
Abstract
In pancreatic cancer, postoperative complications (POCs) are associated with disease outcomes. The geriatric nutritional risk index (GNRI) is known to predict POCs after pancreatoduodenectomy (PD) or distal pancreatectomy (DP) in patients with hepatobiliary pancreatic tumors, including pancreatic cancer. Through POC occurrence risk, we aimed to determine whether GNRI could predict prognosis in patients who underwent PD or DP for resectable pancreatic cancer. This retrospective study examined 139 patients who underwent radical pancreatectomy for resectable pancreatic cancer at Ehime University. All patients were subjected to nutritional screening using GNRI and were followed up for POC diagnosis and patient outcomes such as overall survival (OS). Patients were divided based on the GNRI value of 99 (Low group: N = 74, GNRI < 99; High group: N = 65, GNRI ≥ 99), which was determined by receiver operating characteristic curve analysis. Multivariate analysis showed that GNRI < 99 was statistically correlated with POCs after curative pancreatic resection (p = 0.02). Univariate and multivariate analyses confirmed that GNRI < 99 was significantly associated with long OS (p = 0.04). GNRI could be a potential prognostic marker for resectable pancreatic cancer after curative pancreatic resection despite being a simple and noninvasive approach.
Similar content being viewed by others

Introduction
Pancreatic resection, such as pancreatoduodenectomy (PD) and distal pancreatectomy (DP), has been the gold standard surgical method for malignant pancreatic tumors. Despite the progress in surgical skills, energy devices, and perioperative management, surgery-related mortality rates following PD and DP can be up to 5%1,2,3. Among the potential postoperative complications (POCs), the most common are surgical site infections (SSIs), delayed gastric emptying (DGE), and postoperative pancreatic fistula (POPF). Particularly, SSIs—including intra-abdominal surgery-related and wound infections—and post-pancreatectomy hemorrhage (PPH) are occasionally caused by POPF4. Recent evidence revealed that POPF was associated with a poor prognosis in patients with pancreatic cancer5. The reported POCs, including the POPF rate, were 30–50%6,7 in patients with DP and 40% in those with PD1. Previously, we showed that a low geriatric nutritional risk index (GNRI) could predict SSI, POPF, and PPH in patients who underwent PD or DP for hepatobiliary diseases8,9,10,11. GNRI has favored assessing elderly patients’ nutritional status and predicting clinical outcomes12.
More importantly, GNRI is easily accessible and inexpensive, requiring only data on body weight, height, and serum albumin levels. Thus, this study evaluated the association between GNRI and outcomes such as overall survival (OS) in patients who underwent PD or DP for resectable pancreatic cancer. Identifying prognostic markers for resectable pancreatic cancer may help identify patients with a high risk of a poor prognosis.
Materials and methods
Patients
Between August 2013 and December 2020, 169 patients who underwent surgery for pancreatic cancer were enrolled in this study at the Department of Hepatobiliary and Transplantation Surgery, Ehime University Graduate School of Medicine, Japan. Exclusion criteria were as follows: cases of (1) exploratory laparotomy due to peritoneal dissemination, (2) choledochojejunostomy, and (3) total pancreatectomy. Moreover, (4) patients at Stage 0 and/or lacking information about the outcomes were excluded. All surgical procedures were performed by surgeons with substantial experience in pancreatic surgery. The definition of POC was defined and clarified according to the Clavien–Dindo (CD) classification13 and the International Study Group for Pancreatic Surgery in 201614. In this study, CD grade ≥ IIIa was defined as a POC. Clinical data were collected from both inpatient and outpatient medical records. This study was approved by the ethical committee of the Ehime University in 2021 (Approval number: 2101214) and followed the Declaration of Helsinki as revised in 2013. All patients provided informed consent prior to enrollment in this study. In addition, retrospectively registered patients or their guardians, provided verbal consent to use their medical information for scientific research.
Collection of clinical and laboratory data
As preoperative parameters, clinical data were obtained and analyzed, which included demographic variables (e.g., sex and age), anthropometric parameters (e.g., height, weight, and body mass index [BMI]), American Society of Anesthesiologist (ASA)’s physical status classification, comorbidities including diabetes mellitus, location of the tumors, neoadjuvant chemotherapy, preoperative albumin value, and GNRI. Moreover, data on intraoperative or postoperative parameters, surgery duration, estimated blood loss, blood transfusion, POC, POPF, SSI, DGE, and PPH were collected from individual medical records. The pathological stage was assigned following the TNM classification (8th edition)15.
Definition of GNRI
GNRI was measured by body weight, height, and serum albumin. Data obtained before surgical procedure were as follows: GNRI = [14.89 × serum albumin (g/L)] + [41.7 × present/ideal body weight (kg)]. The ideal body weight was defined as 22 × patient height (m)2. If the current body weight was higher than the ideal body weight, the present/ideal body weight was 112.
Perioperative management and follow-up study
All patients preoperatively underwent routine blood tests—including serum albumin and tumor marker assessment—and a physical examination that included the measurement of body weight and height. Prophylactic antibiotics were administered through a peripheral vein before anesthetic induction. All patients who underwent DP or PD under general anesthesia received proton pump inhibitors. Amylase values from ascitic fluid obtained from the drainage tube were measured on postoperative days 1, 2, 3, 5, and 7 until removing the drains. Furthermore, dynamic computed tomography was performed to evaluate fluid collections before decannulation of the drainage tubes. Almost all patients were followed up every three months in the first two years and every six months in the following 3–5 years.
In addition, most patients undertook adjuvant chemotherapy due to S-1 for 6 months. The follow-up period started on the date of surgical procedure and ended on the date of death, at the last follow-up, or after a maximum of 60 months. OS was evaluated based on the cause of death as determined from medical records or letters and calculated using the period from the date of surgery to the date of death from any cause or last follow-up.
Statistical analysis
All statistical significances were calculated using GraphPad Prism v5.0 (GraphPad Software Inc., La Jolla, CA, USA) and SPSS (SPSS Inc., Chicago, IL, USA). Patient backgrounds were expressed as median and interquartile ranges for nonparametric distribution. Categorical data were expressed as numbers and percentages. On the other hand, statistical significance was determined using Mann–Whitney's U test, χ2 test, or Fisher’s exact test for patient backgrounds and outcomes. A receiver operating characteristic (ROC) curve was analyzed to identify the optimal cutoff value of GNRI for evaluating the risk of POCs. In addition, cutoff value was determined using Youden-Index. OS following pancreatic resection was analyzed by the Kaplan–Meier method, and survival curves were compared using the log-rank test with p-values and 95% confidence intervals (CIs) of hazard ratios (HRs). Univariate and multivariate Cox proportional hazard regression models were used to identify independent prognostic factors affecting OS. A cutoff value for continuous variables was calculated by the respective median. The probability of p < 0.05 was considered statistically significant.
Results
GNRI and clinicopathological features
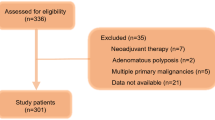
In this study, 169 patients underwent surgical procedure for pancreatic cancer in the same term. Except for 30 cases of exclusion criteria (total pancreatectomy: 3 patients, Stage 0: 3, Not pancreatic cancer: 8, No information of the prognosis: 16), 139 patients were enrolled. Patients were divided into two groups according to the presence or absence of POCs, which were CD classification13 ≥ grade IIIa. Table 1 summarizes clinical and demographic data from each group. No statistically significant differences in sex, age, BMI, ASA classification, presence of diabetes mellitus, neoadjuvant chemotherapy, surgical procedures, surgery duration, estimated blood loss, presence of blood transfusions, adjuvant chemotherapy (gemcitabine or S-1 for 6 months), and the completion rate, and time to adjuvant chemotherapy after surgery were observed between patients with (N = 33) and without (N = 106) POC. However, statistically significant differences were observed for preoperative albumin (p < 0.001), surgical procedure (DP or PD; p = 0.04), GNRI values (p < 0.001), and postoperative hospital stays (p < 0.001).
Optimal GNRI cutoff value calculation by ROC curve
The optimal cutoff value for evaluating the risk of POCs was determined using ROC curve analysis (Fig. 1). With an area under the curve of 0.71 (95% CI: 0.62–0.80), the most appropriate cutoff value was determined to be 99. This value had a sensitivity of 56.6% and a specificity of 78.8%. Patients were then divided into two groups according to the established cutoff value: Low (GNRI < 99, N = 72) and High (GNRI ≥ 99, N = 67) groups. The background profiles were compared between these two groups (Table 2). BMI, preoperative albumin, surgical procedure, and POC rate varied significantly between the two groups. The observed POC rates and the detail in the Low and High groups were 34.7% (N = 25) and 10.4% (N = 7), respectively (Table 3). Univariate analysis revealed that the Low group had a significantly higher rate of POC incidence than the High group (Table 3; p = 0.001).

Selection of GNRI cutoff value using receiver operating characteristic (ROC) curve analysis.
OS due to the cutoff value of GNRI
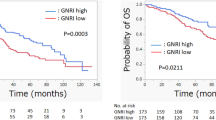
Kaplan–Meier analysis and the log-rank test demonstrated that patients in the Low group had a significantly worse prognosis in terms of OS than those in the High group (p = 0.002; Fig. 2). GNRI value was significantly associated with OS as a prognostic marker. Moreover, Stage II patients were compared according to GNRI cutoff value because they accounted for 77.8% and 70.1% of the Low and High groups, respectively (Fig. 3).

Overall survival curves between the Low and High GNRI groups. The High group shows a better prognosis than the Low group.

Overall survival curves between the Low and High GNRI groups in Stage II patients. OS is associated with a low GNRI level in Stage II patients.
Cox regression analysis for OS
Univariate analysis showed that OS was significantly associated with GNRI cutoff value (p = 0.003). Multivariate analysis revealed that GNRI < 99 (HR: 2.45; 95% CI: 1.02–5.86; p = 0.04), sex (HR: 3.01; 95% CI: 1.57–5.77; p = 0.001), and surgical procedure (HR: 2.30; 95% CI: 1.16–4.55; p = 0.02) were significant independent prognostic potential markers for OS (Table 4).
Discussion
Despite the advanced surgical procedure and perioperative management, POCs after PD or DP (rate: 40–60%) remain a cause of high morbidity in patients with pancreatic cancer16,17. The most common major POCs are the development of POPF, DGE, intra-abdominal infection, and PPH. POPF is particularly known as major POC, which is a potentially fatal complication after PD or DP16,17. Several studies have reported that POPF was associated with sex, BMI, blood transfusion, pancreatic texture, preoperative biliary drainage, lower serum albumin level, CRP level, and nutritional status3,18. However, a definitive risk factor for POPF remains incompletely understood19. Generally, POCs have been associated with poor OS, likely due to chemotherapy delay and cancer progression caused by chemokines/cytokines induced POC-associated inflammation in several type of cancers including pancreatic cancer5,20,21.
Therefore, the primary goal of the surgeons is to prevent these POCs, especially POPF, to reduce poor survival. Previous studies have also reported pancreatic volume, completion of adjuvant chemotherapy, cancer antigen 19-9, carcinoembryonic antigen level, and prognostic index as prognostic factors in patients with pancreatic cancer22,23,24.
Recent evidences revealed that nutritional status such as prgnostic nutritional index (PNI) and GNRI are strongly associated with POCs or patients outcomes25,26. The PNI is defined using serum albumin and lymphocyte count. Luan et al.25 showed that levated PNI is correlated with a better prognosis in head and neck patients. However, AUC was compared with PNI and GNRI using ROC curve analysis. As the result, AUC showed that GNRI was higher than PNI (GNRI: 0.71 vs PNI: 0.60) in this study. On thie other hand, Hayama, et al.26 reported that lower GNRI was significantly associated with a poor prognosis compared to PNI in elderly patients with colorectal cancer. Thus, we believe GNRI will be better prpgnostic marker than PNI.
Using the nutritional status as an objective nutritional screening tool, Bouillanne et al.12 first reported that GNRI, which includes albumin and BMI, is a prognostic factor of morbidity and mortality in hospitalized elderly patients. Subsequently, several studies have consistently shown that a relationship exists among GNRI, POCs, and cancer prognosis as well since nutritional status was strongly associated with cancer prognosis25,27,28,29. For example, Kushiyama et al.30 reported that GNRI is associated with POCs after gastrectomy. Furthermore, recent reports revealed that GNRI is an important predictor of POCs and OS in patients with gastric cancer31,32. Recent evidence revealed that GNRI is a significant prognostic factor in advanced lung33 and colorectal34 cancers. Hu et al., showed that GNRI could be a useful prognostic indicator in patients who underwent surgery35,36, notably, in pancreatic cancer.
Previous studies have shown that GNRI is associated with a high risk of POCs, including SSIs, POPF, and PPH after PD or DP8,9,10,11. Briefly, a lower GNRI value was related to a higher risk of SSI and reported to be a potential marker for developing POPF and PPH after pancreatic surgery. We have recently reported the role of GNRI as a risk factor for POPFs after DP in 37 patients with pancreatic tumor or invasive gastric cancer8 and for SSIs after PD in 93 patients with hepatobiliary pancreatic or duodenal cancer11. In the present study, we further investigated the predictive value of GNRI for not only the POCs but also long-term postoperative survival after PD or DP in 139 patients with pancreatic cancer treated in a different institution.
In this study, there were 32 patients (23.0%) who developed POCs, including POPF (10.8%), bile leakage (2.9%), PPH (3.6%), and SSIs (7.9%), after PD or DP, which corresponded to CD classification ≥ IIIa and sometimes overlapped. The GNRI value of < 99 was strongly associated with a high risk of POCs, supporting the use of nutritional assessment before an elective procedure. Furthermore, a low GNRI value was significantly associated with poor long-term prognosis. The occurrence of POCs also showed a tendency to deteriorate the OS, although not statistically significant. The development of POCs is considered a potential predictor of worse outcomes because POCs are intimately associated with the delayed induction of adjuvant chemotherapy. In addition, a preoperative poor nutritional condition reflected by a lower GNRI value can affect the postoperative recovery, tolerance for adjuvant chemotherapy, and antitumor immune defense. The exact mechanisms underlying the association between lower GNRI and poorer survival outcome should be determined in further studies. However, some reports showed that body weight or nutritional status were associated with worse prognosis in pancreatic cancer patients, which evidence strongly supported our result34,35. At present, our results are consistent with those of a previous study on several cancer36,37,38. Moreover, their cutoff values were close to present study, although one of them was age restricted study39. Thus, present study strengthened that GNRI might be useful predictor for prognosis in patients with pancreatic cancer who underwent radical surgery.
Our study has several limitations in terms of the interpretation of the study results. First, there was a lack of statistical power caused by the relatively small sample size. Second, our data were collected at a single center. The third limitation lies in the retrospective nature of the study. Finally, present study cannot break the racial line, because only asian data have been reprted. Therefore, a more comprehensive large-scale prospective study should be conducted in the future to validate our study findings.
Finally, we believe that although GNRI can be easily acquired from preoperative routine work without an invasive procedure, it can predict OS in patients with pancreatic cancer after pancreatic resection. Therefore, future prospective randomized studies are warranted to investigate the significance of GNRI for improving outcomes in patients with pancreatic cancer after curative surgery.
Data availability
The data is available from the corresponding author on reasonable request.
References
Aoki, S. et al. Risk factors of serious postoperative complications after pancreaticoduodenectomy and risk calculators for predicting postoperative complications: A nationwide study of 17,564 patients in Japan. J. Hepatobil. Pancreat. Sci. 24, 243–251 (2017).
Sahora, K. et al. Preoperative biliary drainage does not increase major complications in pancreaticoduodenectomy: A large single center experience from the Massachusetts General Hospital. J. Hepatobil. Pancreat. Sci. 23, 181–187 (2016).
Hirono, S. et al. Risk factors for pancreatic fistula grade C after pancreatoduodenectomy: A large prospective, multicenter Japan-Taiwan collaboration study. J. Hepatobil. Pancreat. Sci. 27, 622–631 (2020).
Ryu, Y. et al. Validation of original and alternative fistula risk scores in postoperative pancreatic fistula. J. Hepatobil. Pancreat. Sci. 26, 354–359 (2019).
Uchida, Y. et al. Postoperative pancreatic fistulas decrease the survival of pancreatic cancer patients treated with surgery after neoadjuvant chemoradiotherapy: A retrospective analysis. Surg. Oncol. 35, 527–532 (2020).
Peng, Y. P. et al. Risk factors of postoperative pancreatic fistula in patients after distal pancreatectomy: A systematic review and meta-analysis. Sci. Rep. 7, 185 (2017).
Sugimoto, M. et al. Risk factor analysis and prevention of postoperative pancreatic fistula after distal pancreatectomy with stapler use. J. Hepatobil. Pancreat. Sci. 20, 538–544 (2013).
Funamizu, N. et al. Lower geriatric nutritional risk index predicts postoperative pancreatic fistula in patients with distal pancreatectomy. Mol. Clin. Oncol. 12, 134–137 (2020).
Funamizu, N. et al. Geriatric nutritional risk index predicts surgical site infection after pancreatoduodenectomy. Mol. Clin. Oncol. 9, 274–278 (2018).
Funamizu, N. et al. Geriatric nutritional risk index less than 92 is a predictor for late postpancreatectomy hemorrhage following pancreatoduodenectomy: A retrospective cohort study. Cancers (Basel) 12, E2779 (2020).
Funamizu, N. et al. Geriatric nutritional risk index serves as risk factor of surgical site infection after pancreatoduodenectomy: A validation cohort Ageo study. Gland. Surg. 9, 1982–1988 (2020).
Bouillanne, O. et al. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 82, 777–783 (2005).
Clavien, P. A. et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 250, 187–196 (2009).
Bassi, C. et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 161, 584–591 (2017).
Brierley, J. D. et al. UICC TNM Classification of Malignant Tumours 8th edn. (Wiley Blackwell, New York, 2017).
Hackert, T. et al. Treatment of pancreatic cancer What can we really predict today?. Cancers (Basal). 3, 675–699 (2001).
Li, Z. et al. Blumgart anastomosis reduces the incidence of pancreatic fistula after pancreaticoduodenectomy: A systematic review and meta-analysis. Sci. Rep. 21(10), 17896 (2020).
Kolbinger, F. R. et al. The image-based preoperative fistula risk score (preFRS) predicts postoperative pancreatic fistula in patients undergoing pancreatic head resection. Sci. Rep. 12, 4064 (2022).
Suzuki, S. et al. Pancreaticoduodenectomies with a duct-to-mucosa pancreaticojejunostomy anastomosis with and without a stenting tube showed no differences in long-term follow-up. J. Hepatobil. Pancreat. Sci. 18, 258–262 (2011).
DeOliveira, M. L. et al. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann. Surg. 244, 931–937 (2006).
Smyth, M. J. et al. Cytokines in cancer immunity and immunotherapy. Immunol. Rev. 202, 275–293 (2004).
Fukumoto, T. et al. Pancreatic volume is one of the independent prognostic factors for resectable pancreatic ductal adenocarcinomas. J. Hepatobil. Pancreat. Sci. 23, 472–479 (2016).
van Manen, L. et al. Stage-specific value of carbohydrate antigen 19–9 and carcinoembryonic antigen serum levels on survival and recurrence in pancreatic cancer: A single center study and meta-analysis. Cancers (Basel) 12, 2970 (2020).
Sawaki, A. et al. Practical prognostic index for patients with metastatic pancreatic cancer treated with gemcitabine. J. Gastroenterol. Hepatol. 8, 1292–1297 (2008).
Luan, C. W. et al. Pretreatment prognostic nutritional index as a prognostic marker in head and neck cancer: A systematic review and meta-analysis. Sci. Rep. 11, 17117 (2021).
Hayama, T. et al. The preoperative geriatric nutritional risk index (GNRI) is an independent prognostic factor in elderly patients underwent curative resection for colorectal cancer. Sci. Rep. 12, 3682 (2022).
Hiraoka, A. et al. Impact of muscle volume and muscle function decline in patients undergoing surgical resection for hepatocellular carcinoma. J. Gastroenterol. Hepatol. 33, 1271–1276 (2018).
Guo, W. et al. Screening of the nutritional risk of patients with gastric carcinoma before operation by NRS 2002 and its relationship with postoperative results. J. Gastroenterol. Hepatol. 25, 800–803 (2010).
Wang, S. et al. The value of L3 skeletal muscle index in evaluating preoperative nutritional risk and long-term prognosis in colorectal cancer patients. Sci. Rep. 10, 8153 (2020).
Kushiyama, S. et al. The preoperative geriatric nutritional risk index predicts postoperative complications in elderly patients with gastric cancer undergoing gastrectomy. In Vivo 32, 1667–2172 (2018).
Hirahara, N. et al. Prediction of postoperative complications and survival after laparoscopic gastrectomy using preoperative geriatric nutritional risk index in elderly gastric cancer patients. Surg. Endosc. 35, 1202–1209 (2020).
Sugawara, K. et al. Geriatric nutrition index influences survival outcomes in gastric carcinoma patients undergoing radical surgery. J. Parenter. Enteral. Nutr. 45, 1042–1051 (2020).
Peng, S. M. et al. The geriatric nutritional risk index as a prognostic factor in patients with advanced non-small-cell lung cancer. Nutr Cancer 2020, 1–10 (2020).
Sasaki, M. et al. The geriatric nutritional risk index predicts postoperative complications and prognosis in elderly patients with colorectal cancer after curative surgery. Sci. Rep. 10, 10744 (2020).
Carnie, L. et al. Impact on prognosis of early weight loss during palliative chemotherapy in patients diagnosed with advanced pancreatic cancer. Pancreatology 20, 1682–1688 (2020).
Kim, K. H. et al. Oncologic impact of preoperative prognostic nutritional index change in resected pancreatic cancer following neoadjuvant chemotherapy. Pancreatology 20, 247–253 (2020).
Hu, S. P. et al. The prognostic value of preoperative geriatric nutritional risk index in patients with pancreatic ductal adenocarcinoma. Cancer Manag. Res. 12, 385–395 (2020).
Kanno, H. et al. Geriatric nutritional risk index predicts prognosis in hepatocellular carcinoma after hepatectomy: A propensity score matching analysis. Sci. Rep. 11, 9038 (2021).
Sakamoto, T. et al. The prognostic significance of combined geriatric nutritional risk index and psoas muscle volume in older patients with pancreatic cancer. BMC Cancer 21, 342 (2021).
Funding
This study received no external funding.
Author information
Authors and Affiliations
Contributions
Conception: N.F. and Y.T. Acquisition of data: A.S., T.U. and M.U. Analysis of data: N.F., M.I., C.I. and K.T. Writing: S.N.F., K.S. and K.O. Critical revision: all authors. Final approval: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Funamizu, N., Sakamoto, A., Utsunomiya, T. et al. Geriatric nutritional risk index as a potential prognostic marker for patients with resectable pancreatic cancer: a single-center, retrospective cohort study. Sci Rep 12, 13644 (2022). https://doi.org/10.1038/s41598-022-18077-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-18077-z
This article is cited by
-
The impact of preoperative nutritional status on postoperative outcomes: an insight from Geriatric Nutritional Risk Index in elderly pancreaticoduodenectomy patients
BMC Surgery (2024)
-
Combined Systemic Immune-inflammatory Index (SII) and Geriatric Nutritional Risk Index (GNRI) predict survival in elderly patients with hip fractures: a retrospective study
Journal of Orthopaedic Surgery and Research (2024)
-
Prognostic potential of nutritional risk screening and assessment tools in predicting survival of patients with pancreatic neoplasms: a systematic review
Nutrition Journal (2024)
-
Prognostic value of preoperative geriatric nutritional risk index in intrahepatic cholangiocarcinoma after hepatectomy: a single‑center retrospective cohort study
Langenbeck's Archives of Surgery (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
