
Abstract
This systematic review was aimed to evaluate occurrence of secondary caries and marginal adaptation in ion-releasing materials versus resin composite. Electronic search of PubMed, Scopus, and Open Grey databases with no date or language restrictions until May 21st, 2021, was conducted. Randomized clinical trials that compared ion-releasing restorations versus resin composite were included. For quantitative analysis, a random-effects meta-analysis with risk difference as an effect measure and a 95% confidence interval was used. Quality of evidence was assessed using The Grading of Recommendations, Assessment, Development, and Evaluation criteria. The risk of bias was evaluated using the Cochran Collaboration Risk of Bias tool. The inclusion criteria were met by 22 studies, and 10 studies were included in the meta-analysis. Three follow-up periods (1 year, 18 months–2 years, and 3 years) were evaluated. The overall quality of evidence for secondary caries and marginal adaptation outcomes was low. The results of the meta-analysis showed no significant difference (p > 0.05) in both outcomes between ion-releasing materials and resin composite. The occurrence of secondary caries was not dependent on the nature of the restorative material. It is more likely a complex process that involves the same risk factors as primary carious lesions.
Similar content being viewed by others


Introduction
Over the last decade, remarkable advances in resin composite formulations have been made to address clinical challenges. Bulk-placement techniques, new filler formulations, and simplified adhesion protocols have resulted in a more user-friendly application1,2. However, the clinical problems of technique sensitivity, polymerization shrinkage, and lack of antibacterial properties remained unchanged3,4,5 and similarly, the main reasons for its failure remain to be secondary caries and bulk fractures1,6.
Secondary caries can be defined as caries lesions at the margins of existing restorations7 or caries associated with restorations or sealants (CARS) (secondary caries and caries around restorations are used synonymously in this review)8,9. The complexity of caries around restorations is related to its multifactorial origin, combining the pathological pathway of primary carious lesions with the influence of the formulations of different restorative materials9. It has been reported that thicker biofilms accumulate around resin composite than glass ionomer restorations10. In vivo plaque studies have also shown that the levels of lactic acid-producing bacteria are significantly higher around resin composite restorations than on either amalgam or glass ionomer restorations11,12. Therefore, fluoride-releasing materials that possess remineralization and/or antibacterial properties have gained popularity in recent years13 with the hope of preventing secondary caries formation.
Conventional glass ionomer cement (GICs) and its evolutions such as: high-viscosity glass ionomer (HV-GIC), resin-modified glass ionomer (RMGIC), and compomers are the most frequently used fluoride-releasing restorative materials. An inherent disadvantage of GIC is its low fracture toughness, which limits its clinical applications to low load-bearing areas such as the buccal and lingual surfaces. Nevertheless, increasing the powder-liquid ratio, and modifications in its chemical composition have shown to lead to improved physical properties and prolonged clinical survival14,15.
Modified versions of the conventionally set GIC such as HV-GIC were introduced with the hope of extending the indications of GIC to include load-bearing areas on posterior teeth to provide an alternative for patients with limited resources16,17,18. Promising 10-years clinical results have recently emerged for HV-GIC used in class I and II restorations, where no restoration had to be replaced due to unacceptable clinical wear19. In addition to HV-GIC, glass hybrid materials such as Equia Forte were introduced in 2015. According to the manufacturer, these materials are modified with highly reactive glass particles of different sizes to significantly increase their mechanical properties20,21.
Nonetheless, the clinical indications of GIC and its evolutions in multiple-surface restorations in the stress-bearing posterior regions of the mouth are still limited due to their poor fracture toughness, tensile strength, wear resistance, and hardness. A recent systematic review reported that the annual failure rates of approximal or multi-surface GIC restorations were greater than those of single-surface occlusal restorations22. A solution to counteract this limitation of GIC is to incorporate resin composite restorations (which have superior mechanical properties than GIC) with reactive fillers that can protect the tooth against secondary caries23. Up to press date, there are several new commercially available ion-releasing composites with claimed bioactivity such as ACTIVA™ BioACTIVE-RESTORATIVE™ (Pulpdent Corporation, Watertown, MA, USA), Cention N (Ivoclar Vivadent, Schaan, Liechtenstein), and Surefil one (Dentsply Sirona). These materials are relatively recent additions to the realm of ion-releasing materials, that are claimed by their respective manufacturer, to release sufficient amounts of ions other than fluoride to promote remineralization24,25,26 around restorations. Tiskaya et al. 27, reported significant release of Al3+ and Ca2+ ions from Cention N and Activa Bioactive in acidic media of pH 4, which in turn indicate an ability to protect against secondary caries.
Clinical investigations regarding their ability to inhibit caries around restorations are scarce in the current literature. While in vitro studies have shown that fluoride-releasing restorative materials such as GICs can inhibit tooth demineralization adjacent to restoration margins28,29,30, the caries inhibitory effect of these new ion-releasing materials remains unclear. Therefore, this systematic review and meta-analysis were aimed to answer the following question: Is there a difference in the occurrence of secondary caries and marginal adaptation in ion-releasing restorations compared to resin composite?
Materials and methods
The recommendation of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) were followed in this review31,32.
Eligibility criteria and PICO question
The research question was as follows: Is there a difference in the incidence secondary caries and marginal adaptation in ion-releasing restorations compared to resin composite?
The following PICO questions were established:
-
Population: patients with permanent dentition in need of restorations.
-
Intervention: ion-releasing restorations. From here forth, the term ‘ion-releasing’ will be used in this article to encompass fluoride and all other ion-releasing materials. All GIC derivatives including (RMGIC, HV-GIC, conventional GIC, and glass hybrid), polyacid-modified composite (compomer), giomer, and any material stated by the manufacturer to be capable of ion-release will be in the intervention group.
-
Comparison: the intervention should be compared with a resin composite restoration applied in conjunction with any adhesive system.
-
Outcomes: caries around restorations and marginal adaptation.
Inclusion criteria
-
1.
Randomized clinical trials in patients with permanent dentition comparing an ion-releasing material to resin composite in any form of cavities (Black’s Class I, II, V) and non-carious cervical lesions (NCCLs).
-
2.
Parallel or split-mouth studies.
-
3.
A minimum follow-up period of 1 year.
-
4.
Evaluation criteria: FDI criteria and/or USPHS.
-
5.
The investigated materials must be commercially available. Any study investigating discontinued products was excluded.
Exclusion criteria
-
1.
Editorial letters, pilot studies, historical reviews, literature reviews, systematic reviews, in vitro studies, cohort, observational and descriptive studies, such as case reports and case series.
-
2.
Randomized clinical trials were excluded if.
-
a.
Ion-releasing materials were compared to each other with no resin composite restoration as a reference for comparison.
-
b.
Restorations were done on primary teeth,
-
c.
The follow-up period was less than 1 year.
-
a.
Information source and search strategy
An electronic search within the following databases (Medline via PubMed and Scopus) was conducted until May 21st, 2021. Grey literature was searched through the Open Grey database http://www.opengrey.eu/.
The following keywords were used in the electronic search: “FDI criteria AND randomized clinical trial”, “modified USPHS criteria AND randomized clinical trials”, “Secondary caries OR caries adjacent to restorations and randomized clinical trials”, “marginal adaptation and randomized clinical trial”, “ion releasing restorations OR bioactive resin composite OR bio interactive restorations AND clinical trials”. To identify ongoing clinical trials, we also searched the ClinicalTrials.gov website. The outcome of the search among the abovementioned databases was comprehensively checked and duplicated results was excluded.
To minimize publication bias, no language or publication date restrictions were applied. Two reviewers (E.H. and H.H.) independently extracted data and assessed their eligibility and risk of bias. Any disagreements were resolved by consulting a third reviewer (H.C.).
Study selection and assessment of eligibility
According to the search strategy, assessment of the eligibility of trials was performed by the two reviewers according to the relevance of the title. Abstracts of studies that could not be excluded based on the title were retrieved and evaluated. At the final stage of evaluation, full texts were assessed to determine if they met the predetermined inclusion criteria. The included studies received an identification code composed of the first author’s last name and the year of publication.
Two reviewers extracted data from included studies such as the number of patients and restorations per group, intervention, and comparator, follow-up period, study design, evaluation criteria, adhesive strategy, cavity design, isolation technique, patient’s age, settings, and location of data collection. In studies that reported multiple follow-up periods, data from the longest follow-up were extracted. If more than one type of resin composite was used, the data were combined into a single entry. For ion-releasing restorations, GIC-based restorations (HVGIC, glass hybrid, and RMGIC) were combined into a single entry and compomer restorations were pooled together.
Assessment of risk of bias
The Risk of Bias (RoB) of the included studies was assessed using the Cochrane Collaboration Risk of Bias Tool (version 2.0) for RCTs33. The six domains of the RoB Tool are assessment of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of the outcome assessors, incomplete outcome data (attrition bias), selective outcome reporting, and other sources of bias. In this study, the other sources of bias domain was not included. Each entry received a judgment of low, unclear, or high risk of bias. At the study level, a study was considered at low risk of bias if all 5 domains of the RoB tool for each outcome were at low risk of bias. If one or more domains were judged to have unclear risk, the study was judged to have unclear risk. If at least one item was considered at high risk of bias, the study was considered to have a high risk of bias.
Assessment of quality of evidence
The confidence in evidence was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE)34. According to GRADE, the body of evidence can be rated as high, moderate, low, or very low. The GRADE pro-Guideline Development Tool (www.gradepro.org) was used to create a summary-of-findings table.
The strength of cumulative evidence was assessed based on, the risk of bias, inconsistencies, indirectness, imprecision, and publication bias. The data were summarized in the summary of findings (Table 2). The quality of evidence for the first 4 domains may be downgraded by 1, 2, or 3 levels based on “serious or very serious risks. Publication bias may either be suspected or undetected. In the case of suspected bias, downgrading by 2 levels was made35,36.
Synthesis of data
Data were analysed using Revman 5.4 (Review Manager Version 5.4, The Cochrane Collaboration, Copenhagen, Denmark). Data from included studies were either dichotomous for the “Secondary Caries” outcome measure or ordinal for the “Marginal Adaptation” outcome measure. Marginal adaptation data were dichotomized to NO representing Alpha and Bravo scores of the modified USPHS criteria, and scores 1 and 2 of the FDI criteria, or YES corresponding to Charlie and Delta scores of the modified USPHS criteria, and 3, 4, and 5 scores of the FDI criteria. Risk differences as an effect measure with 95% confidence intervals and random effects model were employed. Heterogeneity was evaluated using the Q test and I2 statistics, where 25%, 50%, and 75% represent low, moderate heterogeneity, and high heterogeneity respectively. For both the outcomes (secondary caries and marginal adaptation), data from 3 follow-up periods were included, i.e., 1 year, 18 months—2 years, and 3 years. For secondary caries outcome, two analyses were performed, one with all types of cavities, and one for load-bearing cavities.
Results
Search details
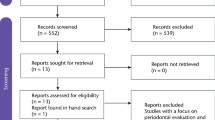
The initial search in the databases resulted in 3744 studies being identified after duplicates exclusion. After title screening, 3584 articles were excluded, and the remaining 160 abstracts were further assessed for eligibility. Articles that had multiple reports corresponding to different follow-up periods were combined into a single entry and the data of the longest follow-up were included in this study. This process culminated in 39 studies that were to be progressed to full-text analysis. Subsequent full-text analysis of these studies resulted in 22 studies that met the inclusion criteria (Fig. 1).

Prisma flow chart of the study selection process.
Risk of bias evaluation
Overall, 3 studies were deemed to have a low risk of bias19,37,38, 3 studies showed39,40,41 unclear risk of bias while the remaining 16 studies had a high risk of bias. Seven studies17,42,43,44,45,46,47 did not report random sequence generation, while 50% of the included studies reported allocation concealment. Performance bias was unclear in the majority of studies (16 out of 22), while outcome assessment was blinded in all studies except for 343,48,49. No attrition bias was noticed in any of the included studies except for one44, which did not adequately report the number of dropouts (Fig. 2).

Risk of bias summary: authors' judgments about each risk of bias item for each included study. Filled Green circle Low ROB Filled Red circle High ROB Filled Yellow Circle Unclear ROB.
Included studies characteristics
The characteristics and methodological assessment of the 22 included studies are summarized in Table 1. In 15 of the included studies16,19,37,38,41,42,43,44,46,47,48,50,51,52,53, split-mouth design was employed while 7 studies reported a parallel study design17,39,40,45,49,54,55. Most of the studies employed the modified USPHS criteria for restorations evaluation except for 4 studies16,17,50,51 that used FDI criteria. One study43 used the McComb et al., criteria56. Five studies used HV-GIC16,17,19,39,49. Two studies used glass hybrid38,51. Resin-modified glass ionomer was used in 9 studies37,41,42,43,45,50,52,54,57, while 2 studies used conventional GIC43,53. Compomer (poly-acid modified composite) was used in 7 studies40,44,45,46,47,48,54. Most of the studies used nano- or micro-hybrid composite. Bulk-fill composite was used in one study39. Nano-filled composite was used in 2 studies46,57 while one study used micro-filled composite44. Most follow-up periods ranged between 2 and 3 years. Long-term follow-up was reported in 2 studies19,40 which had a follow-up period of 10 and 7 years respectively. One study41 was terminated after 1 year due to an unacceptable failure rate. Class II cavities were reported in 7 studies19,39,41,47,49,51. Class I cavities were evaluated in 3 studies 17,19,41. Non-carious cervical lesions were evaluated in 11 studies16,38,42,44,45,46,48,50,52,53,57. Class V carious lesions were evaluated in 4 studies37,40,43,54. For HV-GIC, glass hybrid, and conventional GIC, Cavity conditioner of poly-acrylic acid was used in all studies except 2 which did not report any type of pre-treatment38,53. For RMGIC, 2 studies used 37% phosphoric acid etching for 5 s37,41. Two studies used Vitremer primer45,52 while another study used GC cavity conditioner for RMGIC, and Ketac nano primer for nano-filled RMGIC42,57. For Compomer, 5 studies used self-etch adhesive (SE)40,45,46,48,54, while 2 studies used etch-and-rinse adhesive (ER)44,47.
For resin composite,8 studies used ER adhesive system16,37,42,43,44,45,47,52,57 while 9 studies used SE adhesives17,19,40,41,46,48,50,51,54. Two studies used a universal adhesive in selective etch mode38,49, 1 in SE mode39, and 1 in ER mode53. For moisture control, cotton rolls and saliva ejectors were reported in the majority of studies except for 3 studies that used rubber dam isolation44,51,52.
Patients in all studies had no systemic diseases except two43,53. In one study53, patients were required to have at least one systemic disease and the other one43 included subjects who were xerostomic, head and neck, cancer patients who received radiation therapy. Ten studies16,19,37,38,39,41,49,50,51,53 were published in the years (2018–2020) with 6 in 2020, 3 in 2019, and 1 in 2018. No studies were identified from January to May of 2021. Five studies17,40,43,52,57 were published between 2010 and 2014. Seven studies42,44,45,46,47,48,54 were published before 2010.
Descriptive analysis
Studies that reported secondary caries and marginal adaptation in different follow-up periods were included in the meta-analysis (Figs. 3, 4, 5). For secondary caries outcome for all types of cavities, the meta-analysis was grouped as follows: ion releasing materials (GIC) vs resin composite (RC) with the following 3 follow-up periods, i. e. 1 year, 18–24 months, and 3 years. For secondary caries in load-bearing cavities, ion-releasing material (GIC and compomer) vs resin composite, and data were extracted from the last follow-up.

Forest plot of comparison: Ion releasing restoration (GIC) versus resin composite, outcome: 1.1 Secondary caries for all types of cavities.

Forest plot of comparison: Ion releasing restoration versus resin composite, outcome: 1.2 Secondary caries for load-bearing cavities.

Forest plot of comparison: Ion releasing restoration (GIC) versus resin composite, outcome: 1.3 marginal adaptation.
The difference in the number of studies in each follow-up is attributed to whether the outcome was reported by the authors. For marginal adaptation outcome, GIC vs resin composite comparison was evaluated at the same 3 follow-up periods. secondary caries was not reported in all studies that compared compomer and resin composite at different follow-up periods. Therefore, no meta-analysis was performed for compomer vs resin composite comparison. Out of a total of 1448 GIC restorations, only 15 showed secondary caries with a percentage of 0.8%. Similarly, 16 composite restorations failed due to caries out of 1637 with a percentage of 0.9%. In all studies that compared compomer and resin composite, no occurrence of secondary caries was observed over the follow-up periods which ranged between 2 and 3 years.
Meta-analysis
Secondary caries
The risk difference for the comparison between GIC and RC for the 1-year and18 month–2 years follow-up periods was -0.00 with 95% CI between [− 0.1–0.01]. The 3-year follow-up risk difference was 0.00 with 95% CI between [− 0.2–0.02] with no occurrence of secondary caries in both arms. There was no statistically significant difference (P = 0.61) between GIC and RC in secondary caries development at any of the follow-up periods. For a total of 1448 GIC restorations, 15 failed due to secondary caries, in comparison with 16 out of 1637 composite restorations. Overall heterogeneity was low with I2 = 0%. (Fig. 3). For secondary caries in load-bearing cavities, the risk difference was 0.0 with 95% CI between [− 0.01–0.02]. No statistically significant difference (P = 0.77) was found between ion-releasing material and secondary caries.
Marginal adaptation
The risk difference for the 1-year follow-up was 0.0.1 with 95% CI between [− 0.02–0.03]. Heterogeneity was high with an I2 = 75%. No statistically significant difference (p ˃ 0.5) was found between the 2 materials. At 18 months–2 years follow-up, the risk difference was 0.03 with 95% CI between [− 0.02–0.08]. Heterogeneity was high with an I2 = 94%. At the 3-year follow-up, the risk difference was 0.00 with 95%CI between [− 0.02–0.02]. Heterogeneity was low with an I2 = 0%.
The overall risk difference was 0.01 with 95%CI between [− 0.01–0.03]. Out of a total of 1255 GIC restorations, 78 showed unacceptable marginal adaptation compared to 16 out of 1470 RC restorations. No statistically significant difference was found between the 2 materials. Overall heterogeneity was high with an I2 = 84%. (Fig. 4).
GRADE quality of evidence
Assessment of the quality of evidence for secondary caries and marginal adaptation outcomes for the 3 follow-up periods (1 year, 18–24 months, and 3 years) was low. This finding suggests that the confidence in the effect estimate is limited, and that further research is likely to have an impact on the confidence of the estimate of effect (Table 2).
Discussion
This systematic review discussed the occurrence of secondary caries in ion-releasing materials versus resin composite. Glass ionomer and its derivatives are the most clinically reported ion-releasing materials. Compomer was less frequently used. The results of the meta-analysis showed no significant difference between the secondary caries in resin composite and all derivatives of GIC.
Secondary caries is influenced by several factors with the most frequent ones being: the location of the lesion (cervical, proximal, or occlusal), patient’s caries risk, age, and socioeconomic status, operator’s skills variation, and detection methods and criteria58. The majority of studies included in this review were conducted in university settings with trained operators and under standardized conditions with patients who demonstrated moderate oral hygiene. This could explain the low number of events. Secondary caries was found to be more frequent in practice-based settings7. This could be attributed to the technique sensitivity of composite placement that requires highly skilled and calibrated operators which is often the case in university settings59. Regarding operative procedures, the majority of studies in this review used cotton rolls and saliva ejectors for moisture control while only 3 studies reported rubber dam isolation. Previous literature reported no significant difference between the survival of composite restorations performed under either of the isolation protocols60.
The location of the lesion is an important factor that could explain the generally low incidence of events. Around 45% of the included studies involved NCCL which are less affected by secondary caries than posterior occlusal and proximal cavities59. Secondary caries is reported to be more frequent with deep proximal restorations with gingival margins extending beyond the cementoenamel junction with dentine and cementum as the substrate61,62. Furthermore, the placement of such restorations is highly technique sensitive and isolation in every restorative step cannot be strictly followed9.
The Patient’s caries susceptibility is crucial in secondary caries development, as primary caries and secondary caries are inherently the same diseases and consequently patients with high caries risk are more suspectable to secondary caries63. The findings of this review were based on the results of studies performed on a population of healthy individuals with good to moderate oral hygiene and with no debilitating conditions. One exception is the study by De Moor et al.43, in which the population was head and neck xerostomic cancer patients who received radiation therapy. De Moor et al. 43, reported a significantly higher failure rate due to secondary caries in resin composite restorations in comparison with conventional GIC. Nevertheless, the findings of this study cannot be generalized as this population is highly specific. However, the difference in the performance of different materials in populations with compromised oral health indicates that patient factors could be more influential than the choice of material.
Adhesive strategy and interfacial gap formation were speculated to play a role in secondary caries development. Gaps at the margins of restorations can permit bacterial invasion and biofilm accumulation along the tooth/restoration interface64. However, until now there is no Conesus in the literature regarding the role of gaps in secondary caries development. In a study by Kidd et al.,65, it was suggested that microleakage cannot solely induce active demineralization beneath a restoration, only when bacterial invasion takes place at the composite-restoration interface, the size of the gap becomes pertinent.
The durability of the adhesive interface is critical for the survival of resin composite restorations, especially with dentin margins. Several attempts have been made to increase the durability of adhesives to dentine including using MMPs inhibitors, biomimetic remineralization, and increasing the hydrophobicity of the adhesive66,67,68. The adhesion protocols in this systematic review varied between etch-and-rinse (9 studies) and self-etch adhesives (8 studies), while 2 studies used universal adhesives in selective etch mode38,49, one in SE mode39 and one in ER mode53. The findings of this systematic review suggest that regarding secondary caries development, all adhesive strategies performed similarly considering the low number of events. In a previous study that utilized a short-term in vitro biofilm model69, the adhesive type affected carious lesion development and progression in gaps. However, a recent systematic review and Network meta-analysis showed similar performance of all adhesive strategies in preventing secondary caries70. It is worth mentioning that the impact of adhesive strategy/type on secondary caries development was not assessed quantitatively in this review, considering the overall scarcity of secondary caries occurrence in the included follow-up periods.
The short follow-up period (2–3 years) in the majority of studies might have contributed to an overall low incidence of events. Longer-term follow-up clinical trials showed an increased reporting of secondary carious lesions71,72. According to the findings of a recent review59, the highest mean incidence of secondary caries development was recorded after five years. Interestingly, the only long-term 10-year follow-up study for posterior restorations (class I and II) in this review19, did not report failure due to secondary caries for composites and glass ionomer restorations over the 10-year observational period. Furthermore, the detection methods and criteria of evaluation might have played a role in reporting secondary caries. According to a systematic review by Brouwer et al.73, only visual assessment would mean that 40% of secondary carious lesions will be missed, while 20% of sound surfaces will be misdiagnosed as carious. Until now, there is no clear consensus on what constitutes a secondary carious lesion that requires intervention8,9.
While the findings of in vitro studies74,75 reported a reduced risk of secondary caries in ion-releasing restorations such as GICs and their derivatives, the relation between the restorative material and secondary caries development is not clear in clinical settings. It is worth mentioning that clinical reporting in the form of randomized clinical trials on the recently developed ion-releasing materials is still scarce. Developments such as RMGIC with ionic resin matrix (Activa Bioactive) which is claimed to release ions in sufficient quantities to induce remineralization and inhibit secondary caries have not been thoroughly evaluated. The short-term performance was disappointing with an unacceptable failure rate due to the absence of an adhesive41. (a protocol no longer recommended by the manufacturer). Recent in vitro data regarding the ion-releasing Cention n showed its ability to neutralize the acidic environment76. However, no clinical evidence in the literature is available to validate the laboratory data.
The quality of the interface between the tooth structure and the restoration can play a significant role in the occurrence of secondary caries. While not the only route for secondary caries, the presence of a defective restoration margin can allow acidic fluids or biofilm to enter the interface via gaps. However, there is currently no agreement on the role of microleakage in the development of caries near composites. Nonetheless, some in vivo and in vitro studies suggest that the presence of a gap next to a composite restoration can result in the formation of a "wall lesion.". The literature also suggests the presence of a correlation between the size of the gap and the size of the dentinal wall lesions59,64,77,78,79.
The results of marginal adaptation between GIC derivatives showed comparable performance with resin composite restorations with no significant difference between them. Marginal adaptation of restorations is highly dependent on the quality of the adhesive interface80,81. Traditionally, attachment of resin composite restorations was achieved through micromechanical adhesion that involved the etching of the dental substrates82. Due to their user-friendly application, simplified universal adhesives have grown in popularity. According to the literature, these adhesives are a single-bottle, no-mix adhesive system that works well with any adhesion strategy and bonds adequately to tooth structure as well as various direct and indirect restorative materials83,84. However, the simplification came at the expense of hydrophilicity which can lead to water seepage through the hybrid layer causing nano leakage 85. Therefore, different protocols have been suggested to improve the performance of simplified adhesives including increasing the application time86, the addition of a hydrophobic resin layer over the adhesive87, and application of several layers of the simplified adhesive88. There is no clear consensus in the literature on the optimal way to improve the long-term performance of simplified adhesives.
The results of this systematic review showed a wide variation in the adhesion protocol for the ion-releasing materials, ranging from no pre-treatments to polyacrylic acid conditioners, ER, and SE adhesives. Nevertheless, the overall incidence of marginal deterioration was low. It is important to highlight that the adherent substrate which is a determining factor in the quality of the adhesion, is not consistent in all studies, with margins being in enamel, dentine, or cementum. GICs were applied in the majority of studies after pre-treatment with a cavity conditioner of poly-acrylic acid. It has been proposed that a tooth-GIC interaction interphase layer is seen after GIC comes in contact with pre-treated dentin, as the pre-treatment facilitates diffusion of ions into the demineralized substrate89,90.
A recent systematic review has shown that this interphase layer is notably resistant to acidic dissolution and hence improving the quality of the adhesive interface91. It is important to note that in this review, scores 1 and 2 of the FDI criteria in the marginal adaptation outcome were considered to be a sign of no significant marginal deterioration. This was done to distinguish early stages of marginal deterioration between ion-releasing materials and resin composite restorations. Since, the presence of small marginal gaps, ditches could potentially be a culprit in secondary caries development.
The risk of bias in more than 60% of the included studies was high, with only 3 studies reporting a low risk of bias19,37,38. Performance bias was high or unclear in most studies as the nature and presentation of the used materials are different and easily identified by dentists. It should be noted that the overall risk of bias of the study was not considered as a ground for meta-analysis exclusion. Therefore, the results of this analysis should be cautiously interpreted. The GRADE assessment of the quality of evidence was low for both outcomes (secondary caries and marginal adaptation) which weakens confidence in the effect estimate. Consequently, the true effect might be substantially different from the estimate of the effect. Imprecision and risk of bias for both outcomes had to be downgraded by one level each. The risk of bias for 2 of the primary domains (performance bias and selection bias) was high for studies that contributed to the weight of the analysis. The absence of events in control and intervention arms led to a downgrading for impression by one level92.
There are some limitations to this review. Firstly, no restriction was placed on the date of publication. Studies that were published in the early 2000s presented a higher risk of bias and inadequate reporting which affected their quality assessment. Although the Consolidated Standards of Reporting Trials (CONSORT) statement was developed in 199693 and undergone a couple of revisions94,95, many clinical trial reports remained inadequate. Furthermore, short follow-up periods resulted in an overall low number of events. Also, several new ion-releasing materials have emerged in the last 5 years. The results of this analysis were based on two broad categories of materials (GICs and compomers). The findings of this review cannot be applied to all commercially available ion-releasing materials.
Conclusions
-
1.
Within the limitation of this work, this systematic review and meta-analysis revealed that secondary caries occurrence is not dependent on the ion-releasing capability of restorative material.
-
2.
Short-term follow-ups are a common denominator among the available body of evidence. Longer follow-ups are recommended to accurately detect the performance of different restorative materials after prolonged clinical service.
-
3.
Several new ion-releasing materials lack high-quality clinical reporting and need further investigations.
Data availability
The data used in this article are available upon request from the corresponding author.
References
van Dijken, J. W. & Pallesen, U. A randomized 10-year prospective follow-up of Class II nanohybrid and conventional hybrid resin composite restorations. J. Adhes. Dent. 16, 585–592. https://doi.org/10.3290/j.jad.a33202 (2014).
van Dijken, J. W. & Pallesen, U. Randomized 3-year clinical evaluation of Class I and II posterior resin restorations placed with a bulk-fill resin composite and a one-step self-etching adhesive. J. Adhes. Dent. 17, 81. https://doi.org/10.3290/j.jad.a33502 (2015).
Barata, J. S. et al. Influence of gaps in adhesive restorations in the development of secondary caries lesions: An in situ evaluation. Am. J. Dent. 25, 244–248 (2012).
Da Rosa Rodolpho, P. A. et al. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent. Mater. 27, 955–963. https://doi.org/10.1016/j.dental.2011.06.001 (2011).
Kramer, N. et al. Determination of caries risk at resin composite margins. Am. J. Dent. 20, 59–64 (2007).
Opdam, N. J. et al. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 93, 943. https://doi.org/10.1177/0022034514544217 (2014).
Mjor, I. A. & Toffenetti, F. Secondary caries: A literature review with case reports. Quintessence Int 31, 165–179 (2000).
Machiulskiene, V. et al. Terminology of dental caries and dental caries management: Consensus report of a workshop organized by ORCA and cariology research group of IADR. Caries Res. 54, 7–14. https://doi.org/10.1159/000503309 (2020).
Askar, H. et al. Secondary caries: What is it, and how it can be controlled, detected, and managed?. Clin Oral Investig 24, 1869–1876. https://doi.org/10.1007/s00784-020-03268-7 (2020).
de Fucio, S. B. et al. Analyses of biofilms accumulated on dental restorative materials. Am. J. Dent. 22, 131–136 (2009).
Hansel, C., Leyhausen, G., Mai, U. E. & Geurtsen, W. Effects of various resin composite (co)monomers and extracts on two caries-associated micro-organisms in vitro. J. Dent. Res. 77, 60–67. https://doi.org/10.1177/00220345980770010601 (1998).
Zalkind, M. M., Keisar, O., Ever-Hadani, P., Grinberg, R. & Sela, M. N. Accumulation of Streptococcus mutans on light-cured composites and amalgam: An in vitro study. J. Esthet. Dent. 10, 187–190. https://doi.org/10.1111/j.1708-8240.1998.tb00356.x (1998).
Pires, P. M. et al. Contemporary restorative ion-releasing materials: Current status, interfacial properties and operative approaches. Br Dent J 229, 450–458. https://doi.org/10.1038/s41415-020-2169-3 (2020).
Lohbauer, U. Dental glass ionomer cements as permanent filling materials? – Properties. Limit. Future Trends 3, 76–96 (2010).
Banerjee, A. The role of glass-ionomer cements in minimum intervention (MI) caries management. In Glass-Ionomers in Dentistry (ed. Sidhu, S. K.) 81–96 (Springer International Publishing, Cham, 2016).
Celik, E. U., Tunac, A. T. & Yilmaz, F. Three-year clinical evaluation of high-viscosity glass ionomer restorations in non-carious cervical lesions: A randomised controlled split-mouth clinical trial. Clin. Oral. Investig. 23, 1473–1480. https://doi.org/10.1007/s00784-018-2575-y (2019).
Diem, V. T., Tyas, M. J., Ngo, H. C., Phuong, L. H. & Khanh, N. D. The effect of a nano-filled resin coating on the 3-year clinical performance of a conventional high-viscosity glass-ionomer cement. Clin. Oral Investig. 18, 753–759. https://doi.org/10.1007/s00784-013-1026-z (2014).
Friedl, K., Hiller, K. A. & Friedl, K. H. Clinical performance of a new glass ionomer based restoration system: A retrospective cohort study. Dent. Mater. 27, 1031–1037. https://doi.org/10.1016/j.dental.2011.07.004 (2011).
Gurgan, S., Kutuk, Z. B., Yalcin Cakir, F. & Ergin, E. A randomized controlled 10 years follow up of a glass ionomer restorative material in class I and class II cavities. J Dent 94, 103175. https://doi.org/10.1016/j.jdent.2019.07.013 (2020).
Najeeb, S. et al. Modifications in glass ionomer cements: Nano-sized fillers and bioactive nanoceramics. Int. J. Mol. Sci. https://doi.org/10.3390/ijms17071134 (2016).
Salinovic, I. et al. Mechanical properties of high viscosity glass ionomer and glass hybrid restorative materials. Acta Stomatol. Croat. 53, 125–131. https://doi.org/10.15644/asc53/2/4 (2019).
Ruengrungsom, C., Palamara, J. E. A. & Burrow, M. F. Comparison of ART and conventional techniques on clinical performance of glass-ionomer cement restorations in load bearing areas of permanent and primary dentitions: A systematic review. J. Dent. 78, 1–21. https://doi.org/10.1016/j.jdent.2018.07.008 (2018).
Vallittu, P. K., Boccaccini, A. R., Hupa, L. & Watts, D. C. Bioactive dental materials-Do they exist and what does bioactivity mean?. Dent. Mater. 34, 693–694. https://doi.org/10.1016/j.dental.2018.03.001 (2018).
Garoushi, S., Vallittu, P. K. & Lassila, L. Characterization of fluoride releasing restorative dental materials. Dent. Mater. J. 37, 293–300. https://doi.org/10.4012/dmj.2017-161 (2018).
Todd, J. C. Scientific Documentation: Cention N. Ivoclar Vivadent AG, research and development. Sci. Doc. 1–58. (2016).
Francois, P., Fouquet, V., Attal, J. P. & Dursun, E. Commercially available fluoride-releasing restorative materials: A review and a proposal for classification. Materials (Basel) https://doi.org/10.3390/ma13102313 (2020).
Tiskaya, M., Al-eesa, N. A., Wong, F. S. L. & Hill, R. G. Characterization of the bioactivity of two commercial composites. Dent. Mater. 35, 1757–1768. https://doi.org/10.1016/j.dental.2019.10.004 (2019).
Glasspoole, E. A., Erickson, R. L. & Davidson, C. L. Demineralization of enamel in relation to the fluoride release of materials. Am. J. Dent. 14, 8–12 (2001).
Yaman, S. D., Er, O., Yetmez, M. & Karabay, G. A. In vitro inhibition of caries-like lesions with fluoride-releasing materials. J. Oral Sci. 46, 45–50. https://doi.org/10.2334/josnusd.46.45 (2004).
Okida, R. C., Mandarino, F., Sundfeld, R. H., de Alexandre, R. S. & Sundefeld, M. L. In vitro-evaluation of secondary caries formation around restoration. Bull. Tokyo Dent. Coll. 49, 121–128 (2008).
Hutton, B. et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784. https://doi.org/10.7326/M14-2385 (2015).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G. & Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6, e1000097. https://doi.org/10.1371/journal.pmed.1000097 (2009).
Higgins, J. P. T. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. J. BMJ 343, d5928. https://doi.org/10.1136/bmj.d5928 (2011).
Alonso-Coello, P. et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ 353, i2016. https://doi.org/10.1136/bmj.i2016 (2016).
Guyatt, G. H. et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336, 924–926. https://doi.org/10.1136/bmj.39489.470347.AD (2008).
Balshem, H. et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 64, 401–406. https://doi.org/10.1016/j.jclinepi.2010.07.015 (2011).
Koc Vural, U., Kerimova, L. & Kiremitci, A. Clinical comparison of a micro-hybride resin-based composite and resin modified glass ionomer in the treatment of cervical caries lesions: 36-month, split-mouth, randomized clinical trial. Odontology https://doi.org/10.1007/s10266-020-00550-8 (2020).
Koc Vural, U., Meral, E., Ergin, E. & Gürgan, S. Twenty-four-month clinical performance of a glass hybrid restorative in non-carious cervical lesions of patients with bruxism: A split-mouth, randomized clinical trial. Clin. Oral Investig. 24, 1229–1238. https://doi.org/10.1007/s00784-019-02986-x (2020).
Balkaya, H. & Arslan, S. A two-year clinical comparison of three different restorative materials in class II cavities. Oper Dent. 45, E32-e42. https://doi.org/10.2341/19-078-c (2020).
van Dijken, J. W. & Pallesen, U. A 7-year randomized prospective study of a one-step self-etching adhesive in non-carious cervical lesions. The effect of curing modes and restorative material. J. Dent. 40, 1060–1067. https://doi.org/10.1016/j.jdent.2012.08.017 (2012).
van Dijken, J. W. V., Pallesen, U. & Benetti, A. A randomized controlled evaluation of posterior resin restorations of an altered resin modified glass-ionomer cement with claimed bioactivity. Dent. Mater. 35, 335–343. https://doi.org/10.1016/j.dental.2018.11.027 (2019).
Brackett, W. W., Dib, A., Brackett, M. G., Reyes, A. A. & Estrada, B. E. Two-year clinical performance of Class V resin-modified glass-lonomer and resin composite restorations. Oper. Dent. 28, 477–481 (2003).
De Moor, R. J., Stassen, I. G., van’t Veldt, Y., Torbeyns, D. & Hommez, G. M. Two-year clinical performance of glass ionomer and resin composite restorations in xerostomic head- and neck-irradiated cancer patients. Clin. Oral Investig. 15, 31–38. https://doi.org/10.1007/s00784-009-0355-4 (2011).
Gallo, J. R. et al. Three-year clinical evaluation of a compomer and a resin composite as Class V filling materials. Oper. Dent. 30, 275–281 (2005).
Onal, B. & Pamir, T. The two-year clinical performance of esthetic restorative materials in noncarious cervical lesions. J. Am. Dent. Assoc. 136, 1547–1555. https://doi.org/10.14219/jada.archive.2005.0085 (2005).
Türkün, L. S. & Celik, E. U. Noncarious class V lesions restored with a polyacid modified resin composite and a nanocomposite: A two-year clinical trial. J. Adhes. Dent. 10, 399–405 (2008).
Wucher, M., Grobler, S. R. & Senekal, P. J. A 3-year clinical evaluation of a compomer, a composite and a compomer/composite (sandwich) in class II restorations. Am. J. Dent. 15, 274–278 (2002).
Pollington, S. & van Noort, R. A clinical evaluation of a resin composite and a compomer in non-carious Class V lesions. A 3-year follow-up. Am. J. Dent. 21, 49–52 (2008).
Menezes-Silva, R. et al. Randomized clinical trial of class II restoration in permanent teeth comparing ART with composite resin after 12 months. Clin. Oral Investig. 23, 3623–3635. https://doi.org/10.1007/s00784-018-2787-1 (2019).
Jassal, M., Mittal, S. & Tewari, S. Clinical effectiveness of a resin-modified glass ionomer cement and a mild one-step self-etch adhesive applied actively and passively in noncarious cervical lesions: An 18-month clinical trial. Oper. Dent. 43, 581–592. https://doi.org/10.2341/17-147-c (2018).
Miletić, I. et al. Clinical performance of a glass-hybrid system compared with a resin composite in the posterior region: Results of a 2-year multicenter study. J. Adhes. Dent. 22, 235–247. https://doi.org/10.3290/j.jad.a44547 (2020).
Santiago, S. L. et al. Two-year clinical evaluation of resinous restorative systems in non-carious cervical lesions. Braz. Dent. J. 21, 229–234. https://doi.org/10.1590/s0103-64402010000300010 (2010).
Oz, F. D., Meral, E., Ergİn, E. & Gurgan, S. One-year evaluation of a new restorative glass ionomer cement for the restoration of non-carious cervical lesions in patients with systemic diseases: A randomized, clinical trial. J. Appl. Oral Sci. 28, e20200311. https://doi.org/10.1590/1678-7757-2020-0311 (2020).
Folwaczny, M., Loher, C., Mehl, A., Kunzelmann, K. H. & Hinkel, R. Tooth-colored filling materials for the restoration of cervical lesions: A 24-month follow-up study. Oper. Dent. 25, 251–258 (2000).
Perdigão, J. et al. Randomized clinical trial of four adhesion strategies: 18-month results. Oper. Dent. 37, 3–11. https://doi.org/10.2341/11-222-c (2012).
McComb, D., Erickson, R. L., Maxymiw, W. G. & Wood, R. E. A clinical comparison of glass ionomer, resin-modified glass ionomer and resin composite restorations in the treatment of cervical caries in xerostomic head and neck radiation patients. Oper. Dent. 27, 430–437 (2002).
Perdigão, J., Dutra-Corrêa, M., Saraceni, S. H., Ciaramicoli, M. T. & Kiyan, V. H. Randomized clinical trial of two resin-modified glass ionomer materials: 1-year results. Oper. Dent. 37, 591–601. https://doi.org/10.2341/11-415-c (2012).
Demarco, F. F. et al. Should my composite restorations last forever? Why are they failing?. Braz. Oral Res. 31, e56. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0056 (2017).
Nedeljkovic, I., Teughels, W., De Munck, J., Van Meerbeek, B. & Van Landuyt, K. L. Is secondary caries with composites a material-based problem?. Dent. Mater. 31, e247–e277. https://doi.org/10.1016/j.dental.2015.09.001 (2015).
Raskin, A., Setcos, J. C., Vreven, J. & Wilson, N. H. Influence of the isolation method on the 10-year clinical behaviour of posterior resin composite restorations. Clin. Oral Investig. 4, 148–152. https://doi.org/10.1007/s007840000069 (2000).
Mjor, I. A. Clinical diagnosis of recurrent caries. J. Am. Dent. Assoc. 136, 1426–1433 (2005).
Kuper, N. K. et al. Gap size and wall lesion development next to composite. J. Dent. Res. 93, 108S-S113. https://doi.org/10.1177/0022034514534262 (2014).
Nedeljkovic, I. et al. Secondary caries: Prevalence, characteristics, and approach. Clin. Oral Investig. 24, 683–691. https://doi.org/10.1007/s00784-019-02894-0 (2020).
Cenci, M. S., Pereira-Cenci, T., Cury, J. A. & Ten Cate, J. M. Relationship between gap size and dentine secondary caries formation assessed in a microcosm biofilm model. Caries Res. 43, 97–102. https://doi.org/10.1159/000209341 (2009).
Kidd, E. A. & Fejerskov, O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J. Dent. Res. https://doi.org/10.1177/154405910408301s07 (2004).
Tjaderhane, L. et al. Strategies to prevent hydrolytic degradation of the hybrid layer-A review. Dent. Mater. 29, 999–1011. https://doi.org/10.1016/j.dental.2013.07.016 (2013).
Toledano, M., Yamauti, M., Osorio, E. & Osorio, R. Zinc-inhibited MMP-mediated collagen degradation after different dentine demineralization procedures. Caries Res. 46, 201–207. https://doi.org/10.1159/000337315 (2012).
Tezvergil-Mutluay, A. et al. The requirement of zinc and calcium ions for functional MMP activity in demineralized dentin matrices. Dent. Mater. 26, 1059–1067. https://doi.org/10.1016/j.dental.2010.07.006 (2010).
Kuper, N. K. et al. Restoration materials and secondary caries using an in vitro biofilm model. J. Dent. Res. 94, 62–68. https://doi.org/10.1177/0022034514553245 (2015).
Askar, H., Krois, J., Gostemeyer, G. & Schwendicke, F. Secondary caries risk of different adhesive strategies and restorative materials in permanent teeth: Systematic review and network meta-analysis. J. Dent. 104, 103541. https://doi.org/10.1016/j.jdent.2020.103541 (2021).
Laske, M., Opdam, N. J. M., Bronkhorst, E. M., Braspenning, J. C. C. & Huysmans, M. Ten-year survival of class II restorations placed by general practitioners. JDR Clin. Trans. Res. 1, 292–299. https://doi.org/10.1177/2380084416663192 (2016).
Opdam, N. J., Bronkhorst, E. M., Loomans, B. A. & Huysmans, M. C. 12-year survival of composite vs. amalgam restorations. J. Dent. Res. 89, 1063–1067. https://doi.org/10.1177/0022034510376071 (2010).
Brouwer, F., Askar, H., Paris, S. & Schwendicke, F. Detecting secondary caries lesions: A systematic review and meta-analysis. J. Dent. Res. 95, 143–151. https://doi.org/10.1177/0022034515611041 (2016).
Askar, H., Brouwer, F., Lehmensiek, M., Paris, S. & Schwendicke, F. The association between loading of restorations and secondary caries lesions is moderated by the restoration material elasticity. J. Dent. 58, 74–79. https://doi.org/10.1016/j.jdent.2017.01.002 (2017).
Hetrodt, F., Lausch, J., Meyer-Lueckel, H., Conrads, G. & Apel, C. Evaluation of restorative materials containing preventive additives in a secondary caries model in vitro. Caries Res. 53, 447–456. https://doi.org/10.1159/000496401 (2019).
Gupta, N. et al. Comparison of fluoride ion release and alkalizing potential of a new bulk-fill alkasite. J. Conserv. Dent. 22, 296–299. https://doi.org/10.4103/JCD.JCD_74_19 (2019).
Nassar, H. M. & Gonzalez-Cabezas, C. Effect of gap geometry on secondary caries wall lesion development. Caries Res. 45, 346–352. https://doi.org/10.1159/000329384 (2011).
Thomas, R. Z., Ruben, J. L., ten Bosch, J. J., Fidler, V. & Huysmans, M. C. Approximal secondary caries lesion progression, a 20-week in situ study. Caries Res. 41, 399–405. https://doi.org/10.1159/000104799 (2007).
Espejo, L. C., Simionato, M. R., Barroso, L. P., Netto, N. G. & Luz, M. A. Evaluation of three different adhesive systems using a bacterial method to develop secondary caries in vitro. Am. J. Dent. 23, 93–97 (2010).
Kakaboura, A., Rahiotis, C., Watts, D., Silikas, N. & Eliades, G. 3D-marginal adaptation versus setting shrinkage in light-cured microhybrid resin composites. Dent. Mater. 23, 272–278. https://doi.org/10.1016/j.dental.2006.01.020 (2007).
He, Z., Shimada, Y., Sadr, A., Ikeda, M. & Tagami, J. The effects of cavity size and filling method on the bonding to Class I cavities. J. Adhes. Dent. 10, 447–453 (2008).
Foxton, R. M. Current perspectives on dental adhesion: (2) Concepts for operatively managing carious lesions extending into dentine using bioactive and adhesive direct restorative materials. Jpn. Dent. Sci. Rev. 56, 208–215. https://doi.org/10.1016/j.jdsr.2020.08.003 (2020).
Matos, A. B. et al. Bonding efficiency and durability: current possibilities. Braz. Oral Res. 31, e57. https://doi.org/10.1590/1807-3107BOR-2017.vol31.0057 (2017).
Alex, G. Universal adhesives: the next evolution in adhesive dentistry?. Compend. Contin. Educ. Dent. 36, 15–26 (2015).
Van Landuyt, K. L. et al. The role of HEMA in one-step self-etch adhesives. Dent. Mater. 24, 1412–1419. https://doi.org/10.1016/j.dental.2008.02.018 (2008).
Toledano, M. et al. Increases in dentin-bond strength if doubling application time of an acetone-containing one-step adhesive. Oper. Dent. 32, 133–137. https://doi.org/10.2341/06-32 (2007).
Sezinando, A. et al. Influence of a hydrophobic resin coating on the immediate and 6-month dentin bonding of three universal adhesives. Dent. Mater. 31, e236–e246. https://doi.org/10.1016/j.dental.2015.07.002 (2015).
Chasqueira, A. F., Arantes-Oliveira, S. & Portugal, J. Effect of changes to the manufacturer application techniques on the shear bond strength of simplified dental adhesives. J. Appl. Biomater. Funct. Mater. 11, e117–e121. https://doi.org/10.5301/jabfm.5000156 (2013).
Toledano, M. et al. In vitro mechanical stimulation facilitates stress dissipation and sealing ability at the conventional glass ionomer cement-dentin interface. J. Dent. 73, 61–69. https://doi.org/10.1016/j.jdent.2018.04.006 (2018).
Yilmaz, Y., Gurbuz, T. & Kocogullari, M. E. The influence of various conditioner agents on the interdiffusion zone and microleakage of a glass lonomer cement with a high viscosity in primary teeth. Oper. Dent. 30, 105–112 (2005).
Mustafa, H. A., Soares, A. P., Paris, S., Elhennawy, K. & Zaslansky, P. The forgotten merits of GIC restorations: A systematic review. Clin. Oral Investig. 24, 2189–2201. https://doi.org/10.1007/s00784-020-03334-0 (2020).
Castellini, G., Bruschettini, M., Gianola, S., Gluud, C. & Moja, L. Assessing imprecision in Cochrane systematic reviews: A comparison of GRADE and Trial Sequential Analysis. Syst. Rev. 7, 110. https://doi.org/10.1186/s13643-018-0770-1 (2018).
Begg, C. et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 276, 637–639. https://doi.org/10.1001/jama.276.8.637 (1996).
Moher, D., Schulz, K. F. & Altman, D. G. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet 357, 1191–1194 (2001).
Schulz, K. F., Altman, D. G., Moher, D. & Grop, C. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Trials 11, 32. https://doi.org/10.1186/1745-6215-11-32 (2010).
Funding
This study was funded by 3 M/Key Opinion Leader Scholarship.
Author information
Authors and Affiliations
Contributions
Conception and design of study: H.H. H.A.M.A.M.A., S.H.M., E.A.; Acquisition of data: E.A., H.H. H.A.M.A.M.A., H.C., M.M., S.H.M.; Analysis and/or interpretation of data: E.A., H.H. H.A.M.A.M.A.; Drafting the manuscript: E.A., H.C., H.H. H.A.M.A.M.A., S.H.M.; Revising the manuscript critically for important intellectual content: H.C., H.H. H.A.M.A.M.A., S.H.M.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Albelasy, E.H., Hamama, H.H., Chew, H.P. et al. Secondary caries and marginal adaptation of ion-releasing versus resin composite restorations: a systematic review and meta-analysis of randomized clinical trials. Sci Rep 12, 19244 (2022). https://doi.org/10.1038/s41598-022-19622-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19622-6
This article is cited by
-
Clinical effectiveness of pit and fissure sealants in primary and permanent teeth of children and adolescents: an umbrella review
European Archives of Paediatric Dentistry (2024)
-
Intramedullary bone tissue reaction of ion-releasing resin-modified glass-ionomer restoration versus two calcium silicate-based cements: an animal study
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
