
Abstract
Postoperative acute kidney injury (AKI) is a highly prevalent and serious complication after cardiac surgery. The aim of this study is to identify the predictors of AKI and the cut-off values after isolated off-pump coronary artery bypass grafting (OPCAB). A total of 329 adult patients, who underwent isolated OPCAB between December 2008 and February 2021, were retrospectively analyzed. The patients were divided into three groups: non-AKI, early AKI and late AKI groups. The early AKI group or the late AKI group were defined as ‘having AKI that occurred before or after 48 h postoperatively’, respectively. Multivariate logistic regression analysis was performed to identify the predictors of AKI. Receiver operating characteristic (ROC) curve analysis was used to evaluate the cutoff value, the sensitivity, and the specificity of the predictors. On the multivariate analysis, the emergency surgery, the preoperative serum albumin, and the postoperative day 1 neutrophil to lymphocyte ratio (NL ratio) were identified as the independent predictors of AKI. However, neither albumin nor the NL ratio predicted late AKI. The present study showed the preoperative albumin and the postoperative day 1 NL ratio were the robust and independent predictors of postoperative early AKI in isolated OPCAB.
Similar content being viewed by others
Introduction
Postoperative acute kidney injury (AKI) is a highly prevalent and serious complication after cardiac surgery. The incidence of AKI after cardiac surgery ranges from 13 to 43%, and AKI increases short- and long-term morbidity and mortality1,2,3. To predict postoperative AKI, numerous studies have identified several risk factors, including older age, body mass index, the duration of cardiopulmonary bypass (CPB), preoperative hypertension, the reduced left ventricular ejection fraction, and the preoperative impaired renal function4. The frequency of renal function evaluation after discharge from the intensive care unit decreases, making it difficult to detect and treat AKI early. Thus, the prediction of AKI, especially late-onset AKI, is very important for clinicians. Early appropriate prediction and focused monitoring for patients at high risk of AKI are paramount. C-reactive protein (CRP) is a representative marker of the acute proinflammatory process5 and one of the predictors of AKI6, 7. The postoperative day 1 neutrophil to lymphocyte ratio (NL ratio) is associated with postoperative AKI in cardiovascular surgery with CPB8. The cardiac biomarker, creatine kinase-MB (CK-MB), is also associated with AKI and mortality risk after cardiac surgery9,10. Moreover, an association between hypoalbuminemia and AKI has been reported in contrast-induced nephropathy11 and postoperative AKI in coronary artery bypass grafting (CABG)12. Although some previous reports have especially focused on inflammatory or cardiac markers as predictors of AKI after cardiac surgery9,13, the predictors of AKI in isolated off-pump CABG (OPCAB) have not been elucidated.
The aim of this study was to identify the predictors and cut-off values of AKI after isolated OPCAB. We evaluated whether early or late AKI following isolated OPCAB could be predicted by previously identified predictors of AKI following other cardiac procedures, the preoperative hemoglobin value, albumin, the NL ratio, CK-MB, and CRP on postoperative day (POD) 1.
Results
The total 329 patients in the present study, mean age 70.9 ± 8.9 years old, included 260 men (79.0%). AKI developed in 67 patients (20.4%); 46 patients (68.7%) had stage 1, 11 (16.4%) patients had stage 2, and 10 patients (14.9%) had stage 3 (Table 1). Among 67 patients with AKI, 44 patients (65.7%) had early AKI, and 23 patients (34.3%) had late AKI. Postoperative renal replacement therapy was required for 10 patients (14.9%). The demographic and intraoperative data of the entire cohort were shown in Table 2.
Univariate analysis showed significant differences between the non-AKI group and the AKI group in the preoperative atrial fibrillation (non-AKI group vs AKI group, 2.7% vs 9.0%, P = 0.033), the preoperative chronic kidney disease (38.9% vs 56.7%, P = 0.009), emergency OPCAB (9.2% vs 26.9%, P < 0.001), intraoperative urine volume (918.4 ± 774.1 vs 621.2 ± 580.0, ml, P = 0.004), intraoperative blood loss (370.9 ± 265.7 vs 460.6 ± 320.8, ml, P = 0.019), the preoperative serum albumin (3.9 ± 0.5 vs 3.6 ± 0.6, g/dl, P < 0.001), and the NL ratio (6.7 ± 5.1 vs 9.7 ± 5.4, postoperative day 1, P < 0.001, Tables 2 and 3). With the multivariate analysis, emergency OPCAB, the preoperative albumin, and the NL ratio were identified as independent predictors of AKI (emergency OPCAB: odds ratio (OR): 3.06, 95% confidence interval (CI): 1.45–6.41, P = 0.004; the preoperative albumin: OR: 0.47, 95% CI: 0.28–0.79, P = 0.004; the NL ratio: OR: 1.08, 95% CI: 1.02–1.15, P = 0.007, Table 4). Although both albumin and the NL ratio were significantly changed in the AKI (non-AKI group vs AKI group, albumin: 3.9 ± 0.5 vs 3.6 ± 0.6, P = 0.002, NL ratio: 6.7 ± 5.1 vs 9.7 ± 5.4, P < 0.001) and early AKI group (non-AKI group vs early AKI group, albumin: 3.9 ± 0.5 vs 3.5 ± 0.6, P < 0.001, NL ratio: 6.7 ± 5.1 vs 11.1 ± 5.8, P < 0.001), they did not predict late AKI occurrence (non-AKI group vs late AKI group, albumin: 3.9 ± 0.5 vs 3.8 ± 0.5, P = 0.906, NL ratio: 6.7 ± 5.1 vs 7.1 ± 3.2, P = 0.991) (Table 5). The results of multiple regression analysis were y = 0.626 + 0.012 × (operation time, min) − 0.001 × (Water balance, ml) + 0.003 × (bleeding, ml) − 1.191 × (chronic heart failure) − 0.838 × (chronic kidney disease) for NL ratio, and y = 4.269–0.012 × (age, year) + 0.108 × (chronic heart failure) for albumin. These results indicate the slight confounding effect, but these conditions seem less impacts in the clinical situation.
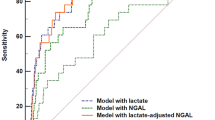
The receiver operating characteristic (ROC) curve analyses of preoperative albumin and the NL ratio were summarized in Table 6 and Figs. 1 and 2. Areas under the curve (AUC) for albumin were 0.635 (P < 0.001) in the AKI group and 0.672 (P < 0.001) in the early AKI group. A threshold postoperative albumin value of 3.8 was associated with the occurrence of AKI with a sensitivity of 67% and specificity of 58%, and that of 3.8 was associated with the occurrence of early AKI with a sensitivity of 73% and specificity of 58%. On the other hand, AUC for NL ratio were 0.693 (P < 0.001) in the AKI group and 0.755 (P < 0.001) in the early AKI group. A threshold postoperative NL ratio value of 7.3 was associated with the occurrence of AKI with a sensitivity of 63% and specificity of 70%, and that of 7.8 was associated with the occurrence of early AKI with a sensitivity of 68% and specificity of 74%.

Receiver operating characteristic curves for albumin and the neutrophil to lymphocyte ratio for predicting acute kidney injury. (a) albumin, (b) neutrophil to lymphocyte ratio.

Receiver operating characteristic curves for albumin and the neutrophil to lymphocyte ratio for predicting early acute kidney injury. (a) albumin, (b) neutrophil to lymphocyte ratio.
Discussion
A total of 329 patients who underwent OPCAB were analyzed, and the incidence of AKI was 20.4%. In this study, the Kidney Disease: Improving Global Outcome (KDIGO) criteria were used to define AKI. The diagnostic criteria for AKI have been updated to the KDIGO from RIFLE or Acute Kidney Injury Network (AKIN). In some previous reports1,2, the RIFLE criteria or AKIN criteria were used for AKI diagnosis. One of the differences between the KDIGO criteria and other AKI guidelines, the RIFLE and the AKIN criteria, is the duration of AKI. The KDIGO criteria defines AKI as 1 week duration, while other criteria define AKI as 48-h duration. Chen et.al.4 revealed the predictive factors of postoperative AKI in the isolated CAB patients with the KDIGO criteria. However, late AKI may be influenced by many factors such as postoperative management, hemodynamic condition, medication, infection and bleeding. Late AKI accounted for 34.3% of all AKI. In the present study, the preoperative albumin and the NL ratio were found to be predictors of AKI and early AKI, and the sensitivity of the NL ratio was higher than that of preoperative albumin. However, these two factors were not significant predictors of late AKI.
AKI is a common complication after CABG that is associated with the postoperative mortality14,15. Most cases of AKI after cardiac surgery are temporary and reversible. Patients with mild AKI are usually responsive to prompt medical interventions, such as avoiding additional renal insults and optimizing volume status. Medical therapy can prevent the progression of perioperative AKI and improve postoperative outcomes such as mortality16,17,18. Early detection of AKI may contribute to improving patients’ outcomes19. Therefore, the reliable predictors of AKI that show changes earlier than decreased urine volume and elevated serum creatinine are needed.
The pathophysiology of AKI after cardiac surgery is multifactorial, including inflammation, ischemia–reperfusion injury, operative trauma, neurohormonal activation, metabolic changes, and oxidative stress20,21,22. Cardiovascular surgery causes an activation of the inflammatory cascade because of the preoperative patients’ disease and surgical trauma. Although cytokines have the role as mediators of immunological responses to surgery, these biomarkers are not quickly available. Some cytokines are commonly well known their pro-inflammatory and anti-inflammatory functions regulating lymphocyte activity23. Neutrophils play an important role in inflammation, and a reduced lymphocyte count reflects physiological stress24,25. Dynamic change in the NL ratio is attributed to systemic inflammation. High NL ratio significantly increased the risk of mortality, post-operative re-intubation, limb amputation, and postoperative atrial fibrillation after cardiovascular operations26 and OPCAB24,27. Moreover, postoperative NL ratio was also independently associated with postoperative AKI following isolated CABG, because elevated NL ratio suggest an association between inflammation and renal failure28. Therefore, NL ratio could contribute to early identification of patients at high risk for periprocedural adverse events29. The relationship between AKI and the NL ratio in patients undergoing isolated OPCAB has not been studied sufficiently. One meta-analysis of the NL ratio for the prediction of AKI estimated an area under the curve of 0.65 in a cardiac surgery subgroup30. In the present study, ROC curve analysis yielded a similar result for the NL ratio (AUC: 0.693) with a cutoff value of 7.3 (63% sensitivity, 70% specificity) (Fig. 1). In addition, the NL ratio can also predict early AKI with a cutoff value of 7.8 (AUC: 0.755, sensitivity 68%, specificity 74%) (Fig. 2).
Hypoalbuminemia (often defined as < 3.5–4.0 g/dL) is a well-established risk factor for morbidity and mortality31,32. An association between hypoalbuminemia and AKI has been reported in contrast-induced nephropathy11 and postoperative AKI following cardiac surgery12,33. In patients with hypoalbuminemia, the glycocalyx might be compromised, leading to the loss of oncotic pressure gradients and barrier function, the fluid leakage into the tissue, and the microvascular flow alterations34,35. The serum albumin protects renal function by maintaining the oncotic pressure, which augments the intravascular volume36, maintains renal perfusion, and improves glomerular filtration37. Albumin also limits tubular cell apoptosis as a scavenger of radical oxygen species and roles as an anti-inflammation effector38,39. The reported cutoff values of albumin vary between previous studies due to the study populations and types of surgery. In a study with non-cardiac surgery patients, the cutoff value of 3.75 g/dL had a sensitivity of 54% and specificity of 67%; meanwhile, among patients undergoing brain tumor surgery, the cutoff value of 3.8 g/dL had a similar sensitivity of 54%, but lower specificity of 27%40,41. Our ROC curve analysis indicated that, albumin with a cutoff value of 3.8 (AUC 0.635, sensitivity 67%, specificity 58%) was a valuable predictor of AKI in isolated OPCAB. Our analysis also showed that albumin could predict early AKI with a cutoff value of 3.8, not for late AKI.
The present study hypothesized that CK-MB and CRP could be the predictors of AKI in isolated OPCAB patients. CK-MB is a specific myocardial marker that increased by myocardial ischemia and hypotension. Therefore, postoperative CK-MB elevation suggests intraoperative myocardial damage. Perioperative cardiac biomarkers including CK-MB are associated with an increased mortality risk after CABG with CPB10. Moreover, cardio-renal syndrome is a well-known interdependency of cardiac and renal dysfunction in cardiac disease. Preoperative CK-MB was a strong and independent predictor of postoperative AKI in cardiac surgery9. CRP is a representative marker of acute inflammation and predicts the severity of acute infection and long-term morbidity or mortality5,42. A high CRP level is a biomarker of AKI or mortality in cardiac disease6,42,43 and post-CABG patients with CPB7. However, they did not predict postoperative AKI in the present study. They are associated with AKI indirectly through myocardial damage or inflammation. Although these factors were measured on POD1, no significant increases were observed. For predictors to be useful, they need to increase early, before AKI is established.
The present study had some limitations. Firstly, this study is a single-center, retrospective, observational study. A prospective, multicenter study is needed to substantiate its broad applicability. Secondary, the period of this study is a long-time span. The surgical and anesthetics technology may be improved during the study period. Finally, we didn’t clarify whether N/L ratio and albumin were correlated with other factors because of limited sample number. The potential correlation may cause bias.
In conclusion, this study showed that preoperative albumin and the POD1 NL ratio are robust and independent predictors of postoperative AKI in isolated OPCAB. Both markers can be easily measured in general ward and detect patients at high risk of AKI and early AKI with high sensitivity. The further investigation of the late AKI predictors should be needed in OPCAB patients.
Methods
Participants and data collection
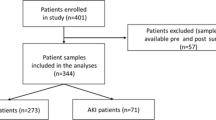
After approval by the ethics committee of Nippon Medical School (No. 2021–192). This study was performed in accordance with relevant guidelines and regulations. 329 adult patients who underwent isolated OPCAB between December 2008 and February 2021 at Nippon Medical School Hospital were retrospectively analyzed. Patients who lacked data or needed preoperative renal replacement therapy or circulatory assist devices in the perioperative period were excluded. Informed consent was obtained from patients through an opt-out method.
The patients’ hospital records, which included patient demographic information (sex, age, body mass index (BMI), preoperative comorbidities, examination data), their surgical management (emergency, duration of surgery, intraoperative blood loss), anesthetic management (water balance, urine volume), and postoperative data (urine volume, laboratory data), were collected. The KDIGO criteria for AKI were used in the present study based on the change in serum creatinine levels (≥ 0.3 mg/dL within 48 h or ≥ 50% within 7 days) or urine output volume less than 0.5 mL/kg/hour for > 6 hours44. The patients were divided into three groups: non-AKI, early AKI and late AKI groups. The early or late AKI group were defined as having AKI that occurred before or after 48 h postoperatively, respectively. The predictors of AKI in preoperative laboratory data, hemoglobin and albumin, in postoperative laboratory data, NL ratio, CK-MB and CRP, were measured within 1 week before surgery and at the postoperative day 1, respectively. NL ratio was calculated by dividing the number of neutrophils to the number of lymphocytes.
Anesthetic technique
All patients underwent general anesthesia with endotracheal intubation and ventilation. Anesthesia was maintained with sevoflurane, fentanyl, and rocuronium. An arterial blood catheter, transesophageal echocardiography, and a central venous catheter were routinely used. When transient hypoperfusion occurred during manipulation of the heart or anastomosis, systemic perfusion pressure was usually maintained by tilting the surgical table and administering intravenous fluids, followed by the administration of noradrenaline as a first-choice vasopressor. All patients were transferred to intensive care unit intubated postoperatively. They were extubated following normalization of orientation, hemodynamic and respiratory functions.
Statistical analysis
Clinical data were recorded and tabulated using Excel software (Microsoft Corp, Redmond, WA, USA). All statistical analyses were performed using JMP version 11 software (SAS Institute Inc., Cary, NC, USA). The results are expressed as means ± SD or n (%). P values of 0.05 were considered significant. Continuous variables were compared between groups using the two-tailed unpaired Student’s t-test. For dichotomous variables, group differences were examined using Fisher’s exact test. The postoperative serum markers were compared among three groups with Tukey’s test. Multivariate logistic regression analysis was performed to identify the predictors of AKI with independent variables. The model was built using variables that demonstrated a P < 0.05 on univariate analysis, except for confounding factors. Significance within the model was evaluated by the likelihood ratio test, and the strength of the association of variables with AKI was estimated by calculating the OR and 95% CI. Multiple regression analysis was performed to evaluate the confounding factors of postoperative day 1 NL ratio and preoperative albumin value. ROC curve analysis was used to compute the cutoff value, sensitivity, and specificity of the predictors.
Data availability
All data generated or analyzed during this study are included in this published article. Anonymized data for the current study are available from the corresponding author upon reasonable request.
References
Hobson, C. E. et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation 119, 2444–2453 (2009).
Ryden, L. et al. Acute kidney injury after coronary artery bypass grafting and long-term risk of myocardial infarction and death. Int. J. Cardiol. 172, 190–195 (2014).
Brown, J. R., Kramer, R. S., Coca, S. G. & Parikh, C. R. Duration of acute kidney injury impacts long-term survival after cardiac surgery. Ann. Thorac. Surg. 90, 1142–1148 (2010).
Chen, S. W. et al. Comparison of contemporary preoperative risk models at predicting acute kidney injury after isolated coronary artery bypass grafting: a retrospective cohort study. BMJ Open 6, e010176 (2016).
Povoa, P. C-reactive protein: a valuable marker of sepsis. Intensive Care Med. 28, 235–243 (2002).
Shacham, Y. et al. High sensitive C-reactive protein and the risk of acute kidney injury among ST elevation myocardial infarction patients undergoing primary percutaneous intervention. Clin. Exp. Nephrol. 19, 838–843 (2015).
Han, S. S. et al. C-reactive protein predicts acute kidney injury and death after coronary artery bypass grafting. Ann. Thorac. Surg. 104, 804–810 (2017).
Kim, W. H., Park, J. Y., Ok, S. H., Shin, I. W. & Sohn, J. T. Association between the neutrophil/lymphocyte ratio and acute kidney injury after cardiovascular surgery: a retrospective observational study. Medicine (Baltimore). 94, e1867 (2015).
Bucholz, E. M. et al. Cardiac biomarkers and acute kidney injury after cardiac surgery. Pediatrics 135, e945-956 (2015).
Domanski, M. J. et al. Association of myocardial enzyme elevation and survival following coronary artery bypass graft surgery. JAMA 305, 585–591 (2011).
Murat, S. N., Kurtul, A. & Yarlioglues, M. Impact of serum albumin levels on contrast-induced acute kidney injury in patients with acute coronary syndromes treated with percutaneous coronary intervention. Angiology 66, 732–737 (2015).
Lee, E. H. et al. Preoperative hypoalbuminemia is a major risk factor for acute kidney injury following off-pump coronary artery bypass surgery. Intensive Care Med. 38, 1478–1486 (2012).
Scrascia, G., Guida, P., Rotunno, C., de Luca Tupputi Schinosa, L. & Paparella, D. Anti-inflammatory strategies to reduce acute kidney injury in cardiac surgery patients: a meta-analysis of randomized controlled trials. Artif. Organs. 38, 101–112 (2014).
Han, S. S. et al. Effects of acute kidney injury and chronic kidney disease on long-term mortality after coronary artery bypass grafting. Am. Heart J. 169, 419–425 (2015).
Nigwekar, S. U., Kandula, P., Hix, J. K. & Thakar, C. V. Off-pump coronary artery bypass surgery and acute kidney injury: a meta-analysis of randomized and observational studies. Am. J. Kidney Dis. 54, 413–423 (2009).
Kwon, J. T., Jung, T. E. & Lee, D. H. Predictive risk factors of acute kidney injury after on-pump coronary artery bypass grafting. Ann. Transl. Med. 7, 44 (2019).
Mehta, R. L. et al. Nephrology consultation in acute renal failure: does timing matter?. Am. J. Med. 113, 456–461 (2002).
Balasubramanian, G. et al. Early nephrologist involvement in hospital-acquired acute kidney injury: a pilot study. Am. J. Kidney Dis. 57, 228–234 (2011).
Ponce, D., Zorzenon Cde, P., dos Santos, N. Y. & Balbi, A. L. Early nephrology consultation can have an impact on outcome of acute kidney injury patients. Nephrol. Dial. Transpl. 26, 3202–3206 (2011).
Takaki, S. et al. Perioperative change in creatinine following cardiac surgery with cardiopulmonary bypass is useful in predicting acute kidney injury: a single-centre retrospective cohort study. Interact. Cardiovasc. Thorac. Surg. 21, 465–469 (2015).
Harky, A. et al. Acute kidney injury associated with cardiac surgery: a comprehensive literature review. Braz. J. Cardiovasc. Surg. 35, 211–224 (2020).
Kramer, R. S., Herron, C. R., Groom, R. C. & Brown, J. R. Acute kidney injury subsequent to cardiac surgery. J. Extra Corpor. Technol. 47, 16–28 (2015).
Serra, R. et al. Novel biomarkers in cardiovascular surgery. Biomark. Med. 15, 307–318 (2021).
Gibson, P. H. et al. Preoperative neutrophil-lymphocyte ratio and outcome from coronary artery bypass grafting. Am. Heart J. 154, 995–1002 (2007).
Kurtul, A. & Ornek, E. Platelet to lymphocyte ratio in cardiovascular diseases: a systematic review. Angiology 70, 802–818 (2019).
Cho, J. H. et al. Neutrophil-lymphocyte ratio in patients with acute heart failure predicts in-hospital and long-term mortality. J. Clin. Med. 9 (2020).
Gibson, P. H. et al. Usefulness of neutrophil/lymphocyte ratio as predictor of new-onset atrial fibrillation after coronary artery bypass grafting. Am. J. Cardiol. 105, 186–191 (2010).
Parlar, H. & Saskin, H. Are pre and postoperative platelet to lymphocyte ratio and neutrophil to lymphocyte ratio associated with early postoperative AKI following CABG?. Braz. J. Cardiovasc. Surg. 33, 233–241 (2018).
Serra, R. et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as biomarkers for cardiovascular surgery procedures: a literature review. Rev. Recent Clin. Trials. 16, 173–179 (2021).
Chen, D., Xiao, D., Guo, J., Chahan, B. & Wang, Z. Neutrophil-lymphocyte count ratio as a diagnostic marker for acute kidney injury: a systematic review and meta-analysis. Clin. Exp. Nephrol. 24, 126–135 (2020).
Vincent, J. L., Dubois, M. J., Navickis, R. J. & Wilkes, M. M. Hypoalbuminemia in acute illness: is there a rationale for intervention? A meta-analysis of cohort studies and controlled trials. Ann. Surg. 237, 319–334 (2003).
Engelman, D. T. et al. Impact of body mass index and albumin on morbidity and mortality after cardiac surgery. J. Thorac. Cardiovasc. Surg. 118, 866–873 (1999).
Kim, W. H. et al. Potentially modifiable risk factors for acute kidney injury after surgery on the thoracic aorta: a propensity score matched case-control study. Medicine (Baltimore). 94, e273 (2015).
Schiefer, J. et al. Alterations of endothelial glycocalyx during orthotopic liver transplantation in patients with end-stage liver disease. Transplantation 99, 2118–2123 (2015).
Woodcock, T. E. & Woodcock, T. M. Revised Starling equation and the glycocalyx model of transvascular fluid exchange: an improved paradigm for prescribing intravenous fluid therapy. Br. J. Anaesth. 108, 384–394 (2012).
Lee, E. H. et al. Effect of Exogenous albumin on the incidence of postoperative acute kidney injury in patients undergoing off-pump coronary artery bypass surgery with a preoperative albumin level of less than 40 g/dl. Anesthesiology. 124, 1001–1011 (2016).
Aksoy, R. et al. Is Hypoalbuminemia a predictor for acute kidney injury after coronary bypass grafting in diabetes mellitus patients?. Braz. J. Cardiovasc. Surg. 34, 565–571 (2019).
Quinlan, G. J. et al. Albumin influences total plasma antioxidant capacity favorably in patients with acute lung injury. Crit. Care Med. 32, 755–759 (2004).
Bauer, M., Huse, K., Settmacher, U. & Claus, R. A. The heme oxygenase-carbon monoxide system: regulation and role in stress response and organ failure. Intensive Care Med. 34, 640–648 (2008).
Li, N. et al. Preoperative hypoalbuminemia was associated with acute kidney injury in high-risk patients following non-cardiac surgery: a retrospective cohort study. BMC Anesthesiol. 19, 171 (2019).
Kim, K. et al. Association of preoperative hypoalbuminemia with postoperative acute kidney injury in patients undergoing brain tumor surgery: a retrospective study. J. Neurosurg. 128, 1115–1122 (2018).
Zacho, J., Tybjaerg-Hansen, A. & Nordestgaard, B. G. C-reactive protein and all-cause mortality–the copenhagen city heart study. Eur. Heart J. 31, 1624–1632 (2010).
Gao, F. et al. C-reactive protein and the risk of contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. Am. J. Nephrol. 34, 203–210 (2011).
Okusa, M. D. & Davenport, A. Reading between the (guide)lines–the KDIGO practice guideline on acute kidney injury in the individual patient. Kidney Int. 85, 39–48 (2014).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
M.Is. analyzed the data. M.Is., M.Iw., D.N., M.Y., and T.M. drafted the manuscript. A.S. and Y.I. supervised the drafting of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ishikawa, M., Iwasaki, M., Namizato, D. et al. The neutrophil to lymphocyte ratio and serum albumin as predictors of acute kidney injury after coronary artery bypass grafting. Sci Rep 12, 15438 (2022). https://doi.org/10.1038/s41598-022-19772-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19772-7
This article is cited by
-
Machine-learning predictions for acute kidney injuries after coronary artery bypass grafting: a real-life muticenter retrospective cohort study
BMC Medical Informatics and Decision Making (2023)
-
The ratio of monocytes to lymphocytes multiplying platelet predicts incidence of pulmonary infection-related acute kidney injury
European Journal of Medical Research (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
