
Abstract
In this study, the accuracy of the positional relationship of the contact between the inferior alveolar canal and mandibular third molar was evaluated using deep learning. In contact analysis, we investigated the diagnostic performance of the presence or absence of contact between the mandibular third molar and inferior alveolar canal. We also evaluated the diagnostic performance of bone continuity diagnosed based on computed tomography as a continuity analysis. A dataset of 1279 images of mandibular third molars from digital radiographs taken at the Department of Oral and Maxillofacial Surgery at a general hospital (2014–2021) was used for the validation. The deep learning models were ResNet50 and ResNet50v2, with stochastic gradient descent and sharpness-aware minimization (SAM) as optimizers. The performance metrics were accuracy, precision, recall, specificity, F1 score, and area under the receiver operating characteristic curve (AUC). The results indicated that ResNet50v2 using SAM performed excellently in the contact and continuity analyses. The accuracy and AUC were 0.860 and 0.890 for the contact analyses and 0.766 and 0.843 for the continuity analyses. In the contact analysis, SAM and the deep learning model performed effectively. However, in the continuity analysis, none of the deep learning models demonstrated significant classification performance.
Similar content being viewed by others
Introduction
Third molar extraction is the most common surgery performed by dentists and maxillofacial surgeons. The mandibular third molar has more complications than the maxillary third molar, including post-extraction infection, postoperative pain, and inferior alveolar nerve damage1,2. Among these complications, inferior alveolar nerve damage should be avoided because it stresses patients for a prolonged period.
In clinical practice, panoramic radiographs are generally used to determine the difficulty of the mandibular third molar, including the contact with the inferior alveolar nerve, depth of the mandibular third molar, and distance to the mandibular ramus. If contact between the inferior alveolar canal and mandibular third molar is suspected after the panoramic screening, computed tomography (CT) is used to identify defects in the cortical bone around the inferior alveolar nerve. The cortical bone defects are significantly risky for postoperative inferior alveolar nerve damage3. Accurately determining the positional relationship between the inferior alveolar nerve and the mandibular third molar with a two-dimensional panoramic radiograph is difficult, but preoperative diagnosis using CT in 3D is very effective4. Although CT cannot directly image the nerve, it can clarify the positional relationship between the tooth and the nerve by depicting the inferior alveolar nerve and the bony border5. However, CT imaging cannot be applied in all cases owing to radiation exposure and high cost6. Therefore, developing an assistant diagnostic tool to diagnose the contact relationship with the inferior alveolar nerve from panoramic radiograph images is essential.
Convolutional neural networks (CNN) have revolutionized deep learning in recent years. CNN-based classifiers have proved highly accurate for image recognition7 and have consequently impacted diagnostic imaging in the medical field. They have been applied to the detection of lung cancer from chest X-ray images8, determination of retinal detachment9, detection of osteoporosis10, screening of breast cancer11, etc. In addition, many deep learning-related studies have been reported in the field of dentistry, and classifiers have been developed for areas such as caries12, periapical lesions13, dental implants14, maxillary sinusitis15, and position classification of the mandibular third molars16. Furthermore, deep learning has occasionally been more accurate than human diagnosis17,18. In contact analysis using deep learning, Fukuda et al.19 examined images of different sizes and reported that the results were more accurate when the images were small and condensed only to those that required a large amount of information. Thus, deep learning diagnostic imaging has great potential and must be explored. We therefore hypothesized that deep learning could accurately diagnose the positional relationship between the mandibular third molar and inferior alveolar nerve on panoramic radiographs.
This study aimed to explain the accuracy of the positional relationship of the contact between the inferior alveolar canal and the mandibular third molar using deep learning. To this end, in this CNN deep learning-based study, we first investigated the diagnostic performance of the presence or absence of contact between the mandibular third molar and inferior alveolar canal. Subsequently, we explored the diagnostic performance of bone continuity between the mandibular third molar and inferior alveolar canal, diagnosed using CT.
Materials and methods
Study design
This study analyzed the diagnostic performance of the positional relationship between the inferior alveolar canal/nerve and the mandibular third molar from panoramic radiographs using an optimized CNN deep learning model.
Ethics statement
This study was approved by the Institutional Review Board of Kagawa Prefectural Central Hospital (approval number: 1023; approval date: 8th March 2021). The board reviewed our retrospective non-interventional study design and analytical study with anonymized data and waived written documentation of personal informed consent. All methods were performed following the relevant guidelines and regulations. The study was registered at jRCT (jRCT1060220021).
Preparation of image datasets
We retrospectively used radiographic imaging data collected at the Department of Oral and Maxillofacial Surgery in a single general hospital from April 2014 to December 2021. The study data included patients aged 20–76 years in the mature mandibular third molar who had panoramic radiographs and CT taken on the same day. This study confirms the positional relationship between the mandibular third molar and the inferior alveolar canals by panoramic radiography. An unclear image (three teeth) and an image of the remaining titanium plate after the mandibular fracture (one tooth) were excluded. Finally, 1279 tooth images were used in this study.
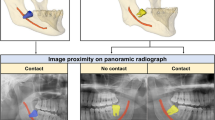
Digital image data were obtained using dental panoramic radiographs taken with either of the two imaging devices (AZ3000CMR or Hyper-G CMF; ASAHIRENTOGEN Ind. Co., Ltd., Kyoto, Japan). All digital image data were output in a tagged image file format (digital image size: 2776 × 1450, 2804 × 1450, 2694 × 1450, or 2964 × 1464 pixels) using the Kagawa Prefectural Central Hospital Picture Archiving and Communication Systems system (Hope Dr. Able-GX, Fujitsu Co., Tokyo, Japan). Under the supervision of an expert oral and maxillofacial surgeon, two oral and maxillofacial surgeons used Photoshop Elements (Adobe Systems, Inc., San Jose, CA, USA) to crop the areas of interest manually. The image was cropped by selecting the area, including the apex of the mandibular third molar and the inferior alveolar canal within 250 × 200 pixels (Fig. 1). Each cropped image had a resolution of 96 dpi and was saved in the portable network graphic format.

Classification of the relationship between the mandibular third molar and inferior alveolar canal/nerve.
Classification of mandibular third molar and inferior alveolar nerve
First, using panoramic radiographs, we classified the contact and superimposition between the mandibular third molar and inferior alveolar canal. This is because contact between the inferior alveolar duct on panoramic radiographs is a risk factor for nerve exposure4,20.
Second, we classified the presence or absence of direct contact between the mandibular third molar and inferior alveolar nerve using CT. The classification criteria and distributions are as follows and are also shown in Fig. 1.
-
1.
Relationship between the mandibular third molar and inferior alveolar canal.
-
(a)
Non-contact or superimposition of the mandibular third molar and inferior alveolar canal.
-
(b)
Contact or superimposition between the mandibular third molar and the inferior alveolar canal.
-
(a)
In this study, contacts and superimposition/overlaps were grouped together.
-
2.
Relationship between the mandibular third molar and inferior alveolar nerve.
If there was discontinuity of the cortical bone at the inferior alveolar canal due to the mandibular third molar, it was classified as a defect.
-
(a)
Contact between the mandibular third molar and inferior alveolar nerve (i.e., defect or discontinuity in the cortical bone of the inferior alveolar canal).
-
(b)
Non-contact between the mandibular third molar and inferior alveolar nerve (i.e., continuity of the cortical bone of the inferior alveolar canal).
CNN model architecture
ResNet50 is a 50-layer deep CNN model. Traditional CNNs have the major drawback of the “vanishing gradient problem,” where the gradient value is significantly reduced during backpropagation, resulting in little weight change. The ResNet CNN model uses a residual module to overcome this problem21. ResNet v2 is an improved version of the original ResNet22, with the following improvements compared with the original ResNet (Fig. 2): (1) The shortcut path is completely identity mapped without using the ReLU between the input and output. (2) After branching for the residual calculation, the order is changed to batch normalization23 as -ReLU-convolution-batch normalization-convolution.

Differences between the residual blocks of ResNet and ResNetv2: (a) ResNet Residual Unit; (b) ResNetv2 Residual Unit. BN: Batch Normalization and Conv2D: Two-dimensional convolution layer.
In this study, we selected two CNN models, ResNet50 and ResNet50v2. The ResNet50 and ResNet50v2 CNN models were pre-trained on the ImageNet database and fine-tuned according to the positional relationship classification task for the mandibular third molar and inferior alveolar nerve. The deep learning task process was implemented using Python (version 3.7.13), Keras (version 2.8.0), and TensorFlow (version 2.8.0).
Dataset and CNN model training
Each CNN model training was generalized using K-fold cross-validation in the deep learning algorithm. The models were validated using tenfold cross-validation to ensure internal validity. The digital image dataset was divided into ten random subsets using the stratified sampling technique, and the same classification distribution was maintained for training, validation, and testing across all subsets24. The dataset was split into separate test and training datasets in a ratio of 0.1–0.9 within each fold. Additionally, the validation data comprised one-tenth of the training dataset. The model averaged ten training iterations to obtain prediction results for the entire dataset, with each iteration retaining a different subset for validation.
The cross-entropy—defined by Eq. (1)—was used for the loss function.
where ti is true label and yi is the predicted probability of class i.
Optimization algorithm
This study used two deep learning gradient methods, stochastic gradient descent (SGD) and sharpness-aware minimization (SAM). SGD is a typical optimization method in which the parameters are updated by the magnitude in the obtained gradient direction. The momentum SDG is a method of adding momentum to SGD25. In this study, the momentum was set to 0.9. The momentum SGD is expressed in Eqs. (2) and (3).
where w_t is t-th parameter, η is learning rate, ∇L (w) is differentiation with parameters of the loss function, and α is momentum.
SAM is an optimization method that converges to a parameter with minimal loss and flat surroundings26. It uses a combination of a base optimizer and SAM to determine the final parameters using traditional algorithms. SGD was selected as the base optimizer. The loss function of SAM is defined by Eq. (4). This is used to minimize Eq. (5).
where S is the set of data, w is a parameter, λ is the L2 regularization coefficient, L_s is the loss function, and ρ is the neighborhood size.
This study analyzed the deep learning models using a ρ value of 0.025.
Deep learning procedure
Data augmentation
Data augmentation prevents excessive adaptation to the training data by diversifying the input data27. The following values were selected for the preprocessing layer to convert the images during training randomly. The boundary surface of the missing part was complemented by folding back using the reflect method.
-
Random rotation: range of − 18° to 18°
-
Random flip: horizontally and vertically
-
Random translation: up–down and left–right range of 30%
Learning rate scheduler
Learning rate decay is a technique used to improve the generalization performance of deep learning and reduce the learning rate from a state in which learning has progressed to some extent. Decay in the learning rate can improve accuracy21. The changes due to time-based decay as a learning rate can be found in the appendix. The learning rate decay can be evaluated using Eq. (6).
The learning rate scheduler was executed with an initial learning rate of 0.01 and a decay rate of 0.001. All the models conducted analysis over 300 epochs and with 32 batch sizes without early stopping. These deep learning processes were repeated 30 times for all models using different random seeds for each analysis.
Performance metrics and statistical analysis
To evaluate the performance of each deep learning model, the accuracy, precision, recall, F1 score, and area under the curve (AUC)—calculated from the receiver operating characteristic (ROC) curve—performance metrics were employed. More detailed information on the performance metrics used in this study is present in the Appendix.
Statistical evaluations of the performance for each deep learning model were performed on the data that were independently and repeatedly analyzed 30 times. Data were recorded and stored in an electronic database using Microsoft Excel (Microsoft Inc., Redmond, WA, USA). The database was created and analyzed by using JMP Statistical Software Package Version 14.2.0 for Macintosh (SAS Institute Inc., Cary, NC, USA). All statistical analyses were bilateral with a significance level of 0.05. Normal distribution was evaluated by using the Shapiro–Wilk test. A comparison of classification performance between each CNN model was performed for each metric by using the Wilcoxon signed rank sum test. Effect sizes28 were evaluated using Hedges' g (unbiased Cohen's d), Eqs. (7) and (8).
where M1 and M2 are the mean values for the CNN models with SGD and SAM, s1 and s2 are the standard deviations for the CNN models with SGD and SAM, respectively; and n1 and n2 are the numbers for the CNN models with SGD and SAM, respectively. Effect sizes were categorized as large effect, ≥ 2.0; very large effect, 1.0; large effect, 0.8; medium effect, 0.5; small effect, 0.2; and very small effect, 0.01 based on the criteria proposed by Cohen and extended by Sawilowsky29.
Visualization of judgment regions in deep learning
In this study, the gradient-weighted class activation map (Grad-CAM) algorithm30 was used to visualize the noticeable areas of the image in a heatmap. Grad-CAM is a class activation mapping method that uses gradients for weights adopted by the IEEE International Conference on Computer Vision in 2017 and provides a visual basis for deep learning to improve the explanation of the architecture. Grad-CAM uses the last convolution layer of the ResNet model to visualize the feature area.
Results
Performance metrics of ResNet50 and ResNet50v2 in the SAM and SGD optimizers
Table 1 shows the results of the performance metrics of ResNet50 and ResNet50v2 with the SAM and SGD optimizers in the contact analysis. In the contact analysis of the inferior alveolar canal and mandibular third molar on panoramic radiographic images, ResNet 50v2 using the SAM optimizer showed the highest performance on all performance metrics (Accuracy: 0.860, Precision: 0.816, Recall: 0.791, F1 score: 0.800, and AUC: 0.890).
Table 2 shows the results of the performance metrics of ResNet50 and ResNet50v2 with the SAM and SGD optimizers in the continuity analysis. In the continuity analysis of the inferior alveolar nerve and mandibular third molar on panoramic radiographic images, ResNet50v2 using the SAM optimizer showed the highest performance on all performance metrics and contact analysis (Accuracy: 0.766, Precision: 0.766, Recall: 0.765, F1 score: 0.775, and AUC: 0.843).
Statistical evaluation of performance metrics in each CNN model
Tables 3 and 4 show the statistical evaluation results of both CNN models for each performance metric. Contact and continuity analyses yielded symmetrical results. For the contact analysis results shown in Table 3, both ResNet50 and ResNet50v2 exhibited statistically significant differences on all performance metrics for SAM and SGD. AUC and accuracy for ResNet50 showed the highest effect size equivalent to “very large” using SAM. The comparison of ResNet50v2 and ResNet50 using SAM showed a statistically significantly higher performance for ResNet50v2 on all performance metrics.
For the continuity analysis shown in Table 4, neither ResNet50 nor ResNet50v2 demonstrated a statistically significant difference on any performance metric when comparing SAM and SGD. The effect size was “small” to “very small” for ResNet50. Conversely, a comparison of ResNet50v2 and ResNet50 using SAM demonstrated a statistically higher performance for ResNet50v2 on all performance metrics, and all effect sizes also showed “very large” to “huge.”
Comparison of the learning curves of the CNN models
Figure 3 shows the learning curve for each CNN deep learning model. In the contact analysis, SGD exhibited a tendency for overfitting with increasing epochs, whereas for the CNN model with SAM, SAM exhibited low overfitting. Interestingly, continuity analysis also demonstrated overfitting for the CNN models using SAM.

Learning curves for each CNN model in contact and continuity analyses.
Visualization of model classification by Grad-CAM
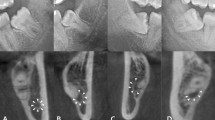
Figure 4 shows the visualization of the area of interest for classification decisions in each deep learning model in the contact and continuity analyses. In the ResNet50 and ResNet50v2-based CNN models, Grad-CAM visualized the final layer of the convolutional layer or the feature area using a heat map. There was no significant difference in the feature areas indicated by the Grad-CAM in contact and continuity analyses. The point of contact between the inferior alveolar canal and mandibular third molar or the closest part was determined to be the characteristic area. This area of interest was the same as the dentist's judgment. In the heatmap visualization using Grad-CAM, the warmer the color, the more significant the contribution to feature determination.

Visualization of regions of interest for CNN classification in contact and continuity analyses.
Discussion
In this study, we analyzed deep learning models using contact and continuity analyses to classify the positional relationship of the inferior alveolar canal. The CNN model demonstrated a high performance in contact analysis. The CNN model using SAM as the optimizer for ResNet 50v2 exhibited the highest performance. However, in the continuity analysis, none of the CNN models showed high classification performance. This study focused on the part in contact with the inferior alveolar canal and mandibular third molar and obtained a high classification performance using CNN models. However, some cases have been misclassified due to the tooth-like sclerotic area between the teeth and the inferior alveolar canal, and the cropped images made it difficult to identify the inferior alveolar canal. Therefore, optimized data collection is required for contact analysis.
In general, as CT and MRI can provide three-dimensional (3D) information, it is possible to accurately determine the positional relationship between the lower alveolar canal and the mandibular third molar by comparing it with a panoramic image31. Analysis using deep learning was performed to determine the 3D positional relationships from panoramic images without using other imaging devices. In continuity analysis, although it is difficult to simply compare performance in deep learning studies conducted on different data, a deep learning classification study conducted on 571 images by Choi et al. reported a classification accuracy of 0.72332. The accuracy of the deep learning model in this study was 0.766, which is almost the same as the classification accuracy. In addition, the diagnostic accuracy of specialists was 0.55–0.72 (average 0.63), and it was difficult for even specialists to evaluate the continuity between the inferior alveolar nerve and the mandibular third molar using only panoramic radiographic images. The diagnostic accuracy of deep learning is also equivalent to the highest value among specialists, suggesting CNN models cannot improve the breakthrough diagnosis of continuity.
SGD identifies a point that minimizes the loss function. Although the loss function becomes small, the peripheral optimization parameters become nonuniform. This leads to overfitting and reduced generalization performance. In contrast, in SAM, the loss function is designed to search for flat parameters. Therefore, the values around the selected parameters also exhibited a uniformly low loss function. It improves the generalization performance and robustness against noise. In this study, SGD showed a tendency for overfitting in the contact analysis in comparison to SAM. By contrast, the continuity analysis showed a trend to overfit even in the CNN model using SAM. This is probably due to inconsistencies between the image data and the correct label. In other words, it suggests that even with the deep learning method, it was not possible to identify the absolute feature showing continuity of the inferior alveolar canals. This is the first study to analyze the relationship between the inferior alveolar nerve and mandibular third molars using SAM. The findings of this study will contribute to the development of deep learning in dentistry in the future.
The characteristics of ResNet, a derivative of ResNet50, are (1) input batch normalization and ReLU activation before the convolution operation and (2) nonlinearity creation as an identity mapping. In other words, the output of the additive operation between the identity mapping and residual map can be passed directly to the next block for further processing to facilitate the propagation of information. In this study, the learning curve of ResNet50v2 exhibited a more stable learning process than that of ResNet50. In addition, ResNet50v2 showed a statistically significant improvement in performance metrics in both the contact and continuity analyses, demonstrating that it is an optimal CNN model.
One problem with deep learning is that the inference process for the input data is a black box and the reason for extracting the features cannot be explained. Model output explanation has been proposed as an approach for explainable artificial intelligence33, to explain the rationale for predicting the output of deep learning. Grad-CAM and guided Grad-CAM are class activation mapping methods that use gradients and are often used in deep learning of medical images34,35. In the Grad-CAM used in this study, the focus area was the contact between the inferior alveolar canal and the mandibular third molar or the closest site in both the contact and continuity analyses. In other words, it is likely that learning is possible with an understanding of the exact feature area. However, it is difficult to understand the characteristic areas at more detailed points, such as the defect of the cortical bone on the upper wall of the inferior alveolar canal. Thus, further research is required to examine the approach of explainable AI with guided backprop36.
This study has several strengths. First, we analyzed the positional relationship between the inferior alveolar canal and the mandibular third molar using panoramic radiographs. We evaluated the continuity of the inferior alveolar canal with contact and CT findings as correct labels from the panoramic radiograph findings. This study was the first to use the same image to determine the ability to classify positional relationships using panoramic radiographs as screening and determine whether to classify the position of the inferior alveolar nerve in three dimensions as a potential evaluation of deep learning. Second, this study is the first to introduce effect size as a statistical evaluation method for the performance metrics of each CNN model that analyzes the positional relationship between the inferior alveolar canal and mandibular third molar. The effect size indicates effectiveness of an analytical operation and the strength of the association between each variable37. Therefore, the detected effect size is an essential prior parameter to help estimate the sample size in studying the relationship between the inferior alveolar canal and mandibular third molar using deep learning.
This study had two limitations. The first is that the data were collected from a single facility and were not validated externally. Internal validity was evaluated using confidence intervals from the dataset via mutual validations. However, to satisfy the external validity criterion, more data must be used in multicenter joint research. The second is the use of only two CNN models. In this study, we analyzed the data using ResNet50 and ResNet50v2. By examining previously published CNN and original CNN models, it may be possible to identify a better model for classifying the relationship between the inferior alveolar canal and the mandibular third molar.
Conclusions
In this study, we investigated the effects of a deep learning model using contact and continuity analyses to classify the positional relationship of the inferior alveolar canal. Contact analysis classified the presence or absence of contact with the mandibular third molar on panoramic radiographs, and continuity analysis classified the presence or absence of bone continuity in the inferior alveolar canal on CT images. CNN models showed a high performance in contact analysis. The CNN deep learning model using SAM as the optimizer for ResNet50v2 exhibited the highest performance. However, the continuity analysis did not show high classification performance. These results indicate that deep learning plays a vital role in primary screening using panoramic radiographs to evaluate the positional relationship between the inferior alveolar canal and the mandibular third molar. However, further studies are needed on deep learning to replace CT imaging for 3D evaluation.
Data availability
The image data are not publicly available due to privacy. The other statistical data in this study are available on request from the corresponding author.
References
Mendes, M. L. T., DoNascimento-Júnior, E. M., Reinheimer, D. M. & Martins-Filho, P. R. S. Efficacy of proteolytic enzyme bromelain on health outcomes after third molar surgery. Systematic review and meta-analysis of randomized clinical trials. Medicina Oral Patologia Oral Cirugia Bucal 24, 61–69 (2019).
Sukegawa, S. et al. What are the risk factors for postoperative infections of third molar extraction surgery: A retrospective clinical study? Med. Oral Patol. Oral Cir. Bucal 24, e123–e129 (2019).
Su, N. et al. Predictive value of panoramic radiography for injury of inferior alveolar nerve after mandibular third molar surgery. J. Oral Maxillofac. Surg. 75, 663–679 (2017).
Reia, V. C. B. et al. Diagnostic accuracy of CBCT compared to panoramic radiography in predicting IAN exposure: A systematic review and meta-analysis. Clin. Oral Invest. 25, 4721–4733 (2021).
Valdec, S. et al. Comparison of preoperative cone-beam computed tomography and 3D-double echo steady-state MRI in third molar surgery. J. Clin. Med. 10, 4768 (2021).
Bell, G. W. Use of dental panoramic tomographs to predict the relation between mandibular third molar teeth and the inferior alveolar nerve: Radiological and surgical findings, and clinical outcome. Br. J. Oral Maxillofac. Surg. 42, 21–27 (2004).
Krizhevsky, A., Sutskever, I. & Hinton, G. E. ImageNet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 25, 84 (2012).
Hong, W. et al. Deep learning for detecting pneumothorax on chest radiographs after needle biopsy: Clinical implementation. Radiology https://doi.org/10.1148/radiol.211706 (2022).
Ohsugi, H., Tabuchi, H., Enno, H. & Ishitobi, N. Accuracy of deep learning, a machine-learning technology, using ultra-wide-field fundus ophthalmoscopy for detecting rhegmatogenous retinal detachment. Sci. Rep. 7, 1 (2017).
Yamamoto, N. et al. Effect of patient clinical variables in osteoporosis classification using hip x-rays in deep learning analysis. Med. 57, 846 (2021).
Aboutalib, S. S. et al. Deep learning to distinguish recalled but benign mammography images in breast cancer screening. Clin. Cancer Res. 24, 5902–5909 (2018).
Bayrakdar, I. S. et al. Deep-learning approach for caries detection and segmentation on dental bitewing radiographs. Oral Radiol. https://doi.org/10.1007/s11282-021-00577-9 (2021).
Lee, J. H., Kim, D. H. & Jeong, S. N. Diagnosis of cystic lesions using panoramic and cone beam computed tomographic images based on deep learning neural network. Oral Dis. 26, 152–158 (2020).
Sukegawa, S. et al. Deep neural networks for dental implant system classification. Biomolecules 10, 1–13 (2020).
Mori, M. et al. A deep transfer learning approach for the detection and diagnosis of maxillary sinusitis on panoramic radiographs. Odontology 109, 941–948 (2021).
Sukegawa, S. et al. Evaluation of multi-task learning in deep learning-based positioning classification of mandibular third molars. Sci. Rep. 12, 1 (2022).
Haggenmüller, S. et al. Skin cancer classification via convolutional neural networks: Systematic review of studies involving human experts. Eur. J. Cancer 156, 202–216 (2021).
Shen, J. et al. Artificial intelligence versus clinicians in disease diagnosis: Systematic review. JMIR Med. Inform. 7, e10010 (2019).
Fukuda, M. et al. Comparison of 3 deep learning neural networks for classifying the relationship between the mandibular third molar and the mandibular canal on panoramic radiographs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 130, 336–343 (2020).
Matzen, L. H., Petersen, L. B., Schropp, L. & Wenzel, A. Mandibular canal-related parameters interpreted in panoramic images and CBCT of mandibular third molars as risk factors to predict sensory disturbances of the inferior alveolar nerve. Int. J. Oral Maxillofac. Surg. 48, 1094–1101 (2019).
He, K., Zhang, X., Ren, S. & Sun, J. Deep residual learning for image recognition. https://doi.org/10.48550/arxiv.1512.03385 (2015).
He, K., Zhang, X., Ren, S. & Sun, J. Identity mappings in deep residual networks. In: Computer Vision—ECCV 2016. ECCV 2016 (eds. Leibe, B., Matas, J., Sebe, N., Welling, M.), Vol. 9908, Lecture Notes in Computer Science (Springer, Cham, 2016). https://doi.org/10.1007/978-3-319-46493-0_38.
Ioffe, S. & Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. https://doi.org/10.48550/arxiv.1502.03167 (2015).
Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. Int. Jt. Conf. Artif. Intell. 1995, 1137–1143 (1995).
Gitman, I., Lang, H., Zhang, P. & Xiao, L. Understanding the role of momentum in stochastic gradient methods. arXiv:1910.13962 (2019).
Foret, P., Kleiner, A., Mobahi, H. & Neyshabur, B. Sharpness-aware minimization for efficiently improving generalization. arXiv:2010.01412 (2020).
Gontijo-Lopes, R., Smullin, S. J., Cubuk, E. D. & Dyer, E. Affinity and diversity: Quantifying mechanisms of data augmentation. arXiv:2002.08973 (2020).
Nakagawa, S. & Cuthill, I. C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. 82, 591–605 (2007).
Sawilowsky, S. S. New effect size rules of thumb. J. Mod. Appl. Stat. Methods 8, 597–599 (2009).
Selvaraju, R. R. et al. Grad-CAM: Visual explanations from deep networks via gradient-based localization. Int. J. Comput. Vis. 128, 336–359 (2016).
Al-Haj Husain, A., Stadlinger, B., Winklhofer, S., Piccirelli, M. & Valdec, S. Magnetic resonance imaging for preoperative diagnosis in third molar surgery: A systematic review. Oral Radiol. https://doi.org/10.1007/s11282-022-00611-4 (2022).
Choi, E. et al. Artificial intelligence in positioning between mandibular third molar and inferior alveolar nerve on panoramic radiography. Sci. Rep. 12, 1 (2022).
Guidotti, R. et al. A survey of methods for explaining black box models. arXiv:1802.01933 (2018).
Xu, F. et al. The clinical value of explainable deep learning for diagnosing fungal keratitis using in vivo confocal microscopy images. Front. Med. 8, 797616 (2021).
Sukegawa, S. et al. Identification of osteoporosis using ensemble deep learning model with panoramic radiographs and clinical covariates. Sci. Rep. 12, 6088 (2022).
Ayhan, M. S. et al. Clinical validation of saliency maps for understanding deep neural networks in ophthalmology. Med. Image Anal. 77, 102364 (2022).
Wilkinson, L. Statistical methods in psychology journals: Guidelines and explanations. Am. Psychol. 54, 594–604 (1999).
Funding
This work was supported by JSPS KAKENHI (grant number JP19K19158) and JST, CREST (JPMJCR21D4), Japan.
Author information
Authors and Affiliations
Contributions
The study was conceived by S.S. and T.H., who also set up the experiments. F.T., S.S., and K.Y. (Kazumasa Yoshii) conducted the experiments. S.S., K.Y. (Katsusuke Yamashita), T.H., K.T., H.K., K.N. and H.N. generated the data. All authors analyzed and interpreted the data. S.S. and T.H. wrote the manuscript. All authors have read and approved the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sukegawa, S., Tanaka, F., Hara, T. et al. Deep learning model for analyzing the relationship between mandibular third molar and inferior alveolar nerve in panoramic radiography. Sci Rep 12, 16925 (2022). https://doi.org/10.1038/s41598-022-21408-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-21408-9
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
