
Abstract
Little is known regarding the association between depressive symptoms and metabolic syndrome (MetS) among older Chinese adults. This study aimed to examine the association of depressive symptoms with MetS and its components among Chinese elderly. Based on whether they showed depressive symptoms at baseline, 262 age-gender-matched participants from a community-based cohort study were included. The presence of depressive symptoms was measured using the nine-item Patient Health Questionnaire (PHQ-9). MetS was defined according to the Adult Treatment Panel III of the National Cholesterol Education Program. Linear regression and logistic regression analyses were performed to assess associations of depressive symptoms with MetS and its components. The incidence of MetS among the participants with depressive symptoms at baseline was 15.27% (20/131). The association of the presence of depressive symptoms with MetS was significant (odds ratio [OR] = 2.53, 95% confidence intervals [CI] = 1.07, 5.95). There was a negative association between depressive symptoms and hypertension (OR = 0.04, 95% CI = 0.002, 0.98). The change in mean arterial pressure varies approximately 1.03 mmHg with a 1-point change in PHQ-9 score. In this study, baseline depressive symptoms were associated with subsequent MetS. The presence of depressive symptoms was negatively associated with elevated mean arterial pressure.
Similar content being viewed by others


Introduction
Metabolic syndrome (MetS) is one of the prevalent concerns to global public health1,2. It is characterized by a clustering of cardiovascular risk factors including low level of high-density lipoprotein cholesterol (HDL-C), abdominal obesity, high blood pressure (BP), high level of triglycerides (TG), and elevated fasting plasma glucose (FPG) or diabetes. Current literatures have acknowledged that there is a bidirectional association of mental health with physical health3,4. Modern Chinese rural elderly people are facing much severer mental and physical challenge than ever5. Various factors such as aging6 and chronic disease7 which put a detrimental effect on mental health led to bad outcomes including the risk of disorders8 and mortality9 of the elderly. It has demonstrated that depression is one of the most common psychiatric illnesses in later life, with a prevalence of 4.5–37.4% in different studies10. There is substantial evidence to support that depression is also linked to cardiovascular disease11 and diabetes12. Hence, it’s reasonable to hypothesize that there is a relationship between depression and MetS.
In China, the development of MetS has risen rapidly, with the prevalence of 33.9% (31.0% in male and 36.8% in female)13. Previous studies have demonstrated the association of MetS with cognitive impairment14, dementia, and Alzheimer’s disease15. A recent system review reported that the depression was associated with 1.34 times the odds of developing the MetS16. To date, some cross-sectional studies indicated that depression or the presence of depressive symptoms was associated with MetS17 and the components of MetS18, whereas some studies did not detect such an association19,20. Some lifestyle habits were observed to contribute to the subsequent MetS21. However, few studies have assessed the relationship among Chinese22 and most of the longitudinal research is carried in developed countries or areas16,23. In East Asia, a Korean research24 revealed a positive correlation between depression trajectory and MetS in a retrospective cohort, which still remained a lack of control over demographic characteristics that may confuse the results.
It’s well known that lifestyles and living habits vary widely across geographical settings and different cultural backgrounds. Unique culture and lifestyle could alter the real association between depressive symptoms and MetS. Thus, the impact of different cultural differences on diseases is worthy of further exploration.
Accordingly, the aim of this study was to assess the association of initial depressive symptoms with subsequent MetS in Chinese adults aged 60 years or older, and further examine the extent to which potential explanatory factors impact the incidence of MetS in older people with or without depressive symptoms.
Methods
Study population
Data of this study were from the Weitang Geriatric Diseases study, which is a community-based cohort study conducted in Weitang town among adults aged 60 years and above in Suzhou, China. More detailed information of the study protocols has been described elsewhere25. According to the official record, 6,030 adults aged 60 years or older received an invitation letter. Participants were deemed eligible to participate in further study if (1) he or she had not migrated from the residential address; (2) residents had been living in the town for longer than six months; (3) he or she stayed alive. Finally, 4579 participants completed both interviewer-administered questionnaires and clinical examinations. The baseline investigation was conducted in 2014 and the follow-up investigation was carried out five years later.
Figure 1 describes the selection of participants included and excluded in the current analysis. We screened out 919 participants who had MetS at baseline, 153 participants who had departed and 564 participants with incomplete data. Of the remaining 2,961 participants, we found that a large discrepancy in age and gender between participants with or without the presence of depressive symptoms. Therefore, each participant with depressive symptoms was matched with one non-depressive counterpart based on the strategy of the same gender and same age, namely 131 participants with the presence of depressive symptoms and 131 were free of depressive symptoms.

Flow diagram showing the screening of study participants. MetS metabolic syndrome.
All participants provided written informed consent before data collection. The study was undertaken in agreement with the Declaration of Helsinki and approved by the Institutional Review Board of Soochow University.
Assessment of depressive symptoms
The nine-item Patient Health Questionnaire (PHQ-9), a widely utilized screening tool for depression and depressive symptoms in clinical settings26, was used to assess depressive symptoms at baseline. Items on the scale correspond to the criteria of Diagnostic and Statistical Manual of Mental Disorders (DSM, Fourth Edition)27. Eight items of the PHQ-9 evaluate how often they suffered from the depressive symptoms over the past two weeks, and the last item is about the frequency of thoughts that hurt themselves during the past two weeks. The response options are on a four-point Likert scale (0 = not at all, 1 = several days, 2 = more than half of the days, and 3 = nearly every day), and higher scores denote higher levels of depressive symptoms. A score of 5 or higher is indicative of having depressive symptoms28.
Measurement of MetS and its components
MetS was defined according to the Adult Treatment Panel III of the National Cholesterol Education Program (ATP III-NCEP)29. Participants were considered as having MetS if they had three or more of the following conditions: (1) overweight or obesity (body mass index ≥ 25 kg/m2)30; (2) BP ≥ 130/85 mmHg or history of antihypertensive treatment; (3) the serum level of TG > 150 mg/dL (1.69 mmol/L); (4) HDL-C < 40 mg/dL in men or < 50 mg/dL in women; (5) FPG ≥ 7.0 mmol/L or previously confirmed diagnosis of diabetes mellitus.
Assessment of covariates
Covariates were included as possible confounding variables affecting the metabolic abnormalities or depression31,32,33,34,35,36. All covariates included in the model were collected at baseline. Information of socio-demographic characteristics (i.e., age, gender, marital status, and education level) was collected through the pre-designed questionnaire. Marital status was divided into living ‘with’ or ‘without’ spouse. The education level was divided into two groups, one was participants who have completed elementary education or junior high school education or senior high school education or the university and above. The other group, namely ‘no formal education’ referred to participants who have completed none of them. Lifestyle-related factors were also recorded such as smoking (present/past/never), alcohol consumption (drinkers/non-drinkers), tea consumption (drinkers/non-drinkers), dietary patterns (normal/vegetarian) and physical activity (yes/no). The alcohol consumption referred to the answers of ‘whether the participants had drunk alcohol drink in the past three months’. Normal diet referred to participants who ate meat or fish. The histories of cardiovascular diseases including heart disease (yes/no) and stroke (yes/no) were self-reported by participants.
Statistical analysis
Given the high correlation of systolic and diastolic blood pressure, we rescaled them into a single measure of mean arterial pressure (MAP), using the following standard Eq. (1)37: \(\mathrm{MAP}=\frac{(2*{\varvec{P}}\boldsymbol{ } {\text{diastolic}}+{\varvec{P}}\boldsymbol{ } {\text{systolic}})}{3}\).
Categorical variables of participants with or without depressive symptoms were compared with a cross-tabulation, using Pearson’s χ2 test. The cumulative incidence of MetS was estimated as the number of cases divided by persons at risk only those who fully completed the follow-up (selected through the matching).
To estimate the associations of depressive symptoms (defined as the PHQ-9 scores as a continuous variable) with the change in each component of MetS, multivariate regression models were fitted, adjusting for education level, marital status, smoking, alcohol consumption, tea consumption, physical activity and heart disease. The model assumptions were checked. Variance infiltration factor (VIF) was used to identify the multicollinearity between the variables in each model. A VIF > 10.0 was considered significant multicollinearity in the regression model38. The change in each component is calculated as the results of follow-up clinical examination minus the results at baseline. Before proceeding to analyze the associations of depressive symptoms with the change in each component of MetS, we excluded subjects who met the clinical criteria for individual components of MetS at baseline.
To evaluate the extent to which the risk factors may explain the excess incidence of MetS in participants with depressive symptoms compared with those without depressive symptoms, we estimated the percentage of reduction in odds associated with adjustment for these factors based on the following formula: (Ra-Rb)/(Ra-1) × 100, where Ra is the OR of MetS in the participants with depressive symptoms compared with their non-depressive counterparts in the crude model, and Rb is the OR in models after additional adjustment. Such method was applied in previous research39. In this study, the excess incidence referred to the incidence of MetS in participants with depressive symptoms compared to participants without depressive symptoms.
To test whether depressive symptoms were associated with MetS and each of its components, logistic regression models were performed and odds ratios (OR) and 95% confidence intervals (CI) were shown. Education level, marital status, smoking, alcohol consumption, tea consumption, physical activity and history of heart disease were included in the analytic models as covariates.
All statistical analyses were carried out using IBM SPSS Statistics for Windows (Version 22.0. Armonk, NY: IBM Corp., USA), and a P value of less than 0.05 was considered statistically significant.
Results
Table 1 lists the demographic characteristics of study participants at baseline. The mean age of participants was 74.41 years (age range 63–90). Among them, the mean age in the oldest-old participants (> 80 years) was 84.01 ± 5.87 years compared with 70.70 ± 4.86 years in more young-old (≤ 80 years) participants. Among the samples, the incidence of MetS was 15.27% in participants with depressive symptoms at baseline and 6.9% in people who were free of depressive symptoms at baseline. People without depressive symptoms tended to live with spouse. Compared with the non-depressive counterparts group, people with depressive symptoms had less physical activity, higher consumption of tea, and higher prevalence of stroke.
The change in MAP varied approximately 1.03 mmHg with a 1-point increase in PHQ-9 score. The change in MAP was significantly associated with the presence of depressive symptoms (as a continuous variable) (P = 0.047), after adjusting for education level, marital status, smoking, alcohol consumption, tea consumption, physical activity and heart disease (Table 2). None of the variables showed significant collinearity with each other (all VIF < 10.0). Additionally, no significant association were observed between the depressive symptoms and different variations of risk factors numbers (data not shown).
We estimated the reduction in odds of MetS associated with the presence of depressive symptoms with adjustment of MetS-related variables. Adjustment for education level, smoking, alcohol consumption or history of heart disease led to reduction in the excess incidence of MetS in participants with depressive symptoms by 4.17%, 4.86%, 0.69% or 0.69%, respectively. On the contrary, adjustment for marital status and physical activity increased the excess incidence of MetS by 6.25%, 5.56%, relatively (Table 3).
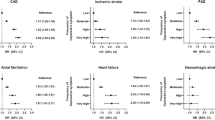
In the total study sample, the presence of depressive symptoms was significantly associated with MetS and MAP. Compared with non-depressive counterparts, the presence of depressive symptoms increased odds of MetS, after adjusting for education level, marital status, smoking, alcohol consumption, tea consumption, physical activity and heart disease (OR = 2.53, 95% CI = 1.07, 5.94, P = 0.03). Only the relationship between depressive symptoms with MAP (OR = 0.04, 95% CI = 0.002, 0.98, P = 0.048) was significant after adjusting for confounding factors rather than in the crude model (Fig. 2).

Relationship between depressive symptoms and metabolic components with or without multivariate adjustment in participants. (a) Crude model; (b) adjusted for education level, marital status, smoking, alcohol consumption, tea consumption, physical activity and heart disease. MetS metabolic syndrome, BMI body mass index, FPG fasting plasma glucose, HDL high-density lipoprotein cholesterol, OR odds ratio.
Discussion
In this community-based cohort study among older people aged 60 years or over, we found that participants with initial depressive symptoms tended to have increased risk of MetS. Focusing on the individual components of MetS, the presence of depressive symptoms (as a continuous variable) was associated with the change in MAP after adjusting for potential confounders. However, the magnitude of the association was relatively weak. Our findings also provided information for which the interventions targeting lifestyle risk factors could reduce the development of MetS.
In the present study, the presence of depressive symptoms at baseline was associated with approximately twice the odds of having MetS in the full sample; this association remained statistically significant after controlling for the confounding variables. Several studies have linked depression or depressive symptoms with MetS. However, the findings are controversial and most of these studies are cross-sectional design. Our finding is consistent with a cross-sectional analysis among older people in Japan40 and a cohort study among middle-aged people in French (65–70 years old at baseline)41. It is especially noted that researchers demonstrated opposite results in two of the largest studies in Norway42 and Finland20, respectively. Nevertheless, some plausible pathophysiological mechanisms have been proposed to help elucidate the association between depression and MetS. Firstly, the hypothalamic-pituitary adrenal axis associated with the clinical depression is activated in MetS, which is related to visceral obesity43 and impaired insulin sensitivity44,45. Besides, the prospective relationship between initial depressive symptoms and later MetS involves effects of physiological correlates of stress and dysphoric emotion46, which also influence the dysregulations mentioned above. Secondly, the dysregulation of the autonomic nervous system via such pathways as aberrant serotonergic functioning47 has been proposed as a possible mechanism.
The present results also indicated that the presence of depressive symptoms was inversely associated with the change in MAP. We defined BP as a single measure of MAP, on account of MAP is more accurate in predicting future MetS among the elderly population37,48. The association remained negatively significant in logistic regression models. Our finding is in line with prior prospective study investigating the association of depressive symptoms with developing MetS among Iranian elderly population, especially in women19. The interaction between depression and hypertension is pathophysiologically reasonable49. A meta-analysis of prospective cohort found that patients with depressive and hypertension have increased sympathetic tone and increased secretion of adrenocorticotropic hormone and cortisol50. Meanwhile, researchers have proposed a relationship between sympathetic activity and increased BP and emotional problems with MetS51. The possible reason for our result may be the side effects of antidepressant use. Some drug therapies have been reported that could negatively affect BP in elderly individuals52,53. Moreover, follow-up study has reported that the positive correlation between initial depression and later hypertension may exist during the follow-up for 5 years and longer54. More research is encouraged to clarify this relationship.
Although the incidence of MetS was higher among participants with depressive symptoms compared with their counterparts, a 4.86%, 0.69%, and 0.69% of the excess incidence was due to the current smoking, alcohol consumption and history of heart disease on the cohort, respectively. Tea consumption reduced 9.72% of the excess incidence, though did not reach the statistical significance (P = 0.05). We think that nowadays tea culture prevails in more than 160 countries, especially in China. This is not sufficient to turn around the onset of MetS worldwide, but the result indicates that tea consumption is negatively associated with MetS. A growing body of evidence suggests that several bioactive components in tea have the potential in adjusting blood lipids35 and benefit cardiovascular and metabolic health55.
The strengths in this study include its longitudinal design among older people and the use of standard assessment of depressive symptoms. Some limitations of this study should also be noted. First, we measure the depressive symptoms with a symptom scale, which did not reflect the depression as accurately as diagnosis. Second, for living habits, self-report method is adopted, which could lead to information bias (e.g., recall bias and reporting bias). Third, this study focused on whether depressive symptoms at baseline associated with subsequent metabolic syndrome, rather than the changing trend of the association. Finally, our study is based on a community-dwelling population, which the number of depression patients is relatively smaller than that of the clinical population.
In conclusion, this study demonstrated a significant association of the presence of depressive symptoms with MetS and its component in the sample of Chinese elderly. However, hypertension was negatively associated with depressive symptoms when adjusted for confounders. Further research is warranted to investigate the association of BP with depression using large longitudinal cohorts.
Abbreviations
- MetS:
-
Metabolic syndrome
- HDL-C:
-
High-density lipoprotein cholesterol
- BP:
-
Blood pressure
- TG:
-
Triglycerides
- FPG:
-
Fasting plasma glucose
- PHQ-9:
-
The nine-item patient health questionnaire
- MAP:
-
Mean arterial pressure
- VIF:
-
Variance infiltration factor
- OR:
-
Odds ratio
- CI:
-
Confidence intervals
References
Ortiz-Rodríguez, M. A. et al. Prevalence of metabolic syndrome among elderly Mexicans. Arch. Gerontol. Geriatr. 73, 288–293. https://doi.org/10.1016/j.archger.2017.09.001 (2017).
Denys, K., Cankurtaran, M., Janssens, W. & Petrovic, M. Metabolic syndrome in the elderly: An overview of the evidence. Acta Clin. Belg. 64, 23–34. https://doi.org/10.1179/acb.2009.006 (2009).
Sheng, T. et al. The influence of physical and mental health symptoms on Veterans’ functional health status. J. Rehabil. Res. Dev. 53, 781–796. https://doi.org/10.1682/jrrd.2015.07.0146 (2016).
Pérez-de la Cruz, S. Mental health in Parkinson’s disease after receiving aquatic therapy: a clinical trial. Acta Neurol. Belg. 119, 193–200. https://doi.org/10.1007/s13760-018-1034-5 (2019).
Zhao, D. et al. Risk factors of geriatric depression in rural China based on a generalized estimating equation. Int. Psychogeriatr. 30, 1489–1497. https://doi.org/10.1017/s1041610218000030 (2018).
Gong, Y., Wen, X., Guan, C., Wang, Z. & Liang, Y. The associations between family characteristics and depressive symptoms in older adults: A community-based survey in rural China. Int. Psychogeriatr. 24, 1226–1234. https://doi.org/10.1017/s1041610211002663 (2012).
Moussavi, S. et al. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet (London, England) 370, 851–858. https://doi.org/10.1016/s0140-6736(07)61415-9 (2007).
Tseng, T. J. et al. Association between health behaviors and mood disorders among the elderly: A community-based cohort study. BMC Geriatr. 19, 60. https://doi.org/10.1186/s12877-019-1079-1 (2019).
Plana-Ripoll, O. et al. A comprehensive analysis of mortality-related health metrics associated with mental disorders: A nationwide, register-based cohort study. Lancet (London, England) 394, 1827–1835. https://doi.org/10.1016/s0140-6736(19)32316-5 (2019).
Luppa, M. et al. Age- and gender-specific prevalence of depression in latest-life–systematic review and meta-analysis. J. Affect Disord. 136, 212–221. https://doi.org/10.1016/j.jad.2010.11.033 (2012).
O’Brien, E. C. et al. Depressive symptoms and risk of cardiovascular events in blacks: findings from the Jackson heart study. Circ. Cardiovasc. Qual. Outcomes 8, 552–559. https://doi.org/10.1161/circoutcomes.115.001800 (2015).
Nouwen, A. et al. Longitudinal associations between depression and diabetes complications: A systematic review and meta-analysis. Diabet. Med. 36, 1562–1572. https://doi.org/10.1111/dme.14054 (2019).
Lu, J. et al. Metabolic syndrome among adults in China: The 2010 China noncommunicable disease surveillance. J. Clin. Endocrinol. Metab. 102, 507–515. https://doi.org/10.1210/jc.2016-2477 (2017).
Feinkohl, I. et al. Associations of the metabolic syndrome and its components with cognitive impairment in older adults. BMC Geriatr. 19, 77. https://doi.org/10.1186/s12877-019-1073-7 (2019).
Panza, F. et al. Metabolic syndrome, mild cognitive impairment, and dementia. Curr. Alzheimer Res. 8, 492–509. https://doi.org/10.2174/156720511796391818 (2011).
Pan, A. et al. Bidirectional association between depression and metabolic syndrome: A systematic review and meta-analysis of epidemiological studies. Diabetes Care 35, 1171–1180. https://doi.org/10.2337/dc11-2055 (2012).
Ra, J. S. & Kim, H. S. Sex-based association between depression and metabolic syndrome in Korean middle-aged and older adults. Osong. Public Health Res. Perspect. 8, 130–137. https://doi.org/10.24171/j.phrp.2017.8.2.05 (2017).
Ruas, L. G. et al. Components of the metabolic syndrome and depressive symptoms in community-dwelling older people: The Bambuí Cohort Aging Study. Braz. J. Psychiatry 38, 183–189. https://doi.org/10.1590/1516-4446-2015-1856 (2016).
Bakhtiari, A. et al. The relationship between depression and metabolic syndrome in the elderly population: The cohort aging study. Iran J. Psychiatry 13, 230–238 (2018).
Herva, A. et al. Co-occurrence of metabolic syndrome with depression and anxiety in young adults: The Northern Finland 1966 Birth Cohort Study. Psychosom. Med. 68, 213–216. https://doi.org/10.1097/01.psy.0000203172.02305.ea (2006).
Matta, J. et al. Diet and physical activity in the association between depression and metabolic syndrome: Constances study. J. Affect Disord. 244, 25–32. https://doi.org/10.1016/j.jad.2018.09.072 (2019).
Yu, S., Yang, H., Guo, X., Zheng, L. & Sun, Y. Metabolic syndrome and depressive symptoms among rural Northeast general population in China. BMC Public Health 17, 43. https://doi.org/10.1186/s12889-016-3913-0 (2017).
Goldbacher, E. M., Bromberger, J. & Matthews, K. A. Lifetime history of major depression predicts the development of the metabolic syndrome in middle-aged women. Psychosom. Med. 71, 266–272. https://doi.org/10.1097/PSY.0b013e318197a4d5 (2009).
Kim, E. Y. et al. Depression trajectories and the association with metabolic adversities among the middle-aged adults. J. Affect Disord. 188, 14–21. https://doi.org/10.1016/j.jad.2015.08.024 (2015).
Yin, J. Y. et al. Blood pressure is associated with tea consumption: A cross-sectional study in a rural, elderly population of Jiangsu China. J. Nutr. Health Aging 21, 1151–1159. https://doi.org/10.1007/s12603-016-0829-4 (2017).
Smarr, K. L. & Keefer, A. L. Measures of depression and depressive symptoms: beck depression inventory-II (BDI-II), center for epidemiologic studies depression scale (CES-D), geriatric depression scale (GDS), hospital anxiety and depression scale (HADS), and patient health questionnaire-9 (PHQ-9). Arthritis Care Res. (Hoboken) 63(Suppl 11), S454-466. https://doi.org/10.1002/acr.20556 (2011).
Kroenke, K., Spitzer, R. L., Williams, J. B. & Löwe, B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. Gen. Hosp. Psychiatry 32, 345–359. https://doi.org/10.1016/j.genhosppsych.2010.03.006 (2010).
Kroenke, K. Enhancing the clinical utility of depression screening. CMAJ 184, 281–282. https://doi.org/10.1503/cmaj.112004 (2012).
Cleeman, J. I. et al. Executive summary of the third report of the national cholesterol education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama-J. Am. Med. Assoc. 285, 2486–2497. https://doi.org/10.1001/jama.285.19.2486 (2001).
Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet (London, England) 363, 157–163, doi:https://doi.org/10.1016/s0140-6736(03)15268-3 (2004).
Jenkins, A. I. C. et al. Prospective associations between depressive symptoms and marital satisfaction in Black couples. J. Fam. Psychol. 34, 12–23. https://doi.org/10.1037/fam0000573 (2020).
Kiama, C. N. et al. Prevalence and factors associated with metabolic syndrome in an urban population of adults living with HIV in Nairobi, Kenya. Pan Afr. Med. J. 29, 90. https://doi.org/10.11604/pamj.2018.29.90.13328 (2018).
Sin, N. L., Kumar, A. D., Gehi, A. K. & Whooley, M. A. Direction of association between depressive symptoms and lifestyle behaviors in patients with coronary heart disease: The heart and soul study. Ann. Behav. Med. 50, 523–532. https://doi.org/10.1007/s12160-016-9777-9 (2016).
Deen, J. F. et al. Metabolic syndrome in adults with congenital heart disease. J. Am. Heart Assoc. https://doi.org/10.1161/jaha.114.001132 (2016).
Chu, S. L. et al. A randomized double-blind placebo-controlled study of Pu’er tea extract on the regulation of metabolic syndrome. Chin. J. Integr. Med. 17, 492–498. https://doi.org/10.1007/s11655-011-0781-4 (2011).
Suliga, E. et al. Consumption of alcoholic beverages and the prevalence of metabolic syndrome and its components. Nutrients https://doi.org/10.3390/nu11112764 (2019).
Smith, T. W., Eagle, D. E. & Proeschold-Bell, R. J. Prospective associations between depressive symptoms and the metabolic syndrome: The spirited life study of methodist pastors in North Carolina. Ann. Behav. Med. 51, 610–619. https://doi.org/10.1007/s12160-017-9883-3 (2017).
Carsten, F. D. et al. Collinearity: A review of methods to deal with it and a simulation study evaluating their performance. Ecography 2, 2 (2013).
Wong, T. Y. et al. Racial differences in the prevalence of hypertensive retinopathy. Hypertension 41, 1086–1091. https://doi.org/10.1161/01.Hyp.0000064181.63546.53 (2003).
Morikawa, M. et al. Association between depressive symptoms and metabolic syndrome in Japanese community-dwelling older people: A cross-sectional analysis from the baseline results of the Fujiwara-kyo prospective cohort study. Int. J. Geriatr. Psychiatry 28, 1251–1259. https://doi.org/10.1002/gps.3950 (2013).
Akbaraly, T. N. et al. Metabolic syndrome and onset of depressive symptoms in the elderly: Findings from the three-city study. Diabetes Care 34, 904–909. https://doi.org/10.2337/dc10-1644 (2011).
Hildrum, B., Mykletun, A., Midthjell, K., Ismail, K. & Dahl, A. A. No association of depression and anxiety with the metabolic syndrome: The Norwegian HUNT study. Acta Psychiatr. Scand. 120, 14–22. https://doi.org/10.1111/j.1600-0447.2008.01315.x (2009).
Weber-Hamann, B. et al. Hypercortisolemic depression is associated with increased intra-abdominal fat. Psychosom. Med. 64, 274–277. https://doi.org/10.1097/00006842-200203000-00010 (2002).
Brunner, E. J. et al. Adrenocortical, autonomic, and inflammatory causes of the metabolic syndrome: Nested case-control study. Circulation 106, 2659–2665. https://doi.org/10.1161/01.cir.0000038364.26310.bd (2002).
Weber-Hamann, B. et al. Activity of the hypothalamus-pituitary-adrenal system and oral glucose tolerance in depressed patients. Neuroendocrinology 81, 200–204. https://doi.org/10.1159/000087003 (2005).
Goldbacher, E. M. & Matthews, K. A. Are psychological characteristics related to risk of the metabolic syndrome? A review of the literature. Ann. Behav. Med. 34, 240–252. https://doi.org/10.1007/bf02874549 (2007).
Muldoon, M. F. et al. The metabolic syndrome is associated with reduced central serotonergic responsivity in healthy community volunteers. J. Clin. Endocrinol. Metab. 91, 718–721. https://doi.org/10.1210/jc.2005-1654 (2006).
Hsu, C. H. et al. Mean arterial pressure is better at predicting future metabolic syndrome in the normotensive elderly: A prospective cohort study in Taiwan. Prev. Med. 72, 76–82. https://doi.org/10.1016/j.ypmed.2014.12.036 (2015).
Li, H. et al. Association of depressive symptoms with incident cardiovascular diseases in middle-aged and older Chinese adults. JAMA Netw. Open 2, e1916591. https://doi.org/10.1001/jamanetworkopen.2019.16591 (2019).
Meng, L., Chen, D., Yang, Y., Zheng, Y. & Hui, R. Depression increases the risk of hypertension incidence: A meta-analysis of prospective cohort studies. J. Hypertens. 30, 842–851. https://doi.org/10.1097/HJH.0b013e32835080b7 (2012).
Lambert, E. et al. Association between the sympathetic firing pattern and anxiety level in patients with the metabolic syndrome and elevated blood pressure. J. Hypertens. 28, 543–550. https://doi.org/10.1097/HJH.0b013e3283350ea4 (2010).
Scalco, M. Z., Serro-Azul, J. B., Giorgi, D., Almeida, O. P. & Wajngarten, M. Effect of nortriptyline on the day-night systolic blood pressure difference in hypertensive and normotensive elderly depressed women. Am. J. Cardiol. 91, 1279–1281. https://doi.org/10.1016/s0002-9149(03)00286-8 (2003).
Scalco, A. Z., Scalco, M. Z., Azul, J. B. & Lotufo Neto, F. Hypertension and depression. Clinics (Sao Paulo) 60, 241–250. https://doi.org/10.1590/s1807-59322005000300010 (2005).
Jonas, B. S., Franks, P. & Ingram, D. D. Are symptoms of anxiety and depression risk factors for hypertension? Longitudinal evidence from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. Arch. Fam. Med. 6, 43–49. https://doi.org/10.1001/archfami.6.1.43 (1997).
Wolfram, S. Effects of green tea and EGCG on cardiovascular and metabolic health. J. Am. Coll. Nutr. 26, 373s–388s. https://doi.org/10.1080/07315724.2007.10719626 (2007).
Acknowledgements
We would like to thank all the participants who participated in this study for their time and willingness to contribute.
Funding
This study was supported by the Science and Technology Bureau of Xiangcheng District in Suzhou, China under Grant nos. XJ201706 and GSWS2019090.
Author information
Authors and Affiliations
Contributions
Q.W. carried out the statistical analysis and wrote manuscript. Y.Y.H. extracted data and performed the statistical analysis. Q.H.M. and Y.X. collected the data. X.C. and C.W.P. designed the study and revised the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wu, Q., Hua, YY., Ma, QH. et al. Depressive symptoms and 5-year incident metabolic syndrome among older adults. Sci Rep 11, 14842 (2021). https://doi.org/10.1038/s41598-021-94503-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-94503-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
