
Abstract
Educational quality may be a closer correlate of physical health than more commonly used measures of educational attainment (e.g., years in school). We examined whether a widely-used performance-based measure of educational quality is more closely associated with cardiometabolic health than educational attainment (highest level of education completed), and whether perceived control (smaller sample only), executive functioning (both samples), and health literacy (smaller sample only) link educational quality to cardiometabolic health. In two samples (N = 98 and N = 586) collected from different regions of the US, educational quality was associated with cardiometabolic health above and beyond educational attainment, other demographic factors (age, ethnoracial category, sex), and fluid intelligence. Counter to expectations, neither perceived control, executive function, nor health literacy significantly mediated the association between educational quality and cardiometabolic health. Findings add to the growing literature suggesting that current operationalizations of the construct of education likely underestimate the association between education and multiple forms of health. To the extent that educational programs may have been overlooked based on the apparent size of associations with outcomes, such actions may have been premature.
Similar content being viewed by others


Testing the unique effect of educational quality on BMI and central adiposity in adulthood and hypothesized mediators
Major disparities in health by socioeconomic status persist in the Unites States despite enormous health care expenditures and decades of codified commitment to reducing health disparities1. Education is one indicator of socioeconomic status that has been consistently associated with multiple indicators of health over the life course2,3, including cardiometabolic disease and risk factors for poor cardiometabolic health such as greater BMI and central adiposity4,5. However, common measures of education used to inform policy and interventions on health outcomes may vastly underestimate the importance of education. The present study examines individual-level differences in educational quality and physical health outcomes beyond traditional measures of education in two diverse community samples. Additionally, we tested multiple mechanisms hypothesized to explain why increased education may result in better physical health.
Does educational quality matter?
Although empirical evidence has largely examined educational attainment (e.g., years of education or highest degree attained) in relation to health, educational quality is likely a better measure of the construct of education in health research. Preliminary evidence suggests incremental predictive utility of educational quality above and beyond educational attainment6,7. Educational quality might be a stronger predictor of health compared to assessments of educational attainment because it more directly measures cognitive and skill-based benefits of both formal and informal education that are thought to confer benefits to health8. For example, education is hypothesized to influence cardiovascular risk, in part, through the acquisition of skills and abilities that lead to better income and employment, increased health literacy and general knowledge, and greater self-efficacy and perceived control9,10,11. Not all individuals that attain a higher level of education also experience the same gains in such skills and abilities. Further, educational quality may be a more useful measure for understanding educational disparities in health across race and socioeconomic status in the United States, given that similar quantities of educational attainment (e.g., years in school) tend to result in lower educational quality for racial and ethnic minority students12. As Sentell, Zhang and Ching stated, “Many minority adults thus get less ‘education’ for their years of schooling, ” suggesting that measures of educational attainment do not fully capture racial and ethnic disparities in schooling that may influence health13.
To date, much of the small empirical literature on educational quality and health has focused on cognitive health outcomes rather than physical health, despite the well-established association between education and physical health14,15. For example, improvements in educational quality at the state-level (e.g., student–teacher ratio) have been associated with reduced risk for dementia16, and educational quality assessed using an individually assessed word-reading subtest has been associated with memory decline even after controlling for educational attainment15. Current research also tends to focus on differences in educational quality between groups as broad context or policy differences (e.g., funding, length of school days, racial segregation) or examines the implementation of high-quality early childhood education such as Head Start. While these studies inform whether educational quality may be associated with different outcomes across groups of learners, they cannot speak to individual level outcomes or the psychobiological processes that may help explain how educational quality can protect against poor health, perhaps even over and above educational attainment. An individual and objective measure of educational quality might fill such gaps.
Theoretical mechanisms connecting educational quality to cardiovascular health
Education is thought to influence cardiovascular health through multiple pathways including perceived control, executive functioning, and health literacy7,17. Perceived control, the belief that one’s actions can directly influence life outcomes, has been consistently linked to better health, physical functioning, and lower mortality risk18,19,20. Further, perceived control appears to mediate associations between education and poor health, including outcomes of mortality, incident disease, and biological risk factors21,22,23. Education is hypothesized to increase perceived control through the development of analytic and communication skills24,25. Self-reported perceptions of control also are more predictive of outcomes than actual control, perhaps because feeling in control is associated with lower psychological stress10,26.
Education may also influence cardiovascular health through executive functioning. Executive functioning is a set of higher order cognitive processes that involve reasoning, problem solving, and the planning, organization, and execution of behavior27,28,29. Executive functioning is associated with educational quality30,31, and educational quality has been shown to be a better predictor of decline in executive function than educational attainment in an ethnically diverse cohort32 (p.215). Deficits in executive functioning have also been implicated in the onset and progression of multiple diseases, including cardiovascular and metabolic diseases, and have been specifically implicated in weight management (for a review see33). For example, inhibition, a core component of executive function, is germane to weight management because it is associated with lower risk of overeating33.
Lastly, educational quality may also influence cardiometabolic health, in part, through health literacy. Health literacy is the ability to obtain and understand basic health information and services1. General literacy and analytic skills are fundamental to the development of health literacy. Greater health literacy is associated with more education and higher educational quality34,35 and lower morbidity including from cardiometabolic diseases36,37. Poorer health literacy is thought to contribute to poorer health, in part, because it is associated with poorer comprehension of health care services and outcomes as well as poorer health behaviors38. Additionally, educational quality appears to be more closely related to objective measures of health literacy than educational attainment14,15.
The current study
The current study tested whether educational quality was associated with BMI and two measures of central adiposity (visceral fat, waist circumference), all of which are risk factors for poor cardiometabolic health39,40. We examined whether effects remained after adjustment for demographic factors as well as educational attainment, and we tested whether perceived control, executive function, or health literacy mediated the association between educational quality and our health outcomes.
To validate our findings, two independent samples were used. An exploratory analysis used data from the Alabama Brain Study on Risk for Dementia (ABSoRD)41, which had more relevant measures including visceral fat, waist circumference, perceived control, and health literacy. The confirmation analysis used data from the Human Connectome Project-Aging (HCP-A)42 and had many overlapping measures (e.g., BMI, education quality, and executive function).
Methods
Design and participants
All participants provided written, informed consent and the research was performed as approved by the Institutional Review Board at the University of Alabama. Additionally, all research was performed in accordance with the Declaration of Helsinki. Both data sets were studies that also collected neuroimaging data and excluded middle-aged and older adults with MRI contraindicators, who self-reported any neuropsychological disorders or scored low on dementia screeners, a history of stroke, and traumatic brain injury (for details see ref. 41 and 42). ABSoRD data included 98 participants (62% females; 62% non-Hispanic White) with a mean age of 51.12 years (SD = 17.46) collected from Birmingham, AL. Educational attainment varied considerably in this sample (see Supplemental Table 1), with 34.4% of the sample reporting a high school degree or less, 16.7% an associate’s degree, 33.3% a bachelor’s degree, and 15.6% a graduate degree. The HCP-A data included 586 participants (59% females; 65% non-Hispanic White) with a mean age of 58.10 (SD = 13.85) collected from four sites: St. Louis, MI, Minneapolis, MN, Boston, MA, and Los Angeles, CA. Educational attainment also varied considerably in this sample, ranging from 7 to 21 years of education, though almost three-fourths of participants (72.35%) reported more than 16 years of education (see Supplemental Table 2).
Measures
Educational quality
Consistent with past research8,43,44,45,46,47, educational quality was measured by oral word reading performance using the WRAT-4 in ABSoRD48 or the Oral Reading Recognition Test from the NIH Toolbox49. Up to 55 English words of various difficulty were read aloud by participants. Word reading has been validated as a measure of education quality by showing high correlations with a self-reported Quality of Education Scale50 and with objective measures of student funding, student–teacher ratio, and days of school43.
Educational attainment
In the exploratory analyses in the smaller sample, educational attainment was operationalized using six levels: primary school, high school, associate's degree, bachelor's degree, master's degree/MBA/JD, doctoral degree. In the larger confirmation sample, years of education was used, which also extends the generalizability of educational attainment.
BMI, waist circumference, and visceral fat
Height was self-reported by participants. Both weight and visceral fat (fat surrounding internal organs) were assessed using an OMRON body composition BF511 scale (Omron, Japan), which uses bioelectrical impedance to measure visceral fat. BMI was calculated as weight (kg) / height (m)2. Waist circumference was assessed by trained study staff who measured circumference at the level of the navel.
Perceived control
Perceived control was only measured in the ABSoRD study, and was measured using the internal control subscale of the Locus of Control Scale (LOC)51. This subscale consists of eight items, each on a 6-point likert scale and has demonstrated reliability and validity 52. Items included “Whether or not I get to be a leader depends mostly on my ability.”
Executive function
Executive functioning was measured using the same two assessments in both the ABSoRD and HCP-A samples: the Trail Making Test—part B (TMT-B) and the Flanker from the Attention Network Test (ANT). The TMT-B is designed to assess frontal lobe functioning, and is a frequently used neuropsychological test of executive function that records participants’ speed alternating between several numbers and letters. The TMT-B measures one major component of executive functions—switching. The TMT-B has demonstrated adequate reliability and validity53. The Flanker measures another major component of executive functioning—response inhibition54. The task intersperses predictive and misleading visual cues. In this task, participants are asked to press a key on the keyboard to indicate whether a center arrow is pointing to the left or right as fast as they can. On some trials, several arrows to the left and right of the central arrow also are presented that are either in the same direction as the central arrow (congruent trials) or in the opposite direction (incongruent trials). Participants must inhibit the tendency to respond in line with the flanking arrows in the incongruent trials, usually resulting in a slowing down of response times. An executive attention score is created by subtracting reaction times in the congruent condition from reaction times in the incongruent task such that higher scores represent a greater difficulty inhibiting the flanking arrows (i.e., poorer performance). This measure of the Flanker has been shown to have a split-half reliability of 0.7055.
Health literacy
Health literacy was only measured in the ABSoRD study, and measured with the Health and Financial Literacy Assessment56. The nine questions from the health literacy section were used, testing participants’ knowledge about Medicare, doctor’s prescription instruction, drug risk information, and leading cause of death in older adults. The nine multiple-choice health literacy questions have shown adequate internal reliability56 and convergent validity57. Items included “True or false? Medicare routinely covers costs associated with extended long-term care, such as nursing home care lasting more than 1 month.”
Fluid intelligence
In ABSoRD, fluid intelligence was assessed using Raven’s Progressive Matrices (RPM)58, and in HCP-A a fluid composite score was used. In ABSoRD, using the RPM, participants viewed a series of patterns with a portion missing and had to choose the pattern that correctly filled the missing portion from eight potential options. Four sets were given with increased difficulty with each set. Only half of each set was used to allow for potential re-use for longitudinal testing, and accuracy was used as the primary outcome variable. In addition, the first one in the set served as practice and was not counted in the final score, leaving a possible total of 23 items. Reliability and validity are good for the RPM. Internal consistency exceeds 0.9059,60, and test–retest reliability up to a year is adequate, exceeding 0.8559. Correlations with other intelligence tests range from 0.54 to 0.8659,60. In HCP-A, a fluid composite score was a precomputed measure that averaged normalized scores from five tasks in the NIH Toolbox: Flanker, Dimensional Change Card Sort, Picture Sequence Memory, List Sorting, and Pattern Comparison61. This composite measure has good internal consistency at 0.83, good test–retest reliability at 0.86, and good convergent validity with standard measures (r = 0.78)62.
Additional covariates
The following demographic variables were included in the models as control variables: age, sex, and ethnoracial category. For the ABSoRD data, ethnoracial category (i.e., race) was coded as White (2), Black/African American (1), and all other identities (0). For the HCP-A data, ethnoracial category was divided into non-Hispanic White, non-Hispanic Asian, non-Hispanic Black, non-Hispanic Other, and Hispanic groups. Age was a continuous variable calculated as the number of years from birth to the date of cognitive testing. Sex was coded as a binary categorical variable; male (0) and female (1).
Overview of statistical analyses
Bivariate correlations were examined among primary study variables and provide an initial estimate of unadjusted effect size between variables. We also examine partial correlations adjusted for age, sex, and ethnoracial category. Multivariate regression analyses were performed to examine unique associations between objectively assessed educational quality and outcomes. Regressions are presented in a hierarchical format, with the first model controlling for demographic covariates (age, sex, ethnoracial category), the second model adding educational quality, and the third model examining whether any effect of educational quality remains after controlling for educational attainment. Sensitivity analyses further controlled for fluid intelligence as an important potential confound in both samples. The viability of mediators was also tested using regression; first verifying that the predictor variable is significantly associated with the mediator and that the mediator is significantly associated with the outcome variable as theoretically hypothesized. The potential mediators of perceived control and health literacy were only available in the ABSoRD data, and two identical measures of executive function were available in both data sets.
Results
Descriptive analyses and correlations
Descriptive statistics as well as bivariate correlations and partial correlations adjusting for demographic variables (age, sex, ethnoracial category) are presented in Tables 1 and 2. In the smaller ABSoRD dataset (Table 1), educational attainment and educational quality were correlated near 0.50 whether unadjusted or adjusted for demographic variables. BMI, visceral fat, and waist circumference were all highly correlated, all r > 0.71, all p < 0.001 whether unadjusted or adjusted for demographic variables. All three outcome variables were similarly and significantly correlated with educational quality in bivariate analyses (all r between −0.32 and −0.24, all p < 0.001). Educational quality was not associated with perceived control or executive function as indexed by Trails B, but was significantly associated with executive function as indexed by the Flanker and health literacy in bivariate correlations. In bivariate analyses, perceived control and executive function as indexed by the Flanker was significantly associated with all three outcome variables, executive function as indexed by Trails B was marginally associated with visceral fat and waist circumference (both p < 0.06), and health literacy was not associated with any outcome variable. In the HCP-A data (Table 2), correlations were overall weaker. BMI was only correlated with years of education and educational quality before covariates were added into the model. BMI was not associated with Flanker or Trails B performance.
Is educational quality associated with BMI and central adiposity?
Table 3 shows results of regression analyses predicting BMI, visceral fat, and waist circumference. In demographic models predicting BMI, age was the only demographic variable significantly associated with BMI. When educational quality was added in Model 2, it was significantly associated with BMI. The addition of educational quality also doubled the predictive utility of the model as indexed by the change in R2 from Model 1 and this was a significant difference; F-change (1, 91) = 8.62, p = 0.004. As seen in Table 4, the same results were found for BMI in the HCP-A sample; F-change (1, 216) = 9.64, p = 0.002. Further adjusting for educational attainment in Model 3 did not significantly increase R2 and educational quality continued to be similarly and significantly associated with BMI.
Models predicting visceral fat showed a very similar pattern of results. In Model 1, sex was a significant predictor of visceral fat in addition to age. In Model 2, educational quality was significantly associated with visceral fat, and adding educational quality to the model significantly improved the predictive utility of the model; F-change (1, 91) = 7.00, p = 0.010. In Model 3, educational quality remained similarly and significantly associated with visceral fat even after adjustment for educational attainment.
Models predicting waist circumference also showed a similar pattern of results. In Model 1, age was the only demographic factor significantly associated with waist circumference. In Model 2, educational quality was significantly associated with waist circumference, and adding educational quality to the model significantly improved the predictive utility of the model; F-change (1, 91) = 6.42, p = 0.013. In Model 3, educational quality remained similarly and significantly associated with visceral fat after adjustment for educational attainment.
Do differences in subjective perceptions of control, executive function, or health literacy help explain the association between educational quality and outcomes?
Perceived control was only available in the smaller ABSoRD dataset. In multivariate regression analyses, perceived control was significantly associated with BMI (b = −1.90, SE = 0.78, p = 0.018), visceral fat (b = −1.27, SE = 0.58, p = 0.032), and waist circumference (b = −5.28, SE = 2.26, p = 0.022) after adjusting for age, ethnoracial category, and sex. However, educational quality was not significantly associated with perceived control after adjusting for age, ethnoracial category, and sex. Given the lack of association between the predictor and the proposed mediator, we did not perform further tests of mediation. Interestingly, when educational quality and perceived control are entered into models simultaneously both are independent predictors of all three outcome variables.
The same two measures of executive function, Trails B and the Flanker task, were available in both samples. Neither measure of executive function was significantly associated with any of the three outcome variables after adjusting for age, ethnoracial category, and sex in either sample. Given the lack of association between this proposed mediator and the outcomes, we did not perform further tests of mediation.
Health literacy was only available in the smaller ABSoRD dataset. Health literacy also was not significantly associated with any of the three outcome variables after adjusting for age, ethnoracial category, and sex. Given the lack of association between this proposed mediator and the outcomes, we did not perform further tests of mediation.
Sensitivity analysis
Like other cognitive assessments, the measure of educational quality used here may also be influenced by fluid intelligence (e.g., general aptitude). Given this, we examined whether educational quality was significantly associated with cardiometabolic health after adjustment for fluid intelligence: RPM from the smaller exploratory sample and a fluid composite score from HCP-A. Results are shown in Table 5. Educational quality remained a statistically significant predictor of BMI, visceral fat, and waist circumference. Fluid intelligence was not a significant predictor of any of the three outcomes. Effect sizes (standardized betas) were statistically indistinguishable from models without adjustment for fluid intelligence (Tables 3 and 4, Model 2).
Discussion
Most prior studies examining educational health disparities have assessed educational attainment, either by years of education or highest degree attained. Educational quality may be more closely related to physical health because it directly assesses the cognitive and skill-based benefits of education (e.g., knowledge, skills, reasoning, effectiveness) that are thought to confer benefits to health8. This study examined whether an objective individual-level assessment of educational quality, which has been widely used in studies of education quality and cognitive health, was associated with cardiometabolic health. Analyses further examined whether perceived control, performance-based assessments of executive function, or health literacy may explain the association between educational quality and cardiometabolic health. We originally performed analyses in a smaller exploratory dataset (ABSoRD) and then a second, larger sample was used to replicate the findings when conceptually similar variables were available. The two samples complemented each other in many respects. For example, ABSoRD had greater variability in educational attainment than the larger HCP-A dataset, and constructs were often operationalized using different measures across studies.
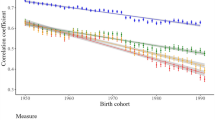
Initial correlations suggested that educational quality was a closer correlate of cardiometabolic health. In the ABSoRD dataset, educational quality (v. educational attainment) was equally or more strongly associated with all outcomes and mediators with the exception of Trails B. In the HCP-A dataset, which also collected Trails B, educational quality was equally or more strongly associated with all outcomes and mediators. Despite the moderate correlation between educational attainment and educational quality (~ r = 0.50 and ~ r = 0.40 for the exploratory and confirmatory samples, respectively), the relationship between educational quality and cardiometabolic health was independent of educational attainment in both samples. The association between educational quality and cardiometabolic health was also unchanged after adjusting for fluid intelligence in both samples (for a visual comparison of the association between educational quality and outcomes using progressive statistical adjustments see Figs. 1 and 2). Thus, associations between cardiometabolic health and educational quality cannot be attributed to underlying differences in general aptitude (e.g., educational quality is not just a proxy for aptitude). These findings contribute additional supporting evidence to the small literature showing that educational quality may be more closely associated with physical health than educational attainment or quantity (e.g., years in school, highest degree attained).

Associations between educational quality and BMI, visceral fat, and waist circumference. The blue line is the association between educational quality and the outcome adjusting for demographics (age, sex, ethnoracial category). The purple line further adjusts for educational attainment as measured by educational attainment. The yellow line further adjusts for fluid IQ. The strength of the association between educational quality and outcomes is virtually unchanged after adjustment for demographics, educational attainment, or fluid IQ.

Associations between educational quality and BMI in the HCP-A data set. The blue line is the association between educational quality and the outcome adjusting for demographics (age, sex, ethnoracial category). The purple line further adjusts for educational attainment as measured by educational attainment. The yellow line further adjusts for fluid IQ. The strength of the association between educational quality and outcomes is virtually unchanged after adjustment for demographics, educational attainment, or fluid IQ.
While associations between educational quality and cardiometabolic health outcomes were highly consistent, we did not find support for the mediating role of perceived control (smaller exploratory sample only), two different measure of executive function (both samples), or health literacy (smaller exploratory sample only). Perceived control is frequently assessed in research examining the association between socioeconomic status and physical health23,63,64. Consistent with this literature, greater perceived control was associated with better cardiometabolic health, even though it did not mediate associations between education and cardiometabolic health. Although education may sometimes increase perceived control, the present study suggests that other factors, at least in the current sample, might have influenced one’s perceived control. For example, having a larger family structure and the social support that family can bring has been shown to be related to perceived control65. Lifetime experiences with healthcare systems, stressors, and social pressures also can impact one’s level of perceived control, which could also affect coping behaviors related to both the physiology underlying eating behaviors (e.g., satiety responses) as well as psychological components of eating to regain feelings of control66. Many of these factors are independent of educational attainment or quality in their impact on cardiometabolic health.
Executive function was assessed using two tasks: one assessing mental switching (Trails Making B, both samples) and another representing response inhibition (Flanker, both samples). Although we found some marginal associations between executive function, education, and cardiometabolic health before adjustment for demographic variables, no significant associations remained after demographic adjustments in either the exploratory or confirmatory samples. Thus, findings did not warrant mediation analyses. In the larger confirmatory sample, the two executive function measures were unrelated to BMI regardless of whether demographic variables were adjusted.
Health literacy was assessed by objective assessment of participants’ knowledge regarding health and healthcare. The measurement and importance of health literacy for cardiometabolic health and health disparities has recently garnered significant attention, in part, because health literacy is low in the United States and is associated with cardiometabolic health67,68. Health literacy was significantly associated with educational quality but not educational attainment in this sample but was not associated with cardiometabolic health (Table 1). The measure of health literacy used here was originally developed in a sample of older adults and contained several questions targeting this age group (e.g., What is Medicare?). Future research using health literacy assessments specific to lifelong health matters or cardiometabolic health may be more sensitive.
Limitations
This study has many methodological strengths that make it an important contribution to the literature such as objective assessment of both independent and dependent variables and examination of two distinct diverse community samples often with differing operationalization of constructs. Further, in-person objective assessments such as those used here can reduce measurement noise compared to larger national data sets in which constructs are assessed via telephone interviews and less reliable measures are used26,69. However, interpretation of results should also consider study limitations. Neither study samples were representative of the population, both were collected in urban locations and both samples consisted primarily of middle-aged and older adults. Although participants did vary considerably in educational attainment, most participants in the larger HCP-A sample reported high levels of education (> 16 years). Thus, results could be interpreted to mean that educational quality is able to differentiate among individuals with similar levels of education. We note, however, that we saw similar incremental utility for educational quality in the ABSoRD sample who did not tend to be highly educated and had more variability in educational attainment. Additionally, although the exploratory sample was not large, we supplemented many of the analyses with a much larger and independent sample that replicated the main findings where possible, despite also being collected from different parts of the country. The potential mediators of health literacy and perceived control were only available in the smaller ABSoRD study, and findings need to be replicated in larger datasets to assess whether mediational analyses may be warranted. Additionally, while we found non-existent to weak correlations with executive functions in both samples. Both executive function tasks examined here used response times to index executive function. Executive functions are very heterogeneous and this does not preclude that other types of executive functions might serve as mediators between education and cardiometabolic health including emotional regulation, working memory updating, and goal-maintenance, to name a few54,70. Measures of executive function that capture lasting control of one’s behaviors to both promote health might serve as a more sensitive mediator of cardiometabolic health than the reaction time measures used here.
Conclusions
Education is one indicator of socioeconomic status that has been consistently associated with multiple health outcomes, including cardiovascular and metabolic health. To date, researchers have primarily assessed education by asking people how many years they attended formal education or their highest attained degree. The present findings suggest that such measures of educational attainment underestimate the association between education and cardiometabolic health. Educational quality may be more closely associated with cardiometabolic health, similar to findings for cognitive health. We do not find support for the hypothesis that executive function, perceived control, or health literacy partially explain the association between educational quality and cardiometabolic health, and executive function was assessed in both samples. These findings have implications for interventions and government policies that aim to improve cardiometabolic health. To the extent that educational programs may have been ignored due to an apparent small relationship between education and cardiometabolic health, such actions may have been premature given that effect sizes for education quality can be appreciably larger than for education attainment even after controlling for demographic factors (Table 3). Although perhaps obvious, programs ensuring high quality educational outcomes is critical, as large variability in educational quality can exist within similar years of schooling or obtaining a similar degree.
Data availability
The ABSoRD dataset used and/or analysed during the current study available from the corresponding author on reasonable request. The HCP-A data generated and/or analysed during the current study are available in the Lifespan Human Connectome Project Aging Study repository, https://www.humanconnectome.org/study/hcp-lifespan-aging. The NDA Study record can be found at https://doi.org/10.15154/1528124.
References
National Center for Health Statistics. (2009). Healthy People 2010: Understanding and Improving Health, Chapter 11. U.S. Department of Health and Human Services. https://www.cdc.gov/nchs/data/hpdata2010/hp2010_final_review_focus_area_11.pdf
Walsemann, K. M., Geronimus, A. T. & Gee, G. C. Accumulating disadvantage over the life course: Evidence from a longitudinal study investigating the relationship between educational advantage in youth and health in middle age. Res. Aging 30(2), 169–199 (2008).
Zajacova, A. & Lawrence, E. M. The relationship between education and health: reducing disparities through a contextual approach. Annu. Rev. Public Health 39, 273–289 (2018).
Hamad, R., Elser, H., Tran, D. C., Rehkopf, D. H. & Goodman, S. N. How and why studies disagree about the effects of education on health: A systematic review and meta-analysis of studies of compulsory schooling laws. Soc. Sci. Med. 212, 168–178. https://doi.org/10.1016/j.socscimed.2018.07.016 (2018).
Hamad, R. et al. Quality and quantity: The association of state-level educational policies with later life cardiovascular disease. Prev. Med. 126, 105750 (2019).
Glymour, M. M. & Manly, J. J. Compulsory Schooling Laws as quasi-experiments for the health effects of education: Reconsidering mechanisms to understand inconsistent results. Soc. Sci. Med. 214, 67–69. https://doi.org/10.1016/j.socscimed.2018.08.008 (2018).
Mirowsky, J., & Ross, C. E. (Eds.). (2003). Education, Social Status, and Health. Routledge. https://doi.org/10.4324/9781351328081.
Sisco, S. et al. The role of early-life educational quality and literacy in explaining racial disparities in cognition in late life. J. Gerontol. B Psychol. Sci. Soc. Sci. 70(4), 557–567. https://doi.org/10.1093/geronb/gbt133 (2015).
Feinstein, J. S. The relationship between socioeconomic status and health: a review of the literature. Milbank Q. 1, 279–322 (1993).
Ross, C. E. & Wu, C. L. The links between education and health. Am. Sociol. Rev. 1, 719–745 (1995).
Matthews, K. A. & Gallo, L. C. Psychological perspectives on pathways linking socioeconomic status and physical health. Annu. Rev. Psychol. 62, 501–530 (2011).
Kirsch, I. S., Jungeblut, A. Jenkins, L., Kolstad, A. (1993). Adult literacy in America: A first look at the results of the National Adult Literacy Survey. US Government Printing Office, Superintendent of Documents, Washington, DC 20402 (Stock No. 065-000-00588-3). http://nces.ed.gov/Pubsearch/pubsinfo.asp?pubid=93275.
Sentell, T., Zhang, W. & Ching, L. K. Insights in public health: The importance of considering educational inequity and health literacy to understand racial/ethnic health disparities. Hawai’i J. Med. Public Health 74(7), 244–247 (2015).
Dotson, V. M., Kitner-Triolo, M. H., Evans, M. K. & Zonderman, A. B. Effects of race and socioeconomic status on the relative influence of education and literacy on cognitive functioning. J. Int. Neuropsychol. Soc. 15(4), 580–589. https://doi.org/10.1017/S1355617709090821 (2009).
Manly, J. J., Touradji, P., Tang, M. X. & Stern, Y. Literacy and memory decline among ethnically diverse elders. J. Clin. Exp. Neuropsychol. 25(5), 680–690. https://doi.org/10.1076/jcen.25.5.680.14579 (2003).
Nguyen, T. T. et al. The role of literacy in the association between educational attainment and depressive symptoms. SSM – Popul. Health 3, 586–593. https://doi.org/10.1016/j.ssmph.2017.07.002 (2017).
Cohen, A. K. & Syme, S. L. Education: a missed opportunity for public health intervention. Am. J. Public Health 103(6), 997–1001 (2013).
Infurna, F. J., Gerstorf, D., Ram, N., Schupp, J. & Wagner, G. G. Long-term antecedents and outcomes of perceived control. Psychol. Aging 26(3), 559 (2011).
Infurna, F. J., Ram, N. & Gerstorf, D. Level and change in perceived control predict 19-year mortality: Findings from the Americans’ changing lives study. Dev. Psychol. 49(10), 1833 (2013).
Turiano, N. A., Chapman, B. P., Agrigoroaei, S., Infurna, F. J. & Lachman, M. Perceived control reduces mortality risk at low, not high, education levels. Health Psychol. 33(8), 883 (2014).
Bosma, H., Schrijvers, C. & Mackenbach, J. P. Socioeconomic inequalities in mortality and importance of perceived control: Cohort study. BMJ 319(7223), 1469–1470. https://doi.org/10.1136/bmj.319.7223.1469 (1999).
Orton, L. C. et al. What is the evidence that differences in ‘control over destiny’lead to socioeconomic inequalities in health? A theory-led systematic review of high-quality longitudinal studies on pathways in the living environment. J. Epidemiol. Commun. Health 73(10), 929–934 (2019).
Zilioli, S., Imami, L. & Slatcher, R. B. Socioeconomic status, perceived control, diurnal cortisol, and physical symptoms: a moderated mediation model. Psychoneuroendocrinology 75, 36–43. https://doi.org/10.1016/j.psyneuen.2016.09.025 (2017).
Mirowsky, J. & Ross, C. E. Education, personal control, lifestyle and health: A human capital hypothesis. Res. Aging 20(4), 415–449 (1998).
Mitchell, U. A., Ailshire, J. A., Brown, L. L., Levine, M. E. & Crimmins, E. M. Education and psychosocial functioning among older adults: 4-year change in sense of control and hopelessness. J. Gerontol.: Ser. B 73(5), 849–859 (2018).
Lachman, M. E., Agrigoroaei, S., Tun, P. A. & Weaver, S. L. Monitoring cognitive functioning: Psychometric properties of the Brief Test of Adult Cognition by Telephone. Assessment 21(4), 404–417. https://doi.org/10.1177/1073191113508807 (2014).
Miyake, A. et al. The unity and diversity of executive functions and their contributions to complex “Frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 41, 49–100. https://doi.org/10.1006/cogp.1999.0734 (2000).
Suchy, Y. Executive functioning: Overview, assessment, and research issues for non-neuropsychologists. Ann. Behav. Med. 37(2), 106–116 (2009).
Williams, P. G. & Thayer, J. F. Executive functioning and health: Introduction to the special series. Ann. Behav. Med. 37(2), 101–105 (2009).
St Clair-Thompson, H. L. & Gathercole, S. E. Executive functions and achievements in school: Shifting, updating, inhibition, and working memory. Q. J. Experim. Psychol. 59(4), 745–759. https://doi.org/10.1080/17470210500162854 (2006).
Thorell, L. B., Veleiro, A., Siu, A. F. & Mohammadi, H. Examining the relation between ratings of executive functioning and academic achievement: Findings from a cross-cultural study. Child Neuropsychol. 19(6), 630–638. https://doi.org/10.1080/09297049.2012.727792 (2013).
Manly, J. J., Schupf, N., Tang, M. X. & Stern, Y. Cognitive decline and literacy among ethnically diverse elders. J. Geriatr. Psychiatry Neurol. 18(4), 213–217. https://doi.org/10.1177/0891988705281868 (2005).
Gettens, K. M. & Gorin, A. A. Executive function in weight loss and weight loss maintenance: A conceptual review and novel neuropsychological model of weight control. J. Behav. Med. 40(5), 687–701. https://doi.org/10.1007/s10865-017-9831-5 (2017).
Martin, L. T. et al. Developing predictive models of health literacy. J. Gen. Intern. Med. 24(11), 1211–1216. https://doi.org/10.1007/s11606-009-1105-7 (2009).
Mõttus, R. et al. Towards understanding the links between health literacy and physical health. Health Psychol. 33(2), 164–173. https://doi.org/10.1037/a0031439 (2014).
Koh, H. K. et al. New federal policy initiatives to boost health literacy can help the nation move beyond the cycle of costly ‘crisis care’. Health Aff. 31(2), 434–443. https://doi.org/10.1377/hlthaff.2011.1169 (2021).
Marzec, L. N. et al. Cognitive dysfunction and poor health literacy are common in veterans presenting with acute coronary syndrome: Insights from the MEDICATION study. Patient Prefer. Adherence 9, 745–751. https://doi.org/10.2147/PPA.S75110 (2015).
DeWalt, D. A., Berkman, N. D., Sheridan, S., Lohr, K. N. & Pignone, M. P. Literacy and health outcomes. J. Gen. Intern. Med. 19(12), 1228–1239. https://doi.org/10.1111/j.1525-1497.2004.40153.x (2004).
Klein, S. et al. Waist circumference and cardiometabolic risk: a consensus statement from shaping America’s health: Association for Weight Management and Obesity Prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Am. J. Clin. Nutr. 85(5), 1197–1202. https://doi.org/10.1093/ajcn/85.5.1197 (2007).
Sironi, A. M. et al. Impact of increased visceral and cardiac fat on cardiometabolic risk and disease. Diabet. Med. 29(5), 622–627. https://doi.org/10.1111/j.1464-5491.2011.03503.x (2012).
McDonough, I. M., Letang, S. K. & Stinson, E. A. Dementia risk elevates brain activity during memory retrieval: A functional MRI analysis of middle aged and older adults. J. Alzheimers Dis. 70(4), 1005–1023. https://doi.org/10.3233/JAD-190035 (2019).
Bookheimer, S. Y. et al. The lifespan human connectome project in aging: an overview. Neuroimage 185, 335–348 (2019).
Crowe, M. et al. Indicators of childhood quality of education in relation to cognitive function in older adulthood. J. Gerontol. Ser. A: Biomed. Sci. Med. Sci. 68(2), 198–204. https://doi.org/10.1093/gerona/gls122 (2013).
Crowe, M., Clay, O. J., Sawyer, P., Crowther, M. R. & Allman, R. M. Education and reading ability in relation to differences in cognitive screening between African American and Caucasian older adults. Int. J. Geriatr. Psychiatry 23(2), 222–223 (2008).
Manly, J. J., Jacobs, D. M., Touradji, P., Small, S. A. & Stern, Y. Reading level attenuates differences in neuropsychological test performance between African American and White elders. J. Int. Neuropsychol. Soc. 8(3), 341–348 (2002).
Manly, J. J., Byrd, D. A., Touradji, P. & Stern, Y. Acculturation, reading level, and neuropsychological test performance among African American elders. Appl. Neuropsychol. 11(1), 37–46 (2004).
Silverberg, N. D., Hanks, R. A. & Tompkins, S. C. Education quality, reading recognition, and racial differences in the neuropsychological outcome from traumatic brain injury. Arch. Clin. Neuropsychol. 28(5), 485–491 (2013).
Wilkinson, G. S., & Robertson, G. J. Wide range achievement test (WRAT4). Lutz, FL: Psychological Assessment Resources (2006).
Gershon, R. C. et al. Language measures of the NIH toolbox cognition battery. J. Int. Neuropsychol. Soc. 20(6), 642–651 (2014).
Sayegh, P., Arentoft, A., Thaler, N. S., Dean, A. C. & Thames, A. D. Quality of education predicts performance on the wide range achievement test-word reading subtest. Arch. Clin. Neuropsychol. 29(8), 731–736 (2014).
Levenson, H. Activism and powerful others: Distinctions within the concept of internal-external control. J. Pers. Assess. 38(4), 377–383. https://doi.org/10.1080/00223891.1974.10119988 (1974).
Sapp, S. G. & Harrod, W. J. Reliability and validity of a brief version of Levenson’s locus of control scale. Psychol. Rep. 72(2), 539–550. https://doi.org/10.2466/pr0.1993.72.2.539 (1993).
Calamia, M., Markon, K. & Tranel, D. The robust reliability of neuropsychological measures: Meta-analyses of test–retest correlations. Clin. Neuropsychol. 27(7), 1077–1105. https://doi.org/10.1080/13854046.2013.809795 (2013).
Friedman, N. P. & Miyake, A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex 86, 186–204. https://doi.org/10.1016/j.cortex.2016.04.023 (2017).
Ishigami, Y. et al. The Attention Network Test-Interaction (ANT-I): Reliability and validity in healthy older adults. Exp. Brain Res. 234(3), 815–827. https://doi.org/10.1007/s00221-015-4493-4 (2016).
James, B. D., Boyle, P. A., Bennett, J. S. & Bennett, D. A. The impact of health and financial literacy on decision making in community-based older adults. Gerontology 58(6), 531–539. https://doi.org/10.1159/000339094 (2012).
Bennett, J. S., Boyle, P. A., James, B. D. & Bennett, D. A. Correlates of health and financial literacy in older adults without dementia. BMC Geriatr. 12(1), 1–9. https://doi.org/10.1186/1471-2318-12-30 (2012).
Raven, J. C. & Court, J. H. Raven’s progressive matrices and vocabulary scales Vol. 759 (Oxford Pyschologists Press, 1998).
Raven, J., Raven, J. C., & Court, J. H. Manualfor Raven's progressive matrices and vocabulary scales. Section 3: The standard progressive matrices. Oxford, UK: Oxford Psychologists Press; San Antonio, TX: The Psychological Corporation (2000).
Court, J. H., & Raven, J. Manualjor Raven's Progressive Matrices and Vocabulary Scales. Section 7: Research and references: Summaries of normative, reliability, and validity studies and references to all sections. Oxford: Oxford University Press: San Antonio, TX.: The Psychological Corporation (1995).
Barch, D. M. et al. Function in the human connectome: task-fMRI and individual differences in behavior. Neuroimage 80, 169–189 (2013).
Heaton, R. K. et al. Reliability and validity of composite scores from the NIH Toolbox Cognition Battery in adults. J. Int. Neuropsychol. Soc. 20(6), 588–598 (2014).
Bosma, H. et al. Low control beliefs, classical coronary risk factors, and socio-economic differences in heart disease in older persons. Soc. Sci. Med. 60(4), 737–745 (2005).
Mooney, C. J., Elliot, A. J., Douthit, K. Z., Marquis, A. & Seplaki, C. L. Perceived control mediates effects of socioeconomic status and chronic stress on physical frailty: Findings from the health and retirement study. J. Gerontol.: Ser. B 73(7), 1175–1184. https://doi.org/10.1093/geronb/gbw096 (2018).
Serin, N. B., Serin, O. & Şahin, F. S. Factors affecting the locus of control of the university students. Procedia. Soc. Behav. Sci. 2(2), 449–452. https://doi.org/10.1016/j.sbspro.2010.03.041 (2010).
Neymotin, F. & Nemzer, L. R. Locus of control and obesity. Front. Endocrinol. 5(159), 1–4. https://doi.org/10.3389/fendo.2014.00159 (2014).
Chan, R. W. Y. & Kisa, A. A scoping review of health literacy measurement tools in the context of cardiovascular health. Health Educ. Behav. 46(4), 677–688. https://doi.org/10.1177/1090198119831754 (2019).
Magnani, J. W. et al. Health literacy and cardiovascular disease: Fundamental relevance to primary and secondary prevention: A scientific statement from the American Heart Association. Circulation 138(2), e48–e74. https://doi.org/10.1161/CIR.0000000000000579 (2018).
Ofstedal, M. B., Fisher, G. G. & Herzog, A. R. Documentation of cognitive functioning measures in the Health and Retirement Study (University of Michigan, 2005). https://doi.org/10.7826/isr-um.06.585031.001.05.0010.2005.
Carlson, S. M., Zelazo, P. D., & Faja, S. (2013). Executive function. In P. D. Zelazo (Ed.), The Oxford handbook of developmental psychology (Vol. 1): Body and mind (pp. 706–743). Oxford University Press.
Funding
Funding was provided by The University of Alabama through startup funds to I.M., the University of Alabama College Academy of Research, Scholarship, and Creative Activity to I.M., and the University of Alabama, Birmingham/The National Institutes of Health, grant/award number: P30AG031054. Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number U01AG052564 and by funds provided by the McDonnell Center for Systems Neuroscience at Washington University in St. Louis. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
J.M.C. drafted the manuscript and R.D.F., S.L. and I.M. provided critical revisions. I.M. conceived the parent project, and I.M. and S.L. collected and scored the data. J.M.C., I.M. and S.L. performed data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cundiff, J.M., Lin, S.SH., Faulk, R.D. et al. Educational quality may be a closer correlate of cardiometabolic health than educational attainment. Sci Rep 12, 18105 (2022). https://doi.org/10.1038/s41598-022-22666-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-22666-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
