
Abstract
We aim to prospectively investigate, in a large and heterogeneous population, the electroencephalogram (EEG)-reading performances of EEG technologists. A total of 8 EEG technologists and 5 certified neurophysiologists independently analyzed 20-min EEG recordings. Interrater agreement (IRA) for predefined EEG pattern identification between EEG technologists and neurophysiologits was assessed using percentage of agreement (PA) and Gwet-AC1. Among 1528 EEG recordings, the PA [95% confidence interval] and interrater agreement (IRA, AC1) values were as follows: status epilepticus (SE) and seizures, 97% [96–98%], AC1 kappa = 0.97; interictal epileptiform discharges, 78% [76–80%], AC1 = 0.63; and conclusion dichotomized as “normal” versus “pathological”, 83.6% [82–86%], AC1 = 0.71. EEG technologists identified SE and seizures with 99% [98–99%] negative predictive value, whereas the positive predictive values (PPVs) were 48% [34–62%] and 35% [20–53%], respectively. The PPV for normal EEGs was 72% [68–76%]. SE and seizure detection were impaired in poorly cooperating patients (SE and seizures; p < 0.001), intubated and older patients (SE; p < 0.001), and confirmed epilepsy patients (seizures; p = 0.004). EEG technologists identified ictal features with few false negatives but high false positives, and identified normal EEGs with good PPV. The absence of ictal features reported by EEG technologists can be reassuring; however, EEG traces should be reviewed by neurophysiologists before taking action.
Similar content being viewed by others


Introduction
Electroencephalograms (EEGs) are widely performed for a large range of indications, including but not restricted to epilepsy and seizure diagnosis and classification1,2, status epilepticus (SE) diagnosis and treatment monitoring3,4,5, the investigation of consciousness disorders6, and prognostication after cardiac arrest7. Although a precise glossary exists to describe the most common EEG features8, and the American Society of Clinical Neurophysiology (ACNS) has established standardized criteria for intensive care unit (ICU) EEG analysis9, EEG interpretation remains subjective and is likely affected by the interpreter’s level of training, location of training, and the patient’s history. Several studies have examined the interrater agreement (IRA) of EEG interpretations after the introduction of the ACNS criteria, especially in ICU settings between experts10,11,12,13. However, evidence regarding the IRA between certified EEG readers and EEG technologists is currently lacking.
The principal role of EEG technologists is to obtain high-quality recordings. However, their contributions often extend beyond this role. For example, EEG technologists were reported to make a significant contribution to the diagnosis of childhood epileptic syndrome by collecting clinical information during the preparation of children for EEGs14. Technologists’ roles are not limited to EEG recording; they may also perform EEG readings. EEG technologists are often the first to read the EEGs at the patient’s bedside and are expected to contact the physicians in charge in case of findings requiring urgent action. Furthermore, with the increasing use of continuous EEG (cEEG) monitoring, EEG technologists are often asked to review EEG monitoring15. A national survey assessing cEEG ICU indications and procedures at 151 institutions in the United States revealed that EEG technologists reviewed 100% of the cEEG records at 26% of institutions and half of the records at 56% of institutions15.
In a large, prospective, single-center cohort, we aimed to investigate the IRA between certified neurophysiologists and EEG technologists. We also aimed to investigate which clinical factors, if any, may alter the EEG-reading performances of EEG technologists.
Methods
Study design
This single-institution, prospective cohort study, was approved by Ethics Commission of Goethe-University Frankfurt (number 278/15) and registered at the German Clinical Trials Register (DRKS Trial Number: DRKS00009863; Universal Trial Number: U1111-1178-2516; Registered 13/01/2016, http://www.drks.de/ DRKS00009863). Informed consent was waived due to the anonymized analysis of EEG and clinical data. The study was performed in accordance with relevant guidelines and regulations.
Patients
Consecutive adults and adolescents (≥ 15 years old) who underwent routine 20-min EEG (rEEG) recordings during a one-year period, starting January 2016, were included. With the exception of EEGs recorded for brain death diagnoses16, any routine EEGs that were recorded at our neurology department during the study period with a minimum duration of 20 min were included, regardless of the clinical indication for the recording or the patient´s localization (ambulatory, neurological ward, ICU or other medical and surgical wards). The indications for recordings were dichotomized between: (1) epileptic indications included SE, seizure or seizure suspicion, and the management of known epilepsy, such as the worsening of seizures or driving wishes; and (2) nonepileptic indications included disorders associated with consciousness or delirium. The final diagnosis was prospectively defined according to the International League Against Epilepsy (ILAE) criteria2: (1) no epilepsy-related diagnosis; (2) known epilepsy; (3) new epilepsy diagnosis; (4) first seizures; and (5) acute symptomatic seizures. Seizures and epilepsy types were prospectively classified according to the ILAE definitions1, 2. Status epilepticus (SE) was defined according to the current guidelines as seizures that persist for longer than 5 min or EEG patterns consistent with non-convulsive SE, as previously defined3,4,17. Collaboration was assessed by EEG-technologists during the EEG recordings and subjectively categorized into good/moderate/poor.
EEG recordings and analysis
EEGs were recorded using at least 21 electrodes, arranged according to the international 10–20 system. Reduced montages were allowed in neurosurgical patients, consistent with common practices, and more extensive montages were possible.
A standardized EEG interpretation sheet was provided to EEG technologists and neurophysiologists. The analyzed parameters included: (1) the presence of sleep figures (K complexes and spindles); (2) posterior dominant rhythm (PDR) presence and main frequency; (3) the presence of a slowing with the characteristics of (3a) slowing localization: focal, hemispheric, or generalized and (3b) slowing duration: intermittent or continuous; (4) the presence of interictal epileptiform discharges (IED) with the characteristics of (4a) IED localization: focal, multifocal, or generalized; (5) the occurrence of seizures; (6) SE; and (7) Global conclusion, dichotomized as normal or pathologic. The EEG interpretation sheet (Supplementary Fig. 1) was first filled by the EEG technologists at the bedside, during EEG recordings, and then by the neurophysiologists, who were blinded to the technologists’ conclusions, during formal EEG readings. A total of 8 EEG technologists, who each had at least three years of training in neurophysiological diagnostics, as “Medizinisch-Technische/r Assistent/in–Funktionsdiagnostik” (MTA-F), and 5 trained neurophysiologists, with board certifications in EEG readings (including PSR, FR, and AS), participated in this study.
EEG readings were performed under “real-life” conditions, with no additional training provided to the EEG technologists before the study. The patients’ clinical data, such as the reason for referral and medical history, including previous seizures or known epilepsy diagnoses, were available to the EEG readers.
Statistical analysis
Continuous and categorical variables are reported as the medians and range and were compared using Wilcoxon or T-tests, as appropriate. Binary variables are reported as the number and percentage and were assessed by Chi-square or Fisher’s exact tests and post hoc, pairwise Fisher’s exact tests. The predictive performances of EEG technologists for the identification of each predefined EEG pattern, when considering the neurophysiologists’ conclusions to be the gold standard, were estimated using exact binomial distributions, and the results are presented as specificity (Sp), sensitivity (Se), positive predictive value (PPV), or negative predictive value (NPV), with 95% confidence intervals (95% CIs). Exams during which EEG technologists reported the specified EEG features as being present when neurophysiologist reported the features as being absent were considered false positives (FPs), whereas those in which neurophysiologists coded the EEG features as being present but the EEG technologists coded the features as being absent were considered false negatives (FNs). The FP percentages are expressed as the FP rate among all exams coded “yes” by the EEG technologists, whereas the FN percentages are expressed as the FN rate among all exams coded “no” by the EEG technologists. Interrater agreement (IRA) was calculated using the Gwet’s agreement coefficient AC1 (for categorical dta) and AC2 (for ordinal data) to avoid the kappa paradox18 and the percentage of agreement (PA). The recommended strength of agreement nomenclature was used: < 0 = Poor; 0–0.20 = Slight; 0.21–0.40 = Fair; 0.41–0.60 = Moderate; 0.61–0.80 = Substantial; 0.81–1.0 = Almost perfect19. The Benjamini–Hochberg (BH) procedure was applied to control for the false-discovery rate, using a q-value of 0.05.
Data analyses were performed using IBM SPSS statistics software, version 27.0 (IBM Corporation, Armonk, New York; USA), and R, version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria). The figure is presented in a color-blind friendly color-scheme20.
Ethics approval
This prospective study was approved by the ethical committee of the medical faculty of the Goethe-University Frankfurt.
Results
The trial included 1528 EEG recordings. The patients’ median age was 55 years (IQR 21.5–88.5; range 15–95), and 51.1% were women (Table 1). The majority of the EEG recordings (1039, 68%) were obtained from very collaborative patients and contained minimal artifacts. EEGs were performed primarily due to epilepsy in 698 cases (45.7%). A total of 909 (59.5%) recordings were performed in patients who had experienced at least one epileptic seizure, and 619 (40.5%) patients did not have any epilepsy-related diagnoses. Among patients who had experienced at least one epileptic seizure, 497 had focal seizures: with temporal onset in 184, frontal onset in 139, parietal onset in 52, occipital onset in 12, multifocal in 57, and lateral onset without further lobe specification in 53; in the remaining 315 patients, seizure onset was unknown or not documented.
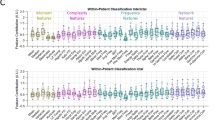
The measured IRA values between neurophysiologists and EEG technologists are shown in Table 2, and the proportions of true positive (TP), true negative (TN), false negative (FN), and false positive (FP) readings by the EEG technologies for the primary EEG feature is presented in Fig. 1. The IRA was scored “almost perfect” for seizure and SE detection (AC1 = 0.97 for both). The EEG technologists were able to diagnose these features with high negative-predictive value (NPV, for both, 99%; 95% CI 98–99%) but low positive predictive value (PPV, 35%; 95% CI 25–38% for seizures; 48%; 95% CI 43–74% for SE). Global conclusion, dichotomized as normal versus pathologic, demonstrated “substantial” IRA (AC1 = 0.71), and EEG technologists were able to identify normal EEGs with 72% (95% CI 68–76%) PPV and 89% (95% CI 87–91%) NPV. Globally, EEG technologists detected ictal elements with a very low FN rate and a high FP percentage (Table 2).

Percentages of true positives (in dark green; EEG patterns coded “yes” by both EEG technologists and neurophysiologists), true negatives (in light green; EEG patterns coded “no” by both EEG technologists and neurophysiologists), false positives (in orange; exams coded “yes” by EEG technologists and “no” by neurophysiologists), and false negatives (in red; exams coded “no” by EEG technologists and “yes” by neurophysiologists). FN False negative, FP false positive, TP true positive, TN true negative, IEDS interictal epileptiform discharges, PDR posterior dominant rhythm, SE status epilepticus, Sz seizures.
We then investigated which factors might influence EEG technologists’ reading abilities (Table 3). In intubated patients, EEG technologists tended to over-diagnose SE (FP rate 8% vs 1.3%, p < 0.001, significant after BH correction), while seizure detection was not affected. In contrast, in patients with known epilepsy, EEG technologists detected SE accurately but presented significantly increased FP for seizure detection (2.9% versus 0.7%, p = 0.001, significant after BH correction). SE diagnosis showed a significantly reduced IRA in older patients (p < 0.001, significant after BH correction), with EEG technologists demonstrating more FP among patients older than 60 years (3.3% versus 0.7%, p < 0.001, significant after BH correction). Patient cooperation significantly influenced EEG technologists’ performances. In poorly cooperating patients, EEG technologists displayed higher rates of FN seizure detection and higher FN and FP SE detection compared with cooperative patients (for all, p < 0.001 significant after BH correction). Among patients with a known history of craniotomy and among patients older than 60 years, the global conclusion showed significantly fewer FN results (i.e., EEG incorrectly coded as “pathological” by EEG technologists; for both p < 0.001, significant after BH correction). Similarly, poorer cooperation was associated with lower global conclusion rates. EEG indication (primary epileptic versus non-epileptic) and patient´s gender did not appear to affect the various studied parameters.
Among the 725 patients with epilepsy diagnoses, epilepsy etiology did not influence seizure detection or the assessment of PDR or slowing. However, epilepsy etiology significantly altered the SE detection agreement rate (p = 0.002, significant after correction for multiple comparison), with neurophysiologist and EEG technologists presenting 97.8% agreement (n = 81) for patients with genetic epilepsy, 99.5% (n = 194) for patients with epilepsy of unknown etiology, and 94.6% (n = 421) among patients with symptomatic epilepsy. Global conclusion presented with significantly lower FN rates (i.e., EEG incorrectly coded as “pathological” by EEG technologists) among patients with symptomatic etiologies (p < 0.001; FN: 12.2%, n = 10 in genetic epilepsy; 14.9%, n = 29 in unknown etiologies; and 4.0%, n = 18 in symptomatic epilepsy).
Among patients who had previously experienced at least one epileptic seizure, none of the investigated EEG features significantly differed according to seizure semiology. Among patients with focal seizures, the EEG technologists’ reading performances, particularly for the detection of seizures, SE, or IEDs, did not differ according to the epileptic focus.
To check for a training effect, we divided our data into two time-periods (EEGs recorded during the 1st and the 2nd half of the study). We did not observe any effect regarding the overall conclusions, presence of seizure, slowing, or preserved PDR.
Discussion
To our knowledge, this is the first study to prospectively investigate the reliability of EEG technologists’ reading performances in a large and heterogeneous population. EEG-technologists and neurophysiologists presented “substantial” IRA for overall EEG conclusion and “almost-perfect” IRA for seizures and SE detection. EEG technologists were able to identify normal EEG patterns with good sensitivity and specificity and detected ictal features (SE and seizures) with excellent NPV but low PPV. Intubation, older age, known epilepsy history, and poor cooperation might potentially alter the EEG technologists’ reading performances.
The IRA for SE and seizure detection was “almost perfect” (PA: 97% and AC1: 0.97 for both). A Canadian study investigated the IRA between experts and 16 neurological residents with brief training in ACNS terminology13. They reported “almost perfect” IRA for seizures but with slightly lower PA and Gwet-AC1 values than those found in our study (PA: 86.4%, AC1: 0.82). Although comparisons between studies should always be made with caution, these results suggested that, at least for ictal pattern detection, EEG technologists’ performances were similar to those of neurological residents. In many centers, in the absence of immediate availability of a certified neurophysiologist (for example at night or during weekends) clinical decisions are made upon neurological residents’ conclusion. Our results suggest that EEG-technologists conclusion might be similarly used.The identification of IEDs was associated with 78% PA and “substantial” IRA, which were in line with the results of a recent study investigating IED detection reliability among experts; who reported 80.9% PA and 69.4% kappa for the determination of whether an EEG contained any IEDs11. One study investigating the performance of automatic spike detection used three senior EEG technologists as alternate gold standards21. Although the IRA among readers was not formally assessed in that study, only 13.2% of the IEDs were detected by all three readers with FP/min ranging between 0.80 ± 1.61 and 1.99 ± 5.15, and sensitivity ranging between 40% and 51.5%21. Because the design of that study was very different from ours, the comparison between these results and our IED detection sensitivity proves difficult.
One striking result was the high specificity demonstrated by EEG technologists for the identification of ictal patterns. EEG technologists were able to diagnose seizures and SE with extremely low FN rates, suggesting that the physicians in charge can be reassured when EEG technologists report the absence of such patterns. However, this high NPV was counterbalanced by a low PPV, which should warn treating neurologists against starting any medications prior to examining the EEG for themselves. Among our cohort, the FP rate for seizures and SE diagnoses was above 50%. EEG overdiagnosis can lead to inappropriate epilepsy diagnoses, which is a well-known problem, even among neurologists, with up to 30% of the patients who are referred to epilepsy centers for refractory seizures eventually being diagnosed with no evidence of epilepsy22,23,24,25,26,27. Few data are available regarding the EEG reading accuracy of non-neurophysiologists. ICU physicians demonstrated limited (approximately 50%) sensitivity but good specificity (approximately 88%) for the identification of seizures28,29. However, because these studies focused on specific ICU populations (prognostication after cardiac arrest and recent clinical seizures), used simplified cEEG montages, and detected seizures based on amplitude-integrated EEGs (aEEGs), their results are difficult to compare with ours. The diagnosis of non-convulsive SE (NCSE) has been reported to be challenging, with experienced neurophysiologists presenting only “moderate” IRA and 47% PPV30. Unfortunately, because SE type was not recorded for study purposes in our population, we were unable to assess the contribution of NCSE to our FP rate.
We identified several factors that might influence the performances of EEG technologists and possibly other EEG readers. Patients with a known history of epilepsy presented with higher FP rates for seizure diagnoses, which is not surprising as “looking too hard” is a well-known cause of EEG overreading. The identification and analysis of overread patterns were beyond the scope of this study. Previous studies described “wicket spikes” and fluctuations in background activity with temporal phase reversal as the most frequently overread patterns23,25,31. Agreement regarding SE diagnoses was significantly lower among older patients. Several hypotheses can be made to explain this finding. First, NCSE, which is known to be more challenging to diagnose, is more common in the elderly32. Second, both ictal manifestations and interictal EEG findings are known to change with age, making the diagnosis of ictal features potentially more difficult among the older population33. However, the identification of seizures and IEDs was not altered by age in the present study. Additionally, the differential diagnosis of seizures or SE in older patients is particularly wide, and IEDs have been reported in up to 30% of patients with nonepileptic events, often leading to the inappropriate prescription of antiseizure medication26,32,33.
EEG indication goes beyond epilepsy, seizure diagnosis, or SE assessment. Around half of the EEGs were asked for non-epileptic reasons such as prognostication in patients with disorder of consciousness. As patients outcome were not available in the present study, the prognostication ability between EEG-technologist and neurophysiologist could unfortunately not be assessed. However, EEG-technologists reading ability, including features involved in prognostication assessment such as the presence of slowing or preservation of PDR, did not differ between EEG recorded for epileptic or non-epileptic reasons, suggesting that EEG-technologists may also contribute to these patients’ management.
In contrast with most previous studies investigating IRA, EEG readings were performed under “real-life conditions” in this study. Therefore, EEG technicians did not receive any specific training for the purposes of the study. Furthermore, as usual, EEG technicians read the EEGs at the patient’s bedside during the recording. Therefore, in addition to the EEG interpretation, they were also responsible for the patient’s care and the technical aspects of the recording. Furthermore, they had a limited amount of time (duration of the recording) to finalize their interpretations. On the other hand, neurophysiologists could read EEGs at their own rhythm.
These likely influenced our results and should be taken into account when interpreting them. In cases of doubt, without time to extensively examine the recording, EEG-technologists may have erred on the side of “overinterpretation” to draw neurophysiologists’ attention, contributing to the high FP rate. However, this “real-life design” might improve the clinical relevance in the everyday practice of our results.
In the absence of baseline evaluation, strong conclusions regarding a potential benefit of a checklist in routine clinical practice cannot be drawn. We did not observe any effect regarding the overall conclusions, presence of seizure, slowing, or preserved PDR. Furthermore, standardized EEG assessment, in which the readers were asked to assess specific EEG-features by choosing from a list of pre-defined terms, had already demonstrated to improve IRA10,34,35,36. Similarly, in other medical fields, it has been demonstrated that standardized assessment with use of predefined terms contributes to higher IRA37.
Some limitations of this study must be acknowledged. Our study included only routine EEG, with low numbers of SE and seizure recordings. This low number of ictal-events, with therefore low numbers of FN and FP, must be considered during the interpretation of our results, especially the analysis regarding potentials factors that may impair EEG-technologists reading performances. Furthermore, during cEEG, a “learning effect” may exist that would consequently lower the false positive rate. Because all EEG readers in this study (both neurophysiologists and EEG technologists) worked at a single academic center, our results do not necessarily represent the diversity of skills and knowledge among the community. Furthermore, all EEG-technologists at our center were certified in neurophysiological diagnostics (three years of specialized training including both theoretical and practical formation). As EEG technologist training varies between countries, this may impair the generalization of our results. Furthermore, our data came from one single tertiary hospital with specialized neuro-ICU and referral hospital for epilepsy surgery and neuro-oncological management. The proportion of patients who underwent prior craniotomy is therefore higher than the one expected in other centers without a neurosurgery department on site.One obvious limitation is the absence of a “true gold-standard test.” Interpretations by our certified neurophysiologists were considered to be correct without further formal assessments and without any “second-look” of EEG with discrepant interpretation between neurophysiologists and technologists. However, as part of the standard care at our institution, recordings with doubtful findings are discussed among various interpreters until a consensus is reached. Finally, as previously mentioned, the design of the study did not allow for the determination of which readers disagreed with specific EEGs.
Conclusion
EEG indications are continually expanding, and the use of cEEG has increased. In this context, trained EEG technologists who are able to identify and recognize EEG abnormalities are essential, allowing them to alert physicians for timely interpretations and take necessary clinical actions. Indeed, credentialed EEG technologists have demonstrated the ability to improve patient management and outcomes38. In our study, EEG technologists demonstrated a “moderate” to “almost-perfect” IRA with neurophysiologists. EEG technologists were able to identify pathological features, especially ictal EEGs (SE, seizures), with almost no FNs, at the cost of a relatively high FP rate, the latter might be due to an “overinterpretation” by EEG technologists to draw neurophysiologists' attention. Physicians in charge should be able to rely on EEG technologists’ initial interpretations when they report the absence of ictal patterns but should always verify the EEG traces before taking medical action when ictal patterns are reported.
Data availability
Anonymized data can be shared upon reasonable request by the corresponding author.
Code availability
All code used is available as part of SPSS, version 27 (IBM Corp., Armonk, NY, USA) and/or R, version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria).
References
Fisher, R. S. et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 58, 522–530. https://doi.org/10.1111/epi.13670 (2017).
Scheffer, I. E. et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 58, 512–521. https://doi.org/10.1111/epi.13709 (2017).
Rosenow, F. et al. Status epilepticus im Erwachsenenalter, S2k-Leitlinie, 2020, in: Deutsche Gesellschaft für Neurologie (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie. (Accessed December 2020); www.dgn.org/leitlinien.
Trinka, E. et al. A definition and classification of status epilepticus—Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia 56, 1515–1523. https://doi.org/10.1111/epi.13121 (2015).
Strzelczyk, A. et al. Costs length of stay and mortality of super-refractory status epilepticus: A population-based study from Germany. Epilepsia 58, 1533-1541. https://doi.org/10.1111/epi.13837 (2017).
Herman, S. T. et al. Consensus statement on continuous EEG in critically ill adults and children, part I: Indications. J. Clin. Neurophysiol. 32, 87–95. https://doi.org/10.1097/WNP.0000000000000166 (2015).
Rossetti, A. O., Rabinstein, A. A. & Oddo, M. Neurological prognostication of outcome in patients in coma after cardiac arrest. Lancet Neurol. 15, 597–609. https://doi.org/10.1016/S1474-4422(16)00015-6 (2016).
Kane, N. et al. A revised glossary of terms most commonly used by clinical electroencephalographers and updated proposal for the report format of the EEG findings. Revision 2017. Clin. Neurophysiol. Pract. 2, 170–185. https://doi.org/10.1016/j.cnp.2017.07.002 (2017).
Hirsch, L. J. et al. American Clinical Neurophysiology Society’s Standardized Critical Care EEG Terminology: 2012 version. J. Clin. Neurophysiol. 30, 1–27. https://doi.org/10.1097/WNP.0b013e3182784729 (2013).
Gaspard, N. et al. Interrater agreement for Critical Care EEG Terminology. Epilepsia 55, 1366–1373. https://doi.org/10.1111/epi.12653 (2014).
Jing, J. et al. Interrater reliability of experts in identifying interictal epileptiform discharges in electroencephalograms. JAMA Neurol. 77, 49–57. https://doi.org/10.1001/jamaneurol.2019.3531 (2020).
Mani, R., Arif, H., Hirsch, L. J., Gerard, E. E. & LaRoche, S. M. Interrater reliability of ICU EEG research terminology. J. Clin. Neurophysiol. 29, 203–212. https://doi.org/10.1097/WNP.0b013e3182570f83 (2012).
Zhuo Ding, J. et al. Resident training and interrater agreements using the ACNS critical care EEG terminology. Seizure 66, 76–80. https://doi.org/10.1016/j.seizure.2019.02.013 (2019).
Sanders, S., Rowlinson, S., Manidakis, I., Ferrie, C. D. & Koutroumanidis, M. The contribution of the EEG technologists in the diagnosis of Panayiotopoulos syndrome (susceptibility to early onset benign childhood autonomic seizures). Seizure 13, 565–573. https://doi.org/10.1016/j.seizure.2004.01.006 (2004).
Gavvala, J. et al. Continuous EEG monitoring: A survey of neurophysiologists and neurointensivists. Epilepsia 55, 1864–1871. https://doi.org/10.1111/epi.12809 (2014).
Walter, U., Noachtar, S. & Hinrichs, H. Digital electroencephalography in brain death diagnostics: Technical requirements and results of a survey on the compatibility with medical guidelines of digital EEG systems from providers in Germany. Nervenarzt 89, 156–162. https://doi.org/10.1007/s00115-017-0431-y (2018).
Leitinger, M. et al. Salzburg consensus criteria for non-convulsive status epilepticus—Approach to clinical application. Epilepsy Behav. 49, 158–163. https://doi.org/10.1016/j.yebeh.2015.05.007 (2015).
Gwet, K. L. Computing inter-rater reliability and its variance in the presence of high agreement. Br. J. Math. Stat. Psychol. 61, 29–48. https://doi.org/10.1348/000711006X126600 (2008).
Landis, J. R. & Koch, G. G. The measurement of observer agreement for categorical data. Biometrics 33, 159–174. https://doi.org/10.2307/2529310 (1977).
Wong, B. Color blindness. Nat. Methods 8, 441. https://doi.org/10.1038/nmeth.1618 (2011).
Scheuer, M. L., Bagic, A. & Wilson, S. B. Spike detection: Inter-reader agreement and a statistical Turing test on a large data set. Clin. Neurophysiol. 128, 243–250. https://doi.org/10.1016/j.clinph.2016.11.005 (2017).
Behrouz, R., Heriaud, L. & Benbadis, S. R. Late-onset psychogenic nonepileptic seizures. Epilepsy Behav. 8, 649–650. https://doi.org/10.1016/j.yebeh.2006.02.003 (2006).
Benbadis, S. R. Errors in EEGs and the misdiagnosis of epilepsy: Importance, causes, consequences, and proposed remedies. Epilepsy Behav. 11, 257–262. https://doi.org/10.1016/j.yebeh.2007.05.013 (2007).
Benbadis, S. R. & Lin, K. Errors in EEG interpretation and misdiagnosis of epilepsy. Which EEG patterns are overread?. Eur. Neurol. 59, 267–271. https://doi.org/10.1159/000115641 (2008).
Benbadis, S. R. & Tatum, W. O. Overintepretation of EEGs and misdiagnosis of epilepsy. J. Clin. Neurophysiol. 20, 42–44. https://doi.org/10.1097/00004691-200302000-00005 (2003).
McBride, A. E., Shih, T. T. & Hirsch, L. J. Video-EEG monitoring in the elderly: A review of 94 patients. Epilepsia 43, 165–169. https://doi.org/10.1046/j.1528-1157.2002.24401.x (2002).
Uldall, P., Alving, J., Hansen, L. K., Kibaek, M. & Buchholt, J. The misdiagnosis of epilepsy in children admitted to a tertiary epilepsy centre with paroxysmal events. Arch. Dis. Child. 91, 219–221. https://doi.org/10.1136/adc.2004.064477 (2006).
Nitzschke, R., Muller, J., Engelhardt, R. & Schmidt, G. N. Single-channel amplitude integrated EEG recording for the identification of epileptic seizures by nonexpert physicians in the adult acute care setting. J. Clin. Monit. Comput. 25, 329–337. https://doi.org/10.1007/s10877-011-9312-2 (2011).
Lybeck, A. et al. Bedside interpretation of simplified continuous EEG after cardiac arrest. Acta Anaesthesiol. Scand. 64, 85–92. https://doi.org/10.1111/aas.13466 (2020).
Goselink, R. J. M. et al. The difficulty of diagnosing NCSE in clinical practice; external validation of the Salzburg criteria. Epilepsia 60, e88–e92. https://doi.org/10.1111/epi.16289 (2019).
Benbadis, S. R. et al. Interrater reliability of EEG-video monitoring. Neurology 73, 843–846. https://doi.org/10.1212/WNL.0b013e3181b78425 (2009).
Manfredonia, F., Saturno, E., Lawley, A., Gasverde, S. & Cavanna, A. E. Prevalence and clinical correlates of non-convulsive status epilepticus in elderly patients with acute confusional state: A systematic literature review. J. Neurol. Sci. 410, 116674. https://doi.org/10.1016/j.jns.2020.116674 (2020).
Thomas, R. J. Seizures and epilepsy in the elderly. Arch. Intern. Med. 157, 605–617 (1997).
Beniczky, S. et al. Standardized computer-based organized reporting of EEG: SCORE. Epilepsia 54, 1112–1124. https://doi.org/10.1111/epi.12135 (2013).
Gerber, P. A. et al. Interobserver agreement in the interpretation of EEG patterns in critically ill adults. J. Clin. Neurophysiol. 25, 241–249. https://doi.org/10.1097/WNP.0b013e318182ed67 (2008).
Stroink, H. et al. Interobserver reliability of visual interpretation of electroencephalograms in children with newly diagnosed seizures. Dev. Med. Child. Neurol. 48, 374–377. https://doi.org/10.1017/S0012162206000806 (2006).
Ellis, D. W. & Srigley, J. Does standardised structured reporting contribute to quality in diagnostic pathology? The importance of evidence-based datasets. Virchows Arch. 468, 51–59. https://doi.org/10.1007/s00428-015-1834-4 (2016).
Agostini, S. D. & Bonner, A. M. The value of the neurodiagnostic professional in patient care. Neurodiagn. J. 55, 227–234. https://doi.org/10.1080/21646821.2015.1109425 (2015).
Acknowledgements
The authors thank all EEG technologists from the Epilepsy Center Frankfurt Rhine-Main for their participation in the study and assistance with data acquisition.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by a LOEWE Grant from the State of Hessen for the “Center for Personalized Translational Epilepsy Research” (CePTER), Goethe University Frankfurt, Frankfurt am Main, Germany.
Author information
Authors and Affiliations
Contributions
I.B.: Analysis and interpretation of data. Preparation of tables and figures. Drafting the manuscript. Critical revision of the manuscript for important intellectual content. S.A.: Conception and design of the study. Acquisition of the data. Critical revision of the manuscript for important intellectual content. P.R.: Conception and design of the study. Acquisition of the data. Critical revision of the manuscript for important intellectual content. N.S.: Acquisition of the data. Critical revision of the manuscript for important intellectual content. F.R.: Acquisition of the data. Critical revision of the manuscript for important intellectual content. A.S.: Conception, design, and supervision of the study. Acquisition of the data. Critical revision of the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
IB: reports a research grant from the Swiss National Science Foundation. SA: reports no conflict of interest. PSR: reports personal fees from Eisai. NS: reports no conflict of interest. FR: reports personal fees from Arvelle Therapeutics, Eisai, GW Pharmaceuticals, Novartis, Medtronic, and UCB, and grants from the Detlev-Wrobel-Fonds for Epilepsy Research, the Deutsche Forschungsgemeinschaft, the LOEWE Program of the State of Hesse, and the European Union. AS: reports personal fees and grants from Arvelle Therapeutics, Desitin Arzneimittel, Eisai, GW Pharmaceuticals companies, LivaNova, Marinus Pharma, Medtronic, UCB, and Zogenix.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
41598_2021_92827_MOESM2_ESM.docx
Supplementary Figure 1. EEG interpretation sheet. The left column was first filled by EEG-technologists during EEG recording and the right column was completed by neurophysiologists blinded to the EEG-technologists interpretation (two sheets pro patients were used). IEDs = Interictal Epileptiform discharges.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Beuchat, I., Alloussi, S., Reif, P.S. et al. Prospective evaluation of interrater agreement between EEG technologists and neurophysiologists. Sci Rep 11, 13406 (2021). https://doi.org/10.1038/s41598-021-92827-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-92827-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
