
Abstract
Bioelectrical impedance techniques are easy to use and portable tools for assessing body composition. While measurements vary according to standing vs supine position in adults, and fasting and bladder voiding have been proposed as additional important influences, these have not been assessed in young children. Therefore, the influence of position, fasting, and voiding on bioimpedance measurements was examined in children. Bioimpedance measurements (ImpediMed SFB7) were made in 50 children (3.38 years). Measurements were made when supine and twice when standing (immediately on standing and after four minutes). Impedance and body composition were compared between positions, and the effect of fasting and voiding was assessed. Impedance varied between positions, but body composition parameters other than fat mass (total body water, intra- and extra-cellular water, fat-free mass) differed by less than 5%. There were no differences according to time of last meal or void. Equations were developed to allow standing measurements of fat mass to be combined with supine measurements. In early childhood, it can be difficult to meet requirements for fasting, voiding, and lying supine prior to measurement. This study provides evidence to enable standing and supine bioimpedance measurements to be combined in cohorts of young children.
Similar content being viewed by others

Introduction
Bioelectrical impedance techniques allow quick, easy measurement of body composition including, total body water (TBW), fat mass (FM), and fat-free mass (FFM). Multi-frequency techniques, including multi-frequency bioimpedance analysis (MFBIA) and bioimpedance spectroscopy (BIS), are further able to distinguish between intracellular (ICW) and extracellular fluids (ECW)1,2. Although not widely used in early childhood, bioimpedance techniques are easy to administer, are inexpensive, and require less co-operation from the child due to their fast measurement time in comparison to other widely used methods, such as dual-energy X-ray absorptiometry (DXA). However, there are many factors that may influence bioimpedance measurements and thus require standardisation3. These factors may be amplified in infants and young children, where compliance is a particular challenge4. One such factor is the requirement for children to lie supine for extended periods prior to measurement.
Brantlov et al.5 reported that of 71 studies identified which used bioelectrical impedance analysis to estimate body composition in populations of healthy children, authors did not consistently report in what body position (i.e., standing or supine) measurements were obtained. Of concern, only 21% reported how long the child was in the position prior to measurement. In adults, it has been shown that standing and supine measurements are not interchangeable and that it takes approximately 5 min for fluid stabilisation to occur to allow measurement of TBW6 and extended periods to establish ECW and ICW stabilisation6,7, which correspond to changes in impedance values8. As such, adult guidelines recommend that bioimpedance measurements be made in the supine position after 4 to 10 min have elapsed9,10. However, no guidelines exist for paediatric populations.
While studies in young children have explored some of the factors which influence impedance measurements, such as movement11 and electrode placement11,12,13, no study has evaluated the effect of body position. In young children, it may be more feasible to obtain bioimpedance measurements while the child is standing; however, it is unclear whether measurements taken in alternate body positions are interchangeable. In addition to recommendations about body position, adult guidelines state that bioimpedance measurements should be made when the subject is fasted and has voided their bladder9,10, as impedance parameters have been found to be modestly reduced following a meal or bladder void8,14,15; however, it is unclear what effect, if any, these factors may have on measurements in young children. Therefore, the aim of this study was to determine whether BIS measurements obtained in different body positions can be used interchangeably and whether fasting and bladder voiding influence associations.
Methods
Subjects
A convenience sample of children aged 3.38 years was selected from the Auckland site of the Nutritional Intervention Preconception and During Pregnancy to Maintain Healthy Glucose Metabolism and Offspring Health (“NiPPeR”) study16. Data were obtained from 50 children selected based on compliance with the NiPPeR BIS protocol (i.e., the child laid supine for ≥ 4 min prior to the initial measurement).
Ethics
The NiPPeR trial was registered on 16 July 2015 with ClinicalTrials.gov (NCT02509988, Universal Trial Number U1111-1171-8056); ethics approval was granted by the Northern A Health and Disability Ethics Committee (15/NTA/21/AM20). Written informed consent was obtained from the parents/guardians of the study subjects. All procedures in this study were conducted according to the ethical principles and guidelines laid down in the Declaration of Helsinki.
Experimental design
Children were measured in three body positions. First, as per the recommendation of Brantlov et al.3 (based on adult guidelines9,10), children were measured supine on non-conductive examination tables with the legs separated and arms by their sides without skin-to-skin contact between arms and the trunk, after at least four minutes had elapsed (thus allowing fluid stabilisation). Second, the children were measured immediately (within one minute) on standing (from being supine) while maintaining correct abduction of the arms and legs. Finally, children were measured in the same standing position after at least four minutes had elapsed. During this period, children were required to remain upright (standing or seated). For each body position, electrode placement remained the same, and it was ensured that the leads were not tangled or touching any metal surfaces. It was not possible to ensure that the leads were not touching the ground during the standing measurements due to the placement of the electrodes.
In addition, whether the child had fasted or voided their bladder was recorded. The effect of consumption of food or drink on impedance measurements has not been explored in preschool aged children. Evidence from infancy suggests that it is time after consumption, rather than volume, that is important11. Thus, time of last meal or drink (> 2 h ago, 1–2 h ago, 30 min–1 h ago, or ≤ 30 min ago) was recorded, as was time of last void. Time of last void was categorised according to whether or not the child had voided their bladder within half an hour of measurement. If the child consumed any food or fluid, or voided their bladder between measurement positions, this was recorded. These children were excluded from analyses evaluating the effect of fasting and voiding on differences in impedance between body positions (n = 5).
Bioelectrical impedance spectroscopy
Bioimpedance measurements were made with the ImpediMed SFB7 device (ImpediMed, Brisbane, Australia). This device measures bioimpedance parameters over a frequency range of 3 to 1000 kHz, resulting in 256 measurements per assessment17. Instrument calibration was checked daily prior to use using a test cell provided by the manufacturer. ImpediMed single-tab gel electrodes (25 \(\times\) 23 mm) were used to attach sense leads to the left or right dorsum wrist and ankle, and the source leads to the palm at the metacarpal heads and the sole at the metatarsal heads on the same side of the body18. No differences in impedance parameters were observed between measurement sides (all p > 0.05). Prior to careful application of the electrodes, the skin was cleaned with 70% isopropyl alcohol wipes and allowed to dry. Any clothing with metal (e.g., clips or buckles) was removed prior to measurement to avoid electrical interference. Otherwise, clothing was only removed to access electrode sites. For each body position, measurements were made in triplicate using the “continuous” setting of the device; each measurement taking less than a second. Cole plots were examined to ensure data quality and measurements were repeated if movement occurred.
Data was analysed using BioImp software version 5.4.0.3 (ImpediMed), using the default settings [frequency range 5–500 kHz, automatic time delay (Td) correction on, no data rejection limit]. The impedance values of interest were as follows: resistance at 0 kHz, R0; resistance at infinite kHz, R∞; impedance at 50 kHz, Z50; resistance at 50 kHz, R50; reactance at 50 kHz, Xc50; and impedance at the characteristic frequency, Zc.
Assessment of body composition
Standing height was measured in triplicate to the nearest 0.1 cm using a calibrated SECA 213 portable stadiometer (SECA, Hamburg, Germany), with median height being used in analyses, while a single weight measurement was obtained to the nearest 100 g using calibrated SECA 899 scales. Along with sex, these values were used to compute body composition measures using two methods: mixture theory in combination with Cole modelling [i.e., the SFB7’s default equations and constants: resistivity of ECW (ρECW) and ICW (ρICW)—females 235.5 and 894.2 Ω/cm, and males 273.9 and 937.2 Ω/cm, respectively; body density (Db) 1.05 g/L; body proportion factor (Kb) 4.30; and hydration factor (HF) 0.732]17,19,20, and an empirically-derived regression equation21.
The SFB7 provides the following body composition values: TBW, ECW, ICW, FFM, and FM. However, the coefficients used by the SFB7 may not be suitable for use in small children;22,23 therefore, measured resistance at 50 kHz was used in a previously published empirically derived regression equation for FFM (FFMRush), which was developed using DXA among a cohort of New Zealand 2-year-olds21. The reported equation is as follows:
FM (FMRush) was computed from FFM considering a two-compartment model of body composition24 and the following equation:
Statistical methods
Mean (SD) bioimpedance parameters (R∞, R0, Zc, R50, Z50, and Xc50) and body composition values (TBWSFB7, ECWSFB7, ICWSFB7, FFMSFB7, FMSFB7, FFMRush, and FMRush) were assessed in each of the body positions (supine, standing ≤ 1 min, and standing ≥ 4 min), with sex differences in impedance parameters being explored using independent samples t tests. Differences in impedance and body composition between supine and both standing positions were assessed using repeated measures ANOVA with Bonferroni post hoc testing, with differences in body composition values between supine and standing (≥ 4 min) positions being presented as percentage differences. The effect of fasting and bladder voiding on differences in impedance measurements was assessed using one-way ANOVA and independent samples t tests.
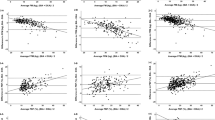
In order to develop equations to allow adjustment of bioimpedance parameters obtained while standing, thus allowing their use in equations where supine body position is indicated, the cohort was split into development (70%) and validation cohorts (30%) using a random number generator within SPSS version 26 (IBM Corp, Armonk, NY, USA). Among the development cohort (n = 35), for each impedance parameter, simple linear regression was used to develop an equation to adjust impedance values obtained while standing (≥ 4 min) to be comparable to those obtained while supine. These resulting equations were then applied to the validation cohort (n = 15). The equations were also applied to standing (≤ 1 min) measurements among the validation cohort to further elucidate the importance of time spent standing. Impedance parameters from supine measurements were compared to the adjusted standing measurements using paired samples t tests and Bland–Altman’s methods25. All tests were two-tailed and were performed within SPSS. P values ≤ 0.05 were considered statistically significant.
Results
Demographics
The sample comprised 50 children, 20 of whom were male and 30 female. On average, the children were 3.38 years old, with boys being somewhat taller and heavier than girls (Table 1).
Sex effects
Mean impedance parameters were larger among girls than boys in each of the body positions. These differences were significant, with the exception of standing (≥ 4 min) mean reactance at 50 kHz (p = 0.065). In contrast, the means of the differences in impedance parameters between supine and standing (≥ 4 min) positions were not significantly different between sexes, with the exception of reactance at 50 kHz (p < 0.001). Given the similarity in all other mean differences, further comparisons were made using the entire cohort.
Differences between standing and supine
Mean impedance parameters for supine and standing (< 1 min and ≥ 4 min) measurements are presented in Table 2. There were significant differences between body positions in all impedance parameters (p < 0.001). Post-hoc comparisons revealed that there were differences between impedance parameters obtained when supine compared to both standing positions (all p < 0.001), with supine values larger than those obtained when standing. Impedance parameters were generally higher when obtained standing immediately from supine (< 1 min) compared to standing (≥ 4 min), with the exception of reactance at 50 kHz where the reverse was true, but these differences were not statistically significant. There were also significant differences (p < 0.001) in all body composition parameters between supine and both standing positions (Table 3). However, these differences were probably of little clinical significance, with percentage differences of less than five percent, with the exception of FM, which exhibited both greater percentage differences and greater variability.
Effect of fasting and voiding
Among children who did not eat, drink, or void between measurements (n = 45), there was no clear pattern (i.e., increasing or decreasing across categories) in mean impedance values according to category of last meal (< 30 min ago, 30 min–1 h ago, 1–2 h ago, or > 2 h ago). Furthermore, differences in impedance between standing (≥ 4 min) and supine measurements (i.e., mean differences) did not vary significantly according to category of last meal (p values: R0 = 0.94, R∞ = 0.30, Zc = 0.64, Z50 = 0.80, R50 = 0.79, Xc50 = 0.59). However, most of the children consumed food within half an hour of measurement. Therefore, the groups 30 min to 1 h (n = 7), 1 to 2 h (n = 9), and over 2 h (n = 5) were collapsed, and differences were assessed using an independent samples t test. Although there was a trend for greater impedance and resistance, but reduced reactance among those who had not eaten within half an hour of measurement, there remained no significant differences in mean impedance parameters (all p > 0.10), or in mean differences in impedance parameters between supine and standing (≥ 4 min) positions (p values: R0 = 0.70, R∞ = 0.86, Zc = 0.74, Z50 = 0.58, R50 = 0.58, Xc50 = 0.83).
Mean impedance parameters were not statistically different between children who had not voided within half an hour of measurement compared to those who had. Likewise, there were no significant variations in the mean differences of impedance parameters according to whether or not the child had voided (p values: R0 = 0.55, R∞ = 0.16, Zc = 0.71, Z50 = 0.84, R50 = 0.86,). Although, there was a borderline significant difference in reactance at 50 kHz, with mean differences being higher among those who had not voided, compared to those who had (p = 0.062).
Adjustment equations
As there were statistically significant differences between supine and standing positions, equations were developed to allow impedance measurements obtained when standing to be adjusted to be comparable to those obtained while supine (Table 4). The development cohort (n = 35) was not different from the validation cohort (n = 15) in age, sex, height, weight, or BMI z score (all p > 0.05).
When the adjustment equations were applied to the validation cohort, there were no significant differences in mean impedance values between supine and adjusted standing measurements (all p > 0.05). Bland–Altman analysis revealed small biases and narrow limits of agreement. These are expressed as absolute values and as percentages of mean supine impedance values (Table 5). The equations were subsequently applied to standing (≤ 1 min) measurements, and there were no significant differences between the adjusted and supine values (all p > 0.05). Bias was larger but was still less than 1% of mean supine impedance; however, limits of agreement were marginally narrower (supplementary Table 1).
Discussion
Although adult guidelines dictate that BIA measurements be made supine after at least 4 min have elapsed9,10, it is not always feasible in infants and young children. In our study of 50 young children, impedance measurements differed between body positions, with higher derived TBW, ECW, ICW, and FFM, and lower FM in the standing body position; most of the body composition values differed by less than 5%, with the exception of FM (FMSFB7 13.75% lower and FMRush 9.12% lower).
A recent study evaluated the effect of body position on phase angle in a cohort of 1298 Mexican children and adolescents aged 4 to 20 years26. Phase angle was higher when measured supine than standing, with differences between body positions increasing with increased phase angle, age, and height. However, the children were measured with two different BIA devices, which had different electrode types (metal and adhesive), and thus are not directly comparable.
Another study examined differences in body fluid according to measurement position (standing and supine) in a cohort of 23 boys (6–14 years) and 26 men (23–82 years)27. Significant impedance differences were also observed (at 50 and 100 kHz in boys and at 100 kHz in men). No significant differences were seen in TBW, FFM, FM, or percentage of body fat (%BF), but body water shifted so that ECW increased and ICW decreased when standing. This is in contrast to our study, where differences were observed in all body composition values, and both ECW and ICW increased when standing. In adults, Gibson et al.6 found that ECW decreased and ICW increased while supine. When standing, although ECW increased incrementally, decreases in ICW were not significant. It has been suggested that it takes extended periods to achieve fluid stabilisation6,28, which may explain this observed discrepancy.
We were unable to explore time-course changes in impedance values; however, previous research has suggested that changes in impedance are greatest immediately on recumbence/ standing, and changes thereafter are gradual8,29. Furthermore, we observed no significant differences in impedance values when measured immediately on standing, compared to after at least four minutes had elapsed.
Regression equations were developed to allow adjustment of standing BIA measurements to be comparable to measurements obtained while supine, irrespective of the amount of time spent standing (Tables 5 and S1). Previously, regression equations have been developed among adults to allow measurements made while sitting upright in a wheelchair to be comparable to measurements made while supine30. Similarly, Rush et al.31 developed adjustment factors to convert standing measurement to equate supine in children and adults (categorised: 5–14 years, 15–30 years, 31–59 years, and 60 + years). Our equations may be of benefit in studies in young children that wish to use a previously published prediction equation where supine body position is dictated, but where this may not be achievable.
To our knowledge, this study is the first to explore the influence of body position on bioimpedance measurements in young children (< 5 years). At this age, children are often non-compliant, and it is not feasible to obtain BIA measurements after extended periods of lying. It may be of benefit to take measurements while the child is in an alternative body position, for example, while standing. A limitation of our study was that electrode placement meant that the leads were touching the ground. Although, only the external insulating plastic sheath was in contact, and the leads are actively shielded against electrical interference. Furthermore, the placement used was necessary to maintain adequate separation of the electrodes9,10. This methodology meant that use of two different BIA devices was avoided. Although some studies have evaluated the effect of body position using different BIA devices26,32, ample evidence suggests that BIA device types are not interchangeable33,34,35. Jensen et al.26 used two differing BIA devices in their study and concluded that electrode type explained approximately half of the observed differences in phase angle between body positions when they conducted additional analyses in a cohort of adults. However, this is likely related to the differing electrode positions, in addition to the electrode type (metal vs adhesive).
The effect of fasting has not previously been evaluated in preschool aged children; however, evidence from infancy suggests that impedance parameters do not change significantly when measured pre- and post-feed11,36. Although, Sesmero et al.11 did observe a general trend for increasing R0 with increasing time after feed, but this was only significant among their 1-week-old infants. The effect of bladder voiding has not been evaluated in any paediatric population. In adults, bladder voiding has been associated with a small measurement error of 1.0%14. In this study, time of last meal or bladder void were often estimated; however, there were no significant differences in impedance between body positions according to fasting or voiding. Nonetheless, half an hour may not be a sufficient difference in time to evaluate the effect of fasting and voiding. However, it would be not be feasible nor ethical to request young children to refrain from eating or voiding for extended periods to evaluate this further, though a larger study group may provide more clarity on this issue.
Other limitations of this research include that the equations used to estimate body composition might not be appropriate for this cohort, as evidenced by the wide standard deviations for FM. However, the aim of the study was not to accurately estimate body composition; rather, body composition values were used to ascertain if clinically significant differences were apparent between body positions. Nonetheless, we used two different methods for estimating body composition (Rush et al.21 and SFB7 equations), and the resulting percentage differences between body positions were comparable. In addition, we did not randomise the order of measurements as inclusion into this sub-study was based on compliance with the NiPPeR protocol. Studies in adults have suggested that position order is not important6,31,37. For example, among children and adults assessed both standing prior to lying supine and standing following a supine measurement, the second standing measurement was lower than the first by only approximately 1 ohm31. Furthermore, in our cohort, we did not standardise measurement side and we were not able to assess if there were any differences between body sides in individuals. We found no significant differences in mean impedance values between measurement sides, although there was a borderline significant difference between R∞ when supine, and R∞ and Zc when measured immediately on standing (p = 0.10, 0.06, and 0.09, respectively). Nonetheless, limb dominance may not be fully established until 4 to 6 years of age38. Furthermore, the consequence of placing BIA electrodes on the left or right side has not been evaluated3, although a study in adults found a small difference in impedance between body sides14, which is likely related to limb dominance.
This study provides the first evidence to describe the influence of body position on bioimpedance measurements in young children. This study suggests that researchers and clinicians can take bioimpedance measurements without requiring the child to meet various requirements for fasting, voiding, and lying supine for extended periods. Future research is required to confirm these findings and to further evaluate the effect of fasting and voiding on bioimpedance measurements in young children.
Data availability
The data will not be openly available as participants did not consent to open access data sharing. Additionally, this is an ongoing longitudinal study in which there will be further future analyses conducted.
References
Cornish, B. H., Thomas, B. J. & Ward, L. C. Improved prediction of extracellular and total body water using impedance loci generated by multiple frequency bioelectrical impedance analysis. Phys. Med. Biol. 38, 337–346. https://doi.org/10.1088/0031-9155/38/3/001 (1993).
De Lorenzo, A., Andreoli, A., Matthie, J. & Withers, P. Predicting body cell mass with bioimpedance by using theoretical methods: a technological review. J. Appl. Physiol. 82, 1542–1558. https://doi.org/10.1152/jappl.1997.82.5.1542 (1997).
Brantlov, S., Ward, L. C., Jodal, L., Rittig, S. & Lange, A. Critical factors and their impact on bioelectrical impedance analysis in children: a review. J. Med. Eng. Technol. 41, 22–35. https://doi.org/10.1080/03091902.2016.1209590 (2017).
Lyons-Reid, J., Ward, L. C., Kenealy, T. & Cutfield, W. Bioelectrical impedance analysis—an easy tool for quantifying body composition in infancy?. Nutrients 12, 920. https://doi.org/10.3390/nu12040920 (2020).
Brantlov, S., Jodal, L., Lange, A., Rittig, S. & Ward, L. C. Standardisation of bioelectrical impedance analysis for the estimation of body composition in healthy paediatric populations: a systematic review. J. Med. Eng. Technol. 41, 460–479. https://doi.org/10.1080/03091902.2017.1333165 (2017).
Gibson, A., Beam, J., Alencar, M., Zuhl, M. & Mermier, C. Time course of supine and standing shifts in total body, intracellular and extracellular water for a sample of healthy adults. Eur. J. Clin. Nutr. 69, 14–19. https://doi.org/10.1038/ejcn.2013.269 (2014).
Scharfetter, H. et al. Effect of postural changes on the reliability of volume estimations from bioimpedance spectroscopy data. Kidney Int. 51, 1078–1087. https://doi.org/10.1038/ki.1997.150 (1997).
Kushner, R. F., Gudivaka, R. & Schoeller, D. A. Clinical characteristics influencing bioelectrical impedance analysis measurements. Am. J. Clin. Nutr. 64, 423S-427S. https://doi.org/10.1093/ajcn/64.3.423S (1996).
Kyle, U. G. et al. Bioelectrical impedance analysis-part II: utilization in clinical practice. Clin. Nutr. 23, 1430–1453. https://doi.org/10.1016/j.clnu.2004.09.012 (2004).
National Institutes of Health. Bioelectrical impedance analysis in body composition measurement: National Institutes of Health Technology Assessment Conference Statement. Am. J. Clin. Nutr. 64, 524S-532S. https://doi.org/10.1093/ajcn/64.3.524S (1996).
Sesmero, M. A., Mazariegos, M., Pedrón, C., Jones, J. & Solomons, N. W. Bioimpedance electrical spectroscopy in the first six months of life: some methodologic considerations. Nutrition 21, 567–573. https://doi.org/10.1016/j.nut.2004.10.010 (2005).
Raghavan, C. V. et al. Estimation of total body water in very-low-birth-weight infants by using anthropometry with and without bioelectrical impedance and H2[(18)O]. Am. J. Clin. Nutr. 68, 668–674. https://doi.org/10.1093/ajcn/68.3.668 (1998).
Sidhu, J. S., Triggs, E. J., Charles, B. G. & Tudehope, D. I. Electrode placement in neonatal bioelectrical impedance analysis. Med. Biol. Eng. Comput. 32, 456–459. https://doi.org/10.1007/BF02524702 (1994).
Gonzalez, C., Evans, J. A., Smye, S. W. & Holland, P. Variables affecting BIA measurement of body water. Med. Biol. Eng. Comput. 37, 106–107 (1999).
Deurenberg, P., Weststrate, J. A., Paymans, I. & van der Kooy, K. Factors affecting bioelectrical impedance measurements in humans. Eur. J. Clin. Nutr. 42, 1017–1022 (1988).
Godfrey, K. M. et al. Nutritional intervention preconception and during pregnancy to maintain healthy glucose metabolism and offspring health (“NiPPeR”): study protocol for a randomised controlled trial. Trials 18, 131. https://doi.org/10.1186/s13063-017-1875-x (2017).
ImpediMed. SFB7, https://www.impedimed.com/products/sfb7/ (2020).
Lingwood, B. E., Coghlan, J. P., Ward, L. C., Charles, B. G. & Colditz, P. B. Measurement of extracellular fluid volume in the neonate using multiple frequency bio-impedance analysis. Physiol. Meas. 21, 251–262 (2000).
Cole, K. S. Permeability and impermeability of cell membranes for ions. Cold Spring Harb. Symp. Quant. Biol. 8, 110–122. https://doi.org/10.1101/SQB.1940.008.01.013 (1940).
Matthie, J. R. Bioimpedance measurements of human body composition: critical analysis and outlook. Expert Rev. Med. Dev. 5, 239–261. https://doi.org/10.1586/17434440.5.2.239 (2008).
Rush, E. C., Bristow, S., Plank, L. D. & Rowan, J. Bioimpedance prediction of fat-free mass from dual-energy X-ray absorptiometry in a multi-ethnic group of 2-year-old children. Eur. J. Clin. Nutr. 67, 214–217. https://doi.org/10.1038/ejcn.2012.182 (2013).
Collins, C. T. et al. Prediction of body water compartments in preterm infants by bioelectrical impedance spectroscopy. Eur. J. Clin. Nutr. 67, S47-53. https://doi.org/10.1038/ejcn.2012.164 (2013).
Ellis, K. J., Shypailo, R. J. & Wong, W. W. Measurement of body water by multifrequency bioelectrical impedance spectroscopy in a multiethnic pediatric population. Am. J. Clin. Nutr. 70, 847–853. https://doi.org/10.1093/ajcn/70.5.847%JTheAmericanJournalofClinicalNutrition (1999).
Heymsfield, S. B., Wang, Z., Baumgartner, R. N. & Ross, R. Human body composition: advances in models and methods. Annu. Rev. Nutr. 17, 527–558. https://doi.org/10.1146/annurev.nutr.17.1.527 (1997).
Bland, J. M. & Altman, D. G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307–310 (1986).
Jensen, B. et al. Configuration of bioelectrical impedance measurements affects results for phase angle. Med. Eng. Phys. 84, 10–15. https://doi.org/10.1016/j.medengphy.2020.07.021 (2020).
Kagawa, M., Wishart, C. & Hills, A. P. Influence of posture and frequency modes in total body water estimation using bioelectrical impedance spectroscopy in boys and adult males. Nutrients 6, 1886–1898. https://doi.org/10.3390/nu6051886 (2014).
Segal, K. R., Van Loan, M., Fitzgerald, P. I., Hodgdon, J. A. & Van Itallie, T. B. Lean body mass estimation by bioelectrical impedance analysis: a four-site cross-validation study. Am. J. Clin. Nutr. 47, 7–14. https://doi.org/10.1093/ajcn/47.1.7 (1988).
Slinde, F., Bark, A., Jansson, J. & Rossander-HulthÉN, L. Bioelectrical impedance variation in healthy subjects during 12 h in the supine position. Clin. Nutr. 22, 153–157. https://doi.org/10.1054/clnu.2002.0616 (2003).
Allison, G. T., Singer, K. P. & Marshall, R. N. The effect of body position on bioelectrical resistance in individuals with spinal cord injury. Disabil. Rehabil. 17, 424–429. https://doi.org/10.3109/09638289509166656 (1995).
Rush, E. C., Crowley, J., Freitas, I. F. & Luke, A. Validity of hand-to-foot measurement of bioimpedance: standing compared with lying position. Obesity (Silver Spring) 14, 252–257. https://doi.org/10.1038/oby.2006.32 (2006).
Esco, M. R. et al. Agreement between supine and standing bioimpedance spectroscopy devices and dual-energy X-ray absorptiometry for body composition determination. Clin. Physiol. Funct. Imag. 39, 355–361. https://doi.org/10.1111/cpf.12585 (2019).
Silva, A. M. et al. Lack of agreement of in vivo raw bioimpedance measurements obtained from two single and multi-frequency bioelectrical impedance devices. Eur. J. Clin. Nutr. 73, 1077–1083. https://doi.org/10.1038/s41430-018-0355-z (2019).
Tinsley, G. M., Moore, M. L., Silva, A. M. & Sardinha, L. B. Cross-sectional and longitudinal agreement between two multifrequency bioimpedance devices for resistance, reactance, and phase angle values. Eur. J. Clin. Nutr. https://doi.org/10.1038/s41430-019-0496-8 (2019).
Ward, L. C. Inter-instrument comparison of bioimpedance spectroscopic analysers. Open Med. Dev. J. 1, 3–10. https://doi.org/10.2174/1875181400901010003 (2009).
Gridneva, Z. et al. Bioimpedance spectroscopy in the infant: effect of milk intake and extracellular fluid reservoirs on resistance measurements in term breastfed infants. Eur. J. Clin. Nutr. 70, 843–851. https://doi.org/10.1038/ejcn.2016.26 (2016).
Demura, S., Yamaji, S., Goshi, F. & Nagasawa, Y. The influence of posture change on measurements of relative body fat in the bioimpedance analysis method. J. Physiol. Anthropol. Appl. Hum. Sci. 20, 29. https://doi.org/10.2114/jpa.20.29 (2001).
Scharoun, S. & Bryden, P. Hand preference, performance abilities, and hand selection in children. Front. Psychol. 5, https://doi.org/10.3389/fpsyg.2014.00082 (2014).
Acknowledgements
J.L-R. is currently receiving University of Auckland Doctoral Scholarship. The authors would like to acknowledge Auckland NiPPeR research staff Christine Creagh, Marysia Depczynski, and Sarah Wilkins for their contribution to this study. Public good funding for the investigator-led NiPPeR study is through the UK Medical Research Council (as part of an MRC award to the MRC Lifecourse Epidemiology Unit (MC_UU_12011/4)); the Singapore National Research Foundation, National Medical Research Council (NMRC, NMRC/TCR/012-NUHS/2014); the National University of Singapore (NUS) and the Agency of Science, Technology and Research (as part of the Growth, Development and Metabolism Programme of the Singapore Institute for Clinical Sciences (SICS) (H17/01/a0/005); and as part of Gravida, a New Zealand Government Centre of Research Excellence. Funding for aspects of the NiPPeR study has been provided by Société Des Produits Nestlé S.A under a Research Agreement with the University of Southampton, Auckland UniServices Ltd, SICS, National University Hospital Singapore PTE Ltd and NUS. K.M.G. is supported by the National Institute for Health Research (NIHR Senior Investigator (NF-SI-0515-10042), NIHR Southampton 1000DaysPlus Global Nutrition Research Group (17/63/154) and NIHR Southampton Biomedical Research Center (IS-BRC-1215-20004)), British Heart Foundation (RG/15/17/3174) and the European Union (Erasmus+ Programme ImpENSA 598488-EPP-1-2018-1-DE-EPPKA2-CBHE-JP). S.Y.C. is supported by a Singapore NMRC Clinician Scientist Award (NMRC/CSA-INV/0010/2016). The funders had no role in the data collection and analysis, and the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
W.S.C. and T.K. supervised all aspects of the research study. K.M.G., S-Y.C., and W.S.C. led the NiPPeR trial conception and design. J.L-R., W.S.C., and T.K. conceived and designed the body position sub-study. J.L-R. compiled the data and carried out the statistical analyses. J.L-R. wrote the manuscript with critical input from all other authors. All authors have approved the final version of this manuscript and have agreed to be accountable for all aspects of this work.
Corresponding author
Ethics declarations
Competing interests
L.C.W. provides consultancy services to ImpediMed Ltd (a manufacturer of devices for bioelectrical impedance analysis). ImpediMed Ltd was not involved in the inception and conduct of this research, or in the writing of this manuscript. K.M.G. has received reimbursement for speaking at conferences sponsored by companies selling nutritional products, and is part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, BenevolentAI Bio Ltd. and Danone. The other authors have no financial or non-financial conflicts of interest to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lyons-Reid, J., Ward, L.C., Tint, MT. et al. The influence of body position on bioelectrical impedance spectroscopy measurements in young children. Sci Rep 11, 10346 (2021). https://doi.org/10.1038/s41598-021-89568-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89568-8
This article is cited by
-
Prediction of fat-free mass in young children using bioelectrical impedance spectroscopy
European Journal of Clinical Nutrition (2023)
-
Associations of overnight changes in body composition with positional obstructive sleep apnea
Sleep and Breathing (2023)
-
Using bioelectrical impedance analysis in children and adolescents: Pressing issues
European Journal of Clinical Nutrition (2022)
-
Fluid balance assessment in pediatric hemodialysis patients by using whole-body bioimpedance spectroscopy (WB-BIS)
Pediatric Nephrology (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
