
Abstract
Weather temperatures affect the incidence of cardiovascular diseases (CVD), but there is limited information on whether CVD hospitalizations are affected by changes in weather temperatures in a super-aging society. We aimed to examine the association of diurnal weather temperature changes with CVD hospitalizations. We included 1,067,171 consecutive patients who were admitted to acute-care hospitals in Japan between April 1, 2012 and March 31, 2015. The primary outcome was the number of CVD hospitalizations per day. The diurnal weather temperature range (DTR) was defined as the minimum weather temperature subtracted from the maximum weather temperature on the day before hospitalization. Multilevel mixed-effects linear regression models were used to estimate the association of DTR with cardiovascular hospitalizations after adjusting for weather, hospital, and patient demographics. An increased DTR was associated with a higher number of CVD hospitalizations (coefficient, 4.540 [4.310–4.765]/°C change, p < 0.001), with greater effects in those aged 75–89 (p < 0.001) and ≥ 90 years (p = 0.006) than among those aged ≤ 64 years; however, there were no sex-related differences (p = 0.166). Greater intraday weather temperature changes are associated with an increased number of CVD hospitalizations in the super-aging society of Japan, with a greater effect in older individuals.
Similar content being viewed by others
Introduction
The prevention of cardiovascular disease (CVD) involves lifestyle patterns that are incorporated as daily habits. According to guidelines for the prevention of CVD development, clinicians and a team-based care approach should guide individuals to establish healthy living, healthy eating, regular exercise, proper sleep guidance, avoidance of tobacco smoking, the management of hypertension and diabetes mellites, and use of aspirin and statin therapy1. Daily habits are greatly influenced by daily variations in the weather. For example, people stay indoors and refrain from walking during stormy days and jog outside on sunny days. In this way, the weather and our daily habits are closely related. Weather forecasting helps people avoid danger, by knowing the maximum and minimum temperatures and natural disasters.
Previous studies have provided important information on how extreme weather temperatures affect morbidity and mortality2,3. For example, lower weather temperatures have been reported to be a risk factor for incident CVD4,5 and cardiovascular death2,3. Weather temperature can be used to guide the prevention of CVD.
However, there are three main limitations of previous studies with regard to discussion on the prevention of CVD. First, previous reports have typically selected specific heart diseases or relatively small study samples2,3. For example, the association of temperature with myocardial infarction, heart failure, or aortic disease is interesting; however, there is a need to prevent all CVDs in the general population. Second, although studies on the absolute effects of weather (hot, cold, or mean temperature) on CVD are well known2,3,4,5, few studies have focused on diurnal temperature changes. Therefore, clinicians are unsure on how to guide their patients to be careful of weather-induced temperature changes. Third, although Japan has the world's largest aging population, there are no studies on the relationship between weather-based temperature and CVD in a super-aging society6. In addition, there are no reports on the association between temperature and the development of CVD, based on an analysis of Japanese nationwide databases.
To address the issue, we conducted an observational study using a nationwide registry database, to investigate whether the number of CVD hospitalizations is related to weather temperature in the super-aging society in Japan. The Japanese Registry of All Cardiac and Vascular Diseases (JROAD) database includes all patients with CVDs who required hospitalization and constitutes a nationwide dataset in Japan. The study aims to assess the relationship between weather temperature and the development of CVD to guide clinicians on recommendations regarding the weather, to improve healthcare for an increasingly aging society.
Methods
Data collection
The JROAD database is a nationwide prospective registry that was designed to assess the clinical activity of each Japanese institution with regard to cardiovascular care and provide adequate feedback to teaching hospitals for improving patient care. A detailed description of the database design and methods has been published previously7. Briefly, the Japanese Circulation Society (JCS) developed the JROAD database, which includes demographic data from each hospital since 2004, and the JROAD-DPC nationwide database, which includes data from the Japanese Diagnosis Procedure Combination/Per Diem Payment System (DPC/PDPS) since 2014. The DPC database is a mixed-case classification system linked with a lump-sum payment system, which was launched in 2002 by the Ministry of Health, Labour and Welfare in Japan8. Compared with other registry databases, the Japanese DPC database enables researchers to conduct nationwide studies of both, descriptive and/or analytical epidemiology in a real-world clinical setting. The DPC database includes data on the following elements: demographics for each patient (e.g., age and sex); principal diagnoses (coded according to the International Classification of Diseases, 10th revision [ICD-10]); comorbidities at admission (ICD-10 coded); complications after admission (ICD-10 coded); procedures, including surgery, medications, and devices used during hospitalization; length of stay; discharge status; and medical expenses7,8. Institutions using the DPC system encompass a wide variety of centers, including academic, urban, and rural hospitals7. All data included in this study were from hospitalized patients with clinically apparent CVD.
We collated and used the dataset of the weather variables in Japan from the National Institute for Environmental Studies (http://www.nies.go.jp). The weather variables included hourly weather temperature and humidity. The weather variables were merged with the DPC database by using the acute-hospitalization day and municipal code provided by the Japanese Ministry of Internal Affairs and Communications (http://www.soumu.go.jp/denshijiti/code.html).
Design
We conducted a cross-sectional study using data from the JROAD, JROAD-DPC, and weather variables between April 1, 2012 and March 31, 2015.
Subjects
In total, 911 hospitals were included in this study, and 2,369,165 consecutive patients were initially screened for study inclusion. However, 1,301,994 patients were excluded because of planned hospitalizations, which included admission for percutaneous coronary intervention for stable angina, follow-up catheterization, diagnostic admissions, scheduled catheter ablation (such as that for atrial fibrillation and supraventricular tachycardia), and scheduled cardiac surgery. In the final analysis dataset, we included data from 1,067,171 patients for statistical analysis (Fig. 1). This research was designed by the authors, and the study protocol was approved by the institutional ethics committee of the St. Marianna University of Medicine. Each hospital anonymized their patient IDs using code-change equations for the original JROAD-DPC data.

Flowchart of patient disposition. The flowchart presents the analyses conducted to evaluate an association between weather and incident cardiovascular disease.
Exposure
Seasons were separated into spring (March 23–June 21), summer (June 22–September 21), fall (September 22–December 21), and winter (December 22–March 22). The average temperature was defined as the average of each hourly temperature and humidity within a day. DTR was calculated by subtracting the minimum weather temperature from the maximum weather temperature in the same day. A higher index represented a greater change of weather temperature. The average and range of weather variables in a certain day were assigned to the day before an emergency hospitalization due to CVD.
Outcomes
The primary outcome was the number of CVD hospitalizations per day. For the purposes of this study, CVD hospitalizations included coronary artery disease, heart failure, arrhythmia, aortic and peripheral artery diseases, cardiac arrest, pulmonary embolism, pulmonary hypertension, endocarditis/pericarditis, and congenital heart disease.
Covariates
The average weather temperature and DTR as continuous and categorical values were subdivided into quintiles, that were adjusted for weather (season and average humidity), hospital (east/west Japan, number of hospital beds, and presence of coronary care unit, cardiac surgery service, and board-certified cardiologist), and patient demographics (age, sex, height, weight, smoking, Charlson Comorbidity Index, angina, acute myocardial infarction, heart failure, atrial fibrillation/flutter, aortic diseases, cardiac arrest, pulmonary embolism, pulmonary hypertension, and Tetralogy of Fallot).
Statistical analysis
Descriptive statistics were analyzed for the demographics of hospital, weather, and patients. The number of cardiovascular hospitalizations by season was compared by one-way analysis of variance with Bonferroni post-hoc comparisons. We used multilevel mixed random-effects and population-averaged linear models to evaluate the association between the number of cardiovascular hospitalizations and weather variables. The multilevel mixed-effect models were used for evaluating the random effects of hospital variations (institutional code) determined by the JROAD study. The average weather temperature and DTR, as continuous and categorical values, respectively, were adjusted for weather, hospital, and patient demographics. The predicted number of cardiovascular hospitalizations per day was calculated using “marginsplot” after the creation of multilevel mixed random-effects and population-averaged linear models in STATA. The random effects and covariates were considered clinically important factors. All analyses were performed using STATA statistical software version 14 (Stata Corp, College Station, TX, USA). Statistical significance was defined as p < 0.05.
Ethics approval
The study protocol was approved by the institutional ethics committee of the St. Marianna University of Medicine (#4038).
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Provenance and peer review
Not commissioned; externally peer reviewed.
Results
Data were collected from a total of 1,067,171 consecutive patients with CVD admitted across 715 acute-care hospitals in Japan between 2012 and 2014. Patient characteristics and demographics are shown in Table 1.
In this study population, the mean age was 71.3 ± 20.1 years and 42.3% of subjects were female. The incidence of acute myocardial infarction, heart failure, and cardiac arrest was 10.6%, 29.4%, and 8.6%, respectively. The overall hospital had a 500-bed count, and 59% of the study centers had cardiosurgical services. The mean weather temperature was 14.5 °C with intraday variations of up to 7.7 °C. Overall, the number of incident CVD hospitalizations tended to be higher in winter (Supplemental Fig. 1).
Association between average weather temperature and CVD hospitalizations
Multilevel mixed-effects linear regression analysis indicated that a number of incident CVD hospitalizations were associated with lower average weather temperature (coefficient, − 3.962 [− 4.081 to − 3.3842] per ℃, p < 0.001) after adjustments for weather (season and average humidity), hospital (east/west Japan, number of hospital beds, presence of a coronary care unit, cardiosurgical service, board-certified cardiologist), and patient (age, sex, height, weight, Brinkmann Index, Charlson Comorbidity Index score, angina, acute myocardial infarction, heart failure, atrial fibrillation/flutter, aortic diseases, cardiac arrest, pulmonary embolism, pulmonary hypertension, and Tetralogy of Fallot) characteristics (Table 2).
The number of CVD hospitalizations was higher in the Q3 (coefficient, 8.613 [6.367–10.860] vs. Q1, p < 0.001), Q4 (coefficient, − 27.966 [− 30.609 to − 25.324] vs. Q1, p < 0.001), and Q5 (coefficient, − 83.74 [− 85.617 to − 79.864] vs. Q1, p < 0.001) groups of average weather temperature than in the Q1 group, after the above-described adjustments (Fig. 2a).

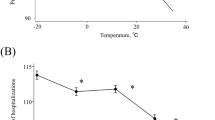
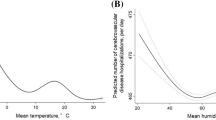
Association of weather temperature with acute hospitalizations for incident cardiovascular disease. The association of the mean adjusted probability of the number of hospitalizations due to cardiovascular disease across the quartiles of average weather temperature (a) and intraday weather temperature change (b). The bars indicate 95% confidence intervals.
Association between weather temperature changes and CVD hospitalizations
The increase in the diurnal weather temperature range (DTR) was associated with a greater number of CVD hospitalizations (coefficient, 4.540 [4.310 to 4.765] per ℃, p < 0.001) after adjusting for weather, hospital, and patient characteristics (Table 2).
The number of CVD hospitalizations was higher in the Q2 (coefficient, 5.736 [3.833 to 7.639] vs. Q1, p < 0.001), Q3 (coefficient, 9.695 [7.722 to 11.669] vs. Q1, p < 0.001), Q4 (coefficient, 4.681 [2.649 to 6.714] vs. Q1, p < 0.001), and Q5 (coefficient, 39.282 [37.121 to 41.442] vs. Q1, p < 0.001) groups of DTR than in the Q1 group, after the abovementioned adjustments (Fig. 2b).
Effects of weather temperature indices in different age groups
The specific risk estimates of incident CVD with respect to average weather temperature are summarized in Fig. 3. A lower average weather temperature was associated with an increased incidence of CVD hospitalization for most patient conditions. Higher average weather temperatures were associated with an increased rate of hospitalization in spring. The effects of average weather temperature on all CVD admissions were greater in the 65–74 (coefficient, − 0.360 [− 0.386 to − 0.335], p < 0.001) and 75–89 (coefficient, − 0.442 [− 0.460 to − 0.424], p < 0.001) years age groups than in the ≤ 64 years age group; however, there were no differences between the ≥ 90 and ≤ 64 years age groups with regard to the effects of temperature on hospitalizations (p = 0.118). Moreover, the effects of average weather temperature were greater in female patients and individuals with heart failure, aortic disease, and pulmonary embolism than in patients without these risk factors (all p < 0.001).

Association between average weather temperature and hospitalizations for cardiovascular conditions. Coefficients greater than zero represent an increase in the number of cardiovascular hospitalizations by the average weather temperature. The coefficient is indicated by a dot, and the lines represent the 95% confidence intervals (CIs).
A higher DTR was associated with an increased risk of incident CVD in all conditions (Fig. 4). The effects of an increased DTR on CVD hospitalization were greater in the 75–89 (coefficient, 0.486 [0.452–0.520], p < 0.001) and ≥ 90 (coefficient, 0.438 [0.362–0.515], p = 0.006) years age groups than in the ≤ 64 years age group; however, no sex-related differences were detected (p = 0.166). Greater effects of DTR were found in patients with angina, heart failure, aortic disease, pulmonary embolism, and cardiac arrest (p < 0.001 for all). The effect was greater in spring than in summer, autumn, and winter (p < 0.001 for all).

Association between weather temperature change and hospitalizations for cardiovascular conditions. Coefficients greater than zero represent an increased risk of incident cardiovascular hospitalization based on the range of weather temperatures. The coefficient is indicated by the dot, and the lines represent the 95% confidence interval (CIs).
Discussion
We present a contemporary analysis of nationwide data from 1,067,171 patients and describe the estimated number of incident CVD hospitalizations. We found that overall, a higher number of incident CVD was associated with: (1) lower average weather temperatures and (2) greater weather temperature change, assessed by DTR. The effects of lower temperatures and DTR on all CVD admissions were more marked in elderly patients than in younger patients (Fig. 5). These observations suggest that in addition to average weather temperature, greater weather temperature changes need to be considered to evaluate the potential for the development of CVD in a super-aging society, such as Japan.

Illustration of the main study findings. A lower average weather temperature and a higher range of weather temperatures were associated with a higher incidence of cardiovascular hospitalization. These observations suggest that besides a reduction in weather temperature, a change in weather temperature may be considered for developing strategies for the prevention of cardiovascular diseases in an aging society.
We found that lower weather temperatures were associated with increased hospitalizations for CVD. Other studies have found that cold-induced systemic hypertension9 and pulmonary hypertension10 are risk factors associated with the renin–angiotensin system, that could modulate the incidence of CVD hospitalizations. Using quantitative coronary angiography in 1980, Raizner et al. reported that the luminal diameter significantly decreased following 1 min of cold-pressor stimulation; this is known as coronary spasm11. Lower temperature ranges may be an additional environmental factor leading to higher incidences of hospitalization in cardiology wards.
However, Moghadamnia et al. conducted a systematic review and meta-analysis and concluded that both cold and hot weather temperatures increased the risk of cardiovascular mortality12. The mechanisms underlying higher weather temperature-related health effects potentially include impaired vascular endothelium, microthrombosis, elevated blood viscosity, disruptions in cholesterol levels, and dehydration13,14. The effects of high temperatures in our study were different; however, they may represent a change in the diurnal temperature and not an absolute effect of cold or hot weather.
Contrary to most previous studies, our study confirmed that a greater weather temperature range is an independent risk factor for CVD in a super-aging society. It has been reported that greater weather temperature range was significantly associated with emergent CVD admissions among the elderly in Beijing15 and South Korea16. A nationwide analysis reported that increased temperature variability was associated with a higher number of hospital admissions for CVD, ischemic heart disease, heart failure, heart rhythm disturbances, ischemic stroke, and arrhythmia17,18. The results from those previous studies are consistent with the findings of this study.
Compared with previous studies, however, we found that the effects of DTR on all CVD admissions increased with older age. The effects of DTR and cold temperature on CVD outcomes are not similar to those of other weather variables. The study by Vutkovici et al.19 found that diurnal variations in temperature are associated with a small increase in non-accidental mortality among the elderly population. Analitis et al. studied the short-term effects of cold weather on mortality in 15 European cities and demonstrated that the increased risk of CVD in cold weather was greater for older age groups20. In a review of recent studies, Astrom et al. explored the impact of heatwaves on morbidity and mortality in the elderly population21. These observations are consistent with the findings from this study. The elderly population is likely to develop complications due to atherosclerosis, infections, chronic obstructive pulmonary disease, cancer, dementia, Alzheimer’s disease, or low socioeconomic status22,23. The elderly population may have a lower thermoregulatory capacity and relatively weak immunological defenses, which could increase their vulnerability to respiratory tract infections in hot and cold weather24. Although there was no difference in the effects of average weather temperature on all CVD admissions between ages < 64 and > 90 years in this study, there were differences in the effects of DTR on all admissions. We believe that a change in temperature, rather than the absolute value of temperature, had a greater effect on the elderly.
We found that lower weather temperatures were associated with increased hospitalizations for CVD, particularly in winter. Data from a recent meta-analysis, that included 15 countries with a total sample size of 237,979 subjects, showed a seasonal pattern for most cardiovascular risk factors, with a higher prevalence in winter25. The potential pathogenic mechanism underlying these effects may be attributed to the effects of seasonal and weather temperature changes on CVD risk factors, such as increased blood pressure26, serum cholesterol27, platelets and fibrinogen activity28, endothelial dysfunction29, and respiratory infection in winter30. In this study, the effect of DTR was greater in spring than in summer, autumn, and winter. We could not identify the reason why a higher weather temperature in the spring conferred a higher risk of incident CVD in this observational study.
Furthermore, CVD hospitalization is a growing public health concern because of an aging population. Therefore, the findings of this study have important implications for risk reduction for CVD and may guide public health interventions to control and prevent the cardiovascular effects of exposure to changes in ambient and weather temperatures, particularly for individuals at high risk for hospitalization due to coronary attacks, arrhythmias, aortic disease, or heart failure. Keeping warm is important in the winter. Maintaining the main rooms at appropriate temperatures to avoid greater changes due to the weather will help prevent factors that can trigger an incident CVD.
One of the limitations of our study is that we included only Japanese Diagnosis Procedure Combination hospitals with cardiovascular beds that meet the JCS requirements. However, the JROAD is the largest cross-sectional study of nationwide cardiac health outcomes in Japan and constitutes a comprehensive database of epidemiological data for population-based studies. Cross-sectional studies do not determine cause and effect; however, the large sample size is a noteworthy strength of this study. Future longitudinal studies on the mechanism of temperature/DTR effects on cardiovascular events and their outcomes are needed. Determinants of the populations that are the most vulnerable to weather changes should be further explored. This study could not clearly identify whether the findings were related to the temperature itself or to the secondary effects on risk factors.
In conclusion, lower weather temperatures and greater intraday weather temperature variations are associated with an increased incidence of cardiovascular hospitalizations in the aging society of Japan. The effects of weather temperature change on all CVD hospitalizations were greater in older age. Keeping warm on cold days and cool on hot days may reduce the risk of CVD, especially in people aged ≥ 75 years. The results of this study may provide guidance to clinicians on instructing patients to remain cautious about weather-related temperature changes in a country with an increasingly aging society.
Data availability
The data that support the findings of this study are available from the JROAD; however, restrictions apply to the availability of these data, which were used under approval for the current study and are thus not publicly available. Data are however available from the JROAD upon reasonable request. Environmental pollution data are available from the National Institute for Environmental Studies, Japan (http://www.nies.go.jp/db/index-e.html).
References
Arnett, D. K. et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 140, e596–e646 (2019).
Danet, S. et al. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: the Lille-World Health Organization MONICA project (monitoring trends and determinants in cardiovascular disease). Circulation 100, E1–E7 (1999).
Atsumi, A. et al. Relationship between cold temperature and cardiovascular mortality, with assessment of effect modification by individual characteristics: Ibaraki prefectural health study. Circ. J. 77, 1854–1861 (2013).
Phung, D. et al. Ambient temperature and risk of cardiovascular hospitalization: an updated systematic review and meta-analysis. Sci. Total Environ. 550, 1084–1102 (2016).
Hensel, M. et al. Relationship between ambient temperature and frequency and severity of cardiovascular emergencies: a prospective observational study based on out-of-hospital care data. Int. J. Cardiol. 228, 553–557 (2017).
Yasuda, S., Miyamoto, Y. & Ogawa, H. Current status of cardiovascular medicine in the aging society of Japan. Circulation 138, 965–967 (2018).
Yasuda, S. et al. The current status of cardiovascular medicine in Japan - analysis of a large number of health records from a nationwide claim-based database, JROAD-DPC. Circ. J. 80, 2327–2335 (2016).
Yasunaga, H. et al. Impact of the Japanese diagnosis procedure combination-based payment system on cardiovascular medicine-related costs. Int. Heart J. 46, 855–866 (2005).
Carroll, D. et al. Blood pressure reactions to the cold pressor test and the prediction of ischaemic heart disease: data from the Caerphilly Study. J. Epidemiol. Commun. Health 52, 528–529 (1998).
Dubiel, J. P. et al. Effect of cold on the pulmonary arterial pressure and right ventricular load in patients with pulmonary hypertension. Acta Med. Pol. 27, 19–29 (1986).
Raizner, A. E. et al. Provocation of coronary artery spasm by the cold pressor test. Hemodynamic, arteriographic and quantitative angiographic observations. Circulation 62, 925–932 (1980).
Moghadamnia, M. T. et al. Ambient temperature and cardiovascular mortality: a systematic review and meta-analysis. PeerJ 5, e3574 (2017).
Lim, Y. H. et al. Effects of cold and hot temperature on dehydration: a mechanism of cardiovascular burden. Int. J. Biometeorol. 59, 1035–1043 (2015).
Bouchama, A. & Knochel, J. P. Heat stroke. N. Engl. J. Med. 346, 1978–1988 (2002).
Zheng, S. et al. Gender, age and season as modifiers of the effects of diurnal temperature range on emergency room admissions for cause-specific cardiovascular disease among the elderly in Beijing. Int. J. Environ. Res. Public Health 13, 447 (2016).
Lim, Y. H. et al. Effect of diurnal temperature range on cardiovascular markers in the elderly in Seoul, Korea. Int. J. Biometeorol. 57, 597–603 (2013).
Tian, Y. et al. Association between temperature variability and daily hospital admissions for cause-specific cardiovascular disease in urban China: a national time-series study. PLoS Med. 16, e1002738 (2019).
Zhao, Q. et al. Temperature variability and hospitalization for cardiac arrhythmia in Brazil: a nationwide case-crossover study during 2000–2015. Environ. Pollut. 246, 528–552 (2019).
Vutcovici, M., Goldberg, M. S. & Valois, M. F. Effects of diurnal variations in temperature on non-accidental mortality among the elderly population of Montreal, Quebec, 1984–2007. Int. J. Biometeorol. 58, 843–852 (2014).
Analitis, A. et al. Effects of cold weather on mortality: results from 15 European cities within the PHEWE project. Am. J. Epidemiol. 168, 1397–1408 (2008).
Astrom, D. O., Forsberg, B. & Rocklov, J. Heat wave impact on morbidity and mortality in the elderly population: a review of recent studies. Maturitas 69, 99–105 (2011).
Pan, W. H., Li, L. A. & Tsai, M. J. Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet 345, 353–355 (1995).
Nogues, R. et al. Influence of nutrition, thyroid hormones, and rectal temperature on in-hospital mortality of elderly patients with acute illness. Am. J. Clin. Nutr. 61, 597–602 (1995).
von Klot, S., Zanobetti, A. & Schwartz, J. Influenza epidemics, seasonality, and the effects of cold weather on cardiac mortality. Environ. Health 11, 74 (2012).
Marti-Soler, H. et al. Seasonality of cardiovascular risk factors: an analysis including over 230 000 participants in 15 countries. Heart 100, 1517–1523 (2014).
Wang, Q. et al. Environmental ambient temperature and blood pressure in adults: a systematic review and meta-analysis. Sci. Total Environ. 575, 276–286 (2017).
Ockene, I. S. et al. Seasonal variation in serum cholesterol levels: treatment implications and possible mechanisms. Arch. Intern. Med. 164, 863–870 (2004).
Crawford, V. L., McNerlan, S. E. & Stout, R. W. Seasonal changes in platelets, fibrinogen and factor VII in elderly people. Age Ageing 32, 661–665 (2003).
Widlansky, M. E. et al. Relation of season and temperature to endothelium-dependent flow-mediated vasodilation in subjects without clinical evidence of cardiovascular disease (from the Framingham Heart Study). Am. J. Cardiol. 100, 518–523 (2007).
Desmond, L. A. et al. Respiratory viruses in adults hospitalised with Community-Acquired Pneumonia during the non-winter months in Melbourne: routine diagnostic practice may miss large numbers of influenza and respiratory syncytial virus infections. Commun. Dis. Intell. 43, 1–13 (2019).
Acknowledgements
The authors thank the other investigators, staff, and participants of the JROAD study for their valuable contributions. A full list of institutions can be found at http://jroadinfo.ncvc.go.jp.
Funding
This work was supported by the Japan Society for the Promotion of Science (KAKENHI Grant Number 18K08119).
Author information
Authors and Affiliations
Contributions
K.Y., M.N., Y.M., S.Y., and H.O. had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Concept and design: All authors. Acquisition, analysis, or interpretation of data: K.T., M.W., T.K., Y.S., Y.I., M.I., and Y.T. Drafting of the manuscript: K.Y., M.N., T.H., and K.T. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: K.Y. and M.N. Administrative, technical, or material support: Y.M., Y.S., Y.I., T.H., S.Y., and H.O. Supervision: T.H., H.O., Y.M., S.Y., and Y.J.A.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yoneyama, K., Nakai, M., Higuma, T. et al. Weather temperature and the incidence of hospitalization for cardiovascular diseases in an aging society. Sci Rep 11, 10863 (2021). https://doi.org/10.1038/s41598-021-90352-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-90352-x
This article is cited by
-
Effects of temperature and humidity on cerebrovascular disease hospitalization in a super-aging society
Scientific Reports (2023)
-
Evaluation of the Effects of Thermal Comfort Conditions on Cardiovascular Diseases in Amasya City, Turkey
Journal of Public Health (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
