
Abstract
This study aimed to investigate the hydration influence on the autonomic responses of coronary artery disease subjects in the immediate recovery period after a cardiovascular rehabilitation session, in view of the risks of a delayed autonomic recovery for this population. 28 males with coronary artery disease were submitted to: (I) Maximum effort test; (II) Control protocol (CP), composed by initial rest, warm-up, exercise and passive recovery; (III) Hydration protocol (HP) similar to CP, but with rehydration during exercise. The recovery was evaluated through the heart rate (HR) variability, HR recovery and by the rate of perceived exertion and recovery. The main results revealed that the vagal reactivation occurred at the first 30 s of recovery in HP and after the first minute in CP. A better behavior of the HR at the first minute of recovery was observed in HP. The rate of perceived exertion had a significant decrease in the first minute of recovery in HP, while in CP this occurred after the third minute. In conclusion, despite an anticipated vagal reactivation found at HP, these results should be analyzed with caution as there were no significant differences between protocols for all variables and the effect sizes were small.
Similar content being viewed by others
Introduction
Subjects with coronary artery disease (CAD) present an autonomic modulation impairment characterized by a decreased vagal activity and a sympathetic hyperactivity1, which is related to a risen risk of ischemic events, and a higher mortality rate2. Thus, the insertion of this population in cardiac rehabilitation programs (CRP) is essential, as physical exercise promotes positive modifications in the autonomic modulation3.
Despite the well-known physical exercise benefits, and although the rate of occurrence of major cardiovascular events during cardiac rehabilitation in stable patients is very low4,5, the post-exercise period represents a vulnerable state of the cardiovascular system, in which arrhythmias, syncope, and sudden death may occur6,7. During the early recovery phase, the autonomic nervous system (ANS) plays a central role in the cardiovascular deceleration, by rapidly decreasing the heart rate (HR) through vagal reactivation within the first minutes of recovery8. However, due to the sympathetic hyperactivity related to CAD, the vagal reentry is delayed in this population9. Thus, the HR, the cardiac workload and the myocardium oxygen consumption remain higher for a longer period, which favors the appearance of sudden events during the recovery10.
Given the risks related to a delayed vagal reactivation and HR reduction, the study of strategies capable of promoting a more efficient recovery on this population immediately after exercise is essential, as a faster recovery is related to a lower risk of sudden events2 and may contribute to the safety of CRP.
Considering that the fluid loss due to transpiration11 can negatively influence the ANS12 and directly affects the baroreflex mechanisms, contributing to the slower HR recovery after the exercise13, the fluid intake has been suggested as a strategy to accelerate the immediate14,15,16,17 and long-term18,19,20 autonomic and HR recovery after exercise. However, this topic has only been studied in healthy populations.
Thus, we highlight the importance of studying the influence of hydration in CAD subjects. Since this technic can be easily implemented in CRP as a strategy to decrease post-exercise risks, opening an important field of research in clinical practice, that may influence the current techniques used in these programs.
Considering these aspects, the study aimed to investigate the influence of hydration in the autonomic modulation of CAD patients, through HR recovery and HR variability, at the immediate recovery period of a cardiac rehabilitation session. Also, as secondary outcomes, its influence in the rate of perceived exertion, discomfort and recovery.
Method
Trial design and setting
This crossover clinical trial followed the Consolidated Standards of Reporting Clinical Trials (CONSORT) extension to randomized crossover trials21, and was registered at clinicaltrial.gov (NCT 03198806 – 26/06/2017).
The experimental procedure was divided into three phases with a minimal interval of 48 h between them and was performed at the Physical Therapy Study and Care Center—Presidente Prudente, São Paulo—Brazil. The phases were: Phase I. Cardiopulmonary Exercise Test; Phase II. Control Protocol (CP); and Phase III. Hydration Protocol (HP).
The volunteers were initially oriented to maintain their habitual physical activity habits while participating in the study, but to avoid vigorous physical activity and consumption of stimulant substances for 24 h before each phase, and to consume a light meal two hours before each phase22.
All procedures were approved by the Committee for Ethics and Research of the São Paulo State University, School of Technology and Science—UNESP (CAAE: 54864716.8.0000.5402) and followed the Helsinki Declaration. The volunteers were informed about the procedures and objectives of this study and, after agreeing to participate, signed the consent form.
Participants
Male patients of CRP who were previously diagnosed by their cardiologists with ischemic coronary artery disease and left ventricular ejection fraction higher than 50% were invited to participate in the study, after the previous analysis of the medical record regarding the inclusion/exclusion criteria.
Participants with less than 3 months of participation in CRP, those who were alcoholics and/or smokers, subjects with respiratory diseases, unstable angina, non-controlled hypertension, significant valvular disease, non-controlled metabolic disease, and/or neurological problems that could preclude the protocol execution were not included. The exclusion criteria were: abnormal hemodynamic responses during the cardiopulmonary exercise test23, presence of a series of RR intervals with less than 95% of sinus heartbeats22 and non-attendance to one of the protocol phases.
Interventions
Cardiopulmonary exercise test
To define the exercise load and to evaluate the hemodynamic responses, the volunteers performed a maximum stress test on a treadmill (INBRASPORT), according to Bruce’s protocol, that was preceded by 5 min of warming-up at 2.5 km/h24. The test was conducted by a physician and was interrupted by voluntary exertion and/or ischemia signs and/or severe arrhythmia. To determine the oxygen uptake (VO2), the exhaled gases were analyzed by the Quark PFT (COSMED) system25 calibrated with volumes and gases of known concentration. The exercise load used in Phases II and III was set as 60–80% of the HR reached at the anaerobic threshold. For those who did not reach the anaerobic threshold during the test, the oxygen uptake peak was considered23,26. This intensity is considered as low-moderate, which is safe and commonly used in CRP26. Exercises performed above the anaerobic threshold may produce negative acute responses in subjects with CAD, such as metabolic acidosis, hyperventilation, and reduction in the capacity of performing the exercise26.
Control and hydration protocols
The protocols were performed between 1:00 and 6:00 pm to avoid the circadian variation and the temperature and humidity of the room were controlled (22–25 °C and 40–60%, respectively)22.
After volunteer arrival, a urine sample was collected to identify the hydration status. Also, body mass and height were measured with a digital scale (BALMAK) and a stadiometer (SANNY), respectively.
After these procedures, the volunteers remained in the orthostatic position for 10 min. Then, they performed 15 min of warming-up, composed by stretching and global exercises, followed by 40 min of treadmill exercise, that was stopped without a cool-down period. After this, volunteers remained on the treadmill in orthostatic position for 10 min performing the passive recovery. After recovery, another urine sample was collected, and the body mass was measured. The axillar temperature was measured with a thermometer (G-TECH) before and immediately after exercise.
During the HP, volunteers ingested four equal portions of mineral water (BONAFONT) every 10 min during the treadmill exercise, as done in other studies18,19,20.
Hydration condition
The volunteers were instructed to ingest 500 ml of water two hours before the protocols to ensure an initial hydrated state27. The amount of water administered during the HP was obtained through the body mass difference verified before and after the CP, considering that one gram is equivalent to one milliliter of fluid lost, as described by Armstrong et al.28 and applied by other studies18,19,20.
The dynamic hydration status before and after the protocols was assessed by the urine analysis (Combur 10 M ROCHE). The urine specific density was used as a marker of the hydration level, and values above 1.020 classified the volunteer as dehydrated28.
Outcomes
Heart rate variability (HRV)
The vagal reactivation and the autonomic modulation were evaluated through HRV29, a non-invasive method based on the oscillations between consecutive RR intervals30 recorded through a HR monitor (POLAR ELECTRO)31.
To assess the vagal reactivation, the RMSSD index (root mean square of successive RR interval differences) was analyzed in 30-s intervals (RMSSD30) as proposed by Goldberger et al.32 and applied by other studies14,15,33. The last 30 s of the initial rest (M1), the last 30 s of the exercise (M2), and the first 2 min of the recovery, divided into four windows of 30 s each (M3, M4, M5, and M6), were considered.
This analysis was complemented by the evaluation of the autonomic modulation during the first 10 min of recovery. The last 5 min of the initial rest (REST) and the 10th-minute recovery divided into REC1 (0–5th minute) and REC2 (5th–10th minute) were considered. The HRV was analyzed in the time and frequency domains, as follows: LF (low-frequency component—0,04 to 0,15 Hz) and HF (high-frequency component—0,15 to 0,40 Hz) in milliseconds squared (ms2); LF/HF ratio; SDNN (standard deviation of all normal RR intervals); and RMSSD30.
The series of RR intervals were submitted to a digital filtration through the Polar Pro Trainer Software® (version 5.0, Polar Inc., Kempele, Finland)34 and only the series with more than 95% of sinus heartbeat were included. Also, visual analysis was performed to ensure the absence of artifacts or cardiac arrhythmias that could interfere in the analysis22. The indexes were calculated with the software Kubios HRV—version 2.035. This analysis was performed by an experienced and blinded researcher.
Heart rate recovery (HRR)
The parasympathetic reactivation after exercise was also indirectly evaluated by the HRR29. In order to determine the HRR, the HR was measured at three moments: at the peak of effort (HRpeak), at the first (HR1) and the second (HR2) minutes of recovery.
The HRpeak was defined as the mean of 5 RR intervals, considering two values before and two values after the HRpeak. The same procedure was used to obtain the HR1 and HR2. The HRR was defined by the difference between the HRpeak and HR1 (HRpeak—HR1 = HRR1) and between HRpeak and HR2 (HRRpeak—HR2 = HRR2)36. This procedure was also performed by an experienced and blinded researcher.
Rate of perceived exertion, recovery, and discomfort
The rate of perceived exertion (RPE) was evaluated by the Borg scale, an easy-to-use clinical tool commonly applied at the CRP to estimate the whole-body perceived effort, and it is known for indirectly correlating with the HR37. The Borg CR10 scale was used to define the perceived discomfort during the protocols. These scales were applied at the 10th minute of the rest, 15th and 35th minute of the exercise and 1st, 2nd, 3rd, 7th, and 10th minute of the recovery.
The rate of perceived recovery (RPR) was evaluated by a 10-point Likert scale, in which 1 corresponds to no recovery and 10 to fully recovered38 and it was applied during the recovery period.
Statistical analysis
The normality of data was determined by the Shapiro–Wilk test. To body mass, urine specific density, and axillar temperature, the comparison between the moments of the same protocol were performed by two-tailed paired Student’s t-test or Wilcoxon test. For the analysis between the protocols, two-tailed unpaired Student’s t-test or Mann–Whitney test were performed.
The comparison of HRR, HRV, RPE, RPR, and Borg CR10 between the protocols and moments was performed by two-way repeated-measures ANOVA. The data were checked for sphericity violation using Mauchly’s test and the Greenhouse–Geisser correction was considered when the sphericity was violated.
To analyze the moments during the same protocol, the Bonferroni post hoc test for parametric distribution or Dunnet post hoc test for non-parametric distributions were applied. The partial eta-squared effect size (η2P) was calculated for the ANOVA results (small ≤ 0.05; medium between 0.06 and 0.13; large ≥ 0.14)39. The HRR1 and HRR2 were analyzed between groups by the two-tailed unpaired Student’s t-test or Mann–Whitney test and the intragroup analysis was performed by the two-tailed paired Student’s t-test or Wilcoxon test. The Cohen’s d effect size was calculated for these analyses (small < 0.50; medium between 0.50 and 0.70; large between 0.80 and 1.20; very large ≥ 1.30)39.
The statistical significance was set at 5%. The analyses were performed using IBM SPSS Statistics—version 22.0 based on a coded data sheet by a blinded researcher.
Sample size
The sample size was based on the RMSSD index. The magnitude of significant difference assumed was 12 ms, considering a standard deviation of 16 ms36, with alfa risk of 5% and a beta risk of 80%, which resulted in a sample size of 28 volunteers. Considering the possible sample losses, we added 10% to the sample size calculated, totalizing 31 volunteers.
Results
Sample characterization and hydration condition
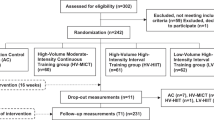
In total, 31 subjects were recruited (Fig. 1). After sample losses, 28 subjects were analyzed (Table 1).

Protocol design.
The body mass, axillar temperature, and urine specific density values are presented in Table 2. A significant reduction of the body mass was observed at the end of CP (0.345 ± 0.121 kg). Significant differences between the protocols for axillary temperature and specific density were not found.
Heart rate variability and heart rate recovery analysis
The RMSSD30 during the early recovery period was compared with the values at rest (Fig. 2b) and at the end of the exercise (Fig. 2a), to address the parasympathetic return to the rest values and the vagal reactivation, respectively. For both analysis, there were no significant differences between the protocols (2a: pvalue = 0.671; η2P = 0.003—small effect size/2b: pvalue = 0.791; η2P = 0.001—small effect size) and at the moments vs protocols interaction (2a: pvalue = 0.610; η2P = 0.012—small effect size/2b: pvalue = 0.469; η2P = 0.016—small effect size). However, there were differences between the moments (2a: pvalue < 0.001; η2P = 0.267—large effect size/2b: pvalue = 0.001; η2P = 0.237—large effect size).

Comparison of RMSSD30 at exercise (a) and initial rest (b) and comparison between HRpeak and HR1 and HR2 (c). Legend: M1 = last 30 s of initial rest; M2 = last 30 s of exercise; M3 = 0–30 s, M4 = 30–60 s, M5 = 60–90 s, M6 = 90–120 s of recovery; HRpeak heart rate at the peak of exercise, HR1 heart rate after 1 min of recovery, HR2 heart rate after 2 min of recovery. *Difference between exercise (a)/initial rest (b) and recovery on control protocol (pvalue < 0.001); #Difference between exercise (a)/initial rest (b) and recovery on hydration protocol (pvalue < 0.05).
For the HR analysis (Fig. 2c), no significant differences were found between the protocols (pvalue = 0.583; η2P = 0.013—small effect size) and at the moments vs protocols interaction (pvalue = 0.305; η2P = 0.021—small effect size). However, between the moments significant differences were found (pvalue = 0.001; η2P = 0.781—large effect size).
In the CP significant differences between HRR1 (11.11 ± 6.57) and HRR2 (14.40 ± 5.41; pvalue < 0.0001; Cohen’s d = 0.55—medium effect size) were observed. However, for HP there were no differences between HRR1 (13.18 ± 8.02) and HRR2 (14.41 ± 6.60; pvalue = 0.132; Cohen’s d = 0.17—small effect size). Comparisons of HRR1 and HRR2 between the protocols showed no significant statistical differences (HRR1: pvalue = 0.237; Cohen’s d = 0.28—small effect size/HRR2: pvalue = 0.554; Cohen’s d = 0.00—small effect size).
The results of the 5 min analysis of SDNN, RMSSD, LF, HF, LF/HF are presented in Table 3. There were no statistical differences between the protocols.
Rate of perceived exertion and recovery analysis
For the RPE and RPR (Fig. 3), there were no significant differences between the protocols (RPE: pvalue = 0.302, η2P = 0,020—small effect size; RPR: pvalue = 0.390, η2P = 0.014—small effect size) and for the moments vs protocols interaction (RPE: pvalue = 0.360, η2P = 0.018—small effect size; RPR: pvalue = 0.743, η2P = 0.005—small effect size). However, for the moments, differences were observed for both scales (RPE: pvalue = 0.001, η2P = 0.519—large effect size; RPR: pvalue = 0.001, η2P = 0.607—large effect size).

Mean and standard deviation for the rate of perceived recovery (a) and exertion (b) scale in both protocols. Legend: Rec 1 = 1st minute of recovery; Rec 3 = 3rd minute of recovery; Rec 5 = 5th minute of recovery; Rec 7 = 7th minute of recovery; Rec 10 = 10th minute of recovery; Res = initial rest; Ex 15 = 15th of treadmill exercise; Ex 35 = 35th minute of treadmill exercise; RPR rate of perceived recovery; RPE rate of perceived exertion. *Difference between Rec 1 and other moments of recovery (a)/initial rest and recovery (b) of control protocol (pvalue < 0.001); #Difference between Rec 1 and other moments of recovery (a)/initial rest and recovery (b) of hydration protocol (pvalue < 0.001).
Discussion
The results revealed that the hydration did not promote significant differences between the protocols for the vagal reactivation, autonomic modulation recovery, RPE, and RPR after a moderate-intensity session of exercise. However, small anticipation of vagal reactivation, autonomic modulation recovery, and RPE was observed when the hydration protocol was performed.
It is reported that hypohydration/dehydrated states promote a linear increase in body temperature40. However, it was not observed in the present study. This suggests that the exercise model used in CRP, even without fluid replacement, does not promote significant hypohydration/dehydration, which contributes to the safety of these programs, considering the deleterious effects of dehydration in the cardiovascular system. However, the hydration strategy used in our study was efficient to avoid fluid losses, as the body mass did not change in the HP.
The analysis of the RMSSD30, a marker of the parasympathetic modulation30, demonstrated the physiological gradual increase of vagal activity during recovery8. In the HP, the vagal reactivation may have occurred sooner, since, after the first minute of recovery, the RMSSD30 was no longer significantly different from the rest and, at the first 30 s of recovery the parasympathetic modulation was significantly higher than at the exercise. In the CP, the RMSSD30 did not return to the rest values and only became significantly higher than the exercise after the first minute of recovery. However, these results should be analyzed with caution due to the non-significant difference between the protocols and small effect sizes.
After exercise, the decrease of HR depends on the vagal reactivation8. The higher HRR1 observed at HP, even without significant difference between protocols, suggests a small acceleration of the parasympathetic reactivation at HP, in accordance with the RMSSD30 results. The low HRR1 and high HRR2 in the CP evidence a slower HR recovery when the volunteers did not ingest water. This response was not observed in HP, where HRR1 was as high as HRR2. Also, this faster HR reduction could explain the faster reduction of the RPE after exercise with water intake, since it is reported that the RPE scale correlates to the HR37.
The HRV indexes analyzed in 5-min windows had a physiological and similar response in both protocols. The significant increase of SDNN, which represents the global modulation at REC1 and its return to the rest value at REC2, in both protocols may be related to the vagal reactivation, evidenced in this study through the RMSSD30. In addition, the passive recovery in the orthostatic position for 10 min was insufficient to promote the total recovery of the parasympathetic modulation, even with the hydration.
This is the first study to investigate the influence of hydration in the immediate autonomic recovery of CAD subjects. This topic was previously studied in health and young males, who ingested 500 ml of water in a single dose immediately after moderate and high-intensity exercises14,15,17 and had a positive effect on the vagal reactivation and autonomic modulation recovery.
However, in our study, the volunteers ingested an individualized amount of water in fractionated doses throughout the exercise, as suggested by the American College of Sports Medicine23. The total amount of water ingested was 0.345 ± 0.11L, which was sufficient to avoid the fluid losses and, even if not significant, it promoted small anticipation of the recovery. However, if it is enough to minimize the appearance of sudden events during the recovery period is still an aspect that needs to be further studied.
Furthermore, another factor that may be responsible for the low effect of the hydration strategy used in our study is the exercise intensity proposed. The exercise in our experiment was performed bellow the anaerobic threshold, that classifies it as low-moderate intensity26, and it is known in the literature that, in healthy and young subjects, the higher the exercise intensity, the higher the sweating rate, fluid losses40, and the cardiovascular41 and autonomic12 perturbations. Thus, this aspect may justify the low effect of the hydration in the vagal reactivation, HRR and RPE.
As a study limitation, the randomization of the protocols was not possible because the amount of water ingested was obtained by assessing body mass loss after the CP. However, all participants were familiar with the proposed exercise protocol, so we believe that the exercise model performed in the study did not influence the outcomes analyzed.
Despite the small and non-significant effects between protocols found in the present study in the immediate recovery period of a cardiac rehabilitation session, the investigation of new hydration strategies capable of accelerating the recovery in CAD subjects is important and should be encouraged, since those individuals present an autonomic impairment1 and have a less efficient recovery after exercise. Therefore, from our preliminary results, new studies that include larger samples and that insert randomization of different hydration strategies during exercise, can be designed. In addition, it may be interesting to analyze a longer recovery period to understand the impact of hydration strategies on the autonomic behavior in the recovery period of CAD patients.
Conclusions
The hydration protocol performed did not promote significative changes in the vagal reactivation, autonomic modulation recovery, and rate of perceived exertion and recovery, when compared to the control protocol. However, the hydration protocol avoided the fluid losses induced by exercise and promoted small anticipation of vagal reactivation and autonomic modulation recovery and a small reduction at the rate of perceived exertion.
References
Floras, J. S. & Ponikowski, P. The sympathetic/parasympathetic imbalance in heart failure with reduced ejection fraction. Eur. Heart J. 36, 1974–1982 (2015).
Qiu, S. et al. Heart rate recovery and risk of cardiovascular events and all-cause. J. Am. Heart Assoc. 6, 1–12 (2017).
Hsu, C., Hsieh, P., Hsiao, S. & Chien, M. Effects of exercise training on autonomic function in chronic heart failure: systematic review. Biomed. Res. Int. 2015, 1–8 (2015).
Feiereisen, P. & Delagardelle, C. Retrospective analysis of cardiac events during cardiac rehabilitation at Centre Hospitalier de Luxembourg during 2014 and 2015. Bull. Soc. Sci. Med. Grand. Duche Luxemb. 2, 13–25 (2016).
Pavy, B., Iliou, M. C., Meurin, P., Tabet, J. Y. & Corone, S. Safety of exercise training for cardiac patients: results of the French registry of complications during cardiac rehabilitation. Arch. Intern. Med. 166, 2329–2334 (2006).
Romero, S. A., Minson, C. T. & Halliwill, X. J. R. Recovery from exercise the cardiovascular system after exercise. J. Appl. Physiol. 122, 925–932 (2017).
Luttrell, M. J. & Halliwill, J. R. Recovery from exercise: vulnerable state, window of opportunity, or crystal ball?. Front. Physiol. 6, 1–6 (2015).
Peçanha, T., Silva-Júnior, N. D. & Forjaz, C. L. D. M. Heart rate recovery: autonomic determinants, methods of assessment and association with mortality and cardiovascular diseases. Clin. Physiol. Funct. Imaging 34, 327–339 (2014).
Imai, K. et al. Vagally mediated heart rate recovery after exercise is accelerated in athlestes but blunted in patients with chronic heart failure. J. Am. Coll. Cardiol. 24, 1529–1535 (1994).
Thompson, P. D. et al. Exercise and acute cardiovascular events: placing the risks into perspective a scientific statement from the American heart association council on nutrition, physical activity, and metabolism and the council on clinical cardiology. Circulation 115, 2358–2369 (2007).
Shibasaki, M., Wilson, T. E. & Crandall, C. G. A physiological systems approach to human neural control and mechanisms of eccrine sweating during heat stress and exercise. J. Appl. Physiol. 100, 1692–1701 (2006).
Castro-Sepúllveda, M. et al. Hydration status after exercise affect resting metabolic rate and heart rate variability. Nutr. Hosp. 31, 1273–1277 (2015).
Charkoudian, N., Halliwill, J. R., Morgan, B. J., Eisenach, J. H. & Joyner, M. J. Influences of hydration on post-exercise cardiovascular control in humans. J. Physiol. 552, 635–644 (2003).
de Oliveira, T. P., Ferreira, R. B., de Mattos, R. A., da Silva, J. P. & de Lima, J. R. P. Influence of water intake on post-exercise heart rate variability recovery. J. Exerc. Physiol. Online 14, 97–105 (2011).
Peçanha, T. et al. Water intake accelerates parasympathetic reactivation after high-intensity exercise. Int. J. Sport Nutr. Exerc. 24, 489–496 (2014).
Teixeira, A. L. et al. The role of water intake on cardiac vagal reactivation after upper-body resistance exercise. Int. J. Sport Med. 36, 204–208 (2015).
Vianna, L. C., Oliveira, R. B., Silva, B. M., Ricardo, D. R. & Araújo, C. G. S. Water intake accelerates post-exercise cardiac vagal reactivation in humans. Eur. Appl. Physiol. 102, 283–288 (2008).
Moreno, I. L. et al. Effects of an isotonic beverage on autonomic regulation during and after exercise. J. Int. Soc. Sport Nutr. 10, 1–10 (2013).
Vanderlei, F. M., Moreno, I. L., Carlos, L., Vanderlei, M. & Pastre, C. M. Effects of different protocols of hydration on cardiorespiratory parameters during exercise and recovery. Int. Arch. Med. 6, 1–10 (2013).
Vanderlei, F. M. et al. Comparison of the effects of hydration with water or isotonic solution on the recovery of cardiac autonomic modulation. Int. J. Sport Nutr. Exerc. 25, 145–153 (2015).
Dwan, K., Li, T., Altman, D. G. & Elbourne, D. CONSORT 2010 statement: extension to randomised crossover trials. BMJ 366, l4378 (2019).
Catai, A. M. et al. Heart rate variability: are you using it properly? Standardisation checklist of procedures. Braz. J. Phys. Ther. 20, 91–102 (2019).
American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription (Wolters Kluwer, 2014).
Meneghelo, R. S. et al. III Diretrizes da Sociedade Brasileira de Cardiologia Sobre Teste Ergométrico. Rev. Bras. Fisioter. 95, 1–26 (2011).
Cabral-Santos, C. et al. Similar anti-inflammatory acute responses from moderate-intensity continuous and high-intensity intermittent exercise. J. Sport Sci. Med. 14, 849–856 (2015).
Mezzani, A. et al. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: a joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitat. Eur. J. Prev. Cardiol. 20, 442–467 (2013).
Sawka, M. N. et al. Exercise and fluid replacement. Med. Sci. Sport Exerc. 39, 377–390 (2007).
Armstrong, L. E. Hydration assessment techniques. Nutr. Rev. 63, S40–S54 (2005).
Peçanha, T. et al. Methods of assessment of the post-exercise cardiac autonomic recovery: a methodological review. Int. J. Cardiol. 227, 795–802 (2017).
Vanderlei, L. C. M., Pastre, C. M., Hoshi, R. A., Carvalho, T. D. & Godoy, M. F. Basic notions of heart rate variability and its clinical applicability. Rev. Bras. Cir Cardiovasc. 24, 205–217 (2009).
Vanderlei, L. C. M., Silva, R. A., Pastre, C. M., Azevedo, F. M. & Godoy, M. F. Comparison of the Polar S810i monitor and the ECG for the analysis of heart rate variability in the time and frequency domains. Braz. J. Med. Biol. Res. 41, 854–859 (2008).
Goldberger, J. J. et al. Assessment of parasympathetic reactivation after exercise. Am. J. Physiol. Heart Circ. Physiol. 290, H2446–H2452 (2006).
Gutierrez, M. G., Ribeiro, F., Gomes, R. L., Valenti, V. E. & Vanderlei, L. C. M. Impact of musical auditory stimulation applied during and after aerobic exercise on vagal reentry in recovery period. J. Cardiol. Ther. 4, 588–593 (2017).
Nunan, D. et al. Validity and reliability of short-term heart-rate variability from the Polar S810. Med. Sci. Sports Exerc. 41, 243–250 (2009).
Tarvainen, M. P., Niskanen, J. P., Lipponen, J. A., Ranta-aho, P. O. & Karjalainen, P. A. Kubios HRV–heart rate variability analysis software. Comput. Methods Prog. Biomed. 113, 210–220 (2014).
Chen, J.-L. et al. Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training. J. Strength Cond. Res. 25, 1546–1552 (2011).
Borg, G. A. V. Psychophysical bases of perceived exertion. Med. Sci. Sport Exerc. 14, 377–381 (1982).
Laurent, C. et al. A practical approach to monitoring recovery: development of a perceived recovery status scale. J. Strength Cond. Res. 25, 620–628 (2011).
Maher, J. M., Markey, J. C. & Ebert-may, D. The other half of the story: effect size analysis in quantitative research. CBE Life Sci. Educ. 12, 345–351 (2013).
Mcdermott, B. P. et al. National athletic trainers’ association position statement: fluid replacement for the physically active. J. Athl. Train. 52, 877–895 (2017).
González-Alonso, J., Mora-Rodríguez, R. & Coyle, E. F. Stroke volume during exercise: interaction of environment and hydration. Am. J. Physiol. Heart Circ. Physiol. 278, 321–330 (2000).
Acknowledgements
We would like to thank the Foundation for Research Support of the State of São Paulo (FAPESP) and the Laboratory of Cell Physiology of Exercise (LAFICE) for having provided the space and equipment.
Funding
This work was supported by the Foundation for Research Support of the State of São Paulo (FAPESP) under Grant Number 2017/03142–1 and by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) under Grant Number 401258/2016–5.
Author information
Authors and Affiliations
Contributions
M.J.L.L., A.K.F.d.S., L.M.V., L.C.M.V. wrote the main manuscript text. M.J.L.L., A.K.F.d.S., L.A.S., F.R., L.M.V. were responsible for designing the study. M.J.L.L., A.K.F.d.S., L.A.S., F.R., D.A.G.C. monitored the study development. M.J.L.L., L.M.V., L.C.M.V. decided and performed the analytic strategy. M.J.L.L., L.A.S., F.R., D.A.G.C. collected and handled the data. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Laurino, M.J.L., da Silva, A.K.F., Santos, L.A. et al. Vagal reactivation after a cardiac rehabilitation session associated with hydration in coronary artery disease patients: crossover clinical trial. Sci Rep 11, 10482 (2021). https://doi.org/10.1038/s41598-021-89840-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89840-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
