
Abstract
Formaldehyde (FA) is a human carcinogen used as formalin in hospital laboratories. We evaluated its association with human chromosomal aberrations (CAs) and the risk/protective role played by several genetic polymorphisms in this relationship, on a cohort of 57 exposed pathologists vs 48 controls. All subjects were assessed for CAs on peripheral blood lymphocytes and genotyped for the most common cancer-associated gene polymorphisms which could be related with the genotoxic outcome: CYP1A1 exon 7 (A>G), CYP1A1*2A (T>C), CYP2C19*2 (G>A), GSTT1 (Positive/Null), GSTM1 (Positive/null), GSTP1 (A>G), XRCC1 (G399A), XRCC1 (C194T), XRCC1 (A280G), XPD (A751C), XPC exon 15 (A939C), XPC exon 9 (C499T), TNFα − 308 (G>A), IL10 − 1082 (G>A), IL10 − 819 (C>T) and IL6 − 174 (G>C). Air-FA concentration was assessed through personal samplers. The comparison between pathologists and controls showed a significantly higher CAs frequency in pathologists. Significant positive correlations were found between CAs frequency and air-FA concentration while significant associations were found between variation in CAs frequency and the mutated allele for CYP1A1 exon 7 (A>G), CYP2C19*2 (G>A), GSTT1-positive, GSTM1-positive and XRCC1 (G399A). Our study confirms the role of FA as genotoxicity inductor, even in workers chronically exposed to low air-FA levels and reveals the role played by some genetic polymorphisms in this association, highlighting the importance of individual susceptibility biomarkers assessment in occupational health studies.
Similar content being viewed by others

Introduction
Formaldehyde (FA) is a compound produced worldwide and employed in an extremely wide variety of industrial and medical processes1, resulting in a widespread exposure in both environmental and occupational contexts2. As it is well-known, FA is responsible of several biological effects, even at lower concentrations than those recommended by the American Conference of Governmental Industrial Hygienists (ACGIH)3,4. Workers exposed to FA are at increased risk of cancer, especially nasopharyngeal cancer and myeloid leukaemia5. Due to these effects, FA is classified as a group I human carcinogen by the International Agency for Research on Cancer (IARC) since 20065,6,7; nevertheless, considerable discrepancies remain among guidelines suggested for occupational exposure to FA. The ACGIH recommended a Threshold Limit Value-Ceiling (TLV-C) of 0.3 ppm until 2016; the value was then dropped to a Time Weighted Average (TLV-TWA) of 0.1 ppm (0.120 mg/m3) and a Short Term Exposure Limit (TLV-STEL) of 0.3 ppm (0.370 mg/m3). Conversely, the European Scientific Committee on Occupational Exposure Limits recently suggested a FA-related TWA of 0.3 ppm, but a STEL of 0.6 ppm (0.740 mg/m3)8.
Formalin is an aqueous solution usually containing 37–40% by weight of dissolved FA: its easy preparation and low cost make this compound the main cytological fixative in pathology laboratories worldwide9,10. Despite these advantages, the health and safety risks associated with formalin use are currently a matter of concern and FA toxicity is nowadays the main issue for its abolition in pathology laboratories3,10,11. Moreover, chronic exposures to FA, such as those present in workplaces, are suspected to be related to genotoxic effects9.
The FA genotoxic effect in occupationally exposed workers is still debated. Cytogenetic outcomes, such as increased chromosomal aberrations (CAs) and micronucleated cells (MNc), were reported in some bio-monitoring studies12,13 on chronic exposures, while this evidence was lacking in other published reports14,15.
However, the genomic damage level due to occupational exposure to xenobiotics depends also on the individual susceptibility. From the genetic point of view, this is due to polymorphisms in a battery of genes, mainly involved in metabolic and DNA-repair pathways16.
Phase I metabolic enzymes mostly consist of the cytochrome P450 (CYP) superfamily of microsomal enzymes17 catalysing oxidative reactions18, while phase II enzymes, such as glutathione S-transferases (GSTs), role is to increase the hydrophilicity of the xenobiotic compounds through conjugation reactions17. FA is quickly detoxified in the nasal tissues by oxidative reactions catalysed by glutathione-dependent and independent dehydrogenases, primarily the alcohol dehydrogenase 519.
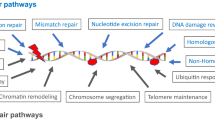
In order to safeguard the genome’s integrity and to prevent the potentially mutagenic consequences of DNA modifications, the cells evolved several mechanisms of DNA repair, according to the type of damage. The Base Excision Repair (BER) and the Nucleotide Excision Repair (NER) correct DNA small base changes (oxidation or alkylation) and bulky adducts, pyrimidine dimers and inter-strand cross-links, respectively20. These DNA-repair genes, which are involved in the protection mechanism against cancer development, are polymorphic20. Several evidences reported that defects in these DNA repair mechanisms could reduce FA tolerance at cellular level21.
Finally, several lines of evidence recently showed the FA role as oxidative stress inductor3,22. This imbalance between the production of Reactive Oxygen Species (ROS) and the capacity of the antioxidant system to counteract them, leads to biomolecular damages triggering inflammation, testified by massive proinflammatory cytokine release23, which is in turn related to carcinogenesis. Some cytokine gene polymorphisms, moreover, were found to modulate the amount of genomic damage associated with inflammatory and cancer diseases. As example, TNF-α, IL-2, IL-6, and TGF-β1 polymorphisms have been showed to influence CAs level in cultured human peripheral blood lymphocytes (PBL)24,25,26. Despite of all these lines of evidence, the role of cytokine gene polymorphisms in modulating the FA exposure associated damage has not been completely clarified yet26.
In order to better elucidate the chronic FA genotoxic effect, we evaluated CAs frequency in PBL of pathologists chronically exposed to low air-FA concentration. This allows the detection of cells carrying unstable aberrations (i.e. chromosome and chromatid breaks, fragments) leading, in turn, to cell death during proliferation27. An increased CAs frequency in PBL is, thus, a powerful predictor of cancer risk significantly associated with the early events of carcinogenesis, as confirmed by previous studies in literature28. In order to evaluate the individual susceptibility role, sampled subjects were assessed for phase I, phase II, and DNA-repair gene polymorphisms, involved in the biotransformation, inactivation, and the DNA-repair processes, respectively. We analysed the most studied cancer-associated gene polymorphisms29,30, namely Cytochrome P450 1A1 (CYP1A1) exon 7 (A>G) CYP1A1 2A (T>C), CYP2C19*2 (G>A), GSTT1, GSTM1, GSTP, X-ray repair cross-complementing group 1 (XRCC1) 399 (G>A), 194 (C>T), 280 (A>G), Xeroderma pigmentosum complementation group C (XPC) exon 15 (A>C), XPC exon 9 (C>T) and Xeroderma pigmentosum complementation group D (XPD) (A>C). Finally, since cytokines play a fundamental role in the inflammatory process leading to genomic damage26, we assessed polymorphisms in TNF-α (− 308, G>A), IL-10 − 1082 (G>A), IL-10 (− 819, C>T), IL-6 (− 174, G>C) as well.
The aim of the present study is thus to evaluate the role of chronic occupational FA exposure risk levels and the role of some genetic polymorphisms as possible modulators of genotoxic effects, in workers chronically exposed to low air-FA concentrations.
Results
The epidemiologic sample includes 57 pathologists and 48 controls. In Table 1 are reported the demographic characteristics of the study population and the measured air-FA concentration on the sampling day. As expected, pathologists turned out to be exposed to an air-FA concentration significantly higher than controls (p < 0.001). No significant differences were found, instead, between the two groups concerning confounding factors such as sex, age, smoking habits and years of employment.
In Table 2 the level of genotoxic damage in the two sample groups is reported. We found three types of aberrations: chromatid break, chromosome break and acentric fragment. As can be seen, when compared to the control group, pathologists showed higher CAs and Ab.C frequencies (p < 0.001). The difference in CAs frequency between exposed and controls subjects is shown in Fig. 1.

CAs frequency in exposed and control groups.
The analyses of correlations performed on the whole sample showed a significant positive correlation between age and years of employment (r = 0.83, p < 0.001), CAs and Ab.C frequencies (r = 1.00, p < 0.001), CAs frequency and air-FA concentration (r = 0.33, p < 0.001) and, lastly, Ab.C frequency and air-FA concentration (r = 0.33, p < 0.001).
Multiple linear regressions were carried out to investigate the influence of the genetic profile in CAs frequency.
The model (Model M0) includes all genetic polymorphisms (wt vs carriers of at least one mutated allele) and confounding factors. There was a significant relationship between CAs frequency and exposure to air-FA (β = 1.027; p < 0.001), CYP1A1 exon 7 (A>G) (β = 0.353; p = 0.019), CYP2C19*2 (G>A) (β = 0.504; p = 0.007), GSTT1-positive (β = − 0.447; p = 0.004), GSTM1-positive (β = − 0.533; p = 0.001) and XRCC1 (399, G>A) (β = − 0.331; p = 0.044) genotypes. A tendency in increasing CAs frequency, albeit not significant, was found for IL-10 1082 (G>A) genotype (β = 0.292; p = 0.054). Figure 2 shows the Relative Risk (RR) of developing CAs according to the presence of mutated allelic variants of the gene considered.

RR (95% CI) of developing CAs according to the various mutated allelic variants of genes considered in the present study, FA exposure and confounding factors as age, years of exposure, sex and cigarette/day (Model M0).
Discussion
Despite the growing awareness regarding the harmful effects of air-FA exposure, FA is currently employed in hospital pathology laboratories raising concerns about pathologists safety31,32.
Many studies demonstrated the FA genotoxicity both in vitro and in vivo, considering various biological systems and endpoints5. Moreover, occupational and environmental exposures are often chronic and mixed, and the analysis of their outcomes should take into account also the eventuality of a cumulative genomic instability induced by chronic exposures33.
As expected, we found significantly higher CAs and Ab.C frequencies in pathologists than in controls, in agreement with literature evidence, even though conflicting results can be found12,34,35. In this regard, Costa et al.34 reported that even at an average FA concentration of 0.38 ppm (i.e., 0.47 mg/m3) frequencies of cytogenetic parameters, such as CAs, were significantly higher in pathologists than in controls. In order to explain the mechanisms leading to FA-induced genotoxicity, several hypotheses have been proposed: DNA–protein cross-links, damage to proteins required for the mitotic process and reduced expression of paxillin, an essential component of the abscission machinery required to complete cytokinesis, which may lead, respectively, to DNA replication stress and DNA breaks, chromosome malsegregation during nuclear division and cytokinesis failure leading to micronucleus formation and aneuploidy7. Moreover, the inflammatory process, due to the activation of neutrophils and eosinophils and/or the altered redox balance in the bone-marrow could play a central role in DNA strand breaks induced by ROS7.
The harmful effects of xenobiotics exposure is extremely shaped by individual susceptibility. The analysis of metabolic and DNA-repair gene polymorphisms in risk assessment of hazardous chemicals assume thus particular importance5,26.
In this context, we focused on the role of several genetic polymorphisms in modulating CAs frequency in subjects occupationally exposed to air-FA compared to a control group.
We found a significant effect of some genetic polymorphisms in CAs frequency modulation, even among genes coding for enzymes not directly involved in FA metabolism.
Specifically, among genes coding for phase I metabolism enzymes, we found a significant increase in CAs frequency in carriers of CYP1A1 exon 7 (A>G) and CYP2C19*2 (G>A) polymorphisms. These genes are members of the cytochrome P450 superfamily of enzymes, mixed-function mono-oxygenases responsible for metabolizing, mainly via oxidative reactions, several exogenous and endogenous compounds, including steroids, fatty acids, retinoid, drugs, vitamins, procarcinogens/promutagens, and environmental compounds36,37.
The CYP1A1 Ile462Val substitution in the heme-binding domain of exon 7, leads to a concurrent increase in the catalytic activity of the protein and was associated with lung cancer risk38,39. The Ile/Ile genotype was also found to be associated with an increase of aberrant cells, and to be a CAs predictor40. Contrary, other studies did not find any association41.
Common variants of the CYP2C19 gene are associated with impaired drug metabolism. CYP2C19*2 results from a guanine (G) to adenine (A) transition at position 681 in exon 5, producing an aberrant splicing site and encoding enzymes with decreased activity42. This polymorphism was related to genotoxicity in a previous study of Santovito et al., where CYP2C19 A/A subjects turned out to show a frequency of sister chromatid exchanges (SCEs) significantly higher with respect to the CYP2C19 G/G homozygote genotypes43.
In phase II enzymes, we found a significant CAs frequency decrease in GSTT1-positive and GSTM1-positive subjects. Accordingly, the higher frequency of genotoxic damage in carriers of the null-allele could be explained considering the role of these genes and their mutations on metabolism. The glutathione S-transferases represent an important group of enzymes, which detoxify both endogenous and exogenous compounds, included pharmaceuticals and environmental pollutants44. The GSTM1 and GSTT1 polymorphisms consist both in the deletion of a part of the gene, leading, in homozygous individuals, to a lack of the enzyme activity45. In literature, the GSTM1-null and GSTT1-null genotypes have been related to increased risk for several cancers, such as lung and colorectal cancer45. These are enzymes directly involved in the FA metabolism. Due to its high-water solubility and reactivity, indeed, airborne FA is absorbed mainly (~ 90%) in the upper respiratory tract, where it quickly forms intermolecular and intramolecular cross-links within proteins and nucleic acids at the site of contact. It is also rapidly metabolized to formate by FA-dehydrogenase requiring glutathione: the depletion of this compound in the absorbing tissues results in more FA bound to DNA within cells46,47. While some reports showed no effect of these polymorphisms in modulating the level of genomic damage12,34,45,46, others found a significant association. As example, Santovito et al.43 observed higher frequencies of SCEs, CAs, and Ab.C among pathologists with GSTT1-null genotypes than in the reference group. Several other epidemiological studies evaluating exposure to organic solvents, reported the GSTM1-null genotype associated with an increase in cytogenetic biomarkers, probably due to the absence of detoxification activity that may affect the amount of DNA damage48,49.
Since DNA damage is a key step in the carcinogenic process50, we also considered polymorphisms in both BER and NER pathways. Unexpectedly, we found a significant relationship only for XRCC1 (399, G>A) polymorphism, which turned out to be related to a reduction in CAs frequency. The X-ray cross-complementing group 1 (XRCC1) is a major DNA repair gene involved in base BER, which is able to fix DNA base damage and single-strand breaks through interacting with DNA components at the damage site. The polymorphisms related to this gene have been linked to the development of several types of cancer51,52. Specifically, the XRCC1 Arg399Gln polymorphism has been reported to reduce the oxidative damage repair activity and the 399Gln allele has been shown to be related to higher mutagen sensitivity and higher levels of DNA adducts53. Therefore, our result appears to be inconsistent with the gene function. Nevertheless, in literature contrasting results can be found. In workers exposed to organic solvents, Hoyos-Giraldo et al. reported that the XRCC1 Arg399Gln polymorphism carriers did not have a significant CAs frequency increase compared to the wild type genotype carriers. Contrary, in benzene-exposed workers, a significant CAs frequency increase related to by XRCC1 Arg399Gln variant was reported48. As well, in a study on active and passive smokers, Gln/Gln carriers reveal a significantly higher number of aberrations than the Arg/Gln and Arg/Arg genotypes in both the controls and exposed subjects54.
No significant relationship was found between CAs frequency and XRCC1 (280, A>G) polymorphism, even though in literature this association has been reported48.
Finally, inflammation and oxidative stress are knowingly interdependent pathophysiological processes55. Since these are two possible mechanisms through which FA could explain its harmful effects, we evaluated the role of polymorphisms on both pro- and anti-inflammatory cytokines genes. No significant result was found, according to the study of Santovito et al.26, which found no association between cytogenetic damage and TNFα − 308 (G>A), IL10 − 1082 (G>A) and IL10 − 819 (C>T) gene polymorphisms, with the only exception of homozygous genotypes for IL-6 G allele, that showed a significant decrease in the frequency of SCEs compared to heterozygous subjects.
These results, however, should be considered cautiously, as we did not consider the eventual effect of all the possible confounding factors that could modulate the studied outcomes, such as the plethora of chemicals to whom pathologists could be exposed in various degrees in laboratories.
Conclusions
Our study confirms FA genotoxic effect, even in workers chronically exposed to low FA levels. Several genetic polymorphisms in metabolism and DNA-repair pathways seem to have an influence in modulating the effect of FA exposure. These findings further highlight the importance of individual susceptibility biomarkers assessment in occupational studies. Due to the extreme FA widespread presence in environmental and occupational settings, studies on both harmful effects related to FA exposure and modulators are crucial to elaborate effective Public Health preventive strategies.
Materials and methods
Epidemiological sample
The epidemiological sample consist of 57 workers occupationally exposed to FA enrolled in two pathology wards of Turin (Italy) and forty-eight hospital workers not exposed to FA recruited in the same two hospitals as control group. Each volunteer signed an informed consent form. The sampling was performed on Wednesday of each sampling week, engaging five to eight subjects every time. Since, routinely, the exposure to FA in pathology wards occurs mainly via inhalation, each participant wore a personal passive sampler for the measurement of air-FA concentration during the sampling-day work shift. At 4 p.m. of the same day, each subject provided a venous blood sample and answered to a questionnaire administered by one interviewer. The study was approved by the Bioethical Committee of the University of Turin and was performed in accordance with the ethical standards laid down in the 2013 Declaration of Helsinki.
Questionnaire
The questionnaire was administered to each subject by an interviewer to obtained information about demographic characteristics (sex, age), personal habits (smoking) during the last year, and work characteristics (length in years of service working and type of work).
Personal air-FA collection and analysis
FA air samples were collected for working shift (8 h) on Wednesday using passive personal air samplers clipped near the breathing zone of the subject, according to Santovito et al.12.
Blood sample collection and chromosomal aberration analysis
Blood sample collection and chromosome aberration analysis were performed according to Santovito et al.12. DNA extraction and genotyping procedure were carried out as described in Ruberto et al.56. Primer sequences, melting temperatures, PCR methodologies used, and expected PCR product sizes are reported in Supplementary Table S1 online.
Statistical analyses
Statistical analysis was assessed using the SPSS software statistical package programme (version 22.0, Chicago, USA) and R (R version 4.0.2). Differences between sex, mean age and years of employment (y.e.) among and between groups were evaluated by analysis of variance. A non-parametric Kruskal–Wallis test was used to compare age, mean y.e. and CAs frequency between groups.
Multivariate general linear model, with Bonferroni’s correction, was used to evaluate the influence of age and years of exposure on CAs frequency in both groups. All p-values were two tailed and the level of statistical significance was set at p < 0.05 for all tests.
Association between both genetic and environmental variables with the level of genomic damage was evaluated by Poisson regression model, due to a Poisson nature and distribution of the dependent variable (CAs) (Supplementary Fig. S1 online). Genetic variables were considered both in binarized (wild type vs. any mutated allele) and multiallelic (wild type vs. heterozygous vs. homozygous).
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Costa, S. et al. Cytogenetic and immunological effects associated with occupational formaldehyde exposure. J. Toxicol. Environ. Health. Part A Curr. Issues 76, 217–229 (2013).
Viegas, S. et al. Genotoxic effects in occupational exposure to formaldehyde: A study in anatomy and pathology laboratories and formaldehyde-resins production. J. Occup. Med. Toxicol. 5, 25 (2010).
Bellisario, V. et al. Towards a formalin-free hospital. Levels of 15–F2t-isoprostane and malondialdehyde to monitor exposure to formaldehyde in nurses from operating theatres. Toxicol. Res. 5, 1122–1129 (2016).
Romanazzi, V. et al. 15–F2t isoprostane as biomarker of oxidative stress induced by tobacco smoke and occupational exposure to formaldehyde in workers of plastic laminates. Sci. Total Environ. 442, 20–25 (2013).
Costa, S. et al. Occupational exposure to formaldehyde and early biomarkers of cancer risk, immunotoxicity and susceptibility. Environ. Res. 179, 108740 (2019).
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, World Health Organization, & International Agency for Research on Cancer. Formaldehyde, 2-Butoxyethanol and 1-tert-Butoxypropan-2-ol. (International Agency for Research on Cancer, 2006).
Fenech, M., Nersesyan, A. & Knasmueller, S. A systematic review of the association between occupational exposure to formaldehyde and effects on chromosomal DNA damage measured using the cytokinesis-block micronucleus assay in lymphocytes. Mutat. Res. Rev. Mutat. Res. 770, 46–57 (2016).
Dugheri, S. et al. An integrated air monitoring approach for assessment of formaldehyde in the workplace. Saf. Health Work 9, 479–485 (2018).
Ladeira, C. et al. Genotoxicity biomarkers in occupational exposure to formaldehyde—The case of histopathology laboratories. Mutat. Res. Toxicol. Environ. Mutagen. 721, 15–20 (2011).
Zanini, C., Gerbaudo, E., Ercole, E., Vendramin, A. & Forni, M. Evaluation of two commercial and three home-made fixatives for the substitution of formalin: A formaldehyde-free laboratory is possible. Environ. Health. A Glob. Access Sci. Source 11, 59 (2012).
Patil, S., Rao, R. S., Ganavi, B. S. & Majumdar, B. Natural sweeteners as fixatives in histopathology: A longitudinal study. J. Nat. Sci. Biol. Med. 6, 67–70 (2015).
Santovito, A. et al. Combined analysis of chromosomal aberrations and glutathione S-transferase M1 and T1 polymorphisms in pathologists occupationally exposed to formaldehyde. Arch. Toxicol. 85, 1295–1302 (2011).
Souza, A. D. & Devi, R. Cytokinesis blocked micronucleus assay of peripheral lymphocytes revealing the genotoxic effect of formaldehyde exposure. Clin. Anat. 27, 308–312 (2014).
Pala, M. et al. Occupational exposure to formaldehyde and biological monitoring of Research Institute workers. Cancer Detect. Prev. 32, 121–126 (2008).
Peteffi, G. P. et al. Environmental and biological monitoring of occupational formaldehyde exposure resulting from the use of products for hair straightening. Environ. Sci. Pollut. Res. 23, 908–917 (2016).
Crocco, P. et al. Inter-individual variability in xenobiotic-metabolizing enzymes: Implications for human aging and longevity. Genes 10, 403 (2019).
Xu, L. & Wei, H. Association between CYP1A1 2454A>G polymorphism and colorectal cancer risk: A meta-analysis. J. Cancer Res. Ther. 11, 760 (2015).
Almazroo, O. A., Miah, M. K. & Venkataramanan, R. Drug metabolism in the liver. Clin. Liver Dis. 21, 1–20 (2017).
Pontel, L. B. et al. Endogenous formaldehyde is a hematopoietic stem cell genotoxin and metabolic carcinogen. Mol. Cell 60, 177–188 (2015).
Langie, S. A. S. et al. Causes of genome instability: The effect of low dose chemical exposures in modern society. Carcinogenesis 36, S61–S88 (2015).
Reingruber, H. & Pontel, L. B. Formaldehyde metabolism and its impact on human health. Curr. Opin. Toxicol. 9, 28–34 (2018).
Bono, R. et al. Formaldehyde-induced toxicity in the nasal epithelia of workers of a plastic laminate plant. Toxicol. Res. 5, 752–760 (2016).
Hussain, T. et al. Oxidative stress and inflammation: What polyphenols can do for us? Oxid. Med. Cell. Longev. 2016, 7432797 (2016).
Higashimoto, T., Panopoulos, A., Hsieh, C. L. & Zandi, E. TNFα induces chromosomal abnormalities independent of ROS through IKK, JNK, p38 and caspase pathways. Cytokine 34, 39–50 (2006).
Westbrook, A. M. et al. The role of tumour necrosis factor-α and tumour necrosis factor receptor signalling in inflammation-associated systemic genotoxicity. Mutagenesis 27, 77–86 (2012).
Santovito, A. et al. Relationships between cytokine (IL-6 and TGF-β 1) gene polymorphisms and chromosomal damage in hospital workers. J. Immunotoxicol. 13, 314–323 (2016).
Garcia-Sagredo, J. M. Fifty years of cytogenetics: A parallel view of the evolution of cytogenetics and genotoxicology. Biochim. Biophys. Acta Gene Regul. Mech. 1779, 363–375 (2008).
Bonassi, S., Znaor, A., Norppa, H. & Hagmar, L. Chromosomal aberrations and risk of cancer in humans: An epidemiologic perspective. Cytogenet. Genome Res. 104, 376–382 (2004).
García-González, M. A. et al. Relevance of GSTM1, GSTT1, and GSTP1 gene polymorphisms to gastric cancer susceptibility and phenotype. Mutagenesis 27, 771–777 (2012).
Song, X. et al. Variants in nucleotide excision repair core genes and susceptibility to recurrence of squamous cell carcinoma of the oropharynx. Int. J. Cancer 133, 695–704 (2013).
Ogawa, M., Kabe, I., Terauchi, Y. & Tanaka, S. A strategy for the reduction of formaldehyde concentration in a hospital pathology laboratory. J. Occup. Health 61, 135–142 (2019).
D’Ettorre, G., Criscuolo, M. & Mazzotta, M. Managing formaldehyde indoor pollution in anatomy pathology departments. Work 56, 397–402 (2017).
Kirsch-Volders, M., Fenech, M. & Bolognesi, C. Validity of the lymphocyte cytokinesis-block micronucleus assay (L-CBMN) as biomarker for human exposure to chemicals with different modes of action: A synthesis of systematic reviews. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 836, 47–52 (2018).
Costa, S. et al. Increased levels of chromosomal aberrations and DNA damage in a group of workers exposed to formaldehyde. Mutagenesis 30, 463–473 (2015).
Jakab, M. G. et al. Formaldehyde-induced chromosomal aberrations and apoptosis in peripheral blood lymphocytes of personnel working in pathology departments. Mutat. Res. Toxicol. Environ. Mutagen. 698, 11–17 (2010).
Autrup, H. Genetic polymorphisms in human xenobiotica metabolizing enzymes as susceptibility factors in toxic response. In Mutation Research—Genetic Toxicology and Environmental Mutagenesis. 464, 65–76 ( 2000).
Pan, S. T. et al. Computational identification of the paralogs and orthologs of human cytochrome P450 superfamily and the implication in drug discovery. Int. J. Mol. Sci. 17, 1020 (2016).
Wright, C. M. et al. Genetic association study of CYP1A1 polymorphisms identifies risk haplotypes in nonsmall cell lung cancer. Eur. Respir. J. 35, 152–159 (2010).
Roszak, A., Lianeri, M., Sowińska, A. & Jagodziński, P. P. CYP1A1 Ile462Val polymorphism as a risk factor in cervical cancer development in the polish population. Mol. Diagn. Ther. 18, 445–450 (2014).
Sram, R. J. et al. Chromosomal aberrations in environmentally exposed population in relation to metabolic and DNA repair genes polymorphisms. Mutat. Res. Fundam. Mol. Mech. Mutagen. 620, 22–33 (2007).
Motykiewicz, G. et al. A molecular epidemiology study in women from Upper Silesia, Poland. Toxicol. Lett. 96–97, 195–202 (1998).
Dehbozorgi, M. et al. Prevalence of the CYP2C19∗2 (681 G>A), ∗3 (636 G>A) and ∗17 (-806 C>T) alleles among an Iranian population of different ethnicities. Mol. Med. Rep. 17, 4195–4202 (2018).
Santovito, A., Gendusa, C. & Cervella, P. Evaluation of baseline frequency of sister chromatid exchanges in an Italian population according to age, sex, smoking habits, and gene polymorphisms. Am. J. Hum. Biol. 29, e23034–e23041 (2017).
Nebert, D. W. & Vasiliou, V. Analysis of the glutathione S-transferase (GST) gene family. Hum. Genomics 1, 460–464 (2004).
Costa, S. et al. Genotoxic damage in pathology anatomy laboratory workers exposed to formaldehyde. Toxicology 252, 40–48 (2008).
Nielsen, G. D., Larsen, S. T. & Wolkoff, P. Re-evaluation of the WHO (2010) formaldehyde indoor air quality guideline for cancer risk assessment. Arch. Toxicol. 91, 35–61 (2017).
Haffner, M. J. et al. Formaldehyde exposure and its effects during pregnancy: Recommendations for laboratory attendance based on available data. Clin. Anat. 28, 972–979 (2015).
Hoyos-Giraldo, L. S., Carvajal, S., Cajas-Salazar, N., Ruíz, M. & Sánchez-Gómez, A. Chromosome aberrations in workers exposed to organic solvents: Influence of polymorphisms in xenobiotic-metabolism and DNA repair genes. Mutat. Res. Fundam. Mol. Mech. Mutagen. 666, 8–15 (2009).
Norppa, H. Cytogenetic biomarkers and genetic polymorphisms. In Toxicology Letters. 149, 309–334 (2004).
Sellappa, S., Balakrishnan, M., Raman, S. & Palanisamy, S. Induction of micronuclei in buccal mucosa on chewing a mixture of betel leaf, areca nut and tobacco. J. Oral Sci. 51, 289–292 (2009).
Qin, C. J. et al. XRCC1 R399Q polymorphism and colorectal cancer risk in the Chinese Han population: A meta-analysis. Tumor Biol. 36, 461–466 (2015).
Wu, Y. G. et al. The association of XRCC1 polymorphism with osteosarcoma risk, clinicopathologic features, and prognosis in a Chinese Han population. Cancer Manag. Res. 10, 4959–4967 (2018).
Takeshita, H., Fujihara, J., Yasuda, T. & Kimura-Kataoka, K. Worldwide distribution of four SNPs in X-ray and repair and cross-complementing group 1 (XRCC1). Clin. Transl. Sci. 8, 347–350 (2015).
Chandirasekar, R. et al. XRCC1 gene variants and possible links with chromosome aberrations and micronucleus in active and passive smokers. Environ. Toxicol. Pharmacol. 32, 185–192 (2011).
Biswas, S. K. Does the interdependence between oxidative stress and inflammation explain the antioxidant paradox?. Oxid. Med. Cell. Longev. 2016, 1–9 (2016).
Ruberto, S. & Santovito, A. Association of TGFβ1 codon 10 (T>C) and IL -10 (G>C) cytokine gene polymorphisms with longevity in a cohort of Italian population. Am. J. Hum. Biol. https://doi.org/10.1002/ajhb.23491 (2020).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization, R.B. and A.S.; Methodology, A.S.; Software, E.C., V.B. and G.S; Validation, A.S., V.B. and G.S.; Formal analysis, E.C., A.S. F.G., M.B.; Investigation, A.S. and F.G.; Resources, R.B.; Data curation, F.G. and M.B.; Writing—original draft preparation, F.G.; Writing—review and editing, F.G. and M.B.; Supervision, A.S. and R.B.; Project administration, A.S. and R.B.; Funding acquisition, A.S. and R.B.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghelli, F., Cocchi, E., Buglisi, M. et al. The role of phase I, phase II, and DNA-repair gene polymorphisms in the damage induced by formaldehyde in pathologists. Sci Rep 11, 10507 (2021). https://doi.org/10.1038/s41598-021-89833-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89833-w
This article is cited by
-
Microfluidic chip-based long-term preservation and culture of engineering bacteria for DNA damage evaluation
Applied Microbiology and Biotechnology (2022)
-
The formation of SCEs as an effect of occupational exposure to formaldehyde
Archives of Toxicology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
