
Abstract
TP53 is one of the most frequently altered genes in prostate cancer. The precise assessment of its focal alterations in primary tumors by immunohistochemistry (IHC) has significantly enhanced its prognosis. p53 protein expression and lymphovascular invasion (LVI) were evaluated for predicting metastatic progression by IHC staining of representative whole-mounted prostate sections from a cohort of 189 radical prostatectomy patients with up to 20 years of clinical follow-up. Kaplan–Meier survival curves were used to examine time to distant metastasis (DM) as a function of p53 expression and LVI status. TP53 targeted sequencing was performed in ten tumors with the highest expression of p53 staining. Nearly half (49.8%) of prostate tumors examined showed focal p53 expression while 26.6% showed evidence of LVI. p53(+) tumors had higher pathologic T stage, Grade Group, Nuclear Grade, and more frequent LVI. p53 expression of > 5% and LVI, individually and jointly, are associated with poorer DM-free survival. TP53 mutations were detected in seven of ten tumors sequenced. Four tumors with the highest p53 expression harbored likely pathogenic or pathogenic mutations. High levels of p53 expression suggest the likelihood of pathogenic TP53 alterations and, together with LVI status, could enhance early prognostication of prostate cancer progression.
Similar content being viewed by others


Introduction
Prostate cancer (PCa) is the most common cancer and the second leading cause of cancer death among American men1. Although the presence of distant metastases at the time of diagnosis is rare, the likelihood of disease progression creates a need for predictive and prognostic biomarkers. Several potential molecular markers have been evaluated in radical prostatectomy (RP) specimens by immuno-histochemistry (IHC)2, and in biopsy tissues by multiplex immunofluorescence3, but none have become widely used in clinical practice. Recent genomic analyses support the association of TP53 mutations with the initiation and progression of diverse neoplasms4,5. In both localized and advanced prostate cancers, TP53 is one of the most frequently altered genes6,7. Approximately 6–7% of primary tumors carry TP53 missense, frameshift, or truncation mutations, and at least 1% have homozygous deletions7,8. Genomic analysis of non-indolent localized PCa revealed TP53 to be one of six genes with > 2% somatic single nucleotide variants (SNVs)9. The higher frequency of TP53 lesions in localized cancers suggests that they arise relatively early in disease progression. In advanced PCa, the rate of TP53 mutations becomes significantly enriched, approaching 40% SNVs, and 10% homozygous deletions or genomic rearrangements10,11,12.
TP53 mutations that increase the stability and half-life of mutant proteins in cancer cells and enhance protein detection by IHC4,13,14 characterize a subgroup of biologically aggressive prostate cancers with high risk of progression after prostatectomy. Multiple studies have reported a correlation between IHC detection of p53 and PCa progression14,15,16,17,18,19,20. DNA sequencing of p53 positive (p53(+)) prostate tumors from 16 patients by Griewe et al., found a 69% correlation between p53 expression and TP53 mutation21. Schlomm et al., reported a low frequency of p53(+) tumors (2.5% or 62/2514) by IHC in a tissue microarray from RP specimens, of which 47% (29/62) were found to harbor mutations associated with more aggressive disease18. In another screen of two overlapping RP patient cohorts with primary prostate tumors, Guedes et al. reported a high positive predictive value (84%) of p53 nuclear staining for underlying TP53 missense mutation4. Importantly, in a single-patient longitudinal study, p53(+) metastatic lesions that developed years post-surgery could be traced to a low-grade p53(+) tumor focus in the primary tumor22. These findings emphasize the biological impact of focal TP53 alterations in the clonal progression of PCa and support p53 IHC detection in primary PCa as a surrogate indicator of TP53 missense mutations.
In PCa, lymphovascular invasion (LVI) has been shown to be associated with aggressive disease and poor prognosis, as defined by reduced biochemical recurrence (BCR) progression-free survival23,24,25, increased risk of PCa-specific mortality26,27 and other pathologic features of aggressive disease28,29. LVI has been evaluated with either TP53 mutation or p53 expression in association with gastric30, colorectal31, bladder32 and breast cancer33 prognosis, but not PCa. This study examines the role of p53 protein expression and LVI in predicting distant metastasis (DM) in a RP cohort with long-term follow-up. We further explored the combined effect of p53 expression and LVI status on DM-free survival. To determine if tumors with higher p53 expression also harbor TP53 mutations, targeted TP53 sequencing was performed on a subset of prostate tumors with the highest percent of p53 expression.
Methods
Study design, population, and clinical assessment
Prostate specimens and clinical-pathologic data were collected from patients undergoing treatment at the Walter Reed National Military Medical Center (WRNMMC) from 1993 to 2013 who provided written informed consent for the use of all data and biospecimens obtained. Patients who had biopsy positive, organ-confined PCa and underwent RP as primary treatment (≤ 6 months post-diagnosis) were included, and those who underwent neo-adjuvant hormonal therapy were excluded. Archived, whole-mounted RP specimens from 50 patients who developed DM at least one year following diagnosis and from 139 patients without evidence of BCR or DM after at least 10 years follow-up, were analyzed. The presence of distant metastases was ascertained by the review of each patient’s complete radiographic scan history that included bone scan, computed tomography (CT), positron emission tomography (PET), as well as pelvic and bone magnetic resonance imaging (MRI). Subjects who reached the end of the study period without evidence of PCa metastases, had their last known follow-up, or died without evidence of metastasis before the end of the study period (December 31, 2013), were defined as non-metastatic. This work was approved by the Institutional Review Boards of WRNMMC, the Uniformed Services University of the Health Sciences (USU), and the Joint Pathology Center (JPC) (Protocol number DBS.2020.110).
Immunohistochemistry and pathologic assessment
Preparation and histologic evaluation of whole-mounted RP specimens were performed as previously described34,35. Adjacent, four-micron sections from a representative tissue block containing the index tumor were stained with hematoxylin and eosin (H&E), anti-p53 mouse monoclonal antibody (DO-7, Biocare Medical, Pacheco, CA), and anti-podoplanin antibody (D2-40, Biocare Medical) to identify p53 and lymphatic vessels, respectively. Slides were reviewed using the 2014 International Society of Urological Pathology (ISUP) guidelines36 by a single genitourinary pathologist (I.A.S.), who was blinded to clinical outcomes. The p53 status in index tumors was scored as positive based on the detection of nuclear p53 staining, percent area stained, and staining intensity. Cells were recorded as p53 positive or p53(+), when brown chromogen (3,3’-Diaminobenzidine (DAB)) used to stain the DO-7 antibody was detected in the nuclei of any tumor cells, and as negative or p53(−) in the absence of any nuclear staining. Occasional tumor cells with exclusive cytoplasmic staining of any intensity were considered “negative”. Percentage of p53(+) staining was estimated as the area of p53(+) tumor cells with nuclear staining divided by total index tumor area16, which was categorized as 0%, 1–5%, and > 5% p53(+) expression. p53 staining intensity was also quantified as 1 + (light), 2 + (medium), and 3 + (maximum) intensity37. An independent pathologist review of p53 staining was performed by A.P.B. Findings were presented as percentage of p53 expression. LVI status was recorded as positive or LVI(+), when tumor cells were present within spaces lined by lymphovascular endothelium with characteristic podoplanin staining, and as negative or LVI(−) in the absence of any staining.
Statistical analysis
Overall and p53-stratified (0%, 1–5%, > 5%) distributions for patient demographics, as well as clinical and pathologic features were compared using Student’s T-test for continuous variables and Chi-square and ANOVA tests for categorical variables. Fisher’s exact test was used when > 20% of expected cell counts had less than five observations. Unadjusted Kaplan–Meier (KM) estimation curves were used to examine time to DM as a function of p53 status. Log-rank test and its associated p-value are reported for KM models. Associations of p53 and LVI with DM-free survival were first evaluated independently and then jointly. Multivariable Cox Proportional Hazards analysis was used to model DM-free survival, controlling for demographic and pathologic factors. The assumption of proportional hazards was tested and confirmed for all KM and Cox models. All statistical tests were 2-sided (summary α-error = 0.05), and the decision rule was based on p < 0.05. All statistical analyses were performed using SAS version 9.4.
TP53 mutation analysis
Index tumors were scraped from two adjacent whole-mounted FFPE sections derived from ten cases that were selected for targeted sequencing. Library preparations and sequencing reactions were conducted at GENEWIZ, Inc. (South Plainfield, NJ). Gene-specific primers targeting the TP53 CDS were multiplexed into three pools. A sequencing library was prepared using the NEBNext Ultra DNA Library Preparation Kit (New England Biolabs, Ipswich, MA), validated using an Agilent TapeStation (Agilent Technologies, Palo Alto, CA), and quantified by Qubit (Invitrogen, Thermo Scientific, Waltham, MA) and real-time PCR (Applied Biosystems, Carlsbad, CA). Multiplexed DNA libraries were loaded on an Illumina MiSeq instrument (Illumina, San Diego, CA) for 2 × 150 bp paired-end sequencing. Image analysis and base calling were performed using MiSeq Control. Raw reads were aligned to the GRCh37 human reference genome using Burrows-Wheeler Aligner-mem. Samtools fixmate was used to correct any flaws in read-pairing introduced during alignment, and duplicate reads were marked using Picard. Alignments were subjected to base quality score recalibration, according to GATK best practices. Variants were identified using GATK Haplotype Caller and FreeBayes and annotated using the Ensembl Variant Effect Predictor toolset that included Sanger Catalogue of Somatic Mutations In Cancer (COSMIC) and ClinVar annotations from March 2021.
Ethics approval and consent to participate
These prostate specimens and clinical-pathologic data in this study were collected from patients undergoing treatment at the WRNNMMC who provided written informed consent for their use. This work was approved by the Institutional Review Boards of the WRNMMC, USU, and JPC (Protocol number DBS.2020.110) and performed in accordance with the Declaration of Helsinki.
Disclaimers
The contents of this publication are the sole responsibility of the author(s) and do not necessarily reflect the views, opinions or policies of the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Uniformed Services University of the Health Sciences (USUHS), the Department of Defense (DoD) or the Departments of the Army, Navy, or Air Force, or any other agency of the US Government. The mention of trade names, specific commercial products, scientific instrumentation, or organizations is considered an integral part of the scientific endeavor and does not constitute endorsement or implied endorsement on the part of the author, DoD, or the US Government.
Results
Association of p53 expression and LVI with pathologic features
Pathologic features of tumors in adjacent whole-mounted prostate sections that were immuno-stained with p53, podoplanin and H&E were evaluated together for p53 expression and LVI status. Representative cases with 1–5% and > 5% p53 staining for each of the three Grade Group (GG) clusters, GG1-3, GG4 and GG5, are shown in Fig. 1. The presence of both lymphovascular invasion and p53 staining in index tumors are represented by cases in Fig. 2. Cells with p53(+) nuclear staining appeared as isolated cells (Figs. 1A and 2A), in clusters (Fig. 1C,G,K, and Fig. 2D), or both (Fig. 1E,I). Focal p53(+) staining was present in 94 (49.8%) and absent in 95 (50.2%) men. Among patients with p53(+) nuclear staining, 40% exhibited 1–5% expression, most (80%) of which had about 1% p53 expression (Table 1). Among the 75 subjects with 1–5% p53 expression, we noted that 60 cases (80%) had 1% expression, four cases had 2% expression, three cases had 3% expression, and eight cases had 5% expression. The median of percentage p53 expression among the 19 subjects with > 5% p53 expression is 25%. Generally, most subjects at or below the threshold of 5% p53 expression showed either light (1 +) (40% or 30 cases) or medium (2 +) (55% or 41 cases) staining intensity, while only 5% (four cases) showed maximum (3 +) staining intensity. In contrast, most subjects with > 5% p53 expression showed 3 + intensity (58% or 11 cases), while the remaining cases showed either 2 + (32% or six cases) or 1 + (10% or 2 cases) staining intensity. Higher levels of p53(+) nuclear staining were associated with aggressive tumor pathologic features, as indicated by pathologic T stage (pT), GG, Nuclear Grade, and LVI.

Representative p53 expression in index tumors clustered by tumor grade. p53 staining, detected at variable degrees of intensity between 1 and 5% (A, E and F) and > 5% (C, G, and K) and their corresponding sections stained with (H&E) are shown for each of the GG clusters: GG 1–3 (A to D), GG 4 (E to H), and GG 5 (I to L). Images were captured at 10X magnification. Arrowhead indicates individual cells stained by the p53 antibody.

Representative p53 and lymphovascular staining in index tumors. p53 staining was detected at variable degrees of intensity between 1 and 5% in single cells (A) and in clusters of cells with greater than 5% (D) in relation to the area of the index tumor. The infiltration of tumor cells into lymphovascular spaces was confirmed by D2-40 IHC staining (B,E). The corresponding (H&E) images are shown in panel (C) and (F). Images were captured at 10X magnification. Arrowhead indicates individual cells stained by the p53 and D2-40 monoclonal antibodies.
Lymphovascular invasion was characterized by the infiltration of tumor cells within spaces lined by D2-40 stained lymphovascular endothelium (Fig. 2B,E), which confirmed features observed in the corresponding hematoxylin and eosin images (Fig. 2C,F, respectively). Evaluation of whole-mounted sections immuno-stained with D2-40 showed that 50 of 188 specimens (26.6%) were LVI(+) while 138 (73.4%) had no evidence of LVI. We observed that lymphovascular invasion was positively associated with p53 expression. Among p53(+) cases, 39.8% (37/93) were LVI(+) compared to p53(−) cases, where only 13.7% were LVI(+). Furthermore, more than half or 55.6% of patients with > 5% p53(+) expression were LVI(+) compared to 36% of patients with 1–5% p53(+) expression and 13.7% of p53(−) patients (Table 1; p < 0.0001). LVI(+) status was also associated with higher diagnostic PSA and pathologic features of more aggressive disease, including higher pT, GG, and Nuclear Grade, and positive surgical margin (Table 2). No association between p53 expression or LVI status with patient self-reported race was observed (Tables 1 and 2).
Focal p53 expression and LVI in RP specimens predict metastatic progression
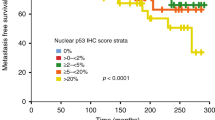
Distant metastasis developed in 68.4% of patients with > 5% p53(+) expression but only in 20% and in 24% of those without p53 or with 1–5% p53(+) expression, respectively (Table 1). Unadjusted univariable KM analysis showed that > 5% p53 expression was associated with significantly poorer DM-free survival (Fig. 3A). Separation in KM curves across levels of p53(+) expression occurred by three years post-RP. Notably, patients without detectable p53 expression and those with 1–5% p53(+) expression, had comparable DM-free survival outcomes.

Product limit estimates for p53 and LVI with distant metastasis-free survival as endpoint events. Unadjusted Kaplan–Meier estimation curves showing models of time from surgery to DM-free survival as a function of p53 expression (A), LVI status (B), and combined p53 expression and LVI status (C), in index tumors as key independent study predictors for all patients (N = 189).
The association between LVI status and DM revealed that 60% (30/50) of LVI(+) patients developed DM compared to 14.5% (20/138) of those without LVI (Table 2). In univariable KM analysis, LVI(+) status predicted significantly poorer DM-free survival (Fig. 3B) with separation in KM curves observed early in subject follow-up. Further evaluation of the association of p53 protein expression together with LVI was performed by merging the 0% and 1–5% p53 expression groups into one 0–5% p53(+) category. KM analysis of the joint roles of p53 and LVI status showed the poorest DM-free survival in patients with > 5% p53(+) and LVI(+) status, among which 81.8% developed DM (Fig. 3C; Table 2).
Multivariable Cox proportional hazard models predict distant metastasis-free survival
Multivariable Cox Proportional hazards analysis was used to examine independent and joint roles of p53 expression and LVI status, together with patient’s age at RP and race, on DM-free survival (Table 3). Three approaches were used: (1) Model One shows a strong correlation between p53 expression of > 5% and increased risk of DM, which increases the hazard for this event by three-fold (hazard ratio (HR) = 3.173; p = 0.0006). (2) Model Two shows that both > 5% p53 expression and LVI(+) are independent predictors of shorter time to DM. When other covariates were held constant, the hazard for DM increased by two-fold (HR = 2.224; p = 0.0225) for > 5% p53 expression, and by four-fold (HR = 4.053; p < 0.0001) for LVI(+) status (3) In Model Three, the joint analysis of p53 expression and LVI status showed that p53 expression of > 5% and LVI(+) status confer incremental risk for DM: the hazard for this event increased by 4.4-fold-fold (HR = 4.428; p = 0.0091) based on > 5% p53 expression alone, and by almost five-fold (HR = 4.839; p < 0.0001) based on LVI(+) status alone, but together they increased the risk by almost eight-fold (HR = 7.976; p < 0.0001). This suggests a strong mutual and additive impact of higher p53 expression and LVI(+) status on DM-free survival. By contrast, in all three models, after adjusting for the patient’s race and p53 expression levels or LVI(+) status, an additional year of age at RP was shown to induce hazards of DM only by a factor of 1.03 to 1.04 (or 3–4%). Thus, increasing age at RP contributes little to the difference in the risk of DM. Likewise, after adjusting for the patient’s age and p53 expression levels, the patient’s race had no significant effect on the hazard of DM. The poorest DM-free survival outcomes were observed among patients who exhibited both > 5% p53(+) and LVI(+) status. In all models, significant correlations between GG and pT with p53 and LVI status prevented their inclusion in multivariate models. Moreover, too few patients were observed in lower GG (1–2) and stage categories.
Association between TP53 mutations and p53 expression or LVI status
Tumor specimens of ten patients with the highest p53 staining (20% to 90%) were selected for targeted TP53 sequencing. The high-depth coverage achieved by TP53 targeted sequencing allowed SNVs to be detected at relatively higher alternate allele frequencies of 0.11 to 0.51. Almost all patients sequenced for TP53 developed aggressive disease, represented by GG 4 or 5, pT3, or DM (Table 4). At least one missense or nonsense TP53 mutation was detected in seven patients, and two mutations were detected in one patient. TP53 mutations were detected in all four patients who had both high (> 30%) expression of p53 and LVI(+) status. Interestingly, in all four patients who had both high expression of p53 and LVI(+) status, the TP53 mutations detected were either likely pathogenic or pathogenic alterations, which were also among the most recurrent TP53 mutations in the COSMIC database. In agreement with results showing an association of LVI(+) status with poorer DM-free survival (Table 2 and Fig. 3B), all five subjects sequenced who were LVI(+) further developed DM. The number of cases sequenced, however, were too small to indicate any association of LVI positivity with specific mutational status.
Discussion
In this study, p53 expression and LVI status were examined as key independent predictors of DM. High p53 expression was significantly associated with DM, the frequency of which was three-fold higher in patients with > 5% p53(+) compared to patients with 0–5% p53(+). By stratifying the data at > 5% cut-off, we were able to distinguish between two clinically relevant p53(+) populations: patients with > 5% p53(+) have significantly shorter DM-free survival than those with 0–5% p53(+). Likewise, the presence of LVI is associated with higher frequency of DM. LVI(+) patients developed DM at a rate that was four-fold higher than those without LVI. Further analysis by unadjusted univariable KM further confirmed that LVI(+) status significantly predicts poorer DM-free survival. Subsequent combined examination of p53 expression and LVI by multivariable analyses showed that together, they exerted an additive increase in risk for DM.
Although multiple studies have shown an association between p53 expression and TP53 mutation4,18,21,22, inconsistencies were noted by others. These discrepancies could be attributed to limitations of the IHC assay, including antibodies used for detection38,39, or to study cohort selection40. The focality of TP53 alterations in primary PCa can lead to differences in IHC interpretations or DNA sequencing assays4,16,21. Since p53 IHC detection depends on the increased half-life of mutant proteins, proteins with destabilizing mutations may escape detection41. The lower frequency of TP53 mutations in localized prostate cancers could reduce the likelihood for finding an association with increased p53 expression18,40. Since p53 nuclear accumulation is far more frequent in higher grade carcinomas, performing IHC on all primary prostate cancers at diagnosis is unlikely to establish the expected association4. By contrast, this study is designed to focus on defining the association of p53 expression and LVI status with DM. Hence, the proportion of subjects with advanced stage (pT3-4) and grade (GG 4 & 5) is greater in this cohort than subjects who undergo RP without neoadjuvant therapy in the general population. One advantage of this study is the availability of primary PCa specimens with associated long-term follow-up (median = 13 years) data obtained from an equal-access military treatment facility. The greater proportion of patients with aggressive disease, who undergo RP without neo-adjuvant therapy in this cohort compared to patients in the general population allowed us to demonstrate the striking association between both focal p53(+) expression and LVI(+) status, and the development of DM. Furthermore, the use of whole-mounted prostate sections augmented the comprehensive evaluation of p53 expression and LVI in index tumors compared to using tissue microarrays18,42 or biopsy specimens38,43. Lastly, the concordant scores of percent p53 expression between two independent pathologists further validated that this approach was more reproducible than by staining intensity alone (92% vs. 72%, respectively).
Based on earlier reports that p53 positive tumors were likely due to mutations that increased the half-life of the p53 protein, we hypothesized that tumors with the highest percentage p53 expression would have a higher probability of harboring TP53 mutations. To test this notion, we selected ten cases with the highest percentage of p53 expression for targeted TP53 sequencing. TP53 mutations were detected in seven of ten cases analyzed. These mutations, which include the most recurrent hotspot at Arginine 273, were previously reported in advanced or metastatic PCa and annotated in COSMIC44 and ClinVar45 databases. Four patients harboring likely pathogenic or pathogenic TP53 mutations had aggressive disease represented by GG 5, pT3 and LVI(+) tumors that progressed to DM. Consistent with earlier reports, concordance between p53 staining and the presence of pathogenic TP53 mutations further supports the prognostic utility of IHC detection as a surrogate read-out for TP53 mutations4,21.
Although LVI is known to be associated with aggressive disease and poor prognosis in PCa, no direct comparison to TP53 mutations or its protein expression has been performed23,24,25,26. One study reported ERG(+) tumors had higher LVI and lower p53 expression in ERG(+) tumors, but no significant association was detected due to sample size (N = 51)46. The most striking finding of this study was that 81.8% of patients with both > 5% p53(+) expression and LVI(+) status developed DM after an extended follow-up period, while 87.7% patients with LVI(−) and < 5% p53(+) were DM-free. The joint interpretation of these two variables is underscored by three key findings: (1) p53(+) expression of > 5% strongly correlates with LVI(+) status, (2) multivariate analysis suggests p53 expression and LVI status to be additive, and (3) tumors with lower p53 expression of 1–5% may represent less aggressive disease as these patients have DM-free survival outcomes that are remarkably similar to patients without p53 staining.
Conclusion
Our findings validated the association between pathogenic TP53 mutations and higher p53 expression, which support the IHC staining of p53 as a substitute for detecting TP53 mutations. Primary prostate tumors with combined focal p53(+) of > 5% and LVI(+) status are highly predictive of future DM and should be classified as highly aggressive tumors. This subset of patients may require a more rigorous treatment plan and follow-up protocol. Taken together, determination of p53 expression and LVI status in primary PCa has promising potential to improve prognostication and early prevention of metastatic progression.
Data availability
The datasets generated and analyzed in this study are not publicly available due to restrictions imposed by the current IRB protocol but can be made available from the corresponding author upon approval of a separate IRB protocol allowing for their subsequent use.
References
Siegel, R. L., Miller, K. D., Fuchs, H. E. & Jemal, A. Cancer statistics, 2021. CA Cancer J Clin 71, 7–33. https://doi.org/10.3322/caac.21654 (2021).
Huber, F. et al. Comprehensive validation of published immunohistochemical prognostic biomarkers of prostate cancer—what has gone wrong? A blueprint for the way forward in biomarker studies. Br. J. Cancer 112, 140–148. https://doi.org/10.1038/bjc.2014.588 (2015).
Blume-Jensen, P. et al. Development and clinical validation of an in situ biopsy-based multimarker assay for risk stratification in prostate cancer. Clin. Cancer Res. 21, 2591–2600. https://doi.org/10.1158/1078-0432.CCR-14-2603 (2015).
Guedes, L. et al. Analytic, pre-analytic and clinical validation of p53 immunohistochemistry for detection of TP53 missense mutation in prostate cancer. Clin. Cancer Res. https://doi.org/10.1158/1078-0432.ccr-17-0257 (2017).
Kandoth, C. et al. Mutational landscape and significance across 12 major cancer types. Nature 502, 333–339. https://doi.org/10.1038/nature12634 (2013).
Alexandrov, L. B. et al. Signatures of mutational processes in human cancer. Nature 500, 415–421. https://doi.org/10.1038/nature12477 (2013).
The Cancer Genome Atlas Research Network. The molecular taxonomy of primary prostate cancer. Cell 163, 1011–1025. https://doi.org/10.1016/j.cell.2015.10.025 (2015).
Barbieri, C. E. et al. Exome sequencing identifies recurrent SPOP, FOXA1 and MED12 mutations in prostate cancer. Nat. Genet. 44, 685–689. https://doi.org/10.1038/ng.2279 (2012).
Fraser, M. et al. Genomic hallmarks of localized, non-indolent prostate cancer. Nature 541, 359–364. https://doi.org/10.1038/nature20788 (2017).
Robinson, D. R. et al. Integrative clinical genomics of metastatic cancer. Nature 548, 297–303. https://doi.org/10.1038/nature23306 (2017).
Grasso, C. S. et al. The mutational landscape of lethal castration-resistant prostate cancer. Nature 487, 239–243. https://doi.org/10.1038/nature11125 (2012).
Armenia, J. et al. The long tail of oncogenic drivers in prostate cancer. Nat. Genet. 50, 645–651. https://doi.org/10.1038/s41588-018-0078-z (2018).
Bartek, J., Iggo, R., Gannon, J. & Lane, D. P. Genetic and immunochemical analysis of mutant p53 in human breast cancer cell lines. Oncogene 5, 893–899 (1990).
Stricker, H. J., Jay, J. K., Linden, M. D., Tamboli, P. & Amin, M. B. Determining prognosis of clinically localized prostate cancer by immunohistochemical detection of mutant p53. Urology 47, 366–369. https://doi.org/10.1016/S0090-4295(99)80454-3 (1996).
Heidenberg, H. B. et al. Alteration of the tumor suppressor gene p53 in a high fraction of hormone refractory prostate cancer. J. Urol. 154, 414–421. https://doi.org/10.1097/00005392-199508000-00024 (1995).
Bauer, J. J. et al. p53 nuclear protein expression is an independent prognostic marker in clinically localized prostate cancer patients undergoing radical prostatectomy. Clin. Cancer Res. 1, 1295–1300 (1995).
Moul, J. W. et al. Protein expression of p53, bcl-2, and KI-67 (MIB-1) as prognostic biomarkers in patients with surgically treated, clinically localized prostate cancer. Surgery 120, 159–166. https://doi.org/10.1016/s0039-6060(96)80283-2 (1996).
Schlomm, T. et al. Clinical significance of p53 alterations in surgically treated prostate cancers. Modern Pathol. 21, 1371–1378. https://doi.org/10.1038/modpathol.2008.104 (2008).
Verma, R. et al. Significance of p53 and ki-67 expression in prostate cancer. Urol. Ann. 7, 488–493. https://doi.org/10.4103/0974-7796.158507 (2015).
Quinn, D. I. et al. p53 nuclear accumulation as an early indicator of lethal prostate cancer. Br. J. Cancer 121, 578–583. https://doi.org/10.1038/s41416-019-0549-8 (2019).
Griewe, G. L. et al. p53 Immunostaining guided laser capture microdissection (p53-LCM) defines the presence of p53 gene mutations in focal regions of primary prostate cancer positive for p53 protein. Prostate Cancer Prostatic Dis. 6, 281–285. https://doi.org/10.1038/sj.pcan.4500665 (2003).
Haffner, M. C. et al. Tracking the clonal origin of lethal prostate cancer. J. Clin. Investig. 123, 4918–4922. https://doi.org/10.1172/jci70354 (2013).
Baydar, D. E., Baseskioglu, B., Ozen, H. & Geyik, P. O. Prognostic significance of lymphovascular invasion in clinically localized prostate cancer after radical prostatectomy. Sci. World J. 8, 303–312. https://doi.org/10.1100/tsw.2008.49 (2008).
Luo, H. L., Chiang, P. H., Chen, Y. T. & Cheng, Y. T. Lymphovascular invasion is a pathological feature related to aggressive cancer behavior and predicts early recurrence in prostate cancer. Kaohsiung J. Med. Sci. 28, 327–330. https://doi.org/10.1016/j.kjms.2011.10.007 (2012).
Fajkovic, H. et al. Validation of lymphovascular invasion is an independent prognostic factor for biochemical recurrence after radical prostatectomy. Urol. Oncol. 34(233), e231-236. https://doi.org/10.1016/j.urolonc.2015.10.013 (2016).
Cheng, L. et al. Lymphovascular invasion is an independent prognostic factor in prostatic adenocarcinoma. J. Urol. 174, 2181–2185. https://doi.org/10.1097/01.ju.0000181215.41607.c3 (2005).
Saeter, T. et al. Combining lymphovascular invasion with reactive stromal grade predicts prostate cancer mortality. Prostate 76, 1088–1094. https://doi.org/10.1002/pros.23192 (2016).
Huang, Y. et al. The prognostic value of lymphovascular invasion in radical prostatectomy: A systematic review and meta-analysis. Asian J. Androl. 18, 780–785. https://doi.org/10.4103/1008-682x.156636 (2016).
Jiang, W. et al. The impact of lymphovascular invasion in patients with prostate cancer following radical prostatectomy and its association with their clinicopathological features: An updated PRISMA-compliant systematic review and meta-analysis. Medicine Baltimore 97, e13537. https://doi.org/10.1097/MD.0000000000013537 (2018).
Tahara, T. et al. Mutation spectrum of TP53 gene predicts clinicopathological features and survival of gastric cancer. Oncotarget 7, 42252–42260. https://doi.org/10.18632/oncotarget.9770 (2016).
Russo, A. et al. The TP53 colorectal cancer international collaborative study on the prognostic and predictive significance of p53 mutation: Influence of tumor site, type of mutation, and adjuvant treatment. J. Clin. Oncol. 23, 7518–7528. https://doi.org/10.1200/JCO.2005.00.471 (2005).
Lotan, Y. et al. Prospective evaluation of a molecular marker panel for prediction of recurrence and cancer-specific survival after radical cystectomy. Eur. Urol. 64, 465–471. https://doi.org/10.1016/j.eururo.2013.03.043 (2013).
Widodo, I. et al. Clinicopathological significance of lymphangiogenesis and tumor lymphovascular invasion in indonesian breast cancers. Asian Pac. J. Cancer Prev. 14, 997–1001. https://doi.org/10.7314/apjcp.2013.14.2.997 (2013).
Furusato, B. et al. ERG oncoprotein expression in prostate cancer: Clonal progression of ERG-positive tumor cells and potential for ERG-based stratification. Prostate Cancer Prostatic Dis. 13, 228–237. https://doi.org/10.1038/pcan.2010.23 (2010).
Cullen, J. et al. Predicting prostate cancer progression as a function of ETS-related gene status, race, and obesity in a longitudinal patient cohort. Eur. Urol. Focus 4, 818–824. https://doi.org/10.1016/j.euf.2017.02.016 (2018).
Egevad, L. et al. International society of urological pathology (ISUP) grading of prostate cancer. Am. J. Surg. Pathol. 40, 858–861. https://doi.org/10.1097/PAS.0000000000000642 (2016).
Heidenreich, A. et al. Immunohistochemical and mutational analysis of the p53 tumour suppressor gene and the bcl-2 oncogene in primary testicular germ cell tumours. APMIS 106, 90–990. https://doi.org/10.1111/j.1699-0463.1998.tb01324.x (1998).
Meyers, F. J. et al. Very frequent p53 mutations in metastatic prostate carcinoma and in matched primary tumors. Cancer 83, 2534–2539 (1998).
Wertz, I. E. et al. Correlation of genetic and immunodetection of TP53 mutations in malignant and benign prostate tissues. Hum Pathol 27, 573–580. https://doi.org/10.1016/s0046-8177(96)90164-1 (1996).
Brooks, J. D. et al. An uncertain role for p53 gene alterations in human prostate cancers. Can. Res. 56, 3814–3822 (1996).
Nagata, Y. et al. The stabilization mechanism of mutant-type p53 by impaired ubiquitination: The loss of wild-type p53 function and the hsp90 association. Oncogene 18, 6037–6049. https://doi.org/10.1038/sj.onc.1202978 (1999).
Merseburger, A. S. et al. Limitations of tissue microarrays in the evaluation of focal alterations of bcl-2 and p53 in whole mount derived prostate tissues. Oncol. Rep. 10, 223–228 (2003).
Stackhouse, G. B. et al. p53 and bcl-2 immunohistochemistry in pretreatment prostate needle biopsies to predict recurrence of prostate cancer after radical prostatectomy. J. Urol. 162, 2040–2045 (1999).
Forbes, S. A. et al. COSMIC: Exploring the world’s knowledge of somatic mutations in human cancer. Nucleic Acids Res. 43, D805-811. https://doi.org/10.1093/nar/gku1075 (2015).
Landrum, M. J. et al. ClinVar: Improvements to accessing data. Nucleic Acids Res. 48, D835–D844. https://doi.org/10.1093/nar/gkz972 (2020).
Suryavanshi, M. et al. Weaker ERG expression in patients with ERG-positive prostate cancer is associated with advanced disease and weaker androgen receptor expression: An Indian outlook. Urol. Oncol. 33(331), e339–e315. https://doi.org/10.1016/j.urolonc.2015.03.017 (2015).
Shi, X. B., Gandour-Edwards, R., Beckett, L. A., Deitch, A. D. & de Vere White, R. W. A modified yeast assay used on archival samples of localized prostate cancer tissue improves the detection of p53 abnormalities and increases their predictive value. BJU Int. 94, 996–1002. https://doi.org/10.1111/j.1464-410X.2004.05093.x (2004).
Abida, W. et al. Genomic correlates of clinical outcome in advanced prostate cancer. Proc. Natl. Acad. Sci. U.S.A. 116, 11428–11436. https://doi.org/10.1073/pnas.1902651116 (2019).
Nguyen, B. et al. Pan-cancer analysis of CDK12 alterations identifies a subset of prostate cancers with distinct genomic and clinical characteristics. Eur. Urol. 78, 671–679. https://doi.org/10.1016/j.eururo.2020.03.024 (2020).
Stopsack, K. H. et al. Oncogenic genomic alterations, clinical phenotypes, and outcomes in metastatic castration-sensitive prostate cancer. Clin. Cancer Res. 26, 3230–3238. https://doi.org/10.1158/1078-0432.CCR-20-0168 (2020).
Kumar, A. et al. Substantial interindividual and limited intraindividual genomic diversity among tumors from men with metastatic prostate cancer. Nat. Med. 22, 369–378. https://doi.org/10.1038/nm.4053 (2016).
Robinson, D. et al. Integrative clinical genomics of advanced prostate cancer. Cell 161, 1215–1228. https://doi.org/10.1016/j.cell.2015.05.001 (2015).
Mateo, J. et al. Genomics of lethal prostate cancer at diagnosis and castration resistance. J. Clin. Investig. 130, 1743–1751. https://doi.org/10.1172/JCI132031 (2020).
Acknowledgements
We thank Dr. Indu Kohaar for her critical reading of the manuscript.
Funding
This research was supported by USUHS-CPDR, HU0001-10-2-0002.
Author information
Authors and Affiliations
Contributions
J.W.M, D.G.M, I.L.R. and S.S. acquired funding for the research; J.C., S.S., and I.A.S. conceptualized the study; W.G., K.B.M., S.-H.T., J.C., and I.A.S. curated the results of the study; J.J., Y.C., H-C.K., S.-H.T., and J.C. implemented computer code, supporting algorithms or software used in the research; W.G., J.J., Y.C., H-C.K., and J.C. performed formal analysis of the research data using statistical, mathematical, computational methods; J.W.M., D.G.M., I.L.R., G.P., S.-H.T., J.C., S.S., and I.A.S. supervised the research; J.W.M, D.G.M, I.L.R., J.C., S.S., and I.A.S. provided resources required to perform the research; W.G., C.S., D.Y., J.F., J.J., Y.C., H-C.K., K.B.M., A.B., S.-H.T., J.C., and I.A.S. created models, and developed methodologies used in the research; W.G., C.S., D.Y., J.F., K.B.M., J.W.M., S.-H.T., and I.A.S. conducted the research and investigation process; A.B., G.P., and I.A.S. performed validation of the experimental results; W.G., D.Y., S.-H.T., and I.A.S. contributed to the visualization of the published work; W.G., A.D., S.-H.T., and J.C wrote the initial draft of the manuscript; A.D., G.P., S.-H.T., J.C., S.S., and I.A.S. were responsible for the administration, planning and execution of the research; W.G., C.S., A.D., G.P., S.-H.T., J.C., S.S., and I.A.S. contributed to the writing, reviewing, revision or editing of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gesztes, W., Schafer, C., Young, D. et al. Focal p53 protein expression and lymphovascular invasion in primary prostate tumors predict metastatic progression. Sci Rep 12, 5404 (2022). https://doi.org/10.1038/s41598-022-08826-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-08826-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
