
Abstract
Increased prevalence of sleep disorders has been found in patients with functional dyspepsia; however, direction of causality remains unclear. Our aim was to compare the risk of incident functional dyspepsia between patients with and without sleep disturbance from a large population-based sample. Utilizing a nation-wide health insurance administrative dataset, we assembled an 11-year historic cohort study to compare subsequent incidence of diagnosed functional dyspepsia between adult patients with any diagnosis of sleep disturbance and age- and gender-matched controls. Hazard ratios adjusted for other relevant comorbidities and medications were calculated using Cox regression models. 45,310 patients with sleep disorder and 90,620 controls were compared. Patients with sleep apnea had a 3.3-fold (95% confidence interval: 2.82 ~ 3.89) increased hazard of functional dyspepsia compared with controls. This increased risk persisted regardless of previously diagnosed depression coexisted. Sleep disturbance was associated with an increased risk of subsequent functional dyspepsia. Potential mechanisms are discussed.
Similar content being viewed by others


Introduction
It is estimated that over 20% of the general population have sleep problems, and more than 8% suffer from chronic sleep disturbance1,2. Sleep disturbance can be categorized into insomnia, or sleep disorders such as intrinsic or extrinsic dyssomnias, and parasomnias3 and have been found to be associated with a wide range of impairments in physical and mental health, as well as in social and emotional function1,4. Associations described with physical disorders have included diabetes5, cardiovascular diseases4, and impaired liver function6,7, although these have focused on moderate or severe sleep apnea rather than wider sleep disturbance.
Functional dyspepsia, affecting about 20% of the population8, is a common gastrointestinal disorder with symptoms of bothersome postprandial fullness, early satiation, epigastric pain, or gastric burning for the last 3 months without evidence of metabolic or structural diseases9. Previous research has suggested disrupted sleep quality in patients with dyspepsia compared to healthy controls, with published odds ratios ranging from 1.7 to 3.410,11,12,13,14. However, some studies have not found this association15 and others have found sleep apnea to be associated with irritable bowel syndrome rather than dyspepsia16,17,18. In addition, most research in this area has involved cross-sectional or case–control designs, providing limited information on the direction of causality.
We therefore aimed to compare the prospective risk of functional dyspepsia between patients with and without diagnosed sleep disturbance using a nationwide database of health service utilization. Interactions of depression and incident dyspepsia were also investigated to clarify further the association of interest.
Results
Comparisons of characteristics in patients with or without sleep disturbances
Table 1 compares demographic characteristics, comorbidities, and medications between the 36,044 patients identified with sleep disturbance (758 apnea, 35,286 non-apnea) and the 66,768 matched controls. The mean age of the sleep disturbance cohort was 52.2 years, and that of the control cohort was 52.0 years. Among those with sleep disturbance, the mean age of those in the apnea subgroup were slightly younger, with more than half under 50 years of age. Males predominated in the apnea subgroup, and females in the non-apnea subgroup. Compared with the control cohort, comorbidities and medications of interest were more common in the sleep disturbance cohort. Mean follow-up durations were 9.76, 9.16 and 9.71 years for the apnea subgroup, non-apnea subgroup, and control cohorts, respectively.
Cumulative incidences of dyspepsia in patients with or without sleep disturbances
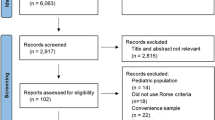
As indicated in Fig. 1, the cumulative incidence of dyspepsia in patients with sleep disturbance was approximately 10.5% higher than that in matched controls (log-rank test p < 0.001). The overall incidence density of dyspepsia was significantly higher in both the apnea and non-apnea subgroups compared to the control cohort (18.9, 210, and 6.73 instances per 1000 person-years, respectively (Table 2)).

Kaplan-Meir method determined cumulative incidence of Dyspepsia compared between sleep disorder cohorts and comparisons without sleep disorder.
Risks of dyspepsia in patients with or without sleep disturbances stratified by comorbidities
Hazard ratios were significantly elevated for both sleep disorder groups within almost all strata (age, gender, most comorbidities, and with or without sleeping pills) after adjustment (Table 2). Only patients with sleep apnea comorbid with depression, obesity, heart failure, and no benzodiazepine (BZD) use did not have significantly elevated risks of dyspepsia.
Risks of dyspepsia by subtypes of sleep disorders
Significantly higher risks of dyspepsia were also found for all subtypes of non-apnea disturbance compared to controls (Table 3). Our sensitivity analysis, excluding incident dyspepsia within the 12 months after the index date, supported the robustness of our primary finding.
Further analyses on risks of dyspepsia categorized by sleep disturbances and comorbidities
Patients with both sleep disorder and depression had the highest risk of dyspepsia (aHR 5.38, 95% CI 4.93 ~ 5.88), while non-depressed patients with sleep disorder still exhibited a significantly elevated risk of developing dyspepsia (aHR 4.07, 95% CI 3.92 ~ 4.24) (Table 4). Patients that had both sleep disturbance and obesity, heart failure, or no BZD use had higher risks of functional dyspepsia than those with comorbidities but without sleep disturbance (Table 4).
Discussion
To our knowledge, this is the first study to investigate the risk of functional dyspepsia associated with sleep disturbances, taking advantage of a population-based dataset derived from a universal health insurance system. We found that risks of functional dyspepsia were significantly higher in patients with sleep disturbances, and that this applied to both the apnea and non-apnea subgroups. These associations remained significantly elevated, following a variety of adjustments and stratifications for demographic factors, comorbidities, and medication use. Further analysis showed that this risk was most elevated in the subgroup of patients with both sleep and depressive disorders.
The associations of interest are consistent with previous cross-sectional and case control studies reporting disrupted or impaired quality of sleep among patients with dyspepsia11,14,19,20,21. However, some studies have suggested stronger associations of dyspepsia with irritable bowel syndrome rather than functional dyspepsia16,17,18 which we did not specifically investigate and would need further research. Our findings help to infer the direction of causation through the prospective design, although the opposite direction of causation (dyspepsia causing sleep disturbance) might also co-explain the cross-sectional relationship and would again need further specific investigation. It is possible that some cases of dyspepsia predate the onset of sleep disturbance despite being diagnosed later; however, this would predict an early divergence in incidence rates that was not sustained over follow-up; this is not apparent in the analysis of cumulative incidence displayed in Fig. 1.
Causal pathways between sleep disturbance and functional dyspepsia remain unclear, but plausible mechanisms include the chronic effects of sleep disturbance on gastrointestinal functions, including hypersensitivity to physiological stimuli, dysfunctions in autonomic nervous regulation, and/or alterations in neuroendocrine responses20,22. These will be considered and discussed in the following paragraphs.
First, visceral sensitivity may be altered due to disruptions of circadian rhythm in patients with sleep disturbances resulting in unpleasant abdominal sensations11,12,13,16,23. For example, Zhen et al. described bowel disturbances being significantly higher in rotating shift nurses compared to regular day nurses and that bowel symptom scores correlated with sleep disturbances positively24. Previous research has also shown that disruption of Stage 4 or slow-wave (deep) sleep, or the loss of rapid eye movement (REM) sleep, results in hyperalgesia or emergence of abdominal symptoms, such as nausea or cramping in healthy volunteers15,25,26,27, and in patients with functional dyspepsia12 or gastroesophageal reflux disease28. In addition, poor sleep quality (i.e. increased awakenings or altered sleep stages) has been found to be associated with gastrointestinal symptoms the next day among women with irritable bowel syndrome29,30. Other clinical studies have found that melatonin is helpful in reducing pain symptoms of irritable bowel syndrome without affecting colonic motility, and have suggested that this might be due to the restoration of circadian rhythms16,31. Although the focus has been more on irritable bowel syndrome than dyspepsia, it is plausible that adverse effects of poor sleep may influence both upper and lower gastrointestinal tracts10 and that routine clinical diagnoses obtained from administrative databases may overlap across the two conditions.
Second, gastric motility might be affected by autonomic dysregulation due to reduced sleep efficiency or increased proportions of REM sleep and intrusions during non-REM sleep10,18,20,32. These changes may indicate more nocturnal autonomic arousals20,33 with similar autonomic effects to waking20, as evidenced by increased sympathetic activity20, elevated cortisol and adrenocorticotropic hormone, or diminished vagal output33, leading to decreased migrating motor complexes in the duodenum19. However, since previous research has only described self-reported gastrointestinal discomfort after poor sleep on the preceding night10,19,20,29, direct evidence is lacking on whether long-term dysregulation of the autonomic nervous system during sleep might induce visceral motor abnormalities leading to dyspepsia34.
Third, sleep disturbance has been found to be associated with alterations in brain regions such as the raphe nuclei, implicated in the release of serotonin, and regulation of circadian rhythm35, or the locus coeruleus, implicated in noradrenergic mediated physiological responses to stress and arousal20,36. These brain regions also receive afferent neuroendocrine signals from the enteric nervous system mediated by ascending serotonergic, cholinergic, or noradrenergic pathyways20, as well as having descending projections that terminate in the dorsal horn to regulate pain sensations. As a neurotransmitter in descending myenteric interneurons, serotonin is responsible for enhancing acetylcholine and calcitonin gene-related peptide release in prokinetic pathways37. Interference with such pathways might block the initiation of reflexes within the enteric nervous system and affect gut motility. However, over-stimulation of such pathways would also cause hypersensitivity and bowel discomfort such as nausea, pain, or bloating.
Previous literature on dyspepsia has suggested that comorbidities from other organ systems and possible underlying psychological problems, such as social stressors or depression should be considered as etiological factors14,21,38,39. Our findings that the risk of dyspepsia was significantly higher in the sleep disorder groups within almost all comorbidities indicated that, in patients with comorbidities from multiple systems, having sleep disturbance is still key to the risk of their dyspepsia. Our findings of significant associations with sleep disturbance in both people with and without previous diagnoses of depression support the importance of including sleep disturbance alone in considering the etiology of dyspepsia, in addition to the other stressors. The risk of dyspepsia was not as significantly elevated in patients without sleep disturbance, and with only obesity, heart failure, or no BZD use implying that the risk of dyspepsia was influenced much by sleep disturbance than the other conditions. Although further elucidation of underlying mechanisms is still needed, we believe the chronic direct/indirect gastrointestinal effects of sleep disturbance may be implicated, including hypersensitivity to physiological stimuli, and/or dysfunctions in autonomic nervous regulation, and/or alterations in neuroendocrine responses.
Major strengths of this study included the use of a population-based dataset large enough to detect the association of interest, as well as the cohort design with a long observation period, and exposure/outcome measures derived from recorded clinical diagnoses rather than screening instruments. However, there are key limitations which need to be considered in interpreting the findings. First, measurement of comorbid physical disorders was limited to those for which ICD-9-CM codes had been listed, since these diagnoses and records were obtained from a database set up for insurance claims rather than for research purposes (although it is important to bear in mind that recorded diagnoses are required to justify treatments received). The diagnoses were clinician- assigned and might not generalize to research diagnoses. We therefore deliberately chose relatively broad and unambiguous diagnostic groups. Second, although we had access to abundant data on medical service utilizations, information was not present on certain other risk factors associated with dyspepsia, such as dietary habits, smoking40, body mass index10,41, and psychosocial stressors39. There were therefore still some residual confounders and some potential causal pathways that we were not able to explore. Third, the accuracy of the recorded diagnosis of functional dyspepsia needs to be considered, particularly when minor gastrointestinal sensations might be amplified by comorbid mental health conditions. Nevertheless, as we mentioned earlier, all insurance claims from the NHI are scrutinized on a regular basis according to the standardized diagnostic criteria in this study. Although our current study has compensating advantages of naturalistic observations from clinical environment, with regards to the above deficiencies, further well-designed long-term cohorts with diagnoses established by diagnostic interviews or laboratory examinations may help overcome these limitations.
Conclusions
Using a large, population-based dataset, we found a raised risk of functional dyspepsia in patients with sleep disturbance, both for apnea and non-apnea subgroups. Underlying mechanisms still need further investigation; however, our findings do indicate that sleep disturbance should be identified more systematically and clinical advice/management considered to reduce the risk of functional gastrointestinal disorders.
Methods
Data source
Data were analysed from the Longitudinal Health Insurance Database 2000 (LHID 2000), a cohort of one million people (approximately 4.4% of the total population) randomly selected from the Taiwan National Health Insurance Database (NHIRD) from 2000 to 2011.The age and gender distributions of the LHID are not significantly different from Taiwan’s population of 23.75 million42. The NHIRD contains and encrypts all healthcare claim data, including diagnostic codes, medical institutions, outpatient and inpatient orders, prescriptions, and expenditures for healthcare from Taiwan’s National Health Insurance (NHI) program launched in 1995: a single-payer insurance program with near-universal coverage of more than 99% of Taiwan’s residents42. Personal information in NHIRD cannot be identified after encryption, and use of the NHIRD must be authorized and audited by the Taiwan Bureau of NHI. Diagnoses are coded by physicians according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and are reviewed by the NHI Review Committee every three months to audit the appropriateness of diagnoses and treatments claimed by clinicians. Related to our study, the accuracy and validity of gastrointestinal or ulcer-related diagnoses from the NHIRD have been found to be acceptable when comparing to diagnoses from the medical charts43. The study described here was approved by the Institutional Review Board of China Medical University in central Taiwan (CMUH-104-REC2-115). All methods were carried out in accordance with relevant regulations and guidelines. Due to the anonymity of the NHIRD, informed consent is not required from patients providing data.
Sample ascertainment
For our study cohort, we identified two groups of patients newly diagnosed with sleep disturbances (ICD-9-CM 780.5X), including insomnia or hypersomnia with sleep apnea (780.51, 780.53, 780.57), and non-apnea sleep disorders (307.4X and 780.5X, excluding 780.51, 780.53, and 780.57) between 1998 and 2001. The non-apnea subgroup was further divided into 3 groups: insomnia (780.52), sleep disturbance (780.5X, excluding 780.51, 780.53, and 780.57), and others (sleep disorders or difficulty initiating or maintaining sleep: 307.4; sleep disturbances: 780.50, 780.58 ~ 780.59; other hypersomnia: 780.54; disruptions of sleep–wake cycle: 780.55; or dysfunctions of sleep stages or arousal from sleep: 780.56). The date of the first diagnosis of any of the above sleep disturbances was defined as the index date. Patients with multiple diagnoses of sleep disturbance were included once and assigned to the first index date. Patients with a recorded diagnosis of dyspepsia (536.8) before the index date or for whom age or sex information was incomplete were excluded. The control cohort patients (those without sleep disturbances) were randomly selected from the LHID 2000 and were matched with sleep disturbance cohort patients by age (± 5 years range), gender, and index year on a 1:2 ratio, applying the same exclusion criteria. All exposed and control patients were followed from the index date until the date of receiving a diagnosis of functional dyspepsia, withdrawal from the NHI program, or the end of 2011.
Outcome and covariates
The primary outcome of our study was dyspepsia (536.8) incorporated from inpatient and outpatient records. Such diagnosis of functional dyspepsia was made by clinicians according to the Rome III and IV criteria: i.e., defining dyspepsia as any combination of four symptoms, including postprandial fullness, early satiety, epigastric pain, and epigastric burning severe enough to affect daily activities and lasted at least 3 days per week over 3 months; with an onset of 6 months in advance. The following baseline recorded diagnoses prior to the index date were also ascertained as comorbidities potentially associated with both sleep disturbance and functional dyspepsia: diabetes (250.XX), hypertension (401.XX ~ 405.XX), hyperlipidemia (272.XX), anxiety (300.00), depression (296.2X ~ 296.3X, 300.4X, 311.XX), cholecystitis (575.XX), cholelithiasis and other disorders of biliary tract (574.XX, 576.XX)9, alcoholism (291.XX, 303.XX, 305.00, 305.01, 305.02, 305.03, 790.3X and V11.3)44, stroke (430.XX ~ 438.XX), ischemic heart disease (410.XX ~ 414.XX), heart failure (428.XX), atrial fibrillation (427.31), chronic kidney disease (CKD) (580.XX ~ 589.XX), chronic obstructive pulmonary disease (COPD) (491.XX, 492.XX, 496.XX), asthma (493.XX), fatigue (780.79), and obesity (278.XX). For inclusion eligibility (as independent or dependent variables or covariates), any disease diagnosis needed to appear in at least three outpatient visits or one hospitalization. Medication that might be associated with both sleep and dyspepsia was also extracted, namely: benzodiazepines (BZD), zolpidem, aspirin, non-steroidal anti-inflammatory drugs (NSAIDs)45, steroids, proton pump inhibitors, and h2-receptor antagonists.
Statistical analysis
Demographic and clinical characteristics of patients with sleep disturbance diagnoses (apnea subgroup and non-apnea subgroup) and controls were compared using chi-squared tests for categorical variables, and student’s t-tests for continuous variables. We computed the incidence rate (per 1000 person-years) of dyspepsia for each cohort. Cox proportional hazards models were used to assess the risk of subsequent dyspepsia associated with exposure status, and hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated. Multivariate models were used to adjust for age, sex, comorbidities, and medication. We also compared the cumulative incidence of dyspepsia between the exposed and control cohorts using the Kaplan–Meier method, and tested their differences by log-rank tests. Additive interactions between comorbidities and sleep disturbance as exposures were also explored. Finally, to reduce the influence of undiagnosed dyspepsia occurring prior to sleep disturbance, a sensitivity analysis excluded dyspepsia in the 12 months after index date. All statistical analyses were performed using SAS (Version 9.3; SAS Institute, Cary, NC, USA) and the significance level was set at 0.05 for two-tailed tests.
Data availability
Datasets being analyzed and results being generated and reported in this article can be obtained from the National Health Research Institute of the Ministry of Health and Welfare in Taiwan. Restrictions applied to these data, which were used under license for our study, and so are not publicly available for duplication. Data can be requested only from the Ministry of Health and Welfare.
References
Fernandez-Mendoza, J. & Vgontzas, A. N. Insomnia and its impact on physical and mental health. Curr. Psychiatry Rep. 15(12), 8 (2013).
Ohayon, M. M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 6(2), 15 (2002).
Schillinger, E., Kushida, C., Fahrenbach, R., Dement, W. & LeBaron, S. Teaching family medicine medical students about sleep disorders. Fam. Med. 35(8), 3 (2003).
Sofi, F. et al. Insomnia and risk of cardiovascular disease: A meta-analysis. Eur. J. Prev. Cardiol. 21(1), 8 (2014).
Morgenstern, M. et al. Obstructive sleep apnea: An unexpected cause of insulin resistance and diabetes. Endocrinol. Metab. Clin. North Am. 43(1), 18 (2014).
Ahmed, M. H. & Byrne, C. D. Obstructive sleep apnea syndrome and fatty liver: Association or causal link?. World J. Gastroenterol. 16(34), 10 (2010).
Tanné, F. et al. Chronic liver injury during obstructive sleep apnea. Hepatology 41(6), 7 (2005).
Zagari, R. M. et al. Epidemiology of functional dyspepsia and subgroups in the Italian general population: An endoscopic study. Gastroenterology 138(4), 1302–1311. https://doi.org/10.1053/j.gastro.2009.12.057 (2010).
Drossman, D. A. & Dumitrascu, D. L. Rome III: New standard for functional gastrointestinal disorders. J. Gastrointestin. Liver Dis. 15(3), 237–241 (2006).
Cremonini, F. et al. Sleep disturbances are linked to both upper and lower gastrointestinal symptoms in the general population. Neurogastroenterol. Motil. 21(2), 128–135. https://doi.org/10.1111/j.1365-2982.2008.01181.x (2009).
Fang, Y. J. et al. Distinct aetiopathogenesis in subgroups of functional dyspepsia according to the Rome III criteria. Gut 64(10), 1517–1528. https://doi.org/10.1136/gutjnl-2014-308114 (2015).
Lacy, B. E., Everhart, K. & Crowell, M. D. Functional dyspepsia is associated with sleep disorders. Clin. Gastroenterol. Hepatol. 9(5), 410–414. https://doi.org/10.1016/j.cgh.2011.02.010 (2011).
Morito, Y. et al. Association between sleep disturbances and abdominal symptoms. Intern. Med. 53(19), 2179–2183 (2014).
Yamawaki, H. et al. Impact of sleep disorders, quality of life and gastric emptying in distinct subtypes of functional dyspepsia in Japan. J. Neurogastroenterol. Motil. 20(1), 104–112. https://doi.org/10.5056/jnm.2014.20.1.104 (2014).
Yu, J. et al. Gastrointestinal symptoms and associated factors in Chinese patients with functional dyspepsia. World J. Gastroenterol. 19(32), 5357–5364. https://doi.org/10.3748/wjg.v19.i32.5357 (2013).
Kim, H. I. et al. Impact of shiftwork on irritable bowel syndrome and functional dyspepsia. J. Korean Med. Sci. 28(3), 431–437 (2013).
Thompson, J. J., Elsenbruch, S., Harnish, M. J. & Orr, W. C. Autonomic functioning during REM sleep differentiates IBS symptom subgroups. Am. J. Gastroenterol. 97(12), 3147–3153. https://doi.org/10.1111/j.1572-0241.2002.07112.x (2002).
Vege, S. S. et al. Functional gastrointestinal disorders among people with sleep disturbances: A population-based study. Mayo Clin. Proc. 79(12), 1501–1506. https://doi.org/10.4065/79.12.1501 (2004).
David, D. et al. Sleep and duodenal motor activity in patients with severe non-ulcer dyspepsia. Gut 35(7), 916–925 (1994).
Fass, R., Fullerton, S., Tung, S. & Mayer, E. A. Sleep disturbances in clinic patients with functional bowel disorders. Am. J. Gastroenterol. 95(5), 1195–2000 (2000).
Miwa, H. Life style in persons with functional gastrointestinal disorders–large-scale internet survey of lifestyle in Japan. Neurogastroenterol. Motil. 24(5), 464–471. https://doi.org/10.1111/j.1365-2982.2011.01872.x (2012).
Van Oudenhove, L. & Aziz, Q. The role of psychosocial factors and psychiatric disorders in functional dyspepsia. Nat. Rev. Gastroenterol. Hepatol. 10(3), 158–167. https://doi.org/10.1038/nrgastro.2013.10 (2013).
Mulak, A. & Bonaz, B. Irritable bowel syndrome: A model of the brain-gut interactions. Med. Sci. Monit. 10(4), 55–62 (2004).
Zhen, Lu. W., Ann Gwee, K. & Yu, H. K. Functional bowel disorders in rotating shift nurses may be related to sleep disturbances. Eur. J. Gastroenterol. Hepatol. 18(6), 623–627 (2006).
Moldofsky, H. & Scarisbrick, P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom. Med. 38(1), 35–44 (1976).
Onen, S. H., Alloui, A., Gross, A., Eschallier, A. & Dubray, C. The effects of total sleep deprivation, selective sleep interruption and sleep recovery on pain tolerance thresholds in healthy subjects. J. Sleep Res. 10(1), 35–42 (2001).
Roehrs, T., Hyde, M., Blaisdell, B., Greenwald, M. & Roth, T. Sleep loss and REM sleep loss are hyperalgesic. Sleep 29(2), 145–151 (2006).
Schey, R. et al. Sleep deprivation is hyperalgesic in patients with gastroesophageal reflux disease. Gastroenterology 133(6), 1787–1795. https://doi.org/10.1053/j.gastro.2007.09.039 (2007).
Goldsmith, G. & Levin, J. S. Effect of sleep quality on symptoms of irritable bowel syndrome. Dig. Dis. Sci. 38(10), 1809–1814 (1993).
Jarrett, M., Heitkemper, M., Cain, K. C., Burr, R. L. & Hertig, V. Sleep disturbance influences gastrointestinal symptoms in women with irritable bowel syndrome. Dig. Dis. Sci. 45(5), 952–959 (2000).
Lu, W. Z., Gwee, K. A., Moochhalla, S. & Ho, K. Y. Melatonin improves bowel symptoms in female patients with irritable bowel syndrome: A double-blind placebo-controlled study. Aliment Pharmacol. Ther. 22(10), 927–934. https://doi.org/10.1111/j.1365-2036.2005.02673.x (2005).
Lee, H., Cho, Y. W. & Kim, H. A. The severity and pattern of autonomic dysfunction in idiopathic rapid eye movement sleep behavior disorder. Mov. Disord. 30(13), 1843–1848. https://doi.org/10.1002/mds.26416 (2015).
Mertz, H. et al. Effect of amitriptyline on symptoms, sleep, and visceral perception in patients with functional dyspepsia. Am. J. Gastroenterol. 93(2), 160–165. https://doi.org/10.1111/j.1572-0241.1998.00160.x (1998).
Quick, C. et al. Gastric dysmotility in major depression. Prog. Neuropsychopharmacol. Biol. Psychiatry. 34(1), 92–97. https://doi.org/10.1016/j.pnpbp.2009.10.003 (2010).
Smith, V. M., Jeffers, R. T. & Antle, M. C. Serotonergic enhancement of circadian responses to light: Role of the raphe and intergeniculate leaflet. Eur. J. Neurosci. 42(10), 2805–2817. https://doi.org/10.1111/ejn.13064 (2015).
Zitnik, G. A. Control of arousal through neuropeptide afferents of the locus coeruleus. Brain Res. 1641(Pt B), 338–350. https://doi.org/10.1016/j.brainres.2015.12.010 (2016).
Gershon, M. D. Review article: Serotonin receptors and transporters—roles in normal and abnormal gastrointestinal motility. Aliment Pharmacol. Ther. 20(Suppl 7), 3–14. https://doi.org/10.1111/j.1365-2036.2004.02180.x (2004).
Jiang, S. M. et al. Incidence and psychological-behavioral characteristics of refractory functional dyspepsia: A large, multi-center, prospective investigation from China. World J. Gastroenterol. 21(6), 1932–1937. https://doi.org/10.3748/wjg.v21.i6.1932 (2015).
Van Oudenhove, L., Vandenberghe, J., Vos, R., Holvoet, L. & Tack, J. Factors associated with co-morbid irritable bowel syndrome and chronic fatigue-like symptoms in functional dyspepsia. Neurogastroenterol. Motil. 23(6), 524-e202. https://doi.org/10.1111/j.1365-2982.2010.01667.x (2011).
Parry, S. D., Barton, J. R. & Welfare, M. R. Factors associated with the development of post-infectious functional gastrointestinal diseases: Does smoking play a role?. Eur. J. Gastroenterol. Hepatol. 17(10), 1071–1075 (2005).
El-Serag, H. B., Graham, D. Y., Satia, J. A. & Rabeneck, L. Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am. J. Gastroenterol. 100(6), 1243–1250 (2005).
NHIRD. National Health Insurance Research Database, Taiwan. Randomization Process of the Longitudinal Health Insurance Database (LHID2000), Taipei. Available at: http://w3.nhri.org.tw/nhird//date_cohort.htm. Accessed 20 January 2010.
Hsieh, C.-Y., Chen, C.-H., Li, C.-Y. & Lai, M.-L. Validating the diagnosis of acute ischemic stroke in a National Health Insurance claims database. J. Formos. Med. Assoc. 114(3), 254–259 (2015).
Kumar, A., Pate, J. & Sawant, P. Epidemiology of functional dyspepsia. J. Assoc. Physicians India. 60(Suppl), 9–12 (2012).
Ofman, J. J. et al. Meta-analysis of dyspepsia and nonsteroidal antiinflammatory drugs. Arthritis Rheumatism 49(4), 508–518 (2003).
Acknowledgements
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the Taiwan National Health Research Institutes, the Republic of China. As well as the Bureau of Health Promotion, Department of Health, R.O.C. (Taiwan) (DOH99-HP-1205); the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002); China Medical University Hospital; Academia Sinica Taiwan Biobank; Stroke Biosignature Project (BM104010092); NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006); Tseng-Lien Lin Foundation, Taichung, Taiwan; Brain Disease Foundation, Taipei, Taiwan; and Katsuzo and Kiyo Aoshima Memorial Funds, Japan. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes. RS is part-funded by: (i) the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London (ii) an NIHR Senior Investigator Award; (iii) the National Institute for Health Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust.
Funding
This series of study received funding from the Bureau of Health Promotion, Department of Health, R.O.C. (Taiwan) (DOH99-HP-1205); the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002); China Medical University Hospital; Academia Sinica Taiwan Biobank; Stroke Biosignature Project (BM104010092); NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006); Tseng-Lien Lin Foundation, Taichung, Taiwan; Brain Disease Foundation, Taipei, Taiwan; and Katsuzo and Kiyo Aoshima Memorial Funds, Japan. RS is part-funded by: (i) the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London (ii) an NIHR Senior Investigator Award; (iii) the National Institute for Health Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust. RS declares research support received in the last 36 months from Janssen, GSK and Takeda. SI is part-funded by Department of Medical Research, Mackay Memorial Hospital (MMH-109112, MMH-10914, MMH-108121, MMH-108146, MMH-TT-10804, MMH-TH-10804). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
S.I.W., K.-L.K., H.-H.S., C.-J.L., F.-C.S., Y.-S.C., designed the study and wrote the protocol. C.-L.L. and S.-I.W. undertook the statistical analysis. S.-I.W., H.-H.S., K.-L.K., F.-C.S., and R.S. wrote the drafts of the manuscript. All authors contributed to the revision and have approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Su, HH., Sung, FC., Kao, KL. et al. Relative risk of functional dyspepsia in patients with sleep disturbance: a population-based cohort study. Sci Rep 11, 18605 (2021). https://doi.org/10.1038/s41598-021-98169-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-98169-4
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
