
Abstract
HLA class II (HLA-II) genes’ polymorphism influences the immune response to Chlamydia trachomatis (Ct), it is considered a sexually transmitted infection. However, associations between HLA-II alleles and Ct-infection have been little explored in humans; this study was thus aimed at determining HLA-DRB1-DQB1 alleles/haplotypes’ effect on Ct-infection outcome in a cohort of Colombian women. Cervical sample DNA was used as template for detecting Ct by PCR and typing HLA-DRB1-DQB1 alleles/haplotypes by Illumina MiSeq sequencing. Survival models were adjusted for identifying the alleles/haplotypes’ effect on Ct-outcome; bioinformatics tools were used for predicting secreted bacterial protein T- and B-cell epitopes. Sixteen HLA-DRB1 alleles having a significant effect on Ct-outcome were identified in the 262 women analysed. DRB1*08:02:01G and DRB1*12:01:01G were related to infection-promoting events. Only the DQB1*05:03:01G allele related to clearance/persistence events was found for HLA-DQB1. HLA-DRB1 allele homozygous women were associated with events having a lower probability of clearance and/or early occurrence of persistence. Twenty-seven peptides predicted in silico were associated with protective immunity against Ct; outer membrane and polymorphic membrane protein-derived peptides had regions having dual potential for being T- or B-cell epitopes. This article describes HLA-DRB1-DQB1 alleles/haplotypes related to Ct-infection resolution and the peptides predicted in silico which might probably be involved in host immune response. The data provides base information for developing future studies leading to the development of effective prevention measures against Ct-infection.
Similar content being viewed by others


Introduction
Chlamydia trachomatis (Ct) is the commonest bacteria-related, sexually-transmitted infection (STI) worldwide1; the WHO’s Report on global sexually transmitted infection surveillance estimated that there are 127 million new cases annually2. Most Ct infections have an asymptomatic clinical course, but some might lead to severe complications, such as pelvic inflammatory disease (PID) and recurrent abortions1.
Ct mainly affects 18–20 year-old women and 20–24 year-old men, asymptomatic cases mainly occurring in women (close to 90%)3; however, symptomatic infections usually occur weeks or months after exposure. Abundant secretion, dysuria and postcoital bleeding are amongst the commonest symptoms3.
Previous studies have revealed that late detection of Ct asymptomatic infection (together with other agents such HPV) could lead to conditions such as squamosas cell carcinoma and cervical cancer (CC)4. It has been shown that a fourth of Ct infections become spontaneously resolved and without treatment; factors, such as host immune response, thus significantly contribute towards eliminating genital tract infection5.
The major histocompatibility complex (MHC) is a mechanism greatly determining infections’ clinical course; establishing its role in Ct infection dynamics would thus explain their outcome5. Some studies have suggested the relationship between class II HLA alleles, Ct and tubal factor infertility (TFI)6 as DQA*03:01, DQA*05:01 and DQB*04:02 have been described as being associated with Ct and DRB1*75:03 and DRB5*01:01 with TFI6.
An efficient immune response against intracellular pathogens like Ct requires cell-mediated immunity, this being stimulated by bacterial peptides presented to T-cells by the MHC7. Predicting these molecules and establishing their potential role in the natural history of Ct infection could contribute towards understanding its dynamics8.
Studies have searched for prophylactic interventions; most have evaluated the immune response in mice experimentally infected by Ct or C. muridarum9,10. Murine model studies have demonstrated the importance of an HLA class II molecule-mediated immune response regarding bacterial infection resolution11. However, few studies have comprehensively evaluated HLA alleles’ role regarding human Ct infection outcome and the peptides probably related to immune response10,12. This study was thus aimed at determining HLA-DRB1-DQB1 alleles/haplotypes’ effect on Ct infection, persistence, clearance and redetection in a cohort of Colombian women. The results provided information for developing suitable prevention measures for managing and controlling Ct infection.
Results
HLA-DRB1-DQB1 allele effects on Ct outcome
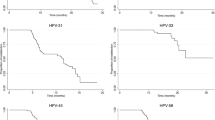
The demographic characteristics of 262 women complying with the retrospective study’s inclusion criteria were analysed; mean age was 41.7 years-old (23.1 SD) and median age at onset of sexual life 18.0 years-old (4.0 IQR) (Table 1). Ct was detected retrospectively; study results gave the highest rate for persistence events (26.0 per 100 women/month), followed by clearance (16.1 per 100 women/month) and redetection events (15.6 per 100 women/month) (Supplementary Fig. S1). Survival data was estimated (using Kaplan Meier survival functions) for each event; Fig. 1 shows the probability of Ct infection, clearance, persistence and redetection risk throughout the follow-up period.

Kaplan–Meier estimator for evaluating Ct infection, clearance, persistence and redetection.
Forty-seven HLA-DRB1 alleles were found using Illumina MiSeq sequencer whose frequency distribution has been previously published13. The DRB1*04:07:01G allele had the greatest prevalence in the target population (Supplementary Table S1); this allele has been categorised as a common allele and has been reported in all continents’ populations14. Multivariate models (parametric and semiparametric) were constructed for identifying data associated with Ct outcomes; they were adjusted to fit the covariables associated with outcomes in univariate analysis (Supplementary Table S2).
Sixteen DRB1 alleles had a statistically significant p value, indicating their possible effect regarding a particular infection event (greater probability (GP), earlier occurrence (EO), later occurrence (LO) and lower probability (LP) (Table 2 and Supplementary Tables S3 and S4). Interestingly, three alleles were related to more than one event; DRB1*08:02:01G and DRB1*12:01:01G had concordant effects (GP for persistence and EO for redetection and LO for infection and GP for clearance) while DRB1*14:02:01G had an opposite effect (LO for infection and GP for persistence) (Table 2). Fourteen HLA-DQB1 alleles were identified in the target population (Supplementary Table S1), of which only DQB1*05:03:01G had a statistically significant p value related to clearance and persistence events, having a GP effect for both (Table 2 and Supplementary Tables S5 and S6). It was also found that HLA-DRB1 homozygous women had a LP effect on clearance and an EO effect related to persistence events, suggesting that this characteristic could represent a genetic disadvantage for its carriers as it makes them more susceptible to Ct infection. However, more experimental evidence is required to confirm such hypothesis.
HLA-DRB1-DQB1 haplotype effect on Ct outcome
Forty-seven of the 142 DRB1-DQB1 haplotypes had statistically significant values when analysing the effect of each haplotype on Ct outcome (Table 3). Twenty-seven associations were found regarding infection events; 16 related to the event (GP/EO) (e.g. DRB1*01:02:01G-DQB1*03:03:02G) whilst 11 associations did not (LO) (e.g. DRB1*12:01:01G-DQB1*03:02:01G). DRB1*09:01:02G-DQB1*03:01:01G and DRB1*12:01:01G-DQB1*03:02:01G had an EO effect on clearance whilst DRB1*04:05:01-DQB1*03:01:01G was associated with LP (Table 3 and Supplementary Table S7).
Eighteen associations were found regarding persistence; sixteen of them related to the event (GP/EO), DRB1*04:05:01-DQB1*03:01:01G and DRB1*11:01:01G-DQB1*03:02:01G having the greatest effect. By contrast, DRB1*10:01:01G-DQB1*05:01:01G and DRB1*14:02:01G-DQB1*05:01:01G reduced persistence (LP/LO). Eight haplotypes were related to redetection events (Table 3 and Supplementary Table S8).
Nine haplotypes were related to more than one event when analysed; 6 were related to some infection events, such as EO for DRB1*04:05:01-DQB1*02:01:01G on infection and redetection, LO for DRB1*12:01:01G-DQB1*03:02:01G on infection and GP on clearance;
whilst others had an opposite effect on events, LO of DRB1*01:01:01G-DQB1*03:01:01G infection and EO on persistence (Table 3).
In silico predicted peptides associated with Ct events
Peptides derived from proteins predicted as being secreted (Supplementary Table S9) were predicted in silico since it has been shown that they could be associated with protective immunity or susceptibility to Ct infection7,10. Fifteen out of 24 proteins had peptides having T-cell epitopes binding strongly to HLA-II-DRB1 but not to -DQB1 molecules (Supplementary Tables S10 to S24). Some peptides might have been related to increased susceptibility against Ct as they were associated with GP and EO effects related to persistence or redetection events. Twenty-seven peptides were related to protection (of which 7 were OMP-derived and 17 from PMP) since they were associated with effects related to Ct elimination (LO of infection, GP of clearance and LP of persistence) (Supplementary Tables S10 to S24). Interestingly, 11 of them had potential B-cell epitope regions, thus highlighting their possible role as cell and/or humoral immune response mediators (Table 4).
Discussion
Ct is the commonest sexually-transmitted bacterial pathogen worldwide; it can provoke serious consequences regarding reproductive sexual health once it becomes a chronic infection. Despite significant advances having been made regarding its control, clear and effective tools for reducing its impact on public health are still not available. Therefore, comprehensively evaluating a Ct infection dynamics-related immune response represents an alternative approach for developing effective control tools15,16.
This study was focused on comprehensively investigating (the first time) the effect of HLA-DRB1-DQB1 alleles on Ct infection outcome, given that it has been shown that HLA molecules could be related to Ct-induced diseases, such as trachoma17, PID6,18 and infertility19,20, or be associated with infection prevalence and bacterial reinfection8,21,22. It was found that HLA-DRB1 alleles were associated with cervical-related Ct infection outcome (Tables 2 and 3). Some alleles were less common for this locus and occurred at lower frequency in the target population. MHC-pathogen coevolution models indicate that less commonly occurring alleles provide greater protection against pathogens than more commonly occurring ones to which pathogens may have become adapted23,24.
DQB1*05:03:01G was only associated with Ct clearance and persistence events (Table 2); however, previous studies have reported HLA-DQB1 (DQB1*06 and DQB1*04:02) alleles’ association with Ct infection and reinfection and increased bacterial persistence marker cHSP608,21,22. Such discrepancy could be explained by the genetic background of the particular population being studied (African compared to South-American in this study) thereby contributing to modulating an immune response to bacterial infection6,25. However, these alleles only had similar associations to those reported in previous studies when configured as haplotypes, i.e. when they have been combined with a DRB1 allele (Table 3).
LP of clearance and EO of persistence were found for homozygous HLA-DRB1 (Supplementary Tables S3 and S4). It has been reported that homozygosity is related to susceptibility to infection whilst heterozygosity is associated with a higher probability of eliminating it, possibly due to a greater immune response, given the broader amount of HLA-II restricted epitopes that can be presented to T-cells24,26,27. It is worth noting that findings regarding alleles causing effects on events promoting or reducing infection (Table 2) are useful when designing Ct infection control strategies; for example, considering peptides presented by DRB1*12:01 could represent a good strategy since it is associated with events related to infection resolution whilst peptides presented by DRB1*08:02 should be avoided as it is related to events associated with infection, such as persistence and redetection.
It has been suggested that Ag presentation during adaptative response could be an important mechanism for controlling Ct infection8,28; identifying T-cell antigens able to stimulate protection-inducing immunity is thus the key for developing anti-Ct vaccines29. Analysing Ct molecules’ T-cell epitopes (Supplementary Tables S10 to S24) whose role in protection-inducing immunity was experimentally evaluated10 revealed that 3-oxoacyl-[acyl-carrier protein] reductase had a peptide related to a GP of Ct clearance (Table 4). This peptide had been found in an immunoproteomics study demonstrating that inoculating dendritic cells previously pulsed with a peptide mixture (including the peptide discussed here) triggered a response partially protecting mice from intranasal and genital tract Chlamydia infection30. It has been demonstrated that CPAF-derived peptides could be related to a protection-inducing effect in a HLA-DR4 (HLA-DRB1*04:01) transgenic mouse model31, however, no allele/peptide association was found in this study (Supplementary Table S12), possibly due to the allele’s low frequency in the studied population (less than 0.2%), suggesting an allele-specific effect.
The OMPs and PMPs had various regions containing T-cell epitopes, the most important ones being related to events associated with Ct infection elimination (Table 4). Interestingly, there was discrepancy amongst several events which could have been explained by binding core mutations for some PMP-derived peptides (PMP-B and PMP-F); these enabled discriminating between invasive (L2 and LGV) and non-invasive variants (A, B, C, D, E, F, H, J, Ja and La) (Supplementary Table S16 and S18).
It has been reported recently that the Ct OMP (CTH522) protein being evaluated in phase 1 trials was able to trigger a more consistent cell-mediated immune response profile after its immunisation using CAF01 liposomes compared to the placebo group, thus highlighting its potential usefulness as a vaccine candidate32. Such result, added to this study’s findings, supports the idea that T-cell epitopes derived from the antigens analysed here (mainly surface-derived molecules, particularly totally conserved ones) could be regions of interest for the future design of novel interventions aimed at controlling Ct infection.
In silico analysis suggested that some protection-related predicted peptides would specifically stimulate T-cells whilst others would stimulate both T- and B-cells (Table 4). Vaccination with various OMP serovars (D, E and F) has elicited an antibody (Ab) response neutralising bacteria in vitro33. Furthermore, PMPs can trigger an immune response against genital34 and ocular35 Chlamydia infection and a serological response in humans36. Mice vaccinated with DC/PMP-derived peptides (G, E and F) or with just immunogens in formulation have developed immunity against genital tract and pulmonary Chlamydia infection, significantly reducing bacteria in UFI assays7,37. Interestingly, phase 1 clinical trial vaccination using the Ct-OMP version showed accelerated seroconversion, increased IgG titres and enhanced mucosal profile, thus making CTH522 a promising candidate for further clinical development32.
As CD4 T-cells are essential for resolving primary genital infection38 and CD8 T-cells are important for eliminating Ct-infected cells by effector mechanisms39, then peptides stimulating both types of effector cells (B- and T), as predicted here, could be considered most suitable for controlling Ct infection and therefore as promising candidates for future studies (Table 4).
Antigenic peptides recognised by both CD4 and CD8 T-cells could be promising diagnostic and therapeutic tool candidates since one of the main limitations for developing an effective vaccine lies in identifying Ct epitopes capable of being recognised by both cell types40; an Ab-mediated immune response would reduce bacterial load, thereby facilitating further elimination of infection via a cell-mediated immune response33,40.
Considering this and given the in silico analysis performed here, it can thus be suggested that a universal anti-Ct vaccine should contain peptides having the following characteristics: they should induce immunity and be protein-derived, have a high degree of conservation, be associated with protection-related events (such as GP of clearance and LP of infection, redetection and persistence) and be able to stimulate T- and B-cell responses.
HLA-DRB1-DQB1 alleles/haplotypes having an effect on Ct resolution have thus been reported here, along with in silico predicted epitopes derived from protection-related proteins targeting Ct infection. However, functional read-outs for demonstrating the effect of presentation regarding the predicted antigens (i.e. wet-laboratory assays) were not performed here, thus failing to obtain a complete panorama of anti-Ct immune responses constitutes a limitation of this study.
Addressing new prophylactic and therapeutic targets must become a high priority as the tools used to date for Ct control have not had a significant impact on reducing bacterial infection load. Future analysis should be aimed at validating predicted epitopes’ immunogenic and immunological in vitro and in vivo properties and their safe and efficacy regarding humans. Such data will provide relevant knowledge for understanding the usefulness of peptides as a vaccine component and the influence of host factors on the clinical course of Ct infection.
Materials and methods
Study design and participants
A cohort was studied between 2007 and 2010; that previous study was aimed at determining the natural history of HPV infection in women from the Colombian cities of Bogotá, Girardot and Chaparral; all the women were attending hospital clinics as outpatients. The study’s objective was explained to them and they voluntarily accepted participating in the study by signing an informed consent form, as described previously13. Retrospective analysis inclusion criteria consisted of having available cervical samples for typing HLA-DRB1 and DQB1 and Ct detection, women having attended at least four follow-up sessions (one base line and three visits) and 6-monthly periods between visits (± 3 months).
The women filled in a survey form during each visit for compiling data regarding sociodemographic information and risk factors. Such information included data regarding whether they had received/used any type of treatment between visits; none of the women reported using antibiotics during follow-up. The women did not receive antibiotic treatment for Ct infections detected during the study, given the retrospective nature of Ct detection. The Universidad del Rosario’s School of Medicine and Health Sciences Research Ethics Committee approved the study (CEI-ABN026-000135). All procedures were performed in accordance with Helsinki Declaration guidelines.
Ct detection and HLA-DRB1-DQB1 typing
Previously obtained genomic DNA (gDNA)13,41 was used as template for detecting Ct by conventional PCR, amplifying a cryptic plasmid ORF2 segment from KL5/KL6 and KL1/KL2 primers41. An Illumina MiSeq (San Diego, CA, USA; Histogenetics, Ossining, NY, USA) sequencer was used for typing HLA alleles from DRB1-DQB1 loci exons 2 and 3; the IPD-IMGT/HLA database (https://www.ebi.ac.uk/ipd/imgt/hla) published in January 2018 (3.31.0) was used for assigning alleles13.
Statistical analysis
Qualitative variables were expressed as percentages. The Chi2 or Fisher’s exact tests were used for evaluating association/concordance amongst categorical variables. Continuous variables were expressed as means [with standard deviations (SD) for measure of dispersion] or medians [interquartile ranges (IQR)].
Ct infection was defined for this study’s purposes as PCR detection of bacterial DNA at any point during follow-up (2 years). Clearance was understood as the elimination of infection via a previous positive Ct result. A percentage of infections persisted before becoming eliminated; this event was evaluated in the study and was defined as Ct being detected during two or more consecutive follow-ups. Redetection was defined as bacterial detection after not having detected bacterial DNA during a previous follow-up.
Incidence rates for events were reported along with 95% confidence intervals (95%CI). The Kaplan–Meier estimator was used for estimating the probability of subjects continuing event-free. Cox proportional hazards models were constructed for evaluating outcome probability; such models’ coefficients were expressed as hazard rate (HR) and used for identifying alleles/haplotypes related to the evens being evaluated. Schoenfeld residuals were plotted to test the proportional hazard assumption; the covariables considered for the plot were those having p < 0.200 in univariate analysis (Supplementary Table S2). Variance inflation factor (VIF) and tolerance values were used for evaluating multicollinearity between covariables13.
Different parametric survival models were constructed when proportional hazards assumptions were not met. Akaike (AIC) and Bayesian (BIC) information criteria were used for selecting the models having the best fit. The Bonferroni method was used for correcting p-values for each model13. All two-tailed hypothesis tests (except those involved in constructing the models) were run with 0.05 significance. STATA14 software was used for analysis.
T- and B-cell epitope prediction
Ct variant-derived protein amino acid (aa) sequences (Supplementary Table S25) were downloaded from the PATRIC 3.5.11 database (https://www.patricbrc.org) and analysed first using classical pathway secretion predictor (SignalP 5.0)42 and those not assigned by this predictor were analysed by the non-classical one, SecretomeP 2.043.
The Technical University of Denmark’s Systems Biology Department’s Center for Biological Sequence Analysis’ NetMHCIIpan 3.2 server was used for assessing peptides having high predicted HLA-DRB1-DQB1 allele binding activity, i.e. proteins predicted as secreted44. Peptides having < 2.0% rank were considered to have strong binding. The BepiPred 2.0 tool (0.6 epitope threshold) was used for calculating B-cell epitopes derived from proteins whose peptides were associated with protection45.
Data availability
The datasets produced and/or analysed during this study are available from the corresponding author on reasonable request.
References
Nguyen, N. D. N. T. et al. Parenteral vaccination protects against transcervical infection with Chlamydia trachomatis and generate tissue-resident T cells post-challenge. NPJ Vaccines 5, 1–12 (2020).
WHO. Report on Global Sexually Transmitted Infection Surveillance. World Health Organization, Geneva, Switzerland. (2018).
Markle, W., Conti, T. & Kad, M. Sexually transmitted diseases. Prim. Care Clin. Off. Pract. 40, 557–587 (2013).
Fogue, P. et al. Molecular characterization of lower vaginal swabs for Human papilloma virus in association with Chlamydia trachomatis infection in Cameroonian women. J. Infect. Public Health 11, 314–320 (2018).
Geisler, W. M. et al. Epidemiological and genetic correlates of incident Chlamydia trachomatis infection in North American adolescents. J. Infect. Dis. 190, 1723–1729 (2004).
Ness, R. B., Brunham, R. C., Shen, C. & Bass, D. C. Associations among human leukocyte antigen (HLA) class II DQ variants, bacterial sexually transmitted diseases, endometritis, and fertility among women with clinical pelvic inflammatory disease. Sex. Transm. Dis. 31, 301–304 (2004).
Yu, H. et al. Chlamydia muridarum T cell antigens and adjuvants that induce protective immunity in mice. Infect. Immun. 80, 1510–1518 (2012).
Geisler, W. M., Tang, J., Wang, C., Wilson, C. M. & Kaslow, R. A. Epidemiological and genetic correlates of incident Chlamydia trachomatis infection in North American adolescents. J. Infect. Dis. 190, 1723–1729 (2004).
Hafner, L. M. & Timms, P. Development of a Chlamydia trachomatis vaccine for urogenital infections: novel tools and new strategies point to bright future prospects. Expert Rev. Vaccines 17, 57–69 (2018).
de la Maza, L. M., Zhong, G. & Brunham, R. C. Update on Chlamydia trachomatis vaccinology. Clin. Vaccine Immunol. 24, e00543 (2017).
Timms, P. & Hafner, L. Development of a vaccine for Chlamydia trachomatis: challenges and current progress. Vaccine Dev. Ther. 5, 45–58 (2015).
Zhong, G. & Brunham, R. C. Update on Chlamydia trachomatis vaccinology. Clin. Vaccine Immunol. 24, 1–25 (2017).
Del Rio-Ospina, L. et al. Identifying the HLA DRB1-DQB1 molecules and predicting epitopes associated with high-risk HPV infection clearance and redetection. Sci. Rep. 10, 7306 (2020).
Hurley, C. K. et al. Common, intermediate and well-documented HLA alleles in world populations: CIWD version 3.0.0. HLA 95, 516–531 (2020).
Unemo, M. et al. Sexually transmitted infections: challenges ahead. Lancet Infect. Dis. 17, e235–e279 (2017).
Ziklo, N., Huston, W. M., Hocking, J. S. & Timms, P. Chlamydia trachomatis genital tract infections: when host immune response and the microbiome collide. Trends Microbiol. 24, 750–765 (2016).
Conway, D. J. et al. HLA class I and II polymorphisms and trachomatous scarring in a Chlamydia trachomatis-endemic population. J. Infect. Dis. 174, 643–646 (1996).
Kimani, J. et al. Risk factors for Chlamydia trachomatis pelvic inflammatory disease among sex workers in Nairobi, Kenya. J. Infect. Dis. 173, 1437–1444 (1996).
Kinnunen, A. H. et al. HLA DQ alleles and interleukin-10 polymorphism associated with Chlamydia trachomatis-related tubal factor infertility: a case-control study. Hum. Reprod. 17, 2073–2078 (2002).
Cohen, C. R. et al. Immunogenetic correlates for Chlamydia trachomatis-associated tubal infertility. Obstet. Gynecol. 101, 438–444 (2003).
Gaur, L. K. et al. Association of Chlamydia trachomatis heat-shock protein 60 antibody and HLA class II DQ alleles. J. Infect. Dis. 180, 234–237 (1999).
Olson, K. M., Tang, J., Brown, L., Press, C. G. & Geisler, W. M. HLA-DQB1*06 is a risk marker for chlamydia reinfection in African American women. Genes Immun. 20, 69–73 (2019).
Borghans, J. A., Beltman, J. B. & De Boer, R. J. MHC polymorphism under host-pathogen coevolution. Immunogenetics 55, 732–739 (2004).
Hedrick, P. W. Pathogen resistance and genetic variation at MHC loci. Evolution 56, 1902–1908 (2002).
Mosaad, Y. M. Clinical role of human leukocyte antigen in health and disease. Scand. J. Immunol. 82, 283–306 (2015).
Blackwell, J. M., Jamieson, S. E. & Burgner, D. HLA and infectious diseases. Clin. Microbiol. Rev. 22, 370–385 (2009).
Burgner, D., Jamieson, S. E. & Blackwell, J. M. Genetic susceptibility to infectious diseases: Big is beautiful, but will bigger be even better?. Lancet Infect. Dis. 6, 653–663 (2006).
Brunham, R. C. Perspective: my 37 year journey through Chlamydia research: Chlamydia antigen analysis using monoclonal antibodies and major histocompatibility complex molecules. Pathog. Dis. 75, 1–9 (2017).
Brunham, R. C. & Rey-Ladino, J. Immunology of Chlamydia infection: implications for a Chlamydia trachomatis vaccine. Nat. Rev. Immunol. 5, 149–161 (2005).
Karunakaran, K. P. et al. Immunoproteomic discovery of novel T cell antigens from the obligate intracellular pathogen Chlamydia. J. Immunol. 180, 2459–2465 (2008).
Li, W. et al. A T cell epitope-based vaccine protects against chlamydial infection in HLA-DR4 transgenic mice. Vaccine 31, 5722–5728 (2013).
Abraham, S. et al. Safety and immunogenicity of the chlamydia vaccine candidate CTH522 adjuvanted with CAF01 liposomes or aluminium hydroxide: a first-in-human, randomised, double-blind, placebo-controlled, phase 1 trial. Lancet Infect. Dis. 19, 1091–1100 (2019).
Olsen, A. W., Follmann, F., Erneholm, K., Rosenkrands, I. & Andersen, P. Protection against Chlamydia trachomatis infection and upper genital tract pathological changes by vaccine-promoted neutralizing antibodies directed to the VD4 of the major outer membrane protein. J. Infect. Dis. 212, 978–989 (2015).
Karunakaran, K. P. et al. Outer membrane proteins preferentially load MHC class II peptides: implications for a Chlamydia trachomatis T cell vaccine. Vaccine 33, 2159–2166 (2015).
Inic-Kanada, A. et al. Delivery of a chlamydial adhesin N-PmpC subunit vaccine to the ocular mucosa using particulate carriers. PLoS ONE 10, e0144380 (2015).
Vasilevsky, S., Stojanov, M., Greub, G. & Baud, D. Chlamydial polymorphic membrane proteins: regulation, function and potential vaccine candidates. Virulence 7, 11–22 (2016).
Yu, H., Jiang, X., Shen, C., Karunakaran, K. P. & Brunham, R. C. Novel Chlamydia muridarum T cell antigens induce protective immunity against lung and genital tract infection in murine models. J. Immunol. 182, 1602–1608 (2009).
Farris, C. M. & Morrison, R. P. Vaccination against Chlamydia genital infection utilizing the murine C. muridarum model. Infect. Immun. 79, 986–996 (2011).
Wizel, B., Nystrom-Asklin, J., Cortes, C. & Tvinnereim, A. Role of CD8(+)T cells in the host response to Chlamydia. Microbes Infect. 10, 1420–1430 (2008).
Russi, R. C., Bourdin, E., Garcia, M. I. & Veaute, C. M. I. In silico prediction of T- and B-cell epitopes in PmpD: first step towards to the design of a Chlamydia trachomatis vaccine. Biomed. J. 41, 109–117 (2018).
Quinónez-Calvache, E. M. et al. Chlamydia trachomatis frequency in a cohort of HPV-infected Colombian women. PLoS ONE 11, 1–14 (2016).
Almagro Armenteros, J. J. et al. SignalP 5.0 improves signal peptide predictions using deep neural networks. Nat. Biotechnol. 37, 420–423 (2019).
Bendtsen, J. D., Kiemer, L., Fausboll, A. & Brunak, S. Non-classical protein secretion in bacteria. BMC Microbiol. 5, 58 (2005).
Nielsen, M. et al. Quantitative predictions of peptide binding to any HLA-DR molecule of known sequence: NetMHCIIpan. PLoS Comput. Biol. 4, e1000107 (2008).
Jespersen, M. C., Peters, B., Nielsen, M. & Marcatili, P. BepiPred-2.0: improving sequence-based B-cell epitope prediction using conformational epitopes. Nucleic Acids Res. 45, W24–W29 (2017).
Acknowledgements
This work was supported by Colombia’s General Royalties System, project BPIN-233, special agreement 021, entitled, “Developing a management plan for controlling cervical cancer in the Amazonas department,” which was approved by the Amazonas Department Local Government and Colombia’s Science, Technology and Innovation Department (COLCIENCIAS). Neither entity participated in developing the study. We would like to thank the Colombia’s Science, Technology and Innovation Department (COLCIENCIAS) for financing MC as part of the Colombian Programme for Promoting Researcher Training—Call 617 (PhD study in Colombia). Sara Cecilia Soto De Leon provided technical support. We would like to thank Jason Garry for translating the manuscript.
Author information
Authors and Affiliations
Contributions
L.P., M.C. and D.A.M.P.: designed the study, performed the experiments, analysed the data, wrote the first draft and revised the final draft of the manuscript. R.S. and L.D.R.O.: designed the study, contributed to data analysis and critically reviewed the first and final drafts of the manuscript. I.M.B.M.: contributed to the experiments and critically reviewed the first and final drafts of the manuscript. M.E.P: and M.A.P.: critically reviewed the first and final drafts of the manuscript. All authors approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pedraza, L., Camargo, M., Moreno-Pérez, D.A. et al. Identifying HLA DRB1-DQB1 alleles associated with Chlamydia trachomatis infection and in silico prediction of potentially-related peptides. Sci Rep 11, 12837 (2021). https://doi.org/10.1038/s41598-021-92294-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-92294-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
