
Abstract
The clinical associations and prognostic implications of the 6-minute walk test (6MWT) distance in patients with rheumatoid arthritis (RA) is yet to be explored. To identify the clinical features and prognostic implications associated with the 6MWT in patients with RA. Cohort study including 387 RA patients who underwent 6MWT. Regression models (linear and logistic) were built to identify independent predictors of shorter 6MWT distance. Cox proportional models were used to study the association of 6MWT distance with cardiovascular outcomes. Patients were subdivided according to 6MWT tertiles: 126 patients walked > 405 m, 129 walked 345-405 m, and 132 walked < 345 m. Older age (> 55 years), elevated waist circumference, NT-pro BNP > 125 pg/mL, anemia, C-reactive protein ≥ 3 mg/dL, and troponin T ≥ 14 pg/mL were independent predictors of walking shorter distances. Patients walking less than 345 m had higher risk of a subsequent cardiovascular hospitalization or cardiovascular death compared with patients walking 345 m or more (adjusted HR: 2.98, 95%CI: 1.37–6.51, p = 0.006). Older age, abdominal obesity, anemia, cardiac dysfunction, and inflammation were associated with walking shorter distances in patients with RA. Walking less than 345 m in the 6MWT was associated with a poor cardiovascular prognosis. The 6MWT is simple, reproducible, and inexpensive, easily performed in routine practice, and provides important information regarding the patients´ status and outcomes, enabling the monitorization of the therapeutic optimization of the various domains of the RA.
Similar content being viewed by others

Introduction
The 6-minute walk test (6MWT) is a simple, reproducible, and inexpensive method that allows to assess patients` physical capacity1,2. The 6MWT reflects well daily physical capacity, and has shown good correlation with quality of life measures and exercise tolerance (e.g., exercise duration and oxygen uptake at the peak of exercise)3,4. Importantly, the distance walked in the 6MWT is strongly associated with prognosis in chronic cardiovascular and respiratory conditions5,6,7,8,9,10,11,12.
Data on the clinical correlations and prognostic implications of the 6MWT in patients with rheumatoid arthritis (RA) are scarce. To the best of our knowledge, to date, no study has evaluated the factors independently associated with the 6MWT distance in patients with RA nor the prognostic implications of the distance walked. Being RA a multisystemic disease, affecting not only the osteoarticular, but also the cardiovascular and respiratory systems13, the 6MWT may serve as an inexpensive tool to comprehensively assess the disease severity, symptom burden and prognosis among patients with RA.
Using a prospective cohort of patients with RA who have performed 6MWT at baseline, we aim to study the clinical correlates and the prognostic implications of the 6MWT in this population.
Results
Baseline characteristics of the patients by tertiles of 6MWT
A total of 387 patients (97% of the overall population of 399 patients) had performed a 6MWT. Among these, 126 (32.6%) walked more than 405 m, 129 (33.3%) walked between 345 and 405 m, and 132 (34.1%) walked less than 345 m. Compared with patients that walked more than 405 m, those that walked less than 345 m were older (median 67 vs. 50 years), had higher body mass index and waist circumference, more frequent dyslipidemia, history of myocardial infarction, angina pectoris, stroke, atrial fibrillation, more frequent echocardiographic alterations, dyspnea, fatigue, anxiety and depression, longer duration of RA (median 10.7 vs. 6.5 years), more frequent DAS28 above 3.2 (33.3 vs. 11.9%), poorer renal function, higher proportion of NT-pro BNP above 125 pg/mL (54.5% vs. 12.7%), more frequent troponin T above 14 pg/mL (19.7% vs. 2.4%), and C-reactive protein above 3 mg/dL (59.8 vs. 40.5%). Prescribed medications reflected the severity of the underlying disease. Compared with patients that walked more than 405 m, those that walked less than 345 m received more corticosteroids, and less ACEi/ARBs and beta-blockers. Patients who walked between 345 and 405 m had characteristics compatible with an “intermediate” risk Table 1.
Factors independently associated with less distance walked in the 6MWT
In multivariable stepwise linear regression models, the factors independently associated with walking less in the 6MWT were: older age (56–65 years and > 65 years vs. < 55 years), elevated waist circumference (≥ 102 cm in men and 88 cm in women), NT-pro BNP > 125 pg/mL, C-reactive protein ≥ 3 mg/dL, troponin T ≥ 14 pg/mL, and anemia (hemoglobin < 13 g/dL in men and < 12 g/dL in women) (p < 0.05 for all) Table 2. Similar factors were independently associated with walking less than 345 m in the 6MWT in multivariable stepwise logistic regression models: older age (56–65 years and > 65 years vs. < 55 years), elevated waist circumference, NT-pro BNP > 125 pg/mL, and anemia (p < 0.05 for all) Table 2.
Association of 6MWT distance and cardiovascular outcomes
Patients walking less than 345 m had the highest risk of cardiovascular events; those walking between 345 and 405 m presented a similar risk to those walking more than 405 m: HR (95%CI) 7.69 (2.69–22.0), p < 0.001 for walking < 345 m, and HR (95%CI) 1.80 (0.53–6.13), p = 0.35 for walking between 345 and 405 m, compared with > 405 m Supplemental Table 1. Patients walking less than 345 m had a three-fold higher risk of a subsequent cardiovascular event (cardiovascular hospitalization or cardiovascular death) compared with patients walking 345 m or more: adjusted HR (95%CI) 2.98 (1.37–6.51), p = 0.006 Table 3 and Fig. 1.

Kaplan–Meier failure curve comparing patients who walked less than 345 m with those who walked 345 m or more in the 6MWT. 6MWT, 6-minute walking test.
Discussion
Our study with RA patients shows that older age, abdominal obesity, elevated NT-pro BNP, c-reactive protein, troponin, and anemia were independently associated with a shorter 6MWT distance. A distance below 345 m was independently associated with poor cardiovascular outcomes. These findings suggest that in RA patients, the 6MWT reflects factors related with ageing, obesity, inflammation, heart failure and anemia, allowing a comprehensive assessment of the patient’ status and prognosis with a simple and inexpensive tool. In routine practice, performing a 6MWT may provide prognostic information and serve as an objective assessment of patients` exercise capacity, allowing a better monitorization of the clinical course of RA and related conditions. The 6MWT is a reproducible method that can be performed in most RA patients (even when exercise capacity in limited by severity of disease or multiple co-morbidities) and may provide reliable information about the patient’s daily activity.
Beyond age, which is an expected factor conditioning walking distance, patients who walked shorter distances, had higher RA activity with higher DAS28 scores and increased levels of c-reactive protein, which is a well-established marker of disease activity and radiologic progression in RA14,15. In patients with systemic sclerosis, older age and increased levels of c-reactive protein were also factors independently associated with shorter 6MWT distance16.
Anemia was a strong and independent predictor of walking shorter distances in the 6MWT. Anemia is present in 30–60% of RA patients, and it is characteristically of inflammatory origin17. Anemia may be a predictor of joint disease activity (RA patients with anemia are more likely to have severe joint disease) and structural damage18. Treating anemia may improve the functional capacity of RA patients17.
Another important comorbidity independently associated with less distance walked in the 6MWT was visceral obesity (higher waist circumference). Abdominal obesity is an independent risk marker of cardiovascular morbidity and mortality19. In RA, obesity is associated with elevated inflammatory markers, chronic pain and disability; which may explain the association between abdominal obesity with shorter distances walked as found in our study19.
As we previously reported, our RA cohort had a considerably high prevalence of heart failure (32%), which was previously under-diagnosed20. In this regard, performing a 6MWT can be used as a tool to improve HF diagnosis, as lower 6MWT distance may reflect a possible underlying HF diagnosis, as shown by the elevated NT-pro BNP and troponin levels among patients walking less than 345 m, both of which are well-established markers of cardiac dysfunction and heart failure20. Elevated troponin (although very mild elevations, as our patients had) may also indicate the possibility of ischemic heart disease, often represent underlying cardiac changes/HF and mismatch between demand/supply (and may not be due to any instable plaque) which should be sought as a cause of exercise intolerance21.
The association of the 6MWT distance with higher rates of cardiovascular events is noteworthy, because the 6MWT is an inexpensive and easy to perform test that can provide important prognostic information. This evidences justifies moving forward with prospective and interventional work in the prevention and treatment of cardiovascular risk in patients who have T6MM below 345 m. The 6MWT reflects exercise tolerance, which can be limited by several cardiovascular and non-cardiovascular factors such as cardiac as respiratory diseases, osteoarticular pathology, obesity, physical conditioning, and/or willingness/motivation to perform the test. In addition, the 6MWT also relies on the ability of skeletal muscle to extract oxygen from blood, which may also have prognostic impact22.
In the future, 6MWT can be used as a follow-up tool—for the treatment of RA and its comorbidities, such as obesity, anemia or HF, and also to measure the impact of improving outcomes.
In summury. the 6MWT is simple, reproducible, and inexpensive, easily performed in routine practice, and provides important information regarding the patients´ status and outcomes, enabling the monitorization of the therapeutic optimization of the various domains of the RA.
Several limitations should be acknowledged in our study. This is an observational study and the associations with 6MWT were cross-sectional, thus causality cannot be ascertained. Other relevant determinants of exercise capacity, such as skeletal muscle abnormalities and non-physiologic factors, including patient motivation and investigator encouragement could play an important role and were not available. The small number of cases resulting in hard CV outcomes requires caution in interpreting models with many numbers of variables. Our cohort came from a single center and some of the findings may reflect specific socio-demographic characteristics and local practice patterns which may limit the generalization of the findings. Finally, we did not perform the Time Up and Go or Grip Strength tests in our study, which would also be inexpensive and easy to perform, and could have provided important clinical and prognostic information. Further studies should assess the prognostic value of such tests in patients with RA.
Methods
Study design
We conducted a prospective single-center cohort study with patients attending the Autoimmune Disease Outpatient Unit of Centro Hospitalar do Porto, Portugal. The study was registered in clinicaltrials.gov under the number NCT0396051520.
Patient selection
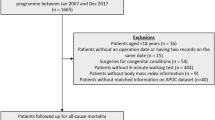
We considered for inclusion all adult patients (18 years or older) with a diagnosis of RA and that were followed-up in our specialized RA clinic. The RA was diagnosed using the 2010 ACR/EULAR Classification Criteria23. All patients presenting an active neoplasm or other severe co-morbid condition potentially associated with a life expectancy shorter than six months, as well as severe dementia, inability to walk or totally dependent on a third person were excluded from our study.
The screening period for the patient enrollment occurred from June 2016 to June 2018. All enrolled patients maintained their usual care under the guidance of their treating physician.
A total of 399 were initially studied, but only patients who underwent 6MWT were included in the study and were followed-up for a median of 1.5 (0.7–2.3) years. The cause of death and hospitalization were independently adjudicated.
Patient evaluation, echocardiography, and routine laboratory tests
We collected demographic data, cardiovascular history and risk factors, comorbid conditions, RA history, daily medication intake and a cardiovascular symptom questionnaire. Physical examination included vital signs, pulmonary and cardiac auscultation, and anthropometric measures. Transthoracic echocardiogram (TTE) was performed by an experienced echocardiographer and included the M-mode, 2D and Doppler measurements acquired according to standard recommendations24,25. Routine laboratory tests included a complete blood count, c-reactive protein, glucose, blood electrolytes, lipid profile, creatinine, high sensitivity troponin T (Elecsys Roche Diagnostics®), and N-Terminal-pro Brain Natriuretic Peptide (NT-pro BNP; Elecsys Roche Diagnostics®).
6-Minute walk test
Six-minute walking test was performed according to the American Thoracic Society protocol26, in a long, straight hospital corridor, over a 30-m distance. Each participant was asked to walk (not run) back and forth along the corridor as briskly as possible, so that the longest possible distance was covered in 6 min. The participant could slow down or stop and rest if necessary, particularly in the case of symptoms such as severe dyspnea or fatigue. During any rest period, the participant was informed of the elapsed time and encouraged to recommence walking when symptoms subsided sufficiently. The participant could discontinue the test at any time. Moreover, the test was interrupted by the investigator immediately if one of the following symptoms appeared: chest pain, severe dyspnea, severe claudication, loss of balance, severe sweating, pallor, or cyanosis. Otherwise, every two minutes during the test, the investigator informed the participant of the amount of time left and encouraged them to continue the test. At 6 min, the participant was advised to stop and sit down. The distance walked was measured in meters (m) to the nearest whole metre.
Statistical analysis
Sample description and comparison of the 6MWT according to tertiles was performed using Chi-square and Kruskal–Wallis tests, as appropriate. Continuous variables are presented by median (interquartile range) and categorical by absolute and relative frequency. Single imputation using median was used to deal with missing data. All variables with a P-value of less than 0.05 in the univariable analysis (Table 1) were entered in a stepwise (forward) model with a P-value of less than 0.05 set for a variable to enter and stay in the final model. Using this procedure, we performed a multivariable linear regression model using 6MWT distance as a continuous variable (per each minus 10 m walked) and a logistic regression model (using the lowest tertile distance as outcome of interest). Cox proportional hazard regression models and Kaplan–Meier curves were used to study the association of 6MWT distance with cardiovascular outcomes, a composite of time-to-first cardiovascular death or cardiovascular hospitalization. The covariates used for adjustment where those from the final multivariable models. All the analyses were performed using STATA® (StataCorp. 2019. Stata Statistical Software: Release 16.1. College Station, TX: StataCorp LP). A P-value < 0.05 was considered as statistically significant.
Ethical approval and consent to participate
This study was conducted following the principles of the Declaration of Helsinki and approved by the Hospital de Santo António, Porto, Portugal ethics committee under number #2016-023 (020-DEFI/020-CES). All participants provided the written informed consent before enrollment in the study. The data used for this study are available upon reasonable request to the corresponding author.
Data availability
The authors state they have full control of all primary data and agree to allow the journal to review their data after reasonable request.
Abbreviations
- 6MWT:
-
6-Minute walk test
- RA:
-
Rheumatoid Arthritis
- ACR/EULAR:
-
American College of Rheumatology/European League Against Rheumatism
- NT-pro BNP:
-
N-Terminal-pro Brain Natriuretic Peptide
- TTE:
-
Transthoracic echocardiogram
- HF:
-
Heart Failure
- ACEi/ARBs:
-
Angiotensin converting enzyme inhibitors/angiotensin receptor blockers
- DAS28:
-
Disease Activity Score 28
References
Faggiano, P., D’Aloia, A., Gualeni, A., Brentana, L. & Dei, C. L. The 6 minute walking test in chronic heart failure: Indications, interpretation and limitations from a review of the literature. Eur. J. Heart Fail. 6(6), 687–691 (2004).
Ingle, L. et al. The reproducibility and sensitivity of the 6-min walk test in elderly patients with chronic heart failure. Eur. Heart J. 26(17), 1742–1751 (2005).
Lipkin, D. P., Scriven, A. J., Crake, T. & Poole-Wilson, P. A. Six minute walking test for assessing exercise capacity in chronic heart failure. Br. Med. J. (Clin. Res. Ed.) 292(6521), 653–655 (1986).
Ingle, L., Goode, K., Rigby, A. S., Cleland, J. G. & Clark, A. L. Predicting peak oxygen uptake from 6-min walk test performance in male patients with left ventricular systolic dysfunction. Eur. J. Heart Fail. 8(2), 198–202 (2006).
Bittner, V. et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction, SOLVD Investigators. JAMA 270(14), 1702–1707 (1993).
Ingle, L., Cleland, J. G. & Clark, A. L. The relation between repeated 6-minute walk test performance and outcome in patients with chronic heart failure. Ann. Phys. Rehabil. Med. 57(4), 244–253 (2014).
Wegrzynowska-Teodorczyk, K. et al. Distance covered during a six-minute walk test predicts long-term cardiovascular mortality and hospitalisation rates in men with systolic heart failure: an observational study. J. Physiother. 59(3), 177–187 (2013).
Ferreira, J. P. et al. Natriuretic peptides, 6-min walk test, and quality-of-life questionnaires as clinically meaningful endpoints in HF trials. J. Am. Coll. Cardiol. 68(24), 2690–2707 (2016).
Ferreira, J. P. et al. Clinical correlates and outcome associated with changes in 6-minute walking distance in patients with heart failure: findings from the BIOSTAT-CHF study. Eur. J. Heart Fail. 21(2), 218–226 (2019).
Waatevik, M. et al. One year change in 6-minute walk test outcomes is associated with COPD prognosis. COPD 17(6), 662–671 (2020).
Blanco Pérez, J. J. et al. The 6-minute walk test as a tool for determining exercise capacity and prognosis in patients with silicosis. Arch. Bronconeumol. 55(2), 88–92 (2019).
Farber, H. W. et al. Predicting outcomes in pulmonary arterial hypertension based on the 6-minute walk distance. J. Heart Lung Transplant. 34(3), 362–368 (2015).
Turesson, C., O’Fallon, W. M., Crowson, C. S., Gabriel, S. E. & Matteson, E. L. Extra-articular disease manifestations in rheumatoid arthritis: Incidence trends and risk factors over 46 years. Ann. Rheum. Dis. 62(8), 722–727 (2003).
Otterness, I. G. The value of C-reactive protein measurement in rheumatoid arthritis. Semin. Arthritis Rheum. 24(2), 91–104 (1994).
Sattar, N., McCarey, D. W., Capell, H. & McInnes, I. B. Explaining how “high-grade” systemic inflammation accelerates vascular risk in rheumatoid arthritis. Circulation 108(24), 2957–2963 (2003).
Sanges, S. et al. Factors associated with the 6-minute walk distance in patients with systemic sclerosis. Arthritis Res Ther. 19(1), 279 (2017).
Wilson, A., Yu, H. T., Goodnough, L. T. & Nissenson, A. R. Prevalence and outcomes of anemia in rheumatoid arthritis: A systematic review of the literature. Am. J. Med. 116(Suppl 7A), 50S-57S (2004).
Chen, Y. F. et al. Inflammatory anemia may be an indicator for predicting disease activity and structural damage in Chinese patients with rheumatoid arthritis. Clin. Rheumatol. 39(6), 1737–1745 (2020).
Neeland, I. J. et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 7(9), 715–725 (2019).
Ferreira, M. B. et al. Prevalence, risk factors and proteomic bioprofiles associated with heart failure in rheumatoid arthritis: The RA-HF study. Eur. J. Intern. Med. 85, 41–49 (2020).
Apple, F. S. et al. Validation of the 99th percentile cutoff independent of assay imprecision (CV) for cardiac troponin monitoring for ruling out myocardial infarction. Clin. Chem. 51, 2198–2200 (2005).
Middlekauff, H. R. Making the case for skeletal myopathy as the major limitation of exercise capacity in heart failure. Circ. Heart Fail. 3(4), 537–546 (2010).
Villeneuve, E., Nam, J. & Emery, P. 2010 ACR-EULAR classification criteria for rheumatoid arthritis. Rev. Bras. Reumatol. 50(5), 481–483 (2010).
Lang, R. M. et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging. 16(3), 233–270 (2015).
Lang, R. M. et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 28(1), 1–39 (2015).
Laboratories ATSCoPSfCPF. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 166(1), 111–117 (2002).
Funding
UIDB/00215/2020; UIDP/00215/2020; LA/P/0064/2020. F.A. Saraiva was supported by Universidade do Porto/FMUP and FSE-Fundo Social Europeu, NORTE 2020-Programa Operacional Regional do Norte, NORTE-08–5369-FSE-000024-Programas Doutorais.
Author information
Authors and Affiliations
Contributions
J.P.F., performed the statistical analysis and drafted the manuscript; M.B.F. drafted the manuscript; F.A.S. performed statistical analysis; F.A.S., T.F., R.C., A.M., J.O., H.C. and P.R. provided critical input and approved the final version of the manuscript. J.P.F. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ferreira, M.B., Saraiva, F.A., Fonseca, T. et al. Clinical associations and prognostic implications of 6-minute walk test in rheumatoid arthritis. Sci Rep 12, 18672 (2022). https://doi.org/10.1038/s41598-022-21547-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-21547-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
