
Abstract
Previous studies have reported the presence of muscle weakness in women with fibromyalgia syndrome (FMS) which is considered a risk factor for developing earlier disability and dependence during activities of daily life (ADL). We aimed to assess the relationship between hand grip force with sociodemographic, clinical, disease-specific, cognitive, and physical function variables in women with FMS. One hundred twenty-six women with FMS completed demographic (age, gender, height, weight, body mass index), pain-related (pain history, pain intensity at rest and during ADL), disease-specific severity (Fibromyalgia Impact Questionnaire -FIQ-S-, Fibromyalgia Health Assessment Questionnaire -FHAQ-, EuroQol-5D, Pain Catastrophizing Scale -PCS-, Pittsburgh Sleep Quality Index-PSQI-, Pain Vigilance and Awareness Questionnaire -PVAQ-, and Central Sensitization Inventory -CSI-), psychological (Tampa Scale for Kinesiophobia, TKS-11; Pain Vigilance and Awareness Questionnaire, PVAQ; Pain Catastrophizing Scale, PCS), and physical function (hand grip force, and Timed Up and Go Test, TUG). Hand grip force was associated with height (r = −0.273), BMI (r = 0.265), worst pain at rest (r = −0.228), pain during ADL (r = −0.244), TUG (r = −0.406), FHAQ (r = −0.386), EuroQol-5D (r = 0.353), CSI (r = −0.321) and PSQI (r = −0.250). The stepwise regression analysis revealed that 34.4% of hand grip force was explained by weight (6.4%), TUG (22.2%), and FHAQ (5.8%) variables. This study found that hand grip force is associated with physical function indicators, but not with fear-avoidance behaviors nor pain-related features of FMS. Hand grip force could be considered as an easy tool for identifying the risk of fall and poorer physical health status.
Similar content being viewed by others

Introduction
Fibromyalgia syndrome (FMS) is a chronic pain condition affecting up to the 6.6% of the general population1, being the third most common musculoskeletal condition after lumbar pain and osteoarthritis2. The annual economic burden per FMS patient is estimated at $38043. FMS is characterized by a plethora of symptoms including widespread pain, physical and mental fatigue, morning stiffness, anxiety, depression, cognitive dysfunctions, sleep problems, autonomic disturbances, exacerbated pain responses (indicators of central sensitization), and reduced health-related quality of quality of life (QoL)4,5,6.
Consistent evidence identifies several sociodemographic, physical, biological, lifestyle, and psychological factors, such as depression, obesity, older age, dietary patterns, smoking, alcohol consumption, higher cortisol levels, greater risk of fall, female sex, lower income and education level, associated with frailty affecting health-related QoL and activities of daily life (ADL)7. Therefore, the fact that the age peak for suffering from FMS is 50–60 years old, the presence of altered cortisol levels, the high prevalence of other associated comorbidities (e.g., anxiety and depression), and considering that 80–90% of FMS sufferers are women8,9 could explain the high impact of FMS on QoL and ADL.
In addition, muscle weakness is a risk factor for developing earlier disability onset and dependence during ADL10 and a preventable contributor to the global burden of morbidity and mortality11. Previous reports have shown that muscle strength is generalized reduced up to 35% of magnitude when comparing FMS women with healthy women12. This generalized weakness may be explained by pathologic changes in muscle fibers, impaired blood circulation, disturbances in regulation of growth and energy metabolism, altered neuromuscular control mechanisms associated with pain and decreased levels of physical activity associated with fear avoidance behaviors, pain, and overweight13,14.
The Hand Grip Force is a reliable, simple, and noninvasive test assessing the strength of the hand muscles used to grasp or grip15,16. This test is considered as a valid indicator to identify frailty and risk of disability among elderly people as is associated with cardiovascular, respiratory, and cancer outcomes and also with mortality17. Evidence supports the presence of reduced hand grip force in women with FMS18,19,20,21,22,23. In addition, reduced hand grip force has been associated with worse severity19,20, higher related-disability21, lower pulmonary muscle strength22, and worse health-related quality of life23 in women with FMS. On the contrary, others did not find an association between hand grip force and severity18,23.
The Time Up and Go test is a physical performance test complementary to the hand grip commonly used tool for screening falls risk and is also considered as a strong predictor of short-term mortality24,25. Most previous studies conducted in FMS included sample sizes < 50 participants and did not consider other variables such as catastrophizing or kinesiophobia which could affect physical function. In fact, an association between physical capacity, including hand grip force, with fear avoidance beliefs has been suggested in FMS13 but also in other pain conditions, e.g., low back pain26. Therefore, the aims of the current study were to analyze the correlation between demographic, pain-related, disease-specific, psychological, physical function measures and hand grip force and also to develop a linear regression model to analyze factors explaining the variance of hand grip force in women with FMS (Fig. 1).

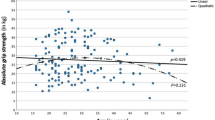
Scatter plot of the adjusted predicted score (r2 adjusted: 0.344) explaining Hand Grip Force score in female patients with fibromyalgia syndrome.
Methods
Study design
An observational cross-sectional study following the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines27 was conducted. The study was approved by the Institutional Ethics Committee of Camilo José Cela University (UCJC 20-10-2020) and Universidad Rey Juan Carlos (URJC 08-30-2020). All participants signed written informed consent prior to their inclusion in the study.
Participants
Consecutive women diagnosed of FMS28 by a rheumatologist and aged between 20 and 70 years old who voluntary responded to a local announcement at AFINSYFACRO Fibromyalgia Association in Madrid (Spain) were screened for eligible criteria. Exclusion criteria included: (1) previous history of whiplash injury, (2) previous surgery; (3) neuropathic condition (e.g., radiculopathy or myelopathy) diagnosed; (4) underlying medical condition (e.g., tumor); or, (5) regular use of drug pharmacological treatment affecting muscle tone or pain perception different than analgesics.
Hand grip force
To evaluate the maximal voluntary hand grip force contraction, a Jamar hand dynamometer (JLW Instruments, Chicago, IL, USA) was used. The Jamar Hydraulic Hand Dynamometer is an enclosed hydraulic system recording the applied strength in kilograms16. The examiner explained and demonstrated the procedure before data collection. To perform the measurement, each subject placed the Jamar in their hand, with the arm beside the trunk, the shoulder in a neutral position, the elbow flexed at 90° and pulled the metal bar with their fingers29. This procedure was conducted bilaterally. The mean of three trials for each side (with 3 min resting periods between repetitions to avoid fatigue) was calculated29. The handle diameter was set at the 19.7% of the participant’s hand length (calculated from the crease of the wrist to the tip of the middle finger with the hand while holding straight and stiff) as recommended by Kong et al.30. The reliability of hand grip force in FMS has been shown to be excellent31.
Pain-related and disease-specific variables
Participants were asked to rate in a 11-point numerical point rate scale (NPRS) their mean pain intensity at rest, the worst pain at rest, and the mean level of pain experienced during ADL. In this scale, 0 was interpreted as “complete absence of pain” and 10 as “the worst imaginable pain”32.
The Spanish version of the fibromyalgia impact questionnaire (FIQ-S) was used to assess the impact of FMS32. This self-reported questionnaire consists of 10 subscales assessing the daily-tasks function, the number of days feeling good during the last 7 days, the interference of FMS with their work, pain intensity, fatigue, night resting, stiffness, anxiety, and depression. The final score ranges from 0 to 100, where greater scores involve greater disability and severity and its reliability has been shown to be good reliability (ICC: 0.81)33.
The Fibromyalgia Health Assessment Questionnaire (FHAQ) is a disease-specific tool used for assessing functional ability in FMS34. Although this self-questionnaire come from the Health Assessment Questionnaire, the FHAQ is a shorter, simpler and easier to quantify in a single questionnaire with 8 items with scores ranging from 0 to 334. The FHAQ final score is calculated as the mean of the 8 items, where lower scores (0) mean less difficulty during their daily functional activities.
Health-related quality of life was assessed with the paper-based five-level version of EuroQol-5D questionnaire since it can be used in specific clinical populations. The EuroQol-5D includes five descriptive health dimensions (mobility, self-care, daily activities, pain and depression/anxiety) ranging from 1 (no problems) to 3 (severe problems). The combination of the scores results in a five-digit value with 243 combinations35. Responses were converted into a single index number between 0 and 1 where 0 corresponds to a health state judged to be equivalent to death and 1 corresponds to optimal health, by applying crosswalk index values for Spain life36.
Sensitization associated-symptoms were assessed with the Central Sensitization Inventory (CSI) since it has excellent test–retest reliability and internal consistency37. This self-reported questionnaire contains a 25-items survey assessing the frequency of symptoms associated with sensitization, rating each question on a 5-point Likert scale where 0 means “never” and 4 means “always”. A total score ranging from 0 to 100 is obtained where a higher total score is associated with more sensitization-related symptoms37.
The Spanish version of the Pittsburgh Sleeping Quality index (PSQI) was used to determine sleep quality38. This valid and reliable self-reported questionnaire consists of 19 questions measuring the subjective sleep quality, duration and latency of sleep, sleep disorders, habitual sleep efficiency, daytime dysfunction and sleep medication in a 0 to 3 scale. The score ranges from 0 (the best sleep quality) to 21 (the worst sleep quality)38. The PSQI has shown proper psychometric properties for assessing sleep quality in FMS39.
Psychological variables
The 11-item short-form of the Tampa Scale for Kinesiophobia (TKS-11)40 was used to quantify the fear of movement since its use is indicated in chronic pain conditions including FMS41. This self-reported questionnaire consists of 11 items where patients have to choose in a 4-point Likert scale how much they agree with each item, being 1 “complete disagreement” and 4 “complete agreement” (total score from 0 to 44)40.
Pain hypervigilance was assessed with the short-form 9-item Spanish Pain Vigilance and Awareness Questionnaire (PVAQ) since this self-reported questionnaire is considered a valid and reliable tool to identify ideas of observing, monitoring and focusing on pain in FMS42.
The Spanish version of the Pain Catastrophizing Scale (PCS) is a 13-item self-reported questionnaire used to assess the patient’s pain catastrophizing response which has demonstrated to be valid for being used in patients with FMS43. All items are answered in a 5-point Likert scale where 0 means “never” and 4 means “always” (score 0–52). This questionnaire analyzes three scales: rumination (constant worry and inability to inhibit thoughts related to pain), magnification (exaggeration of unpleasantness of painful situations and expectations of negative consequences) and despair (inability to face pain)43.
Timed up and go test
We used the Timed Up and Go (TUG) test since is considered an easy, cheap, fast and valid tool providing valuable predictive information to identify patients at a risk of falls25. The patient is placed in sitting position in an armchair and is asked to stand up without the use of the arms, to walk at a comfortable and safe speed up to a line placed at 3 m from the chair, to turn back to the chair, and sit down again. The TUG has shown to be a reliable physical fitness test for assessing agility/dynamic balance in women with FMS44.
Sample size calculation
Sample size calculation was estimated using the G*Power software for Mac OS (v.3.1.6) based on detecting significant small correlations (r = 0.15) between the variables with an alpha level (α) of 0.05 and a desired power (β) of 90%. This generated a sample size of at least 108 participants.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) software v.25 for Mac OS (IBM, Armonk, NY) was used for all statistical analyses. A descriptive analysis was used to describe the sample central tendency and dispersion of all variables. Normal distribution of quantitative variables was verified with Kolmogorov–Smirnov test. Since no side-to-side differences in hand grip force were seen (student t-test for independent samples), the mean was used in the analyses.
The potential associations between the variables were calculated in a correlation matrix by calculating Pearson correlation coefficients (r). In addition, r scores were used to identify multicollinearity and shared variance between the variables (defined as r > 0.80). All statistically significant variables associated with hand grip force (dependent variable) were included into a stepwise multiple linear regression model to quantify their final contribution. The significance criterion of the critical F value for entry into the regression equation was set at P < 0.05. The following independent variables were considered: age, height, weight, body mass index, years with pain, years with FMS, pain intensity, TUG, FIQ-S, FHAQ, EuroQol-5D, CSI, PVAQ, PCS, TSK-11 and PSQI. Changes in adjusted R2 were reported after each step of the regression model to determine the association of the additional variables.
Ethical approval
The Local Ethics Committee of Camilo José Cela University (UCJC 20–10-2020) and Universidad Rey Juan Carlos (URJC 08–30-2020) approved the study design.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Results
One-hundred and forty (n = 140) women with FMS responded to the announcement and were screened for eligibility criteria. Fourteen (10%) were excluded due to previous surgery (n = 8), previous whiplash (n = 4), and pregnancy (n = 2). After exclusion filtering, 126 women (mean age: 52.2 ± 10.7 years) were included. Table 1 shows data of the total sample regarding demographic, pain-related, disease-specific, psychological and physical function.
Bivariate correlation analysis
Bivariate correlation analysis results are reported in Table 2. Hand grip force was negatively associated with the worst pain, PSQI (both, p < 0.05), mean pain during ADL, TUG, FHAQ and CSI (p < 0.01) and positively associated with BMI (p < 0.05), height and EuroQol-5D (p < 0.01). Thus, multiple significant correlations existed among different outcomes (r: 0.189 to 0.640), but none fulfilled multicollinearity level (all, r < 0.80).
Multiple regression analysis
The hierarchical regression analysis explaining the variance of hand grip force is shown within Table 3. Stepwise regression analyses revealed that weight (contributing 6.4%), TUG (additional 22.2%), and FHAQ (additional 5.8%) were significant contributors for hand grip force and, when combined, they explained 34.4% of the variance (r2 adjusted: 0.344). Variance should be interpreted as a measure of how far the observed values differ from the average of predicted values and it ranges from 0 (the dependent variable cannot be explained based on the independent variables listed) to 1 (the dependent variable can be totally explained based on the independent variables).
Discussion
This is the first study performing a regression analysis to identify potential contributors explaining the variance of hand grip force in a female sample of women with FMS. Hand grip force is a reliable and easy to administer way to measure overall physical capacity and muscle strength and a good predictor for impairment, disability and functional ability in a wide variety of rheumatic and neurological conditions45. In fact, recent evidence suggests hand grip force as a possible biomarker of impaired neuromuscular function and a predictor of risk of falls in older women46. Therefore, understanding hand grip force associated factors is essential to develop early screening tools and treatment programs for specific targets in order to avoid the development of earlier disability onset, dependence during ADL, impaired quality of life and early mortality caused by possible accidental falls10,11,12,13,14,19,20,21,22,23. This study revealed that hand grip force was associated with taller size, greater BMI, lower pain intensity at rest and during ADL, better quality of life (i.e., FHAQ and EQ5D), lower sensitization-associated symptoms (i.e., CSI), TUG, and poor sleep quality (i.e., PSQI). These findings support the importance of focusing on physical function assessment and strengthening by including exercise programs as they are clinically effective, no adverse effects and cost-effective complement to the usual care47.
Previous evidence suggests an impact of sex on hand grip force. As hand strength and hand length are closely associated and the fact that hand length is significantly greater in men, this may explain differences48. Similarly, although we did not include male participants due to its limited prevalence and, accordingly, sex differences could not be assessed, we found that demographic features were associated with hand grip force. As hand length can also vary within the same gender as is also associated with anthropometry characteristics, this may explain the height and BMI association with hand grip force. Further, sex differences are more pronounced for the non-dominant than for the dominant hand48. Our results showed that anthropometric variations within the same sex were not enough relevant to involve strength differences between dominant and non-dominant hands.
Pain is the most common symptom associated with FMS and was also associated with hand grip force in the current study. These findings reinforce previous evidence explaining the association between pain intensity with a delay on hand grip initiation, release, and force49. Two mechanisms could explain an initiation delay and prolonged release timings: the avoidance of muscle contraction as a protective mechanism against pain and attributable to fear-avoidance behaviors or hypervigilance, and a reduced quality of sensory feedback caused by sensitization49. A decreased muscle contraction capacity, fear of pain and reinjury and histological muscle changes could explain the decrease muscle strength50. Interestingly, even if hypervigilance, kinesiophobia or catastrophism were associated with multiple variables (pain intensity, quality of life, fibromyalgia impact, sensitization and sleep quality), no association with hand grip force was observed. Other variables (e.g., quantitative sensory tests, neuropathic pain component and psychological factors) not included in our study should be assessed in further research.
Thus, we analyzed the association between hand grip force with life of quality indicators, sleep quality, fibromyalgia impact and TUG. Hip fractures derived from falls are associated with up to a 29% of mortality within one year after injury51. As muscle weakness is the most common modifiable risk factor (in addition to balance deficits and gait instability) associated with fall52 and considering the observed association between FMS impact with TUG, quality of life, kinesiophobia, catastrophism and pain hypervigilance, muscular fitness testing should be included in clinical practice and multidisciplinary exercise programs aiming at improving physical function would be essential to reduce disability, dependence, and risk of falls.
Finally, some potential limitations should be recognized. First, this study consisted of a female sample as male participants accessibility was limited. Therefore, our findings cannot be extrapolated to males. Second, we did not assess pain feature (e.g., neuropathic component), quantitative sensory testing or psychological aspects (e.g., anxiety and depression), which could be potentially associated with physical function in chronic widespread pain syndromes. Finally, longitudinal studies to confirm the association between hand grip force and risk of falls in patients with FMS are needed.
Conclusions
This study found hand grip weakness to be associated with greater sensitization and pain intensity (at rest and during ADL) and poorer quality of life, functional ability and sleep quality whereas larger TUG scores were associated with greater sensitization and poorer quality of life, functional ability, pain catastrophism and kinesiophobia. These finding suggest that both physical tests assess different aspects of FMS and provide synergistic information. Therefore, muscular fitness could be a complementary screening tool during clinical practice and aiming the physical condition strengthening could induce a positive impact on patients’ quality of life, independence, delay on disability onset and risk of early mortality caused by accidental falls.
Data availability
All data derived from this study are presented in the text.
References
Marques, A. P. et al. Prevalence of fibromyalgia: literature review update. Rev. Bras. Reumatol. Engl. Ed. 57, 356–363 (2017).
Spaeth, M. Epidemiology, costs, and the economic burden of fibromyalgia. Arthritis Res. Ther. 11, 117 (2009).
Lacasse, A., Bourgault, P. & Choinière, M. Fibromyalgia-related costs and loss of productivity: a substantial societal burden. BMC Musculoskelet. Disord. 17, 16 (2016).
Sarzi-Puttini, P., Giorgi, V., Marotto, D. & Atzeni, F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 16, 645–660 (2020).
Gostine, M., et al. Clinical characteristics of fibromyalgia in a chronic pain population. Pain Pract. 18, 67–78 (2018)
Demirbag, B. C. & Bulut, A. Demographic characteristics, clinical findings and functional status in patients with fibromyalgia syndrome. J. Pak. Med. Assoc. 68, 1043–1047 (2018).
Feng, Z. et al. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: a systematic review of longitudinal studies. PLoS ONE 12, e0178383 (2017).
Wolfe, F., Walitt, B., Perrot, S., Rasker, J. J. & Häuser, W. Fibromyalgia diagnosis and biased assessment: sex, prevalence and bias. PLoS ONE 13, e0203755 (2018).
Úbeda-D’Ocasar, E. et al. Pain and cortisol in patients with fibromyalgia: Systematic review and meta-analysis. Diagnostics. 10, 922 (2020).
Wang, D. X. M., Yao, J., Zirek, Y., Reijnierse, E. M. & Maier, A. B. Muscle mass, strength, and physical performance predicting activities of daily living: a meta-analysis. J. Cachexia Sarcopenia Muscle. 11, 3–25 (2020).
Celis-Morales, C. A. et al. The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK-Biobank participants. Eur. Heart J. 38(2), 116–122 (2017).
Larsson, A. et al. Controlled, cross-sectional, multi-center study of physical capacity and associated factors in women with fibromyalgia. BMC Musculoskelet. Disord. 19, 121 (2018).
Larsson, A. et al. Pain and fear avoidance partially mediate change in muscle strength during resistance exercise in women with fibromyalgia. J. Rehabil. Med. 49, 744–750 (2017).
Ruggiero, L., Manganelli, F. & Santoro, L. Muscle pain syndromes and fibromyalgia: the role of muscle biopsy. Curr. Opin. Support Palliat. Care. 12, 382–387 (2018).
Hamilton, G. F., McDonald, C. & Chenier, T. C. Measurement of grip strength: validity and reliability of the sphygmomanometer and jamar grip dynamometer. J. Orthop. Sports Phys. Ther. 16, 215–219 (1992).
Lam, N. W. et al. Normative data for hand grip strength and key pinch strength, stratified by age and gender for a multiethnic Asian population. Singapore Med. J. 57, 578–584 (2016).
Celis-Morales, C.A., et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all-cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ. 361, k1651 (2018).
Koklu, K. et al. Handgrip strength in fibromyalgia. Arch. Rheumatol. 31, 158–161 (2016).
Aparicio, V. A. et al. Handgrip strength test as a complementary tool in the assessment of fibromyalgia severity in women. Arch. Phys. Med. Rehabil. 92, 83–88 (2011).
Salaffi, F., Farah, S. & Di Carlo, M. Force-time curve features of handgrip strength in fibromyalgia syndrome. Sci. Rep. 10, 3372 (2020).
Devrimsel, G., Turkyilmaz, A. K., Beyazal, M. S. & Karkucak, M. Assessment of hand function and disability in fibromyalgia. Z. Rheumatol. 78, 889–893 (2019).
Sahin, G., Ulubaş, B., Calikoğlu, M. & Erdoğan, C. Handgrip strength, pulmonary function tests, and pulmonary muscle strength in fibromyalgia syndrome: is there any relationship?. South Med. J. 97, 25–29 (2004).
Harman, H., Ones, K. & Ayna, A. B. The effects of handgrip strength and clinical findings to quality of life in fibromyalgia syndrome. J. Orthop. Res. Physiother. 11, 19 (2015).
Chua, K. Y., Lim, W. S., Lin, X., Yuan, J. M. & Koh, W. P. Handgrip strength and timed up-and-go (TUG) test are predictors of short-term mortality among elderly in a population-based cohort in Singapore. J. Nutr. Health Aging. 24, 371–378 (2020).
Barry, E., Galvin, R., Keogh, C., Horgan, F. & Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta-analysis. BMC Geriatr. 14, 14 (2014).
Lee, J. & Park, S. The relationship between physical capacity and fear avoidance beliefs in patients with chronic low back pain. J. Phys. Ther. Sci. 29, 1712–1714 (2017).
von Elm, E. et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370, 1453–1457 (2007).
Segura-Jiménez, V. et al. Validation of the modified 2010 American College of Rheumatology diagnostic criteria for fibromyalgia in a Spanish population. Rheumatology 53, 1803–1811 (2014).
Hamilton, G. F., McDonald, C. & Chenier, T. C. Measurement of grip strength: validity and reliability of the sphygmomanometer and jamar grip dynamometer. J. Orthop. Sports Phys. Ther. 16(5), 215–219 (1992).
Kong, Y. K. & Lowe, B. D. Optimal cylindrical handle diameter for grip force tasks. Int. J. Ind. Ergon. 35(6), 495–507. https://doi.org/10.1016/j.ergon.2004.11.003 (2005).
Carbonell-Baeza, A. et al. Reliability and feasibility of physical fitness tests in female fibromyalgia patients. Int. J. Sports Med. 36, 157–162 (2015).
Cheatham, S. W., Kolber, M. J., Mokha, M. & Hanney, W. J. Concurrent validity of pain scales in individuals with myofascial pain and fibromyalgia. J. Bodyw. Mov. Ther. 22, 355–360 (2018).
Rivera, J. & González, T. The Fibromyalgia Impact Questionnaire: a validated Spanish version to assess the health status in women with fibromyalgia. Clin. Exp. Rheumatol. 22, 554–560 (2004).
Wolfe, F. et al. The assessment of functional impairment in fibromyalgia (FM): Rasch analyses of 5 functional scales and the development of the FM Health Assessment Questionnaire. J. Rheumatol. 27, 1989–1999 (2000).
Herdman, M. et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20, 1727–1736 (2011).
Van Hout, B. et al. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 15, 708–715 (2012).
Neblett, R. et al. The Central Sensitization Inventory (CSI): establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain. 14, 438–445 (2013).
Hita-Contreras, F. et al. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 34, 929–936 (2014).
Climent-Sanz, C. et al. Patient reported outcome measures of sleep quality in fibromyalgia: a COSMIN systematic review. Int. J. Environ. Res. Public Health. 17, 2992 (2020).
Woby, S. R., Roach, N. K., Urmston, M. & Watson, P. J. Psychometric properties of the TSK-11: a shortened version of the Tampa Scale for Kinesiophobia. Pain 117, 137–144 (2005).
Roelofs, J. et al. Fear of movement and (re)injury in chronic musculoskeletal pain: Evidence for an invariant two-factor model of the Tampa Scale for Kinesiophobia across pain diagnoses and Dutch, Swedish, and Canadian samples. Pain 131(1–2), 181–190 (2007).
Pilar Martínez, M. et al. Spanish version of the Pain Vigilance and Awareness Questionnaire: psychometric properties in a sample of women with fibromyalgia. Span J. Psychol. 17, E105 (2015).
García Campayo, J. et al. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 131, 487–492 (2008).
Collado-Mateo, D. et al. Reliability of the timed up and go test in Fibromyalgia. Rehabil. Nurs. 43, 35–39 (2018).
Nilsen, T. et al. Grip force and pinch grip in an adult population: reference values and factors associated with grip force. Scand. J. Occup. Ther. 19(3), 288–296. https://doi.org/10.3109/11038128.2011.553687 (2012).
Neri, S. G. R., Lima, R. M., Ribeiro, H. S. & Vainshelboim, B. Poor handgrip strength determined clinically is associated with falls in older women. J. Frailty Sarcopenia Falls. 6(2), 43–49 (2021).
Williams, M.A., et al. Strengthening and stretching for Rheumatoid Arthritis of the Hand (SARAH). A randomised controlled trial and economic evaluation. Health Technol. Assess. 19(19),1–222 (2015). doi:https://doi.org/10.3310/hta19190
Wichelhaus, A. et al. Parameters influencing hand grip strength measured with the manugraphy system. BMC Musculoskelet. Disord. 19(1), 54. https://doi.org/10.1186/s12891-018-1971-4 (2018).
Seo, N. J., Sindhu, B. S. & Shechtman, O. Influence of pain associated with musculoskeletal disorders on grip force timing. J. Hand. Ther. 24(4), 335–344. https://doi.org/10.1016/j.jht.2011.06.004 (2011).
Valera-Calero, J. A. et al. Cervical multifidus morphology and quality is not associated with clinical variables in women with fibromyalgia: an observational study. Pain Med. https://doi.org/10.1093/pm/pnab297 (2021).
Haleem, S., Lutchman, L., Mayahi, R., Grice, J. E. & Parker, M. J. Mortality following hip fracture: trends and geographical variations over the last 40 years. Injury 39(10), 1157–1163. https://doi.org/10.1016/j.injury.2008.03.022 (2008).
Medical Advisory Secretariat. Prevention of falls and fall-related injuries in community-dwelling seniors: an evidence-based analysis. Ont. Health Technol. Assess. Ser. 8(2), 1–78 (2008).
Funding
This research was supported by Camilo José Cela University (ID: CENSEN).
Author information
Authors and Affiliations
Contributions
All listed authors participated meaningfully in the study, and they have seen and approved the submission of this manuscript. Conceptualization, C.F.d.-l.-P and J.A.V-C; methodology, all authors; software, all authors; investigation, all authors; resources, all authors; data curation, J.A.V.-C.; writing—original draft preparation, J.A.V-C, and C.F.-d.-l.-P; writing-review and editing, all authors.; visualization, all authors; supervision, J.A.V.-C.; project administration, C.F.-d.-l.-P.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cigarán-Méndez, M., Úbeda-D’Ocasar, E., Arias-Buría, J.L. et al. The hand grip force test as a measure of physical function in women with fibromyalgia. Sci Rep 12, 3414 (2022). https://doi.org/10.1038/s41598-022-07480-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-07480-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
