
Abstract
To test whether heart rate variability (HRV) biofeedback training benefits older adults with different social interaction levels. Methods. 32 older adults (16 were institutionalized and 16 were not). Both groups received 14 sessions, 15 min, 3 times a week, with half of the individuals receiving HRV biofeedback training and the other half receiving control training. The following parameters were assessed immediately before and after training, and 4.5 weeks after the last session (follow-up period): aerobic conditioning, anthropometric data, emotional scores, and HRV components. Results. Before the training, the institutionalized individuals had higher scores of loneliness (p < 0.01) and depression (p < 0.0001) and lower social touches (p < 0.0001), body mass (p = 0.04), and body fat percentage (p = 0.002) than the non-institutionalized individuals. HRV biofeedback improved symptoms of depression in both groups. HRV improved only in the non-institutionalized group, and loneliness only in the institutionalized group. Lastly, all changes persisted after the follow-up period. Conclusions. HRV biofeedback training was effective in improving symptoms of depression in older adults. Improvement of HRV and loneliness was dependent on the level of social interaction.
Similar content being viewed by others
Introduction
Biofeedback training is a therapeutic tool that is useful in the teaching and learning of physiological and psychological processes of self-regulation1. It is an assisted learning method used to modify physiological functions over which one has little conscious control, such as respiratory rate, heart rate, and cerebral impulse activity2. Heart rate variability (HRV) biofeedback is a type of biofeedback that specifically involves respiratory rate modification (decrease in frequency and increase in amplitude) to increase synchronization between respiratory rate and heart rate. This synchronization allows an increase in the amplitude of HRV3.
HRV is a non-invasive measure extracted from electrocardiogram recording that reflects the continuous oscillation of the RR intervals as a function of the action of the sympathetic and parasympathetic branches on the sinoatrial node. RR intervals decrease during inspiration and increase during expiration4,5. HRV has been proposed as a marker of physical and mental health6 and, more specifically, as an important marker of social engagement7,8.
The social relations of older adults may change for a variety of reasons, including geographical migration of family members or friends, death or disability among members of their social networks, and reduction of physical or cognitive abilities9. Another important factor is institutionalization, which is in general linked to the feeling of social rejection10,11,12. Moreover, loneliness, depression (and other mental disorders), and social rejection are strongly correlated, and the negative impact of these variables on the lives of older adults can be significant13,14,15. Lastly, although mental health variables are negatively correlated with HRV, they may be positively modified through HRV biofeedback, as shown in adults10,16.
To our knowledge, there are no studies to date on the impact of HRV biofeedback on the health of the elderly population and, more specifically, on the role of the level of social interaction. Given the above, the objective of this pilot study was to test whether HRV biofeedback training benefits the health of older adults with different levels of social interaction. We specifically investigated whether: (i) there are differences in terms of aerobic conditioning, anthropometric data, emotional scores, and HRV components between institutionalized and non-institutionalized older adults; (ii) HRV biofeedback training improved these parameters among older adults; (iii) these improvements were dependent on institutionalization; and (iv) the benefits persisted after the training intervention.
Results
The total sample of the study comprised 32 volunteers, of whom 16 were institutionalized and 16 were not. The non-institutionalized group was composed of individuals who were members of a recreation club for older adults for 8.75 ± 8.01 years, in which four were men and 12 were women, with a mean age of 72.50 (69.00/76.00) years. The institutionalized group lived in the institution for 6.87 ± 6.94 years and included nine women and seven men with a mean age of 69.50 (67.50/75.50) years.
An investigation of the characteristics of the two study groups was performed before starting the interventions and significant differences were found between them. The comparisons are shown in Table 1.
The institutionalized and non-institutionalized groups differed in assessment 1 with indications of being different groups before the start of any intervention. Therefore, it was decided that all subsequent analyses should be conducted separately for each group (institutionalized and non-institutionalized).
After this characterization, we sought to determine whether training with biofeedback was able to promote changes in the variables evaluated when compared to the control group, and, if so, whether these changes persisted after a follow-up period. The data collected before (assessment 1) and after the 14 training sessions (assessment 2) and after the follow-up period (assessment 3) were compared between the biofeedback group and the control group within the non-institutionalized sample and then within the institutionalized sample.
Non-institutionalized group
Anthropometric and aerobic conditioning variables
In the non-institutionalized sample, the ANOVAs of the anthropometric and aerobic conditioning variables showed an effect of time (assessments 1, 2, and 3) on body fat percentage (F(2, 28) = 5.18, p = 0.01, d = 0.27) but not on body mass (F(2, 28) = 2.31, p = 0.11, d = 0.14), BMI (F(2, 28) = 2.39, p = 0.10, d = 0.15), and aerobic test (F(2, 28) = 0.92, p = 0.40, d = 0.06). There was a reduction in body fat percentage in the second and third assessments relative to the first assessment. There was an effect of group (control and biofeedback) on body mass (F(1, 14) = 4.62, p = 0.04, d = 0.25) biofeedback group with higher body mass than the control group but not on BMI (F(1, 14) = 3.57, p = 0.07, d = 0.20), aerobic test (F(1, 14) = 0.31, p = 0.58, d = 0.02), and body fat percentage (F(1, 14) = 4.29, p = 0.05, d = 0.23). There was no effect of the interaction between time and group on body mass (F(2, 28) = 0.33, p = 0.72, d = 0.02), BMI (F(2, 28) = 0.26, p = 0.76, d = 0.02), aerobic test (F(2, 28) = 0.99, p = 0.38, d = 0.07), and body fat percentage (F(2, 28) = 0.12, p = 0.88, d = 0.009).
Emotional variables
No main effects of time (assessments 1, 2, and 3) were observed in the ANOVAs of the emotional variables on loneliness (F(2, 28) = 2.03, p = 0.14, d = 0.13) and total touch (F(2, 28) = 1.24, p = 0.30, d = 0.08). In addition, there was no effect of group (control and biofeedback) on loneliness (F(1, 14) = 0.40, p = 0.53, d = 0.03), total touch (F(1, 14) = 0.86, p = 0.36, d = 0.06), and symptoms of depression (F(1, 14) = 1.75, p = 0.20, d = 0.11). No interaction between time and group was observed on loneliness (F(2, 28) = 2.03, p = 0.14, d = 0.13) and total touch (F(2, 28) = 2.80, p = 0.07, d = 0.17). However, there was a main effect of time (F(2, 28) = 7.00, p = 0.003, d = 0.33) and of the time and group interaction (F(2, 28) = 7.00, p = 0.003, d = 0.33) on symptoms of depression, which indicates a reduction in the symptoms of depression after biofeedback training; moreover, this reduction persisted after the training intervention (follow-up) (Fig. 1).

Symptoms of depression during assessments 1, 2, and 3 in the group that received biofeedback training (solid black line) and in the group that received the control training (dotted black line) in the non-institutionalized sample. aSignificant difference of assessment 2 and 3 in comparison to assessment 1 (< 0.05) and bsignificant differences between groups (< 0.05).
HRV components
The ANOVAs of HRV showed a main effect of time (assessments 1, 2, and 3) on the RMSSD (F(2, 28) = 3.78, p = 0.03, d = 0.21), SDNN (F(2,28) = 3.69, p = 0.03, d = 0.20), pNN50 (F(2, 28) = 5.19, p = 0.01, d = 0.27), SD1 (F(2, 28) = 3.78, p = 0.03, d = 0.21) and HF (F(2,28) = 5.55, p < 0.01, d = 0.28) . There was no main effect of group (control and biofeedback) on the variables RMSSD (F(1, 14) = 0.04, p = 0.83, d = 0.003), SDNN (F(1, 14) = 0.03, p = 0.86, d = 0.002), pNN50 (F(1, 14) = 0.04, p = 0.83, d = 0.003), SD1 (F(1, 14) = 0.04, p = 0.83, d = 0.003) and HF (F(1, 14) = 0.04, p = 0.84, d = 0.003). There was an effect of the interaction between time and group on all variables: RMSSD (F(2, 28) = 14.99, p < 0.0001, d = 0.52) (Fig. 2A), SDNN (F(2, 28) = 12.88, p = 0.0001, d = 0.47) (Fig. 2B), pNN50 (F(2, 28) = 11.62, p = 0.0002, d = 0.45) (Fig. 2C), SD1 (F(2, 28) = 14.99, p < 0.0001, d = 0.52) (Fig. 2D), and HF (F(2, 28) = 11.37, p = 0.0002, d = 0.45) (Fig. 2E). The post-tests showed an increase in all these variables after biofeedback training. This gain was sustained in the follow-up period. Moreover, at the beginning of the experiment, the RMSSD, SD1 and HF components were higher in the control group than in the biofeedback group, although this difference disappeared after the training.

(A) Values of the root mean square of the successive differences between the RR intervals (RMSSD) in ms; (B) values of logarithmic of the standard deviation of all R-R intervals (log SDNN) in ms; (C) values of logarithmic of the percentage of the successive differences between the R-R intervals that are > 50 ms (log pNN50) in ms; (D) values of standard deviation 1 (SD1) in ms; (E) values of logarithmic of high frequency (log HF) in ms2. All these components were evaluated in assessments 1, 2, and 3 in the group that received biofeedback training (solid black line) and in the group that received the control training (black dotted line) in the non-institutionalized sample. aSignificant difference of assessment 2 and 3 in comparison to assessment 1 (< 0.05) and bsignificant differences between groups (< 0.05).
Institutionalized group
Anthropometric and aerobic conditioning variables
In the institutionalized sample, the ANOVAs of the anthropometric and aerobic conditioning variables showed a main effect of time (assessments 1, 2, and 3) on body fat percentage (F(2, 28) = 3.50, p = 0.04, d = 0.20), with a higher body fat percentage in the last assessment, but not on body mass (F(2, 28) = 0.08, p = 0.91, d = 0.006), BMI (F(2, 28) = 0.11, p = 0.88, d = 0,008) and aerobic test (F(2, 28) = 1.00, p = 0.37, d = 0.07). In addition, there was not a main effect of group (control and biofeedback) on body mass (F(1, 14) = 0.01, p = 0.92, d = 0.0003), BMI (F(1, 14) = 0.003, p = 0.95), aerobic test (F(1, 14) = 0.03, p = 0.85, d = 0.02), and body fat percentage (F(1, 14) = 0.01, p = 0.91, d = 0.0008). Moreover, there was no effect of the interaction between time and group on body mass (F(2, 28) = 0.25, p = 0.77, d = 0.02), BMI (F(2, 28) = 0.19, p = 0.82, d = 0.01), aerobic test (F(2, 28) = 0.06, p = 0.93, d = 0.005), and body fat percentage (F(F(2, 28) = 1.16, p = 0.32, d = 0.08).
Emotional variables
With regard to the ANOVAs of the emotional variables, there was an effect of time (assessments 1, 2, and 3) on loneliness (F(2, 28) = 14.77, p < 0.01, d = 0.51) and symptoms of depression (F(2, 28) = 10.63, p < 0.01, d = 0.43) but not on total touch (F(2, 28) = 1.18, p = 0.32, d = 0.07). In addition, there was no effect of group (control and biofeedback) on total touch (F(1, 14) = 0.16, p = 0.69, d = 0.01), loneliness (F(1, 14) = 1.05, p = 0.32, d = 0.07), or depression (F(1, 14) = 1.07, p = 0.31, d = 0.07). There was no effect of the time and group interaction on touch (F(2, 28) = 0.59, p = 0.55, d = 0.04). However, there was an effect of the time and group interaction on loneliness (F(2, 28) = 3.76, p = 0.03, d = 0.21) and symptoms of depression (F(2, 28) = 7.67, p = 0.002, d = 0.35) (Fig. 3). In sum, feelings of loneliness and symptoms of depression decreased after biofeedback training and this reduction persisted after the training ceased.

(A) Loneliness; (B) symptoms of depression. All scales were evaluated in assessments 1, 2, and 3 in the group that received biofeedback training (solid black line) and in the group that received the control training (dotted black line) in the institutionalized sample. aSignificant difference of assessment 2 and 3 in comparison to assessment 1 (< 0.05).
HRV components
The ANOVAs of the variables of the HRV components showed an effect of time (assessments 1, 2, and 3) on RMSSD (F(2, 28) = 8.77, p = 0.001, d = 0.39), SDNN (F(2, 28) = 5.28, p = 0.01, d = 0.22), and SD1 (F(2, 28) = 8.78, p = 0.001, d = 0.39), with the highest values obtained in the second assessment being for all components, but there are not effect of time to pNN50 (F(2, 28) = 2.82, p = 0.07, d = 0.16), and HF (F(2, 28) = 2.46, p = 0.10, d = 0.15). In addition, there was a main effect of group (control and biofeedback) on RMSSD (F(1, 14) = 1.01, p = 0.32, d = 0.07), SDNN (F(1, 14) = 2.36, p = 0.14, d = 0.014), pNN50 (F(1, 14) = 1.31, p = 0.27, d = 0.07), and SD1 (F(1, 14) = 1.01, p = 0.33, d = 0.07), but not to HF (F(1, 14) = 1.10, p = 0.31, d = 0.09). Moreover, there was no effect of time and group interaction on the variables RMSSD (F(2, 28) = 0.72, p = 0.49, d = 0.05), SDNN (F(2, 28) = 0.33, p = 0.71, d = 0.02), pNN50 (F(2, 28) = 0.66, p = 0.52, d = 0.04), SD1 (F(2, 28) = 0.72, p = 0.49, d = 0.05), and HF (F(2, 28) = 0.31, p = 0.73, d = 0.02).
Discussion
In this pilot study, it was shown that (i) institutionalized older adults had higher baseline scores (before any intervention) regarding symptoms of depression and perceived social isolation and lower scores of social touches, lower body mass, and lower body fat percentage than the non-institutionalized older adults, with no differences in the HRV variables; (ii) HRV biofeedback training improved the symptoms of depression as well as of all HRV components among non-institutionalized older adults, whereas there was an improvement only in perceived social isolation and symptoms of depression in the institutionalized group; (iii) parameters that improved with HRV biofeedback were not all the same in the non-institutionalized and institutionalized groups; (iv) all parameters that were modified by biofeedback training persisted in the follow-up period in both groups.
Peplau12 described loneliness as a painful warning sign that the individual’s social relations are deficient. Accordingly, Kross et al.11 showed through magnetic resonance imaging that social rejection “hurts” not only metaphorically but also physically because social rejection and physical pain activate the same regions of the brain. Depression has been pertinently associated with loneliness13,17,18,19,20. These authors reported that the feeling of loneliness is strongly correlated with depression. The stronger the feeling of loneliness, the higher the depression indices or the probability of experiencing some degree of depression19,20. Lastly, a review conducted by Mushtaq et al.21 reinforced the conclusion that “loneliness can lead to various psychiatric disorders and physical conditions”. We speculate that the findings of Kross et al.11 may apply to older adults rejected by their families or by society. Rejection is one of the major causes of institutionalization14,15. Thus, the results of these studies are in line with our findings of lower scores of social touches and higher scores of perceived social isolation and depression in the institutionalized group than in the non-institutionalized group, whose social networks were preserved.
HRV biofeedback training improved all HRV components among the non-institutionalized but not among the institutionalized older adults. Several studies with samples of young adults showed that HRV biofeedback training improved HRV parameters16. However, there are no studies on the topic with older adults. No study that considered social interaction as a factor that influences the gains generated by biofeedback HRV training was found, regardless of the sampled population. The absence of social interaction in the everyday life of the institutionalized older adults probably prevented them from benefiting more from biofeedback training. Given this low social engagement, the polyvagal theory can provide a consistent theoretical basis for the interpretation of these results7,22,23, because only the group with high levels of social interaction (non-institutionalized group) had the vagal components of HRV improved. It is worth noting that these individuals were members of a club that offered activities such as theater, dance, and physical exercise and that the majority also had close partners. These are important factors for physiological correlates of social interaction, including oxytocin, endorphins, and vagal tone20,24,25.
HRV biofeedback training improved symptoms of depression in both groups, i.e., it was independent of the level of social interaction. Recent studies such as the meta-analysis by Lehrer et al.16 describe the effects of HRV biofeedback training at the central level, in which significant increase in blood flow fluctuations in all areas involved in emotional processing and modulation during training, specifically the limbic system and the cingulate and prefrontal cortices, could explain the improvement of depression-related states. A meta-analysis conducted by Lehrer et al.16 included several studies showing that HRV and depression improved after HRV biofeedback training. However, the literature is very scarce in studies with older adults. To our knowledge, there are only two studies in which HRV biofeedback training was used in the older adults in which mental health was evaluated26,27. Jester, Rozek and McKelley26 performed a 30-min training twice a week for 3 weeks to reduce psychiatric symptoms and improve cognitive functioning. The authors concluded that older adults may benefit from HRV biofeedback training the same way as the younger population. In addition, depression, anxiety, and attentional skills improved significantly after the intervention. This result is very similar to that obtained by Zauszniewski and Musil27, who observed a reduction in the levels of stress and depression among elderly women after 4 weeks of biofeedback training.
Another crucial result of this study was that of the follow-up assessment. We aimed to investigate whether the gains obtained from HRV biofeedback training would persist 4.5 weeks after the end of the intervention. Our findings showed that all gains generated by the training persisted after the intervention ended, in both groups (institutionalized and non-institutionalized). A recent meta-analysis confirmed our results, showing that HRV biofeedback training for a few weeks was effective in improving symptoms of depression in several psychophysiological conditions28. In one study involving patients with cancer, HRV biofeedback training was used with four to six sessions per week for a variable period, depending on the time required by each individual to reach cardiorespiratory coherence. The authors reported a significant improvement of stress, fatigue, and symptoms of post-traumatic stress disorder and depression relative to a control group, as well as in the maintenance of the cardiorespiratory coherence after 1 week of follow-up29. We emphasize that this is also a key and novel point of the study given the scarcity of studies investigating the persistence of the effects of biofeedback training after the follow-up period.
The study had the following limitations: a small sample size, imbalance between the number of men and women, and possible selection bias. To minimize the limitations of the study, (i) each volunteer performed the assessments and training on the same schedule, (ii) the intervention alternated between one individual of the control group and another of the biofeedback group, (iii) selection criteria were lack of volunteers with psychiatric illnesses, severe respiratory or cardiovascular diseases, cognitive impairments, walking difficulties, and smokers, (iv) the researchers who had contact with the volunteers were duly trained and were the same throughout the three assessments, and (v) on the assessment days, the participants were recommended not to ingest caffeine in the 2 h before the intervention and not to perform intense physical exercise and consume alcohol in the 24 h before the intervention.
Methods
Sample
The pilot study included 32 older adults of both genders, aged between 63 and 79 years. They were living in a long-term care institution for at least 6 months (institutionalized group: N = 16) or were members of a recreation club for older adults for at least 6 months (non-institutionalized group: N = 16). In each group, half of the sample was randomly assigned to HRV biofeedback training and the other half to control training.
The exclusion criteria were as follows: a history of serious psychiatric, neurological, respiratory, or cardiovascular diseases (self-reported in the health questionnaire); cognitive impairments (score above the cut-off point in the Mini-Mental State Examination)30; severe waking difficulties; smoking; and regular use of medications acting upon the central nervous system. The study was conducted in accordance with the Declaration of Helsinki. The protocol was approved by the Research Ethics Committee of the Federal University of Ouro Preto (CAAE: 85839018.9.0000.5150) and all volunteers signed the informed consent form. All data were collected before the COVID-19 pandemic.
Aerobic conditioning assessment
The sub-maximal aerobic capacity test, included in the Rikli and Jones battery of tests31, was used. It involves measuring the longest distance covered in a 6-min walk. The Physical Activity Readiness questionnaire32 and the Cardiovascular Risk Stratification (HHQ) questionnaire33 were used to select the individuals able to safely perform the aerobic test.
Anthropometric assessment
The following variables were assessed: height (measured with a portable vertical stadiometer, model Balmak—EST-223, with a range of 0–2.1 m and precision of 1 mm), body mass (measured using an Omron digital scale, model Hn 289, with a capacity of 150 kg and precision of 100 g34), body mass index (BMI) (measured using the data of body mass (kg) and height (m) and the equation: weight/height234), and body fat percentage determined using the Durnin and Womersley equation35, which uses four skinfolds in women (Db = 1.1339 – 0.0648 × log10 (subscapular skinfold + tricipital skinfold + suprailiac skinfold + bicipital skin fold)) and in men, it is calculated as Db = 1.1765 – 0.0744 × log10 (subscapular skinfold + tricipital skinfold + suprailiac skinfold + bicipital skinfold)). Subsequently, skinfold was converted into body fat percentage (%F) using the Siri equation (%F = [(4.95/SF) – 4.50] × 100))36.
Emotional assessment
The social touch scale37 is composed of 28 items and was used to assess the frequency in which the participant performed or received social touches over the last 12 months. Scores ranged from 14 to 98 points in the scales of touching and being touched, whereas total touch scores vary between 28 and 196 points. There is no cut-off point in the scale. The higher the obtained score, the greater the individual’s ability to perform or receive social contact through touch.
The revised UCLA Loneliness Scale38 is a self-evaluation instrument with 20 items about feelings or actions related to loneliness. The higher the score, the stronger the feeling of perceived loneliness.
The Geriatric Depression Scale39 is composed of 15 items and assesses symptoms of depression in the older adults. The sum of the scores of the answers from each participant may vary between 0 and 15 points, and a score of 5 or higher indicates the likelihood of depression.
HRV assessment
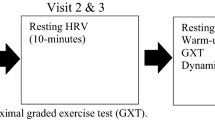
The electrocardiogram (ECG) recording was performed at rest, for 5 min, using the Nexus® 10 device, version 1.2, at three different moments: before and after training (which lasted 4.5 weeks), and on the follow-up (after 4.5 weeks). The unit of time was 1 ms, and the RR interval samples were collected at a sampling frequency of 256 Hz. The ECG electrodes were placed according to the Nexus-10® instructions, i.e., on the chest below the nipples and the clavicle because these points generate fewer artefacts. To prepare the skin for electrode placement, the pertinent areas of the skin were cleaned with ethanol.
Following data acquisition, HRV was extracted using the Kubios HRV Analysis Software (MATLAB, version 2.0 beta, Kuopio, Finland). In Kubios, the series was examined manually and inspected for artefacts. The following HRV components were analyzed: the standard deviation of all normal RR intervals recorded in a time interval (SDNN), which represents overall HRV activity and root mean square of the successive differences between RR intervals (RMSSD), percentage of the successive differences between the RR intervals that are greater than 50 ms (pNN50), standard deviation of instantaneous RR intervals (SD1) and high frequency (HF), which represents the predominance of parasympathetic activation4.
Training
HRV biofeedback training
The Nexus-10® hardware (Mind Media BV) and the BioTrace® software were used to conduct the HRV biofeedback sessions, in addition to recording the RR intervals during training and at rest. During training, the computer screen showed the respiratory rate and heart rate graphs in real-time and the participant was instructed to try to increase the synchronization between heart and respiratory waves trying to increase the amplitude and decrease the frequency of the both waves. For that purpose, the software calculated the resonance frequency in real-time based on the calculation of Pearson’s correlation between heart rate and respiratory rate. The values of resonance frequency ranged from “1” (positive correlation between heart rate and respiratory rate) to “-1” (negative correlation between heart rate and respiratory rate). During the HRV biofeedback session, the participants were instructed to try to increase the resonance frequency. For that purpose, the reference value should be as close as possible to “1”. This training was adapted from the protocol proposed by Lehrer, Vaschillo and Vaschillo1 and consisted of 14 sessions of 15 min each, performed three times a week for a total of 4.5 weeks.
Control training
Three blocks of 50 images with neutral valence obtained from the catalogue of the International Affective Picture System40 were constructed. Within each block, the time of exposure of the photograph varied from 3 to 7 s, and then a blank screen was shown for 2–6 s; this variation in exposure time aimed to minimize habituation to the stimulus. The means of the three blocks did not differ significantly regarding valence (MV) and activation (MA) (Block 1: MV = 5.02; MA = 3.62, Block 2: MV = 5.02; MA = 3.40, Block 3: MV = 5.13; MA = 3.82) and were presented sequentially throughout the control training sessions (e.g., session 1 block 1, session 2 block 2, session 3 block 3, session 4 block 1, and so forth) so that the participants’ attention was engaged on the control task. The structure of this training was the same as that of the experimental training, consisting of 14 sessions of 15 min each, performed three times a week for 4.5 weeks.
An assessment was performed at the end of the training (biofeedback and control).
Follow-up
A period of 4.5 weeks elapsed between the last training session and the re-assessment of the participants. The steps of the experimental design, from sample selection to the last assessment (follow-up assessment) are summarized in Fig. 4.

Experimental design.
Statistical analysis
The datasets used during the current study is available from the corresponding author on reasonable request. Initially, the normality of the raw data was tested using the Kolmogorov Smirnov test. Based on this, the normal (parametric) variables were described using the mean and standard deviation and the non-normal (non-parametric) variables were described using the median and the 25th and 75th percentiles. Subsequently, the t-test (normal variables) and the Mann–Whitney test (non-normal variables) were used for each collected variable (assessment 1) to determine the differences between the institutionalized group and the non-institutionalized group before starting any intervention.
To evaluate the differences between the collected variables before the start of the training (assessment 1), after the 14 training sessions (assessment 2), and after 4.5 weeks of follow-up (assessment 3) in the biofeedback and control groups within the non-institutionalized sample and then within the institutionalized sample, mixed-design repeated-measures ANOVA were performed for each parameter (anthropometric data, aerobic conditioning, emotional scores, and HRV components) using the factors time (assessments 1, 2, and 3) as the within variable and group (control and biofeedback) as the between variable. Subsequently, partial eta-squared was calculated to inform the effect size of all comparisons and Fisher’s post-hoc test was performed for the variables for which significant effects were observed. The SDNN, PNN50 and HF were normalized using logarithmic to use in the analyses.
The level of significance was set at 0.05 in all tests. Statistica 7.0 (StatSoft, Inc.) software was used in the analyses.
Data availability
The datasets used during the current study is available from the corresponding author on reasonable request.
References
Lehrer, P. M., Vaschillo, E. & Vaschillo, B. Resonant frequency biofeedback training to increase cardiac variability: Rationale and manual for training. Appl. Psychophysiol. Biofeedback 25, 177–191 (2000).
Silveira Gomes, J. & Coghi, M. F. Fernandes Coghi, Biofeedback cardiovascular e suas aplicações: revisão de literatura. Avances en Psicología Latinoamericana 32, 1 (2014).
Vaschillo, E. G., Vaschillo, B. & Lehrer, P. M. Characteristics of resonance in heart rate variability stimulated by biofeedback. Appl. Psychophysiol. Biofeedback 31, 129–142 (2006).
Force, T. Heart rate variability. Eur. Heart J. 17, 354–381 (1996).
Laborde, S., Mosley, E. & Thayer, J. F. Heart rate variability and cardiac vagal tone in psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 8, 213 (2017).
Shaffer, F., McCraty, R. & Zerr, C. L. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 5, 1 (2014).
Porges, S. W. Orienting in a defensive world: Mammalian modifications of our evolutionary heritage: A polyvagal theory. Psychophysiology 32, 301–318 (1995).
Porges, S. W. & Furman, S. A. The early development of the autonomic nervous system provides a neural platform for social behaviour: A polyvagal perspective. Infant Child Dev. 20, 106–118 (2011).
Cudjoe, T. K. et al. The epidemiology of social isolation: National health and aging trends study. J. Gerontol. Ser. B 75, 107–113 (2020).
Bzdok, D. & Dunbar, R. I. The neurobiology of social distance. Trends Cogn. Sci. 24, 717–733 (2020).
Kross, E., Berman, M. G., Mischel, W., Smith, E. E. & Wager, T. D. Social rejection shares somatosensory representations with physical pain. Proc. Natl. Acad. Sci. 108, 6270–6275 (2011).
Peplau, L. in Proceedings of the 3rd National Conference on Psychiatric Nursing (Montreal, Quebec, Canada). (1988).
Anderson, C. A. & Arnoult, L. H. Attributional style and everyday problems in living: Depression, loneliness, and shyness. Soc. Cogn. 3, 16–35 (1985).
Colussi, E. L., Pichler, N. A. & Grochot, L. Percepções de idosos e familiares acerca do envelhecimento. Revista Brasileira de Geriatria e Gerontologia 22, 1 (2019).
Ramos, L. R. Fatores determinantes do envelhecimento saudável em idosos residentes em centro urbano: Projeto Epidoso. São Paulo. Cadernos de Saúde Pública 19, 793–797 (2003).
Lehrer, P. et al. Heart rate variability biofeedback improves emotional and physical health and performance: A systematic review and meta analysis. Appl. Psychophysiol. Biofeedback 45, 109–129 (2020).
Anderson, C. A. & Harvey, R. J. Brief report: Discriminating between problems in living: An examination of measures of depression, loneliness, shyness, and social anxiety. J. Soc. Clin. Psychol. 6, 482–491 (1988).
Cacioppo, J. T., Cacioppo, S., Capitanio, J. P. & Cole, S. W. The neuroendocrinology of social isolation. Annu. Rev. Psychol. 66, 733–767 (2015).
Lee, S. L. et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: A 12-year population-based cohort study. The Lancet Psychiatry 8, 48–57 (2021).
Cacioppo, J. T. & Cacioppo, S. Social relationships and health: The toxic effects of perceived social isolation. Soc. Pers. Psychol. Compass 8, 58–72 (2014).
Mushtaq, R., Shoib, S., Shah, T. & Mushtaq, S. Relationship between loneliness, psychiatric disorders and physical health? A review on the psychological aspects of loneliness. J. Clin. Diagn. Res. 8, 1101 (2014).
Porges, S. W. The polyvagal perspective. Biol. Psychol. 74, 116–143 (2007).
Porges, S. W. The polyvagal theory: Phylogenetic contributions to social behavior. Physiol. Behav. 79, 503–513 (2003).
Holt-Lunstad, J. Loneliness and social isolation as risk factors: The power of social connection in prevention. Am. J. Lifestyle Med. 1, 454 (2021).
Holt-Lunstad, J. & Steptoe, A. Social isolation: An underappreciated determinant of physical health. Curr. Opin. Psychol. 1, 1 (2021).
Jester, D. J., Rozek, E. K. & McKelley, R. A. Heart rate variability biofeedback: Implications for cognitive and psychiatric effects in older adults. Aging Ment. Health 23, 574–580 (2019).
Zauszniewski, J. A. & Musil, C. M. Interventions for grandmothers: Comparative effectiveness of resourcefulness training, HRV biofeedback, and journaling. Biofeedback 42, 121–129 (2014).
Pizzoli, S. F. et al. A meta-analysis on heart rate variability biofeedback and depressive symptoms. Sci. Rep. 11, 1–10 (2021).
Burch, J. B. et al. Symptom management among cancer survivors: Randomized pilot intervention trial of heart rate variability biofeedback. Appl. Psychophysiol. Biofeedback 45, 99–108 (2020).
Bertolucci, P. H., Brucki, S., Campacci, S. R. & Juliano, Y. O mini-exame do estado mental em uma população geral: impacto da escolaridade. Arq. Neuropsiquiatr. 52, 01–07 (1994).
Rikli, R. E. & Jones, C. J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 7, 129–161 (1999).
Shepard, R. An analysis of PAR-Q responses in an office population. Can. J. Public Health 72, 37–40 (1981).
Medicine, A. C. S. Position stand on progression models in resistance training for healthy adults. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 34, 364–380 (2002).
R. Fontanive, T. P. d. Paula, W. A. F. Peres, Avaliação da composição corporal de adultos. Duarte ACG. Avaliação nutricional: aspectos clínicos e laboratoriais. São Paulo: Atheneu, 41–63 (2007).
Durnin, J. V. & Womersley, J. Body fat assessed from total body density and its estimation from skinfold thickness: Measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 32, 77–97 (1974).
Moreira, A. J., Nicastro, H., Cordeiro, R. C., Coimbra, P. & Frangella, V. S. Composição corporal de idosos segundo a antropometria. Revista Brasileira de Geriatria e Gerontologia 12, 201–213 (2009).
Nelson, H. & Geher, G. Mutual grooming in human dyadic relationships: An ethological perspective. Curr. Psychol. 26, 121–140 (2007).
Russell, D., Peplau, L. A. & Cutrona, C. E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 39, 472 (1980).
Sheikh, J. I. & Yesavage, J. A. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin. Gerontol. J. Aging Mental Health 1, 1 (1986).
Lang, P. J. International affective picture system (IAPS): Affective ratings of pictures and instruction manual. Tech. Rep. (2005).
Acknowledgements
This work was supported by the National Council for Scientific and Technological Development, Brazil (Conselho Nacional de Desenvolvimento Científico e Tecnológico—CNPq); Coordination for the Improvement of Higher Education Personnel, Brazil (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—CAPES); Research Foundation of the State of Minas Gerais (Fundação de Amparo à Pesquisa do Estado de Minas Gerais—FAPEMIG); and the Federal University of Ouro Preto—Brazil (Universidade Federal de Ouro Preto—UFOP).
Author information
Authors and Affiliations
Contributions
P.M.S wrote the manuscript draft, developed the study concept and study design, created tables, conducted data acquisition, analysed and interpreted the data and prepared all figures. M.C.S and L.A.D. conducted data acquisition, wrote the manuscript draft and critically reviewed the final manuscript. C.R.V.A. analysed and interpreted the data and critically reviewed the final manuscript. M.L; E.V.; O.F.J and T.A.S. critically reviewed the final manuscript. G.G.L.S. developed the study concept and study design, critically reviewed the final manuscript, supervised and administered the project and was responsible for funding acquisition. All authors contributed to and have approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Souza, P.M., de Cássia Souza, M., Diniz, L.A. et al. Long-term benefits of heart rate variability biofeedback training in older adults with different levels of social interaction: a pilot study. Sci Rep 12, 18795 (2022). https://doi.org/10.1038/s41598-022-22303-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-22303-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
