
Abstract
Nonalcoholic fatty liver disease (NAFLD) is an emerging cause of chronic liver diseases and a major health problem worldwide. Dietary patterns may play a critical role in controlling and preventing this disease, but the available evidence is scarce. The current study aims to ascertain the association of adherence to the Dietary Approach to Stop Hypertension (DASH) diet and Mediterranean diet (MeD) with nonalcoholic fatty liver disease (NAFLD) among Iranian adults of the Amol Cohort Study (AmolCS). In a cross-sectional analysis among 3220 adults (55.3% men), age ≥ 18 years (46.96 ± 14.67), we measured usual dietary intake with a validated food frequency questionnaire (FFQ) and then calculated dietary pattern scores for DASH and MeD. Sociodemographic and lifestyle factors were collected by a structured questionnaire. The presence and degree of NAFLD were also determined by abdominal sonography. Multiple regression models were used to estimate NAFLD odds across tertiles of DASH and Mediterranean dietary scores. Dietary DASH and Mediterranean components were adjusted for total energy intake, based on the residual methods. After adjusting for multiple potential confounders, we found an inverse association of DASH and MeD with NAFLD (Ptrend = 0.02, and Ptrend = 0.002, respectively). Those in the highest tertiles of adherence to the DASH and MeD had the lowest risk for NAFLD (OR = 0.80, 95%CI = 0.66–0.96, OR = 0.64, 95%CI = 0.52–0.78, respectively). The results of logistic analysis of MeD, stratified by gender and abdominal obesity, revealed the favorable association was more pronounced in women (OR = 0.42, 95%CI = 0.29–0.61, Ptrend = 0.004), and in participants with or without abdominal obesity (OR = 0.62, 95% CI = 0.47–0.81, Ptrend = 0.03, OR = 0.64, 95%CI = 0.475–0.91, Ptrend = 0.04, respectively). Similar results were obtained for the adherence to DASH diet score with the prevalence of NAFLD patients with abdominal obesity (OR = 0.75, 95% CI = 0.57–0.97, Ptrend = 0.04). The findings suggested the favorable association between DASH and MeD with NAFLD in Iranian adults, especially women and subjects with or without abdominal obesity. Further prospective investigations are needed to confirm the integrity of our findings.
Similar content being viewed by others
Introduction
Nonalcoholic fatty liver disease (NAFLD) is an emerging cause of chronic liver diseases and a major health problem worldwide1. Generally, NAFLD is a term used to describe a wide pathological spectrum, ranging from steatosis, steatohepatitis, steatonecrosis, and cirrhosis, resulting from fat accumulation in the liver2. Epidemiological data suggest that NAFLD prevalence is about 25%, ranging from 13% in Africa to 42% in Southeast Asia3. As a major health problem, NAFLD is a well-known risk factor of cardiovascular diseases and the leading cause of liver transplantation in men and the second in women4.
To date, researchers conducted an intensive study to understand NAFLD etiology better and seek the most effective dietary interventions for treatment. Given there is no consensus with respect to the pharmacological treatment of NAFLD, most therapeutic approaches focus on calorie restriction and physical activity to reach a gradual weight decline. For these reasons, dietary interventions remain the cornerstone of NAFLD management. Similarly, considering the role of diet composition to improve metabolic function is gaining increased attention5,6.
Food groups, food items, and individual nutrients are the components of dietary patterns and represent one of the key lifestyle factors involved in controlling and preventing NAFLD7. The Dietary Approaches to Stop Hypertension (DASH) diet is a healthful low-glycemic index and low-energy-dense diet initially designed to reduce hypertension8,9. This dietary pattern includes a wide variety of high-quality foods rich in antioxidants, magnesium, potassium, and dietary fiber and discourages red or processed meat, sugar, and sodium intakes10,11. In addition to antihypertensive effects, DASH diet is an effective approach for improving chronic diseases, including cardiovascular risks, diabetes, and metabolic syndrome12. Shirani et al., in a meta-analysis, reported that DASH diet score is associated with insulin sensitivity improvement, and some other studies posited that inflammatory markers reduction might be seen as a result of DASH diet adherence13.
The Mediterranean diet (MeD) is defined as a plant-based diet characterized by a high intake of fruits and vegetables, legumes, whole grains, and a high ratio of monounsaturated fatty acids (MUFA), which is associated with a lower risk of many chronic diseases2. Studies have suggested favorable health outcomes followed by adherence to this dietary pattern, including reducing NAFLD severity14. The EASL-EASD-EASO Clinical Practice Guidelines have recently recommended MeD as a dietary choice for NAFLD treatment, particularly through a reduction in insulin resistance and lipid serum concentrations. It can induce regression of steatosis, a significant reduction of cardiovascular events15. Despite the apparent benefits of the Mediterranean and DASH diet for Type 2 diabetes and cardiovascular disease16,17, the evidence for their efficacy in NAFLD is limited18.
Currently, the exact effects and composition of dietary patterns have not been clearly established, and most studies were conducted in Western populations. Indeed, different components of these two dietary patterns in Iranian people and Middle Eastern differ from Western countries19,20. Therefore, owing to the distinct lack of large-scale evidence from an Iranian population, the current study investigates the association of MeD and DASH patterns with NAFLD in a large-scale sample of Iranian adults who participated in the Amol Cohort Study (AmolCS).
Results
General characteristics of the study participants
Of the 3220 recruited in the cohort, 1437 (44.6%) had NAFLD, and 1438 (44.7%) were women. The mean age of participants was 46.96 ± 14.67 years, and all baseline characteristics are shown in Table 1. Anthropometry and metabolic traits were significantly different in NAFLD and non-NAFLD patients. Compared with men, women had a higher rate of BMI (body mass index), diabetes, metabolic syndrome, the use of lipid-lowering agents and hypertension-lowering agents, urban residency, total cholesterol, HDL, FBS, HbA1C, and a lower rate of waist circumstance, alcohol consumption, smoking, heart disease, physical activity level, triglyceride, AlT, AST, GGT (all p < 0.05).
The Characteristics of the study population across tertiles of DASH and MeD scores are provided in Table 2. Total energy intake was higher in the men compared to the women (2458 vs. 2171 kcal/day) (p < 0.05). After residual adjustment for energy intake, compared with men, women had higher DASH and lower Mediterranean diet scores (p < 0.05). According to the DASH component, women had a higher intake of vegetables and lower dairy products but lower red and processed meat and sweetened beverages (p < 0.05). According to the Mediterranean diet component, women had a higher intake of fruit and vegetables and a lower intake of poultry, total meat, and red meat. Also, non-NAFLD patients had a higher Mediterranean diet score compared to NAFLD cases (p < 0.05). Dietary component intakes of the participants across tertiles of dietary DASH score are shown in Supplementary Tables S1 and S2 online.
Association among dietary patterns and other factors with NAFLD
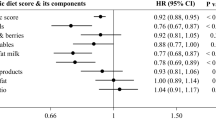
The risk of NAFLD (odds and 95% CI) in each tertile of DASH, as well as Mediterranean diet, score is shown in Table 3. In model 3, after adjusting for multiple potential confounders, we found an inverse association of adherence to DASH and Mediterranean diet with odds of NAFLD (OR = 0.80, 95% CI = 0.66–0.96, p for trend = 0.02; OR = 0.64, 95% CI = 0.52–0.78, p for trend = 0.002, respectively). After stratification for sex, these inverse associations of DASH and Mediterranean diet remained significant for women (OR = 0.72, 95% CI = 0.53–0.98, p for trend = 0.05; OR = 0.42, 95% CI = 0.29–0.61, p for trend = 0.004, respectively).
Table 4 presents the association of NAFLD risk with DASH and Mediterranean diet score stratified by abdominal and non-abdominal obesity. In model 3, after adjusting for all confounders, there was an inverse association between adherence to DASH diet score with the prevalence of NAFLD patients with abdominal obesity (OR = 0.75, 95% CI = 0.57–0.97, p for trend = 0.04). Similar results were obtained for Mediterranean diet score and prevalence NAFLD patients with or without abdominal obesity (OR = 0.62, 95% CI = 0.47–0.81, p for trend = 0.03; OR = 0.64, 95% CI = 0.475–0.91, p for trend = 0.04 respectively).
Discussion
The current study investigated the association of a priori defined DASH and MeD dietary patterns with NAFLD. This study contributes to furthering our understanding of the associations between diet and diseases in specific world regions, where social factors and dietary patterns may be distinctive. Indeed, the findings suggested that favorable adherence to healthful dietary patterns, including DASH and MeD, was inversely associated with NAFLD risk in Iranian adults.
Our findings are consistent with a cross-sectional analysis of a cohort study on 3051 Chinese adults aged 40–75 years, which revealed adherence to the DASH diet was independently associated with a lower prevalence of NAFLD21. A previous randomized controlled clinical trial in 60 overweight or obese Iranian adults with NAFLD revealed adherence to the DASH diet for 8 weeks, compared with the control diet, improved liver enzymes, and some NAFLD risk factors, including weight and serum triglycerides, and inflammatory and insulin resistance markers22.
In addition, the inverse association MeD on NAFLD in our study was concordant with other studies4,23,24. For example, a cohort study by Baratta et al. showed that adherence to MeD had a preventive effect on NAFLD (OR: 0.801, P = 0.018)25. Further, a meta-analysis including seven observational reports and six randomized clinical trials showed that adherence of MeD can significantly reduce BMI (effect size = − 1.23 kg/m2; 95% CI − 2.38 to − 0.09 kg/m2), weight (effect size = − 4.13 kg; 95% CI − 8.06 to − 0.20 kg), serum triglycerides (effect size = − 33.01 mg/dL; 95% CI − 52.84 to − 13.18 mg/dL), and total cholesterol (effect size = − 6.89 mg/dL; 95% CI − 14.90 to 1.12 mg/dL)26, which can theoretically translate to protective effects in NAFLD. Moreover, Kaliora et al., in a 24-week prospective diet intervention study on 44 NAFLD patients with simple steatosis, concluded that adherence to MeD improves liver imaging, liver fibrosis score, blood pressure, fasting glucose, HgA1C, and several other biomarkers, compared with pre-intervention values27.
Several mechanisms have been posited to contribute to the desirable effects of adherence to healthful dietary patterns, including MeD and DASH, on NAFLD, which consist mainly of higher intake of vegetables, fruits, plant-based proteins (nuts and legumes), whole-grain cereals, and micronutrients such as calcium, potassium, and vitamin C, dietary fiber, monounsaturated fatty acids, and omega-3 fatty acids, as well as polyphenols and other antioxidant agents28. Currently, strong evidence-based data supports the advantages of healthy dietary patterns in controlling most risk factors for NAFLD16; for instance, Dorosty et al. reported that consumption of whole grains for 12 weeks, independent of weight loss, beneficially affected liver enzymes concentrations, and fatty liver in patients with NAFLD29. Based on the observed benefits of the MeD components on NAFLD in our study, non-NAFLD individuals had a greater intake of MUFA/SFA and lower intake of animal protein sources (red meats and poultry) than those with NAFLD. Current evidence-based data also suggests a positive association between consumption of red meats and chicken, rather than marine animals, with hepatic status in obese subjects30.
Regarding the possible mechanism associated with a MeD and NAFLD, its effect on improving cardiometabolic outcomes (such as reducing triglycerides or fasting plasma glucose)31 or the antioxidant properties32 of healthy diets can be pointed to. On the other hand, the American Heart Association recommendations, which emphasize healthy dietary patterns such as the DASH or MeD, rather than specific food items, can be referred to33.
According to our findings, the favorable association of DASH and MeD was more pronounced in women and especially subjects with abdominal obesity. After adjusting for multiple confounders in subjects without abdominal obesity, adherence to MeD was also inversely related to NAFLD. The rationale for why the relationship was significant only among women could be attributed to an increased willingness to adopt a healthy diet. In our study, female participants, compared to males, independent of energy intake, had a greater consumption of fruits, vegetables, and lower dairy products, animal protein, and sweetened beverages.
In the current study, adherence to DASH and the Mediterranean diet was inversely associated with NAFLD prevalence in patients with abdominal obesity. Indeed, a similar result remained for MeD and NAFLD patients without abdominal obesity as well. This result suggests that MeD might represent a better choice for NAFLD management, as reported by evidence26.
Although we present a novel addition to the literature, the present study has some limitations. The main limitation of this study is the lack of a liver biopsy as the gold standard to assess the extent of liver damage in NAFLD, which could not be performed on the outpatients, as well as the cross-sectional nature of the study which precludes causal inferences being made. Moreover, recall bias and measurement error related to assessing food intake using validated FFQ cannot be easily ruled out in our study. Further, possible residual effects due to incomplete adjustment for remaining confounders may have affected the outcome variables. Furthermore, since some of the NAFLD participants may have already adopted healthy lifestyles, following physician advice may lead to achieving a high dietary pattern score among patients. However, this tendency may contribute to the unfavorable association between healthy dietary patterns and NAFLD, and we still observed an inverse relationship in our study. Finally, our study population was comprised solely of adults of the north of Iran; therefore, the extrapolation of our findings to all Iranian adults must be made cautiously.
Conclusion
The findings of our study suggested a favorable association between the adherence to DASH and MeD with NAFLD in Iranian adults, especially women and subjects with or without abdominal obesity. However, further prospective investigations are needed to confirm the veracity of this suggestion.
Methods
Study population
This is a population-based cross-sectional study, and participants were drawn from the second phase of AmolCS. A comprehensive data collection was done in two different phases, including 2009–2010 (phase 1) and 2016–2017 (phase 2). A multistage sampling technique was applied. All twenty-five rural and sixteen urban health centers of Amol city, north of Iran, were the source of the sampling frame of the study. Sixteen strata with 10 years intervals including 10–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80–89 years of age were selected. The random selection of study subjects in each stratum was conducted proportionally to the population size. Participants with excessive alcohol consumption of more than 30 g/d for men and more than 20 g/d for women, viral hepatitis, and those on medication known to cause fatty liver, weight loss, or weight gain in the last 3 months before sonography (n 486) and pregnancy/lactation (n 153) were excluded.
Laboratory, anthropometric, and demographic variables were comprehensively were collected in each phase26. An informed consent form was obtained from all participants before the study, and the study protocol was approved by the Iran University of Medical Sciences ethics committee.
After excluding subjects with missing data for abdominal ultrasonography (n 166), covariates (n 186), and food frequency questionnaire (n 249), as well as misreporting energy intake (n 228), ultimately, 3220 subjects, including 1438 women and 1782 men, were analyzed in the study (Fig. 1). Excluded subjects had a comparable socioeconomic level as those who remained in the study.

Flowchart of the study design.
Dietary assessment
Recruited patients answered a 168-items semi-quantitative food frequency questionnaire adapted to the Iranian society to assess usual dietary intake34. Participants reported their average frequency of each food item on the previous year per day, week, month, and year, or never. The reported portion size and frequency of food intake were converted to daily intake, and the portion size was converted to grams by household measures35. Nutrient and energy intake were calculated by the US Department of Agriculture (USDA) Food Composition Table (FCT)36 because the Iranian FCT is incomplete. The Iranian FCT was used alternatively for traditional foods not listed in the USDA FCT37.
Creation of dietary scores
We followed the methodology of Fung et al. to calculate DASH dietary scores38. Accordingly, we constructed a DASH score based on eight components emphasized or minimized in the DASH diet, and each of them was placed into quintiles. One point was allocated for receiving fruits, vegetables, low-fat dairy products, whole grains, nuts, and legumes at the highest quintile, and for the remaining components (intake of sodium, soft drink or sweet beverage, red or processed meats), low intakes were desirable.
MeD Score was calculated based on the Trichopoulou et al. methodology by taking into account the consumption of nine food groups. Whether the participants' adherence to each MeD component they received a score of 0 or 139. Daily servings of fruits, vegetables, whole grain, nuts, legumes ratio of grams of MUFA to saturated fatty acids (SFA) equivalent to, or greater than, the median intake of the study population, and also daily servings of dairy products and meat poultry, red and processed) less than the median intake of the study population received one point.
Residual method energy adjustment was conducted for all food groups before the score ranking. Finally, participants were categorized into tertiles based on their MeD scores.
Abdominal ultrasonography
Sonography was used for NAFLD, and it was defined as hepatic steatosis after the exclusion of secondary causes of fat build-up in the liver (e.g., drug-related steatosis, excess alcohol consumption, and viral hepatitis). One expert sonographer performed all ultrasound examinations and was blind and not involved in any of the cohort procedures. Sagittal, longitudinal, lateral, and intercostal views were provided through a 3–5 MHz transducer. Similarly, related criteria for fatty liver confirmation included blurring of portal or hepatic veins plus a marked increase in hepatic echogenicity.
Laboratory and anthropometric assessments
Serum collected from 2016 to 2017 was applied to the measurement of all laboratory tests. Blood samples were drawn after overnight fasting, and serum obtained from whole blood was used for biochemical analyses using an automatic BS-200 chemistry analyzer (Mindray, China). After whole blood samples incubation at room temperature, they were centrifuged at 3000 rpm for 10 min. Laboratory parameters included; fasting blood sugar (FBS), HDL, TG, total cholesterol, liver enzymes (alanine aminotransferase, aspartate aminotransferase, gamma-glutamyl transferase), CRP, hepatitis B virus surface antigens, and hepatitis C virus antibodies.
After 5 min in a quiet place, participants' blood pressure was measured in a seated position, using a manual sphygmomanometer. Properly fitted cuffs and calibrated monitors were used. Korotkoff noise appearance and disappearance were considered as systolic and diastolic values, respectively. The mean value of the two measurements was taken. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure was used for hypertension evaluation40. Weight and height were measured with participants in minimal clothing, and waist circumference (WC) was also measured based on WHO protocols41.
Statistical analysis
Data were presented as means and standard deviations for continuous variables and frequencies and percentages for categorical ones. The Kolmogorov–Smirnov test and histogram were applied to ensure the normal distribution of variables. Differences between qualitative variables were evaluated by the Chi-square test. Independent t-test and one-way analysis of variance (ANOVA) were applied to determine differences between continuous variables in two and more than two groups, respectively. A univariate analysis was performed for potential confounding variables; variables with PE < 0.2 in the univariate analyses were selected for the final multivariable models; PE (P-value for entry) determines which variables should be included in the multivariable model. Statistical analysis was performed using SPSS 24, and results were, a priori, considered significant at P values < 0.05.
We used multiple regression models to estimate NAFLD risk across tertiles of DASH and Mediterranean dietary scores. The associations of DASH and Mediterranean dietary patterns with NAFLD were adjusted for sex, age, BMI, energy intake, smoking status, physical activity, lowering serum lipid drugs, lowering HPTN drugs, lowering serum glucose drugs, residual areas, heart disease, and diabetes. Dietary DASH and Mediterranean components were adjusted for total energy intake, based on the residual methods (22), such that participants' dietary DASH and Mediterranean scores were residually adjusted for energy intake. A linear trend test was performed, considering each ordinal score variable as a continuous variable in the model. To assess the overall trends of odds ratios of NAFLD across tertiles of dietary DASH and Mediterranean diet score, the median of each tertile was used as a continuous variable in the logistic regression models.
Ethical standards disclosure
The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and procedures involving human subjects/patients were approved by the Iran University of Medical Sciences (IUMS) ethical committee (No.IR.IUMS.REC.1399.1393). Written informed consent was obtained from all participants prior the study.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Younossi, Z. M. et al. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64, 73–84 (2016).
Bach-Faig, A. et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 14, 2274–2284 (2011).
Li, J. et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 4, 389–398 (2019).
Baratta, F. et al. Nonalcoholic fatty liver disease and fibrosis associated with increased risk of cardiovascular events in a prospective study. Clin. Gastroenterol. Hepatol. 18, 2324-2331.e2324 (2020).
Sohouli, M. H. & Lari, A. The association between polyphenols intake and odds of non-alcoholic fatty liver disease (NAFLD) among adult population. Int. J. Nutr. Sci. 5, 122–129 (2020).
Berná, G. & Romero-Gomez, M. The role of nutrition in non-alcoholic fatty liver disease: Pathophysiology and management. Liver Int. 40, 102–108 (2020).
Carneros, D., López-Lluch, G. & Bustos, M. Physiopathology of lifestyle interventions in non-alcoholic fatty liver disease (NAFLD). Nutrients 12, 3472 (2020).
Sacks, F. M. et al. Effects on blood pressure of reduced dietary sodium and the dietary approaches to stop hypertension (DASH) diet. N. Engl. J. Med. 344, 3–10 (2001).
Parikh, A., Lipsitz, S. R. & Natarajan, S. Association between a DASH-like diet and mortality in adults with hypertension: Findings from a population-based follow-up study. Am. J. Hypertens. 22, 409–416 (2009).
Farhadnejad, H. et al. The association of Dietary Approach to Stop Hypertension (DASH) diet with metabolic healthy and metabolic unhealthy obesity phenotypes. Sci. Rep. 9, 1–7 (2019).
Soltani, S., Arablou, T., Jayedi, A. & Salehi-Abargouei, A. Adherence to the dietary approaches to stop hypertension (DASH) diet in relation to all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective cohort studies. Nutr. J. 19, 1–13 (2020).
Karamali, M., Bahramimoghadam, S., Sharifzadeh, F. & Asemi, Z. Magnesium–zinc–calcium–vitamin D co-supplementation improves glycemic control and markers of cardiometabolic risk in gestational diabetes: A randomized, double-blind, placebo-controlled trial. Appl. Physiol. Nutr. Metab. 43, 565–570 (2018).
Pirozeh, R. et al. Effect of DASH diet on oxidative stress parameters: A systematic review and meta-analysis of randomized clinical trials. Diabetes Metab. Syndr. Clin. Res. Rev. 14, 2131–2138 (2020).
Franco, I. et al. Physical activity and low glycemic index Mediterranean diet: Main and modification effects on NAFLD score. Results from a randomized clinical trial. Nutrients 13, 66 (2021).
Plaz Torres, M. C. et al. Mediterranean diet and NAFLD: What we know and questions that still need to be answered. Nutrients 11, 2971 (2019).
Chiavaroli, L. et al. DASH dietary pattern and cardiometabolic outcomes: An umbrella review of systematic reviews and meta-analyses. Nutrients 11, 338 (2019).
De la Iglesia, R. et al. Dietary strategies implicated in the prevention and treatment of metabolic syndrome. Int. J. Mol. Sci. 17, 1877 (2016).
Hekmatdoost, A. et al. Adherence to the dietary approaches to stop hypertension (DASH) and risk of nonalcoholic fatty liver disease. Int. J. Food Sci. Nutr. 67, 1024–1029 (2016).
Watzinger, C. et al. Dietary factors in relation to liver fat content: A cross-sectional study. Nutrients 12, 825 (2020).
Kouvari, M. et al. Mediterranean diet is inversely associated with steatosis and fibrosis and decreases ten-year diabetes and cardiovascular risk in NAFLD subjects: Results from the ATTICA prospective cohort study. Clin. Nutr. 40, 3314–3324 (2021).
Xiao, M.-L. et al. Adherence to the Dietary Approaches to Stop Hypertension (DASH) diet is associated with lower presence of non-alcoholic fatty liver disease in middle-aged and elderly adults. Public Health Nutr. 23, 674–682 (2020).
Razavi Zade, M. et al. The effects of DASH diet on weight loss and metabolic status in adults with non-alcoholic fatty liver disease: A randomized clinical trial. Liver Int. 36, 563–571 (2016).
Sofi, F. & Casini, A. Mediterranean diet and non-alcoholic fatty liver disease: New therapeutic option around the corner?. World J. Gastroenterol. 20, 7339 (2014).
Trovato, F. M., Catalano, D., Martines, G. F., Pace, P. & Trovato, G. M. Mediterranean diet and non-alcoholic fatty liver disease: The need of extended and comprehensive interventions. Clin. Nutr. 34, 86–88 (2015).
Baratta, F. et al. Adherence to mediterranean diet and non-alcoholic fatty liver disease: Effect on insulin resistance. Off. J. Am. Coll. Gastroenterol. 112, 1832–1839 (2017).
Akhlaghi, M., Ghasemi-Nasab, M. & Riasatian, M. Mediterranean diet for patients with non-alcoholic fatty liver disease, a systematic review and meta-analysis of observational and clinical investigations. J. Diabetes Metab. Disord. 19, 575–584 (2020).
Kaliora, A. C. et al. The effectiveness of Mediterranean diet in nonalcoholic fatty liver disease clinical course: An intervention study. J. Med. Food 22, 729–740 (2019).
George, E. S. et al. Practical dietary recommendations for the prevention and management of nonalcoholic fatty liver disease in adults. Adv. Nutr. 9, 30–40 (2018).
Dorosti, M., Heidarloo, A. J., Bakhshimoghaddam, F. & Alizadeh, M. Whole-grain consumption and its effects on hepatic steatosis and liver enzymes in patients with non-alcoholic fatty liver disease: A randomised controlled clinical trial. Br. J. Nutr. 123, 328–336 (2020).
Recaredo, G. et al. Association between different animal protein sources and liver status in obese subjects with non-alcoholic fatty liver disease: Fatty Liver in Obesity (FLiO) Study. Nutrients 11, 2359 (2019).
Garcia, M. et al. The effect of the traditional Mediterranean-style diet on metabolic risk factors: A meta-analysis. Nutrients 8, 168 (2016).
Zamora-Ros, R. et al. Mediterranean diet and non enzymatic antioxidant capacity in the PREDIMED study: Evidence for a mechanism of antioxidant tuning. Nutr. Metab. Cardiovasc. Dis. 23, 1167–1174 (2013).
Eckel, R. H. et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 63, 2960–2984 (2014).
Mirmiran, P., Esfahani, F. H., Mehrabi, Y., Hedayati, M. & Azizi, F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 13, 654–662 (2010).
Ghaffarpour, M., Houshiar-Rad, A. & Kianfar, H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran Nashre Olume Keshavarzy 7, 42–58 (1999).
Fagherazzi, G. et al. Dietary acid load and risk of type 2 diabetes: The E3N-EPIC cohort study. Diabetologia 57, 313–320 (2014).
Kiefte-de Jong, J. C. et al. Diet-dependent acid load and type 2 diabetes: Pooled results from three prospective cohort studies. Diabetologia 60, 270–279 (2017).
Fung, T. T. et al. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 168, 713–720 (2008).
Trichopoulou, A., Costacou, T., Bamia, C. & Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 348, 2599–2608. https://doi.org/10.1056/NEJMoa025039 (2003).
Chobanian, A. V. et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 42, 1206–1252. https://doi.org/10.1161/01.HYP.0000107251.49515.c2 (2003).
WHO. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008. Geneva, Switzerland: World Health Organization, 2011. http://www.who.int/iris/handle/10665/44583 (2018).
Acknowledgements
We greatly appreciate the participants, healthcare executives in public health centers in Amol and, the GILDRC staff (http://www.gildrc.ac.ir), without whom the study would not have been possible.
Funding
This research was conducted by a grant from the Gastrointestinal and liver Diseases Research Center (GILDRC), Iran University of Medical Sciences (IUMS) (Grant No: 99–2-30–19054).
Author information
Authors and Affiliations
Contributions
F.Z., E.S., H.A., M.R.M., and A.D. were responsible for the study concept and design. A.D. and N.M. had full access to all data and took responsibility for the integrity of the data and the accuracy of the data analysis. M.M., and M.N. were involved in data collection. A.D., N.M., C.C., and SE analyzed and interpreted the data. N.A.H., S.E. and M.N. wrote the initial draft of the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final manuscript. F.Z. is the guarantor and takes responsibility for the paper as a whole.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Doustmohammadian, A., Clark, C.C.T., Maadi, M. et al. Favorable association between Mediterranean diet (MeD) and DASH with NAFLD among Iranian adults of the Amol Cohort Study (AmolCS). Sci Rep 12, 2131 (2022). https://doi.org/10.1038/s41598-022-06035-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-06035-8
This article is cited by
-
Dietary approaches to stop hypertension (DASH) diet improves hepatic fibrosis, steatosis and liver enzymes in patients with non-alcoholic fatty liver disease: a randomized controlled trial
European Journal of Nutrition (2024)
-
Dairy products intake and prevalence, incidence, and recovery of non-alcoholic fatty liver disease in Chinese population
Hepatology International (2024)
-
The effect of DASH diet on glycemic response, meta-inflammation and serum LPS in obese patients with NAFLD: a double-blind controlled randomized clinical trial
Nutrition & Metabolism (2023)
-
Associations between an inflammatory diet index and severe non-alcoholic fatty liver disease: a prospective study of 171,544 UK Biobank participants
BMC Medicine (2023)
-
Association between adherence to the Dietary Approaches to Stop Hypertension diet and serum uric acid
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
