
Abstract
Socioeconomic status has been associated with obesity prevalence increase in both males and females worldwide. We examined the magnitude of the difference between the two relationships and explored the independence of both relationships. Country specific data on gross domestic product (GDP) per capita, sex-specific obesity prevalence rates, urbanisation, total calories availability and level of obesity, genetic background accumulation (measured by the Biological State Index, Ibs) were obtained for 191 countries. Curvilinear regressions, bivariate and partial correlations, linear mixed models and multivariate linear regression analyses were used to examine the relationship between GDP and obesity prevalence rates in males and females respectively. Fisher’s r-to-z transformation, F-test and R2 increment in multivariate regression were used to compare results for males and females. GDP significantly correlated with sex-specific obesity prevalence rates, but significantly more strongly with male obesity prevalence in bivariate correlation analyses. These relationships remained independent of calories availability, Ibs and urbanization in partial correlation model. Stepwise multiple regression identified that GDP was a significant predictor of obesity prevalence in both sexes. Multivariate stepwise regression showed that, when adding GDP as an obesity prevalence predictor, the absolute increment of R2 in male fit model (0.046) was almost four (4) times greater than the absolute increment in female model fit (0.012). The Stepwise analyses also revealed that 68.0% of male but only 37.4% of female obesity prevalence rates were explained by the total contributing effects of GDP, Ibs, urbanization and calories availability. In both Pearson’s r and nonparametric analyses, GDP contributes significantly more to male obesity than to female obesity in both developed and developing countries. GDP also determined the significant regional variation in male, but not female obesity prevalence. GDP may contribute to obesity prevalence significantly more in males than in females regardless of the confounding effects of Ibs, urbanization and calories. This may suggest that aetiologies for female obesity are much more complex than for males and more confounders should be included in the future studies when data are available.
Similar content being viewed by others

Introduction
Obesity (defined by body mass index, BMI ≥ 30 kg/m2) is a complex, multifactorial, and largely preventable condition1,2. Enormous efforts have been made to control obesity increase all over the world. However, unfortunately, except Singapore who implemented very aggressive exercise based programmes3, no other country has achieved their expected results in the past decades1. Now, obesity, along with overweight, has been affecting over a third of the world’s population1,2,4. Obesity has been considered a major risk factor for various health issues5,6,7, such as cardiovascular diseases, type 2 diabetes, osteoarthritis, premature death, depression and certain types of cancer8,9,10.
The causes of obesity may be both biological and social11. However, research into biological factors has been far more thorough than into social risk factors, and biological research and the importance of its findings continue to grow. GDP has been significantly and strongly associated with total calories availability (r > 0.7, p < 0.001) in previous studies12,13. Accordingly individual major food groups which contribute to total calories availability have also been associated with obesity, such as fat14,15,16, meat protein13,17,18, carbohydrates19,20 and soybean21. Gluten in cereal crops and trypsin and phytates in soy food products have been associated with metabolic syndrome leading to obesity12,21,22. Urbanization and urban industries contribute to more than 80% of global GDP23, but it has been associated with sedentary lifestyle and poor diet structure, which have been posing major risk factors for obesity24,25,26,27,28,29. In the recent years, better healthcare services in developed countries have been thought to reduce natural selection and allow the accumulation of obesity related genetic background, which genetically contributes to population level obesity prevalence30,31,32.
Veblen in 1889 may be the first scientist to relate socioeconomic status (SES) to body weight in both sexes, males and females33. One hundred years later, a review of 144 published studies of the relationship between SES and obesity reveals a strong inverse relationship among women, but inconsistent for men in developed societies34,35,36,37. Contrarily, in developing countries, there are not enough studies on the relationships between SES and female and male obesity for drawing conclusions yet35,38. The underlying reasons may be that there have been no sufficient comparable data to explore and compare the sex-specific correlations for males and females at population level, for example between developed and developing countries, or within a nation.
Constantly, studies have revealed that obese people would have significant health benefit if they lose their weight moderately39,40,41. Due to physiological differences, males and females may have different negative consequences from obesity. For instance, obesity may be nearly three times more deadly for men than it is for women42. However, females are at higher risk of developing morbid obesity than males43.
With the advantage of ecological studies to have more access to population level information, this study aimed to supplement the previous studies with the internationally comparable data for exploring and comparing the correlations of GDP to sex-specific obesity prevalence rates. In order to examine the independent relationships, total calories availability, urbanization, and accumulation of genetic background of obesity (measured by Biological State Index, (Ibs)) were included in the data analyses as the potential confounders.
Materials and methods
The population (country) level data were obtained from international organisations for this ecological study.
Data sources
Gross domestic product per capita (GDP, expressed in US dollars 2010) was extracted from the website of the World Bank as the independent variable44. It will be called “economic affluence” interchangeably in this study.
The WHO Global Health Observatory (GHO) data (2014) on estimated sex-specific obesity prevalence rates by country were obtained and used as the dependent variables45. The estimates of sex-specific prevalence rates of obesity are expressed as the percentages of population aged 18+ with BMI equal to or over 30 kg/m2.
There are 3 country specific potential confounding factors in this study. We intentionally backdated the years of predicting variable, GDP, and potential confounding variables, calories, obesity genetic background accumulation and urbanization, because of their delayed presentations in obesity prevalence. For example, males who moved today into urban areas, may not be obese the next day. It may take some years for their bodies to accumulate fat.
-
1.
Calories availability, expressed as the mean grand total calories supply/availability per capita per day during the period of 3 years 2011–201346.
Overconsumption of calories due to increased affordability has been a well-established risk factor for body weight increase47,48,49. We need to acknowledge that calories availability published by the FAO only means the availability of food products which may not be the actual intake, although a large majority of the available food products is consumed by people.
-
2.
Biological State Index (Ibs), estimating the magnitude of accumulation of obesity genetic background and other obesity associated deleterious genes in a population due to relaxed natural selection30,32,50,51.
Ibs calculation was based on the fertility data of each country published by United Nations52,53,54 and the mortality data of life tables published by World Health Organization (WHO) in 201255. These calculations were the same as in the previous study published by Budnik and Henneberg32.
-
3.
Urbanization (URBAN), expressed as a percentage of the population living in urban areas in 201056
Living in an urban setting leads to sedentary lifestyle (less physical activity) and poor diets (sugar, less vegetables), which have been considered an important factor to increase the risk of obesity57,58,59,60. Urban living setting also mirrors the Western lifestyle.
The independent variable (GDP) and all the three potential confounders were aligned with the listing of the prevalence rates of obesity (BMI ≥ 30 kg/m2) in females and males. A set comprising 191 country specific data was established and put in a uniform format in the Microsoft® Excel 2016 for subsequent data analysis. Each country was treated as an individual subject and all of their available information was analysed. For some countries an estimate of one or the other variable was missing, thus specific analyses have sample sizes varying from 168 to 191.
International organizations, such as the WHO, FAO and the World Bank monitor and publish population specific data in relation to the health status, nutrition and diet, and economic development. These data have been helping governments, policymakers, funders and researchers track and investigate the priorities of health research and development based on public health needs and ensure that funds and resources are used to meet the priorities. Their data have been recently used to examine the relationships between nutrients and obesity12,13,21,61,62, diabetes51,63,64,65, and relationship between natural selection and obesity32,66 and type 1 diabetes51 and cancers66,67,68 respectively.
Data are freely available from the websites of the UN agencies (WHO, the World Bank and FAO). Data sources were described in the manuscript and their specific URLs were indicated in the section of References. No ethical approval or written informed consent for participation was required.
Data multicollinearity check
We conducted the diagnostic test to rule out the potential multicollinearity between the variables for our data analyses. The test criteria are set up with the tolerances over 0.20 and the Variance Inflation Factors (VIF) less than 569.
Data analysis
The country specific data were collected for the ecological analyses in this study, which proceeds with six steps:
-
1.
Microsoft Excel® was applied to produce scatter plots with raw (non-logarithmed) data for exploring and visualizing the worldwide relationships between the GDP and the obesity prevalence rates in males and females respectively. Accordingly, the two trendlines were indicated in the graphs to reflect the relationships between economic affluence and obesity prevalence rates in males and females respectively.
For other analyses in SPSS, the variable values were logarithmically transformed to bring their distributions closer to normality. This allowed us to examine and compare the correlations between economic affluence and obesity prevalence rates in males and females worldwide, and in different country groupings.
-
2.
The Pearson product-moment correlation coefficients (Pearson’s r) were explored for the measures of the strengths of a linear association between variables (independent, dependent and potential confounders).
Considering the deviations from homoscedasticity, subsequently, nonparametric correlation (Spearman’s rho) analysis was performed with the same set of data to examine the magnitude of the potential differences between correlation coefficients for each sex-specific obesity prevalence rate and all variables calculated in Pearson and nonparametric correlation analyses.
-
3.
Partial correlation analysis was performed to explore the independent linear correlations of GDP to male and female obesity prevalence rates respectively while we controlled for calories availability, Ibs and urbanization.
Fisher’s r-to-z transformation was conducted to assess the level of difference and its significance in each individual association between GDP and sex-specific obesity prevalence rate in the data analysis models of Pearson’s r, Spearman’s rho and partial correlation.
-
4.
Standard multivariate linear regression (Stepwise) was performed to assess which non-GDP predictor(s) made substantial contributions to variation in obesity, and then GDP was added to the list of predictors to show improvement in model fits for males and females. The magnitudes of improvements in the two model fits were compared with the absolute improvement values obtained from “the R2 improvement in male prevalence due to adding GDP” and “the R2 improvement in female prevalence due to adding GDP” respectively.
Standard multivariate linear regression (Enter) was conducted on log-transformed data to obtain and compare the Beta coefficients between sex-specific obesity prevalence and all independent variables, which included economic affluence, calories availability, Ibs and urbanisation. The two Beta coefficients were compared to test the level of difference70.
-
5.
The universal correlations between GDP and sex-specific obesity prevalence rates were explored and compared (Fisher’s r-to-z transformation) in different country groupings:
-
1.
the UN common practice of defining the developed and developing countries71;
-
2.
the World Bank income classifications: high income, upper middle income, low-middle income and low income;
-
3.
the WHO regional classifications: Africa (AFR), Americas (AMR), Eastern Mediterranean (EMR), Europe (EU), South-East Asia (SEAR) and Western Pacific (WPR)72;
-
4.
countries with the strong contrast in terms of geographic distributions, per capita GDP levels and/or cultural backgrounds. We analysed the correlation in the six country groupings: Asia Cooperation Dialogue (ACD)73; The Asia–Pacific Economic Cooperation (APEC); the Arab World74, countries with English as the official language (government websites), European Economic Area (EEA)75, European Union (EU)76, Latin America and the Caribbean (LAC)77, the Organisation for Economic Co-operation and Development (OECD) and non-OECD grouping78, and the Southern African Development Community (SADC)79.
In our analysis, we only included those countries for which we could access their data for the specific groupings. To a large extent, grouping countries for analysis may also allow to align our findings against previous local or regional studies regarding heterogeneous epidemiology approaches due to various geographic locations and ethnicity.
-
1.
-
6.
The importance of GDP in determining the regional variation of sex-specific obesity prevalence rates was compared within the six (6) WHO regions, and UN developed and developing country groupings respectively.
Obesity prevalence rates in both males and females vary by region significantly and the variations have rapidly increased between 1980 and 200811,80. The role of GDP in determining significant regional variations of obesity prevalence rates in males, but not in females, between the six (6) WHO regions was demonstrated.
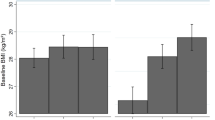
Equations of the best fitting trendline displayed in the scatter plots analysis of relationships between GDP and obesity prevalence rates in males and females were used to calculate and remove the contributing effect of GDP on obesity prevalence rate in males and females respectively. This allowed us to create two new dependent variables, “Residual of male obesity prevalence standardised on GDP” and “Residual of female obesity prevalence standardised on GDP”. Countries were categorized as per the WHO regions72 and UN common practice on defining more developed and developing countries71 for investigating the regional variations based on mean difference. Means of obesity prevalence rates in both males and females, and “Residual of male obesity prevalence standardised on GDP” and “Residual of female obesity prevalence standardised on GDP” of all the countries were calculated for each of the six WHO regions, and UN developed and developing countries. Post hoc Scheffe (Oneway ANOVA) and Independent Samples T-test were conducted to compare the means between the six WHO regions and UN country groupings respectively.
Standard deviation is a measure of how dispersed the data are in relation to the mean. Low standard deviation means data are clustered around the mean, and high standard deviation indicates data are more spread out. We calculated the sex-specific standard deviations used for facilitating our Discussion.
Pearson’s r, Spearman’s rho coefficient, partial correlation, the linear Mixed Model Analysis and multiple-linear regression analyses were conducted using SPSS v. 25. The statistical significance was set at the 0.05 level, but the significance levels at 0.01 and 0.001 were also reported.
Results
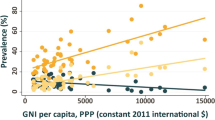
Economic affluence (GDP) was in strong and significant correlation with both male obesity prevalence rate (logarithmic, r = 0.721 p < 0.001, Fig. 1–1) and female obesity (logarithmic, r = 0.471, p < 0.001, Fig. 1–2). Fisher r-to-z revealed that GDP was in significantly stronger correlation with male obesity than with female obesity (z = 3.21, p < 0.001). GDP explained 51.98% of male obesity prevalence variance, which is more than double female obesity prevalence variance (22.20%).

Relationship between GDP per capita and sex-specific obesity prevalence rate.
In Pearson correlation analysis, worldwide, GDP was significantly correlated with both male and female obesity prevalence rates (Table 1). Similar values of correlation coefficients were observed in Spearman’s rho analysis as well indicating that log-transformation is sufficient to avoid substantial deviations from linear regressions in moment-product correlations (Table 1).
Fisher r-to-z transformation revealed that GDP significantly more strongly correlated with male obesity than with female obesity in Pearson’s r (z = 4.06, p < 0.001) and Nonparametric correlation (z = 4.16, p < 0.001) respectively (Table 2).
Partial correlation analysis showed that, worldwide, the GDP was still significantly correlated with the male and female obesity prevalence while we controlled for calories availability, Ibs and urbanization (Table 2). GDP was in partial correlation significantly stronger correlated with male obesity prevalence than with female obesity prevalence (z = 1.64, p < 0.05) (Table 2).
The effect size of GDP on male obesity prevalence is 0.110, which is much greater than on female prevalence, 0.026 (Table 2).
The above results suggest that economic affluence indexed with GDP per capita played a significantly stronger role in male obesity than in female obesity.
Multivariate regression model (Enter) revealed that GDP was a strongly significant predictor of male obesity prevalence when Ibs, calories availability, GDP and urbanization were entered as the predicting variables. In contrast, GDP was only a relatively weak, though still significant predictor of female obesity prevalence (Table 3–1). The influence of GDP on male obesity prevalence rate was stronger than on female obesity prevalence (overlap = 0.033).
Stepwise multivariate regression model results indicated that GDP was strongest and significant predictor of both male and female obesity prevalence. However, GDP explained 60.6% male obesity prevalence, but only 26.8% female obesity prevalence (Table 3–2). The influence of GDP on male obesity prevalence rate was significantly stronger than on female obesity prevalence (overlap = 0.00%).
In the Stepwise regression, the absolute improvement of R2 value due to adding GDP in male model fit was 0.046 (from 0.634 to 0.680), which was nearly four times the absolute improvement value 0.012 (from 0.272 to 0.284) due to adding GDP to female model fit (Table 3–2).
In the Stepwise multivariate regression model, when calories availability, GDP, Ibs and urbanization were included as the independent predicting variables, all the four variables, explaining 68.0% male obesity in total, were selected as the predictors that have the most influence on male obesity (Table 3–2). Interestingly, only GDP and Ibs were selected as the predictor which have the most influence on female obesity, and all the four variables only explain 28.4% female obesity in total (Table 3–2). This may suggest that, statistically, female obesity can be explained by other factors, such as psychological and social expectations etc.
Table 4 shows and compares the bivariate relationships between GDP and male and female obesity prevalence rates in different country groupings. The general trend was that, in the wealthy countries, GDP correlated with male obesity prevalence rate significantly stronger than it correlated with female obesity prevalence rate. This can be observed in the UN developed countries, the World Bank high income countries, the WHO Europe regional area, European Economic Area, European Union and Organisation for Economic Co-operation and Development. Contrarily, in the countries with lower GDPs, differences between GDP correlations with male and female obesity prevalence rates were generally smaller and insignificant.
The significant difference was also observed in the different country groupings with stratified socioeconomic levels. For instance, the difference between male and female obesity correlations with GDP were greater and significant in UN developing country grouping while not in the developed countries respectively. The similar pattern occurred between the low-income countries and the high-income countries in the World Bank country classifications.
Table 5 shows that GDP determined regional variation of male obesity prevalence rate, but not female obesity prevalence rate. Post hoc Scheffe analysis of 30 comparisons of means between the six (6) WHO regions, found in 18 out of 30 the significant differences in male obesity prevalence rate. However, all the eighteen (18) differences lost the significant levels when the contribution to obesity prevalence of GDP was removed in the same analysis model. The same analysis approach was applied to compare the means of female obesity prevalence rate. With and without GDP contributions to female obesity prevalence rate, the numbers of significant differences remained the same within the six (6) WHO regions.
This was further confirmed with the Independent T-test to compare the sex-specific obesity prevalence rates in the UN developed and developing countries. The mean of male obesity prevalence rate was significantly different between developed and developing country groupings (T = 4.549, p < 0.001). However, for female obesity prevalence rate, the difference was negligible and insignificant (T = − 0.388) between developed and developing country groupings. When GDP contributions to male and female obesity prevalence rates were removed, the mean of male obesity prevalence rate in developed country grouping is significantly lower than that in developing country grouping (T = 4.33, p < 0.001). However, when GDP contributions were removed, the mean differences of prevalence rates in males and females between developed and developing countries are similar (T = 5.551 vs 4.325, p < 0.001).
Discussion
The findings in this study confirmed that both male and female obesity prevalence rates were in non-linear relationships with GDP per capita as in previous studies. The scatter plots showed that sex-specific obesity prevalence rates initially increase with income, flatten out and then are attenuated with further GDP increase. However, the difference between the associations of GDP with sex-specific obesity prevalence rates is more complex than often argued.
With the advantages of ecological studies, we extracted the comparable data for examining and comparing the correlations between GDP and obesity prevalence rates in males and females globally and in different country clusters. Our data analyses revealed that, worldwide, GDP per capita was in significantly stronger correlations with male obesity prevalence rates than with female obesity prevalence rates. Furthermore, this significantly different relationship was independent of other major obesity risk factors, total calories availability, urban lifestyle and obesity genetic background accumulation. We also found that, in developing countries, the correlations of both sex-specific obesity prevalence rates with GDP were stronger than their counterparts in the developed countries.
Worldwide, GDP has been a major drive for obesity prevalence rate. However, surprisingly, it has fuelled male obesity prevalence rate significantly more than it has done for female obesity prevalence rate. It is not clear to us how genetic background influences the correlations between GDP and sex-specific obesity prevalence rate. There are several possible environmental factors which may have been altering correlations of GDP with obesity prevalence rates more in females than males30. Males and females may be differently exposed to socioeconomic inequalities. Wells et al. argued that in developing countries, females with low and insecure income may not have as much access to nutritious food as males, and this may influence their body mass increase81. Worldwide, different sociocultural beliefs and practices may affect female disparities in excessive weight gain11,82,83,84,85,86. Discriminatory social practices measured with the Gender Inequality Index, the Global Gender Gap Index and the Social Institutions and Gender Index were applied to explain the more prevalent female obesity87.
An important double social standard on people’s appearance has made females more appearance-focused than males88,89,90 which leads females to modify their personal environment, such as work routine, dietary pattern and physical exercise to adjust their body mass to appearance standards90,91. Therefore, although females may share with males the same level of natural genetic endowment for the phonotype of body weight, their body weights have been influenced by specific practices to meet different social and cultural values. For instance, in the developing world, secularly, a large body size of female is desired and considered a sign of wealth and health92,93, which is even linked to higher fertility11 as reproduction is a nutritionally expensive process for women94,95. Additionally, in some cultures and religions96, females have been overprotected and restricted from publicly participating in physical activities97. These can be seen in not only some developing countries, for instance, North Africa98 and Middle East99 regions, but also in some developed countries such as Saudi Arabia100, Kuwait101,102 and Oman101,103.
In the economically transitioning countries, agriculture industrialisation has replaced more agrarian laborious jobs of females than males. Accordingly, this transition has reduced the physical activity for females more than males which may have increased the obesity prevalence rates in females more than in males11,104,105. Agriculture industrialisation toward the end of the twentieth century also released more females to become salaried workforce106,107. For time-saving purposes, they may choose to purchase more pre-packaged foods leading to body weight increase108. Those females who experienced periods of deprivation during childhood, may purchase more food due to their stronger motivation to ensure food security109.
In contrast, in developed countries, lots of females practice more healthy lifestyles, such as healthy diet patterns110,111 and more physical exercise112,113 and even psychological meditation114,115,116. These body control approaches may have worked successfully which is typically reflected with the inverse correlations between GDP and female obesity prevalence rates in our bivariate correlation models (Table 4). However, in the Western societies, females still show greater obesity prevalence than those in developing countries. This may have several explanations. Females in the developed world show greater consumption of those foods and drinks which pose higher risk for gaining body weight, such as alcoholic beverages117,118, sugar62,119, and meat products13,62,120. Social network is culturally more acceptable in the Western world for females, and it may exacerbate their trend to gain more body weight82,121. Additionally, their declining total fertility rate leading to the increase of estrogen production may explain their body weight increase as well122,123,124. At population level, it is reflected with greater obesity prevalence rates.
The above factors have modified the population level male and female obesity prevalence significantly. To support this statement, we compared the calculated standard deviations of male and female obesity prevalence rates (10.5182 and 12.1482 respectively) with the F-test. It was identified that there is a significant difference between the two standard deviations (F = 1.33, p < 0.05). This may indicate that female obesity prevalence rates in different countries are more spread due to more complex modifications, which include those above mentioned factors.
Greater economic affluence may allow people to have more opportunity to modify body weight though a number of interventions, which may be significant depending on socioeconomic status. Driven more by appearance, females may take more advantage of greater economic affluence to manage their body weight. The scatterplots exploring the relationships between male and female obesity prevalence show that, in the developed countries, male obesity prevalence only explains 59.51% of female obesity, but 92.14% in the developing countries. This may be partially because females in the developed countries have been exerting more modifications to manage their body weight.
The similar sources of data on economic affluence and sex-specific obesity prevalence rates were extracted and their relationships have been examined by other researchers. Wells et al. reported the correlations of GDP to obesity prevalence rates in both males and females at population level81. However, in their study the correlation of GDP to female obesity prevalence rates did not reach the significant level. Most likely, this was due to the small sample size (n = 73, instead of 191 with available data on obesity prevalence rates). This may have led to biased correlation which could not represent the general worldwide correlations between GDP and sex-specific obesity prevalence rates. The other significant difference from our study is that the potential major confounders were not appropriately considered. Total fertility rate was included in the regression model for exploring that GDP correlated with female obesity prevalence rate independently, but it has not been established as a possible risk factor for obesity yet. Our study included the three well established population level potential confounders of obesity (calories availability, Ibs and urbanization), and we found that the GDP correlated with obesity prevalence rates in both sexes significantly and independently in both partial correlation and multivariate linear regression models. With large similarities, the non-linear relationships between GDP and sex-specific obesity prevalence rates were observed and economic affluence variables were stratified for correlation analyses as well125,126. However, these studies did not quantify the level of differences in the correlation of GDP with sex-specific obesity prevalence rates. Nor did they include the potential confounders for GDP for ruling out their contributions to explore the independent correlations between GDP and sex-specific obesity prevalence rates. For instance, Eggers et al. acknowledged urban living as a major risk factor for obesity and analysed the relationships between urbanization and the obesity prevalence rates in both males and females125. However, the independence of the relationships was not considered in their study. At individual level, a study conducted in Korean population (45+) revealed that household income significantly correlated with male overweight, but not with female overweight prevalence due to cultural perception that drove females to manage their body weight for good looking body shape to increase their confidence and efficiency in work environment90. Obviously, high income applied more to male obesity increase than to females’ in the studied population. Again, the level of difference was not reported and the correlations of household income with sex-specific obesity were not corrected for any potential confounders.
Multiple variables (GDP, calories availability, urbanization and obesity gene accumulation) were included for the data analyses in this study. It is necessary to align our study findings with other related hypotheses.
High calories intake has been unarguably considered as the risk factor for obesity. In our study, the same total calories availability was correlated with both male and female obesity prevalence rates, but it significantly correlated with male obesity rather than with female obesity (z = 3.30, p < 0.001, and z = 4.31, p < 0.001) in Pearson’s and non-parametric correlations respectively, Table 1). This difference was confirmed in the subsequent Stepwise linear regression that calories availability was selected as the 3rd most influential predictor for male obesity (increasing R2 up to 0.673), but it was not shown as one of the most significant risk factors for female obesity prevalence (Table 3–2).
There are several limitations in this study. Firstly, like other data analysis-based studies, the relationships observed between the various variables may not be causal, but just correlational. Secondly, as this is an ecological study, with the intrinsic ecological fallacy, we could only demonstrate the relationships between the GDP and the sex-specific obesity prevalence rates at country/population level, which do not necessarily hold true at the individual level. Thirdly, Sex-specific obesity prevalence rates were not correlated with sex-specific exposures in this study due to data unavailability. However, it would be very interesting to see how the sex-specific obesity prevalences correlate to the sex specific exposure, such as economic welfare. Fourthly, the cross-sectional data, instead of longitudinal data, were analysed in this study. Therefore, the correlations identified may not be able to necessarily reflect historical trends of the relationships between economic affluence and sex-specific obesity prevalence rates. Finally, we controlled for the major risk factors involved in total calories availability, obesity genetic background accumulation (measured by Ibs) and lifestyle change (measured by urbanization) in our data analyses, but there are still residuals of obesity which were not explained by these confounders and the independent variable. For instance, GDP and its three potential confounders explained 68.0% of male obesity prevalence rate, but only 28.4% of female obesity prevalence rate (Table 3–2). This also highlighted that more complex aetiologies of female obesity, such as adaptation for fertility127, oestrogen124 and double X chromosomes in cells128,129 may be at work. These factors may have confounded the correlations between GDP and sex-specific obesity prevalence rates, but we could not access or include the data for our analyses.
It is worth highlighting a strength or novelty of this study in comparison with the previous research in exploring the relationships between economic affluence and sex-specific obesity prevalence rates. The results in this study revealed that, surprisingly, the difference between females and males has reached the level of statistical significance globally. Furthermore, this significance level remains in different data analysis models with and without considering the competing effects of calories, urban lifestyles and genetic background of obesity accumulation.
Conclusions
Worldwide, economic affluence (measured by GDP) is still the major drive for the increase of obesity prevalence rates in both sexes, but it plays a much stronger role in male obesity prevalence increase. Different from previous studies, we demonstrate that sexual disparity has reached the significance level, and is independent of the other common obesity drives, urbanization, calories availability and obesity associated genetic background.
Data availability
All data for this study are publicly available from the United Agencies’ websites. The specific sources are described in the section of “Data sources”, and a whole set of data for this study is attached as s Supplemental Excel document. The purpose of using these in this study meets the terms and conditions of the relevant UN agencies. The formal permission is not required to download and analyse the data in this study.
References
Ng, M. et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945), 766–781 (2014).
Stevens, G. et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metrics 10, 1–16 (2012).
Simmons, R., Unwin, N. & Griffin, S. An Update of the Evidence Concerning the Prevention of Type 2 Diabetes (IDF, 2010).
Rokholm, B., Baker, J. L. & Sørensen, T. I. A. The Levelling Off of the Obesity Epidemic Since the Year 1999—A Review of Evidence and Perspectives, 835–846 (2010).
Wilson, M. Z. et al. Timing of postoperative infections after colectomy: Evidence from NSQIP. Am. J. Surg. 212(5), 844–850 (2016).
Frasson, M. et al. Risk factors for anastomotic leak and postoperative morbidity and mortality after elective right colectomy for cancer: Results from a prospective, multicentric study of 1102 patients. Int. J. Colorectal Dis. 31(1), 105–114 (2016).
Brathwaite, S. et al. Risk factors for surgical site infection in open and laparoscopic Hartmann closure: A multivariate analysis. Surg. Laparosc. Endosc. Percutaneous Tech. 27(1), 51–53 (2017).
Park, B. K. et al. Lifestyle, body mass index, diabetes, and the risk of pancreatic cancer in a nationwide population-based cohort study with 7.4 million Korean subjects. Br. J. Cancer 1–9 (2022).
Luppino, F. S. et al. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 67(3), 220–229 (2010).
Ogunbode, A. et al. Obesity: An emerging disease. Niger. J. Clin. Pract. 14(4), 390–394 (2011).
Kanter, R. & Caballero, B. Global gender disparities in obesity: A review. Adv. Nutr. 3(4), 491–498 (2012).
You, W. et al. Gluten consumption may contribute to worldwide obesity prevalence. Anthropol. Rev. 83(3), 327–348 (2020).
You, W. & Henneberg, M. Meat consumption providing a surplus energy in modern diet contributes to obesity prevalence: An ecological analysis. BMC Nutr. 2(1), 1–11 (2016).
Cândido, F. G. et al. Impact of dietary fat on gut microbiota and low-grade systemic inflammation: Mechanisms and clinical implications on obesity. Int. J. Food Sci. Nutr. 69(2), 125–143 (2018).
Hu, S. et al. Dietary fat, but not protein or carbohydrate, regulates energy intake and causes adiposity in mice. Cell Metab. 28(3), 415-431.e4 (2018).
Hall, K. D. Did the food environment cause the obesity epidemic?. Obesity 26(1), 11–13 (2018).
You, W. & Henneberg, M. Meat in modern diet, just as bad as sugar, correlates with worldwide obesity: An ecological analysis. J. Nutr. Food Sci. 6(517), 4 (2016).
Grantham, J. P. et al. Modern diet and metabolic variance—A recipe for disaster?. Nutr. J. 13, 15 (2014).
Lennerz, B. & Lennerz, J. K. Food addiction, high-glycemic-index carbohydrates, and obesity. Clin. Chem. 64(1), 64–71 (2018).
Hall, K. A review of the carbohydrate–insulin model of obesity. Eur. J. Clin. Nutr. 71(3), 323–326 (2017).
Roccisano, D. & Henneberg, M. Soy consumption and obesity. Food Nutr. Sci. 03(02), 260–266 (2012).
You, W. & Henneberg, M. Cereal crops are not created equal: Wheat consumption associated with obesity prevalence globally and regionally. AIMS Public Health 3(2), 313–328 (2016).
The World Bank. Urban Development-Overview (2020) https://www.worldbank.org/en/topic/urbandevelopment/overview#:~:text=With%20more%20than%2080%25%20of,and%20new%20ideas%20to%20emerge (Accessed 25 June 2022).
Malik, V. S., Willett, W. C. & Hu, F. B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 9(1), 13–27 (2013).
Johnson, J. A. III. & Johnson, A. M. Urban-rural differences in childhood and adolescent obesity in the United States: A systematic review and meta-analysis. Childhood Obes. 11(3), 233–241 (2015).
Carruba, M. O. et al. The European Association for the study of obesity (EASO) endorses the milan charter on urban obesity. Obes. Facts 14(1), 163–168 (2021).
WHO. Obesity and overweight-key facts (2021) https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Pirgon, Ö. & Aslan, N. The role of urbanization in childhood obesity. J. Clin. Res. Pediatr. Endocrinol. 7(3), 163–167 (2015).
Fezeu, L. et al. Waist circumference and obesity-related abnormalities in French and Cameroonian adults: The role of urbanization and ethnicity. Int. J. Obes. 34(3), 446–453 (2010).
You, W. & Henneberg, M. Relaxed natural selection contributes to global obesity increase more in males than in females due to more environmental modifications in female body mass. PLoS ONE 13(7), e0199594 (2018).
Staub, K. et al. Increasing variability of body mass and health correlates in Swiss conscripts, a possible role of relaxed natural selection? Evol. Med. Public Health (2018) (Accepted April 23, 2018).
Budnik, A. & Henneberg, M. Worldwide increase of obesity is related to the reduced opportunity for natural selection. PLoS ONE 12(1), e0170098 (2017).
Veblen, T. Theory of the Leisure Class (Kelley, 1889).
Wang, Y. & Lim, H. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int. Rev. Psychiatry 24(3), 176–188 (2012).
Newton, S., Braithwaite, D. & Akinyemiju, T. F. Socio-economic status over the life course and obesity: Systematic review and meta-analysis. PLoS ONE 12(5), e0177151 (2017).
Keane, E. et al. Measured parental weight status and familial socio-economic status correlates with childhood overweight and obesity at age 9. (2012).
Akarolo-Anthony, S. N. et al. Obesity epidemic has emerged among Nigerians. BMC Public Health 14(1), 1–9 (2014).
Seubsman, S.-A. et al. Socioeconomic status, sex, and obesity in a large national cohort of 15–87-year-old open university students in Thailand. J. Epidemiol. 20(1), 13–20 (2010).
Hall, K. D. & Kahan, S. Maintenance of lost weight and long-term management of obesity. Med. Clin. 102(1), 183–197 (2018).
Ryan, D. H. & Yockey, S. R. Weight loss and improvement in comorbidity: Differences at 5%, 10%, 15%, and over. Curr. Obes. Rep. 6(2), 187–194 (2017).
Bacon, L. & Aphramor, L. Weight science: Evaluating the evidence for a paradigm shift. Nutr. J. 10(1), 1–13 (2011).
Di Angelantonio, E. et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 388(10046), 776–786 (2016).
Choquet, H. & Meyre, D. Genetics of obesity: What have we learned?. Curr. Genomics 12(3), 169–179 (2011).
The World Bank: International Comparison Program database: World Development Indicators. GDP (current US$) per capita per year (2010) http://data.worldbank.org (Accessed 26 Nov 2015).
WHO. Global Health Observatory, the data repository. (WHO, 2015) https://www.who.int/data/gho/data/indicators/indicator-details/GHO/uv-radiation (Accessed 26 Nov 2015).
FAO. Food Balance Sheets. A Handbook (Food and Agriculture Organization, 2021).
Rao, N. D. et al. Healthy, affordable and climate-friendly diets in India. Glob. Environ. Chang. 49, 154–165 (2018).
Colchero, M. A. et al. Affordability of food and beverages in Mexico between 1994 and 2016. Nutrients 11(1), 78 (2019).
Bai, Y. et al. Cost and affordability of nutritious diets at retail prices: Evidence from 177 countries. Food Policy 99, 101983 (2021).
You, W. et al. Greater family size is associated with less cancer risk: An ecological analysis of 178 countries. BMC Cancer 18(1), 1–14 (2018).
You, W.-P. & Henneberg, M. Type 1 diabetes prevalence increasing globally and regionally: The role of natural selection and life expectancy at birth. BMJ Open Diabetes Res. Care 4(1), e000161 (2016).
Henneberg, M. Reproductive possibilities and estimations of the biological dynamics of earlier human populations. J. Hum. Evol. 5, 41–48 (1976).
Henneberg, M. & Piontek, J. Biological state index of human groups. Przeglad Anthropologiczny XLI, 191–201 (1975).
The United Nations. World Fertility Data 2008 (2012) http://www.un.org (Accessed 29 July 2015).
WHO. World Health Statistics. Life Tables for WHO Member States 2012 (World Health Organization, 2012).
WHO. Urban Health (2022) https://www.who.int/health-topics/urban-health#tab=tab_1 (Accessed 12 Mar 2022).
Congdon, P. Obesity and urban environments. Int. J. Environ. Res. Public Health 16(3), 464 (2019).
Contreras, D. A. et al. Rural–urban differences in body mass index and obesity-related behaviors among low-income preschoolers. J. Public Health 43(4), e637–e644 (2021).
de Bont, J. et al. Urban environment and obesity and weight-related behaviours in primary school children. Environ. Int. 155, 106700 (2021).
WHO. WHO|Obesity. (WHO, 2015) http://who.int/topics/obesity/en/.
Siervo, M. et al. Sugar consumption and global prevalence of obesity and hypertension: An ecological analysis. Public Health Nutr. 17(3), 587–596 (2014).
You, W. & Henneberg, M. Meat in modern diet, just as bad as sugar, correlates with worldwide obesity: An ecological analysis. J. Nutr. Food Sci. 6(517), 4 (2017).
Basu, S. et al. The relationship of sugar to population-level diabetes prevalence: An econometric analysis of repeated cross-sectional data. PLoS ONE 8(2), e57873 (2013).
Basu, S. et al. Nutritional determinants of worldwide diabetes: An econometric study of food markets and diabetes prevalence in 173 countries. Public Health Nutr. 16(1), 1–8 (2013).
Weeratunga, P. et al. Per capita sugar consumption and prevalence of diabetes mellitus—Global and regional associations. BMC Public Health 14, 186–191 (2014).
You, W. & Henneberg, M. Cancer incidence increasing globally: The role of relaxed natural selection. Evol. Appl. 00, 1–13 (2017).
You, W. et al. Decreasing birth rate determining worldwide incidence and regional variation of female breast cancer. Adv. Breast Cancer Res. 07(01), 1–14 (2018).
You, W., Symonds, I. & Henneberg, M. Low fertility may be a significant determinant of ovarian cancer worldwide: An ecological analysis of cross-sectional data from 182 countries. J. Ovarian Res. 11(1), 68 (2018).
O’brien, R. M. A caution regarding rules of thumb for variance inflation factors. Qual. Quant. 41(5), 673–690 (2007).
Cumming, G. Inference by eye: Reading the overlap of independent confidence intervals. Stat. Med. 28(2), 205–220 (2009).
United Nations Statistics Division. Composition of macro geographical (continental) regions, geographical sub-regions, and selected economic and other groupings (2013) http://unstats.un.org (Accessed 03 Oct 2016).
WHO. WHO regional offices. http://www.who.int (Accessed 26 Nov 2015).
Asia Cooperation Dialogue. Member Countries. (2018) http://www.acddialogue.com.
The World Bank. Arab World|Data. (2015) http://data.worldbank.org/region/ARB.
The European Free Trade Association. What is the European Economic Area? http://www.efta.int/eea (Accessed 24 Sept 2015).
European Union. EUROPA-Countries (2022) http://europa.eu (Accessec 18 June 2015).
The United Nations Educational Scientific and Cultural Organization. UNESCO Regions-Latin America and the Caribbean. (2014) http://www.unesco.org.
OECD. List of OECD Member countries. (2015) http://www.oecd.org.
South Africa Development Community. Southern African Development Community: Member States. (2015) http://www.sadc.int (Accessed 18 June 2015).
Finucane, M. M. et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 377(9765), 557–567 (2011).
Wells, J. C. et al. Associations of economic and gender inequality with global obesity prevalence: Understanding the female excess. Soc. Sci. Med. 75(3), 482–490 (2012).
Lee, A., Cardel, M. & Donahoo, W. T. Social and Environmental Factors Influencing Obesity (2015).
Addo, I. Y. et al. Socio-cultural beliefs about an ideal body size and implications for risk of excess weight gain after immigration: A study of Australian residents of sub-Saharan African ancestry. Ethn. Health 26(8), 1209–1224 (2021).
Chatham, R. E. & Mixer, S. J. Cultural influences on childhood obesity in ethnic minorities: A qualitative systematic review. J. Transcult. Nurs. 31(1), 87–99 (2020).
Heather, A. K. et al. Biological and socio-cultural factors have the potential to influence the health and performance of elite female athletes: A cross sectional survey of 219 elite female athletes in Aotearoa New Zealand. Front. Sports Active Living 27 (2021).
Siega-Riz, A. M. et al. The current understanding of gestational weight gain among women with obesity and the need for future research. NAM Perspect. 2020 (2020).
Garawi, F. et al. Global differences between women and men in the prevalence of obesity: Is there an association with gender inequality?. Eur. J. Clin. Nutr. 68(10), 1101 (2014).
Quittkat, H. L. et al. Body dissatisfaction, importance of appearance, and body appreciation in men and women over the lifespan. Front. Psychiatry 10, 864 (2019).
Voges, M. M. et al. Gender differences in body evaluation: Do men show more self-serving double standards than women?. Front. Psychol. 10, 544 (2019).
Noh, J.-W. et al. Gender differences and socioeconomic status in relation to overweight among older Korean people. PLoS ONE 9(5), e97990 (2014).
Joh, H.-K. et al. Gender and socioeconomic status in relation to weight perception and weight control behavior in Korean adults. Obes. Facts 6(1), 17–27 (2013).
Ferris, W. F. & Crowther, N. J. Once fat was fat and that was that: Our changing perspectives on adipose tissue. Cardiovasc. J. Afr. 22(3), 147–154 (2011).
Ngo, N. T. What historical ideals of women’s shapes teach us about women’s self-perception and body decisions today. AMA J. Ethics 21(10), E879-901 (2019).
Ma, X. et al. Diet and human reproductive system: Insight of omics approaches. Food Sci. Nutr. 10(5), 1368–1384 (2022).
Gurven, M. et al. Health costs of reproduction are minimal despite high fertility, mortality and subsistence lifestyle. Sci. Rep. 6(1), 1–10 (2016).
Miles, C. & Benn, T. A case study on the experiences of university-based Muslim women in physical activity during their studies at one UK higher education institution. Sport Educ. Soc. 21(5), 723–740 (2016).
WHO. Global Strategy on Diet, Physical Activity and Health-Physical Activity and Women (2021) https://www.who.int/dietphysicalactivity/factsheet_women/en/ (Accessed 25 Dec 2021).
WHO, GHO|By category|Insufficient physical activity, in WHO (World Health Organization, 2015).
Kahan, D. Adult physical inactivity prevalence in the Muslim world: Analysis of 38 countries. Prev. Med. Rep. 2, 71–75 (2015).
Al-Eisa, E. S. & Al-Sobayel, H. I. Physical activity and health beliefs among Saudi women. J. Nutr. Metab. 2012 (2012).
Alrashidi, K. & Sekhar, K. C. Overweight and obesity among adolescents school females in Buraidah city. World J. Pharm. Res. 9(12), 821–834 (2020).
Mabry, R. et al. Evidence of physical activity participation among men and women in the countries of the Gulf Cooperation Council: A review. Obes. Rev. 11(6), 457–464 (2010).
Al-Habsi, A. & Kilani, H. Lifestyles of Adult Omani Women: Cross-sectional study on physical activity and sedentary behaviour. Sultan Qaboos Univ. Med. J. 15(2), e257 (2015).
Deforche, B. et al. Changes in weight, physical activity, sedentary behaviour and dietary intake during the transition to higher education: A prospective study. Int. J. Behav. Nutr. Phys. Act. 12(1), 1–10 (2015).
McCarthy, C. & Warne, J. P. Gender differences in physical activity status and knowledge of Irish University staff and students. Sport Sci. Health 1–9 (2022).
Stivens, M. Becoming modern in Malaysia: Women at the end of the twentieth century. In Women in Asia 16–38 (Routledge, 2020).
Safa, H. I. The Myth of the Male Breadwinner: Women and Industrialization in the Caribbean (2018).
Horning, M. et al. Reasons parents buy prepackaged, processed meals: It is more complicated than “I don’t have time”. J. Nutr. Educ. Behav. 49(1), 60-66.e1 (2016).
Whitsett, D., Sherman, M. F. & Kotchick, B. A. Household food insecurity in early adolescence and risk of subsequent behavior problems: Does a connection persist over time?. J. Pediatr. Psychol. 44, 4478–4489 (2019).
Bissonnette-Maheux, V. et al. Exploring women’s beliefs and perceptions about healthy eating blogs: A qualitative study. J. Med. Internet Res. 17, e87 (2015).
Alkazemi, D. Gender differences in weight status, dietary habits, and health attitudes among college students in Kuwait: A cross-sectional study. Nutr. Health 25(2), 75–84 (2018).
van Uffelen, J. G. Z., Khan, A. & Burton, N. W. Gender differences in physical activity motivators and context preferences: A population-based study in people in their sixties. BMC Public Health 17(1), 624–624 (2017).
Mao, H.-Y., Hsu, H.-C. & Lee, S.-D. Gender differences in related influential factors of regular exercise behavior among people in Taiwan in 2007: A cross-sectional study. PLoS ONE 15(1), e0228191–e0228191 (2020).
Asadollahi, T. et al. Effectiveness of mindfulness training and dietary regime on weight loss in obese people. J. Med. Life 8(Spec Iss 4), 114–124 (2015).
Camilleri, G. M. et al. Association between mindfulness and weight status in a general population from the NutriNet-Santé study. PLoS ONE 10(6), e0127447–e0127447 (2015).
Salvo, V. et al. Mindfulness as a complementary intervention in the treatment of overweight and obesity in primary health care: Study protocol for a randomised controlled trial. Trials 19(1), 277–277 (2018).
Traversy, G. & Chaput, J.-P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 4(1), 122–130 (2015).
Albani, V. et al. Examining associations between body mass index in 18–25 year-olds and energy intake from alcohol: Findings from the health survey for England and the Scottish Health Survey. Nutrients 10(10), 1477 (2018).
Faruque, S. et al. The dose makes the poison: Sugar and obesity in the United States—a review. Pol. J. Food Nutr. Sci. 69(3), 219–233 (2019).
Shin, S. M. Association of meat intake with overweight and obesity among school-aged children and adolescents. J. Obes. Metab. Syndr. 26(3), 217–226 (2017).
Serrano Fuentes, N., Rogers, A. & Portillo, M. C. Social network influences and the adoption of obesity-related behaviours in adults: A critical interpretative synthesis review. BMC Public Health 19(1), 1178–1220 (2019).
Nargund, G. Declining birth rate in Developed Countries_A radical policy re-think is required. Facts Views Vis. Obgyn 1(3), 191–193 (2009).
Grantham, J. P. & Henneberg, M. The estrogen hypothesis of obesity. PLoS ONE 9(6), e99776 (2014).
Brown, L. M. et al. Metabolic impact of sex hormones on obesity. Brain Res. 1350, 77–85 (2010).
Egger, G., Swinburn, B. & Islam, F. A. Economic growth and obesity: An interesting relationship with world-wide implications. Econ. Hum. Biol. 10(2), 147–153 (2012).
Ameye, H. & Swinnen, J. Obesity, income and gender: The changing global relationship. Glob. Food Sec. 23, 267–281 (2019).
Power, M. L. & Schulkin, J. Sex differences in fat storage, fat metabolism, and the health risks from obesity: Possible evolutionary origins. Br. J. Nutr. 99(5), 931–940 (2008).
Zore, T., Palafox, M. & Reue, K. Sex differences in obesity, lipid metabolism, and inflammation—a role for the sex chromosomes?. Mol. Metab. 15, 35–44 (2018).
Chen, X. et al. The number of x chromosomes causes sex differences in adiposity in mice. PLoS Genet. 8(5), e1002709 (2012).
Author information
Authors and Affiliations
Contributions
W.Y. conceived the hypothesis and discussed it with M.H. for consolidation. W.Y. extracted the data, and conducted analyses together with M.H. before interpreting the analysis results. W.Y. drafted the text with contributions from M.H.; and both authors reviewed, edited and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
You, W., Henneberg, M. Significantly different roles of economic affluence in sex-specific obesity prevalence rates: understanding more modifications within female body weight management. Sci Rep 12, 15757 (2022). https://doi.org/10.1038/s41598-022-19633-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19633-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
