intake, marriage status, occupation, and education status were adjusted. DIS was adjusted further for body mass index, physical activity, and smoking status. The results showed that the mean of MSR in the highest quartile of the DIS was significantly lower compared to the lowest quartile, (P = 0.024). Across the quartiles of LIS and DLIS, we did not observe any differences in the values of muscle strength and muscle endurance components.
Results of multiple linear regression on the association of dietary inflammation score (DIS), lifestyle inflammation score (LIS), and dietary and lifestyle inflammation score (DLIS) with muscle strength and muscle endurance are presented in Table 4. The results showed that DIS had a significant association with MSR (β: −1.19; P-value: 0.020) and mean muscle strength (MMS) (β: −0.95; P-value: 0.047). After further adjustment for body mass index, physical activity, and smoking status, the association of DIS and MSR remained significant (β: −1.19; P-value: 0.023). Also, DLIS had a marginally significant association with MSR (β: −0.85; P-value: 0.050) that was disappeared after adjustment for confounders in model 2 (P = 0.092). We did not observe any significant association between LIS and any components of muscle strength and muscle endurance.
Discussion
This cross-sectional study examined the association between inflammation score based on diet and lifestyle with muscle strength and muscle endurance in Tehranian adults. We observed a significant inverse association between DIS and the MSR and MMS. Also, a higher adherence to DLIS was inversely related to the MSR. To the best of our knowledge, this is the first study that examined the relation between DLIS with muscle strength and muscle endurance in the Middle East.
Our results suggest a significant inverse association between pro-inflammatory diet and the MSR and the MMS. This result may be obtained by decreasing the consumption of fruit and vegetables across the quartiles of DIS and increasing the consumption of added sugar, and refined grains along with the quartiles of DIS. A previous study indicates that dietary patterns with high intakes of fruits and vegetables are related to a lower risk of frailty41. A prospective study reported that consumption of added sugars had a direct relation with frailty42. In addition,, dietary patterns characterized by high consumption of refined grains had a direct relation with several frailty components43. In a previous study, the dietary patterns containing a high amount of red/processed meat and butter were associated with a lower muscle strength. However, in contrast, the dietary patterns rich in fruits, fish/seafood, eggs, nuts, and whole grains containing a lower amount of red/processed meats and potatoes can increase muscle strength44.
In this study, we did not notice any significant association between the LIS and any components of muscle strength and muscle endurance. A study on a healthy population showed that among lifestyle components only physical activity in freedom times has a positive association with muscle strength45. Although, evidence showed smoking has an inverse association with muscle strength too17 because smoking impairs the muscle protein synthesis process, and decreasing muscular fiber also boosts expression of myostatin and muscle atrophy F-box46. A longitudinal study showed abdominal obesity, no general obesity has an association with augmenting muscle strength decline in men16. Because abdominal obesity more than general obesity can reflect inflammatory activity47 which leads to a reduction in muscle strength48. While a study reported that general obesity can increase the decline in hand muscle strength49. However, we did not observe a significant association between LIS and any components of muscle strength and endurance, which may be obtained by excluding subjects with any comorbidities that can be in connection with their lifestyle.
We showed that DLIS had an inverse association with MSR. In line with our results, a longitudinal study indicated higher DII scores had been associated with a higher incidence of frailty, particularly in men29. A cross-sectional study presented that a higher DII scores had a relation to greater odds of sarcopenia50. Few studies51,52 indicated that the Mediterranean dietary pattern which has components for decreasing systemic inflammation53 may reduce the risk of sarcopenia. In contrast with our results, a cross-sectional study on children indicated no significant relationship between DII and handgrip strength54. Also, a prospective study indicated no relation between higher DII scores and lower handgrip strength27. However, evidence shows that by increasing inflammatory cytokines such as CRP, IL-6, and TNF-a; muscle mass, muscle strength, and physical performance decreased27. Inflammatory cytokines declined anabolic factors such as insulin and insulin-like growth factor (IGF-1) can down-regulate muscle protein synthesis55. Therefore, a high intake of dietary factors with anti-inflammatory properties may have beneficial effects on muscle strength and muscle endurance.
In this study, we indicated that by increasing DIS, right-hand muscle strength decreased. But did not observe a similar association in the left hand. Because continuous use of the right-hand changes its fiber composition and results in different neuromuscular properties of the right-hand muscle in comparison with the left one56.
Strengths of this study are: all measurements were accurate because the collection of the information was done by expert dietitians, using valid and reliable questionnaires and cut-offs; and using a new index that considers important inflammation-related lifestyle components to estimate the joint inflammatory properties of the diet and lifestyle.
However, our study has some limitations that must be considered in interpreting the results. Because of the cross-sectional study design, the temporal sequence and causal relationship could not be determined. In addition, similar to any other cross-sectional study, the present investigation is also susceptible to possible biases such as the recall bias as well as the selection bias. Therefore, further studies with prospective designs in this field are necessary. Moreover, in this study, 18 dietary parameters out of 19 parameters were available for calculating the DIS, and the missing supplementary score. Also, from four lifestyle items to calculate the LIS, one factor (Alcohol-intake) was not considered. The error of measurement and wrong classification of participants cannot be separated from the study. Despite adjusting several distortions in this study, the potential effects of the remaining confounders were uncontrollable.
Conclusions
Overall, we found that a high adherence to a pro-inflammatory diet might be associated to a lower muscle strength. However, lifestyles with greater inflammatory potentials was not related any components of muscle endurance. Further studies with prospective designs are needed to confirm the present findings in further details.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Paddon-Jones, D. & Rasmussen, B. B. Dietary protein recommendations and the prevention of sarcopenia: Protein, amino acid metabolism and therapy. Curr. Opin. Clin. Nutr. Metab. Care 12, 86 (2009).
Nicolay, C. W. & Walker, A. L. Grip strength and endurance: Influences of anthropometric variation, hand dominance, and gender. Int. J. Ind. Ergon. 35, 605–618 (2005).
Gaines, J. M. & Talbot, L. A. Isokinetic strength testing in research and practice. Biol. Res. Nurs. 1, 57–64 (1999).
Prista, A., Maia, J. A. R., Damasceno, A. & Beunen, G. Anthropometric indicators of nutritional status: Implications for fitness, activity, and health in school-age children and adolescents from Maputo, Mozambique. Am. J. Clin. Nutr. 77, 952–959 (2003).
Norman, K., Stobäus, N., Gonzalez, M. C., Schulzke, J.-D. & Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 30, 135–142 (2011).
White, C., Dixon, K., Samuel, D. & Stokes, M. Handgrip and quadriceps muscle endurance testing in young adults. Springerplus 2, 1–8 (2013).
Mancini, D. M. et al. Contribution of skeletal muscle atrophy to exercise intolerance and altered muscle metabolism in heart failure. Circulation 85, 1364–1373 (1992).
Janaudis-Ferreira, T., Wadell, K., Sundelin, G. & Lindström, B. Thigh muscle strength and endurance in patients with COPD compared with healthy controls. Respir. Med. 100, 1451–1457 (2006).
Artero, E. G. et al. Effects of muscular strength on cardiovascular risk factors and prognosis. J. Cardiopulm. Rehabil. Prev. 32, 351 (2012).
Jiménez-Pavón, D. et al. Muscular strength and markers of insulin resistance in European adolescents: The HELENA Study. Eur. J. Appl. Physiol. 112, 2455–2465 (2012).
Jurca, R. et al. Association of muscular strength with incidence of metabolic syndrome in men. Med. Sci. Sports Exerc. 37, 1849 (2005).
Bemben, M. G. Age-related alterations in muscular endurance. Sports Med. 25, 259–269 (1998).
Thomas, D. R. Sarcopenia. Clin. Geriatr. Med. 26, 331–346 (2010).
Chen, H.-T., Wu, H.-J., Chen, Y.-J., Ho, S.-Y. & Chung, Y.-C. Effects of 8-week kettlebell training on body composition, muscle strength, pulmonary function, and chronic low-grade inflammation in elderly women with sarcopenia. Exp. Gerontol. 112, 112–118 (2018).
Thapaliya, S. et al. Alcohol-induced autophagy contributes to loss in skeletal muscle mass. Autophagy 10, 677–690 (2014).
de Carvalho, D. H. T., Scholes, S., Santos, J. L. F., de Oliveira, C. & Alexandre, T. S. Does abdominal obesity accelerate muscle strength decline in older adults? Evidence from the English Longitudinal Study of Ageing. J. Gerontol. Ser. A 74, 1105–1111 (2019).
Saito, T. et al. Relationship between cigarette smoking and muscle strength in Japanese men. J. Prev. Med. Public Health 45, 381 (2012).
Wu, F. et al. Associations of dietary patterns with bone mass, muscle strength and balance in a cohort of Australian middle-aged women. Br. J. Nutr. 118, 598–606 (2017).
Wang, J., Leung, K.-S., Chow, S.K.-H. & Cheung, W.-H. Inflammation and age-associated skeletal muscle deterioration (sarcopaenia). Journal of Orthopaedic Translation 10, 94–101 (2017).
Pankow, J. S. et al. Familial and genetic determinants of systemic markers of inflammation: The NHLBI family heart study. Atherosclerosis 154, 681–689 (2001).
Shivappa, N., Steck, S. E., Hurley, T. G., Hussey, J. R. & Hébert, J. R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 17, 1689–1696 (2014).
Byrd, D. A. et al. Development and validation of novel dietary and lifestyle inflammation scores. J. Nutr. 149, 2206–2218 (2019).
Byrd, D., Holmes, A., Judd, S., Flanders, W. D. & Bostick, R. M. Associations of whole food and lifestyle-based inflammation scores with all-cause, cancer-and cardiovascular disease-specific mortality. Can. Res. 77, 3287–3287 (2017).
Byrd, D. A. et al. Associations of novel dietary and lifestyle inflammation scores with incident colorectal cancer in the NIH-AARP Diet and Health Study. JNCI Cancer Spectrum 4, pkaa009 (2020).
Farhadnejad, H., Parastouei, K., Rostami, H., Mirmiran, P. & Azizi, F. Dietary and lifestyle inflammatory scores are associated with increased risk of metabolic syndrome in Iranian adults. Diabetol. Metab. Syndr. 13, 1–10 (2021).
Farhadnejad, H., Teymoori, F., Mokhtari, E., Mirmiran, P. & Azizi, F. Higher scores of dietary and lifestyle inflammatory indices are associated with increased risk of insulin-related disorders in Iranian adults. Eur. J. Clin. Nutr. https://doi.org/10.1038/s41430-022-01143-0 (2022).
Cervo, M. M. et al. Longitudinal associations between dietary inflammatory index and musculoskeletal health in community-dwelling older adults. Clin. Nutr. 39, 516–523 (2020).
Shahinfar, H. et al. The association between dietary inflammatory index, muscle strength, muscle endurance, and body composition in Iranian adults. Eat. Weight Disord. 27, 463–472 (2022).
Shivappa, N. et al. The relationship between the dietary inflammatory index and incident frailty: A longitudinal cohort study. J. Am. Med. Dir. Assoc. 19, 77–82 (2018).
Ng, A. K., Hairi, N. N., Jalaludin, M. Y. & Majid, H. A. Dietary intake, physical activity and muscle strength among adolescents: The Malaysian Health and Adolescents Longitudinal Research Team (MyHeART) study. BMJ Open 9, e026275 (2019).
Scott, D., Blizzard, L., Fell, J., Giles, G. & Jones, G. Associations between dietary nutrient intake and muscle mass and strength in community-dwelling older adults: The Tasmanian Older Adult Cohort study. J. Am. Geriatr. Soc. 58, 2129–2134 (2010).
Moghaddam, M. B. et al. The Iranian Version of International Physical Activity Questionnaire (IPAQ) in Iran: Content and construct validity, factor structure, internal consistency and stability. World Appl. Sci. J. 18, 1073–1080 (2012).
Ainsworth, B. E. et al. 2011 Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 43, 1575–1581 (2011).
Wareham, N. J. et al. Validity and repeatability of a simple index derived from the short physical activity questionnaire used in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 6, 407–413 (2003).
Mirmiran, P., Esfahani, F. H., Mehrabi, Y., Hedayati, M. & Azizi, F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 13, 654–662 (2010).
Haytowitz, D. et al. USDA National Nutrient Database for Standard Reference, Release 24 (US Department of Agriculture, 2011).
Alba, D. L. et al. Changes in lean mass, absolute and relative muscle strength, and physical performance after gastric bypass surgery. J. Clin. Endocrinol. Metab. 104, 711–720 (2019).
Reis, M. M. & Arantes, P. M. M. Assessment of hand grip strength-validity and reliability of the saehan dynamometer. Fisioterapia Pesquisa 18, 176–181 (2011).
Vaz, M., Thangam, S., Prabhu, A. & Shetty, P. Maximal voluntary contraction as a functional indicator of adult chronic undernutrition. Br. J. Nutr. 76, 9–15 (1996).
Ravisankar, P., Udupa, K. & Prakash, E. S. Correlation between body mass index and blood pressure indices, handgrip strength and handgrip endurance in underweight, normal weight and overweight adolescents. Indian J. Physiol. Pharmacol. 49, 455 (2005).
Rahi, B. et al. High adherence to a Mediterranean diet and lower risk of frailty among French older adults community-dwellers: Results from the Three-City-Bordeaux Study. Clin. Nutr. 37, 1293–1298 (2018).
Laclaustra, M. et al. Prospective association between added sugars and frailty in older adults. Am. J. Clin. Nutr. 107, 772–779 (2018).
León-Muñoz, L. M., García-Esquinas, E., López-García, E., Banegas, J. R. & Rodríguez-Artalejo, F. Major dietary patterns and risk of frailty in older adults: A prospective cohort study. BMC Med. 13, 11 (2015).
Granic, A. et al. Effect of dietary patterns on muscle strength and physical performance in the very old: Findings from the newcastle 85+ study. PLoS ONE 11, e0149699 (2016).
Bartels, E. M., Robertson, S., Danneskiold-Samsøe, B., Appleyard, M. & Stockmarr, A. Effects of lifestyle on muscle strength in a healthy Danish population. J. Lifestyle Med. 8, 16 (2018).
Petersen, A. M. W. et al. Smoking impairs muscle protein synthesis and increases the expression of myostatin and MAFbx in muscle. Am. J. Physiol. Endocrinol. Metab. 293, E843–E848 (2007).
Power, M. L. & Schulkin, J. Sex differences in fat storage, fat metabolism, and the health risks from obesity: Possible evolutionary origins. Br. J. Nutr. 99, 931–940 (2008).
Schaap, L. A., Koster, A. & Visser, M. Adiposity, muscle mass, and muscle strength in relation to functional decline in older persons. Epidemiol. Rev. 35, 51–65 (2013).
Stenholm, S. et al. Long-term determinants of muscle strength decline: Prospective evidence from the 22-year mini-Finland follow-up survey. J. Am. Geriatr. Soc. 60, 77–85 (2012).
Bagheri, A. et al. Inflammatory potential of the diet and risk of sarcopenia and its components. Nutr. J. 19, 1–8 (2020).
Mohseni, R. et al. Relationship between major dietary patterns and sarcopenia among menopausal women. Aging Clin. Exp. Res. 29, 1241–1248 (2017).
Schaap, L. A., Pluijm, S. M., Deeg, D. J. & Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 119, 526.e9-526.e17 (2006).
Esmaillzadeh, A. et al. Dietary patterns and markers of systemic inflammation among Iranian women. J. Nutr. 137, 992–998 (2007).
Amakye, W. K. et al. The relationship between dietary inflammatory index (DII) and muscle mass and strength in Chinese children aged 6–9 years. Asia Pac. J. Clin. Nutr. 27, 1315 (2018).
Granic, A., Sayer, A. A. & Robinson, S. M. Dietary patterns, skeletal muscle health, and sarcopenia in older adults. Nutrients 11, 745 (2019).
Tanaka, M., McDonagh, M. & Davies, C. A comparison of the mechanical properties of the first dorsal interosseous in the dominant and non-dominant hand. Eur. J. Appl. Physiol. 53, 17–20 (1984).
Acknowledgements
Authors thank all those who participated in this study.
Funding
This manuscript has been granted by the Tehran University of Medical Sciences (Grant No: 40186). The funder had no role in the design, analysis, or writing of this article.
Author information
Authors and Affiliations
Contributions
S.S. and K.D. contributed to conception/design of the research and to acquisition of data. E.A. participated in analysis and interpretation of the data, and drafted the manuscript; S.S.-B. critically revised the manuscript, and she agrees to be fully accountable for ensuring the integrity and accuracy of the work. All authors read and approved the final manuscript. This is formally to submit the article entitled “Association of dietary and lifestyle inflammation scores with muscle strength and muscle endurance among adults in Tehran, Iran” prepared by the Tehran University of Medical Sciences for review and, hopefully, publication in your prestigious journal. The authors would like to advise that all authors listed have contributed to the work. All authors have agreed to submit the manuscript to Nutrition. No part of the work has been published before.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Asgari, E., Djafarian, K. & Shab-Bidar, S. Association of dietary and lifestyle inflammation scores with muscle strength and muscle endurance among Tehranian adults. Sci Rep 12, 20343 (2022). https://doi.org/10.1038/s41598-022-23202-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-23202-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
