
Abstract
Studies have suggested that handgrip strength might be a marker for cardiometabolic risk (CMR), but it has not been studied in Hispanic/Latino farmworker population. This study aimed to characterize absolute and relative handgrip strength in Hispanic/Latino farmworkers, and investigate the sex-specific association between handgrip strength and CMR factors. CMR factors and seated isometric absolute (the sum of both hands) and relative (absolute handgrip strength divided by body mass index) handgrip strengths were collected in 173 Hispanic/Latino farmworkers (mean age 35.1 ± 0.7 years; 49% female). The absolute and the relative handgrip strengths were 89.2 ± 1.8 kg, 3.3 ± 0.1 kg among males, and 56.5 ± 1.9 kg, 1.9 ± 0.1 kg among females, respectively. Age was correlated with absolute (r = − 0.17, p = 0.03) and relative handgrip strengths (r = − 0.28, p < 0.01). In males, absolute handgrip was related to triglycerides (r = − 0.25, p < 0.05), whereas relative handgrip was related to waist circumference (r = − 0.32, p < 0.01), waist/hip circumference ratio (r = − 0.36, p < 0.01), high-density lipoprotein (r = 0.24, p < 0.05), and triglycerides (r = − 0.35, p < 0.01). In females, absolute handgrip was related to fasting plasma glucose (r = − 0.28, p = 0.03), whereas relative handgrip was related to waist circumference (r = − 0.38, p < 0.01) and fasting plasma glucose (r = − 0.22, p < 0.05). Males had lower absolute handgrip strength when their triglycerides levels were at risk (p = 0.021), and lower relative handgrip strength when their plasma glucose (p = 0.034) and triglycerides (p = 0.002) levels were at risk. Females had lower relative handgrip strength when their plasma glucose (p = 0.001) and blood pressure (p = 0.004) were at risk. This study suggests that handgrip strength may be associated with sex-specific CMR factors in a Hispanic/Latino farmworker population.
Similar content being viewed by others

Introduction
Every year, approximately 4 million migrant farmworkers generate and support a $30 billion agriculture industry and associated economic vitality in the United States. Eighty percent of them are Hispanic/Latinos1. Despite the important role they play in the United States (US) economy, Hispanic/Latino migrant farmworkers represent one of the most socially vulnerable and disadvantaged workforces due to unstable working and living conditions and barriers to obtaining health services2,3,4. As a result of occupational hazards, and barriers to preventive healthcare services, there are increasing concerns of developing chronic diseases, such as cardiovascular disease (CVD) and its complications in this population. CVD, one of the leading causes of morbidity and mortality in the US5 and worldwide6, has especially high rates in racially and ethnically diverse populations, including Hispanic/Latinos7. Recent data also showed a high prevalence of cardiometabolic risks (CMR) among Hispanic/Latino populations, including diabetes, hypercholesterolemia, hypertension, and obesity8. Despite this increasing occurrence of CMR in the Hispanic/Latino population, very little evidence is available in the Hispanic/Latino migrant farmworkers. Previous studies showed 21.5% hypertension and 16.1% diabetes among farmworkers using self-report data9,10. Our group reported in a previous study that the prevalence of overweight/obesity, prehypertension/hypertension, and prediabetes/diabetes among Hispanic/Latino migrant farmworkers were 78.5%, 57.7%, and 36.7%, respectively11.
A number of epidemiological studies support the association between handgrip strength and cardiovascular health12,13,14. Handgrip strength, a surrogate marker for whole-body strength, is widely used to assess sarcopenia15. Handgrip is an emerging marker for CVD16,17,18 and diabetes19,20. Previous research has also indicated that early-onset obesity was related to decreased grip strength21. However, there are a few gaps in the literature. One study used race, including Hispanic, as a covariate, but did not focus on differences among the races in the relationship between handgrip and cardiovascular health biomarkers16. Mainous et al. showed that lower grip strength in both men and women is related to undiagnosed diabetes and hypertension in normal-weight individuals but not the general adult population22. In another study by the same research team, prediabetes was related to lower grip strength in men and women in whites but not Hispanics23. There is a study of handgrip strength in association with activities of daily living disability that was carried out among older Mexican Americans24. In addition to the absolute handgrip strength, relative handgrip strength consisting of the combination of handgrip strength and body mass index (BMI) was shown to diminish the confounding by body mass and accompanied health risks of elevated body weight16. There is a lack of research on the values of absolute and relative handgrip strength, and its relation to CMR in the younger Hispanic adult population in general, and particularly, Hispanic/Latino migrant farmworkers. The American Diabetes Association suggested that CMR factors include overweight/obese, high LDL cholesterol, low HDL cholesterol, high total cholesterol, high triglycerides, physical inactivity, high BP, high blood glucose, and smoking25. Thus, the aim of this study was first to characterize the values of absolute and relative handgrip strength in this population, followed by investigating the sex-specific association between handgrip strength and CMR factors of Hispanic/Latino farmworkers. We hypothesized that lower handgrip strength would be correlated with greater CMR factors.
Methods
Participants
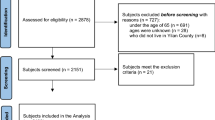
This community outreach project was performed by the university and community partnership between Augusta University and CL Farm from 2013 to 2015. All Hispanic/Latino employees at the plant nursery in Trenton, South Carolina were invited to participate in this health-screening study. The consent form was translated into Spanish. Study information and consent processes were conducted during the farm business hours with the help of medically certified Spanish interpreters. Written informed consent was obtained from 173 participants. The protocol was approved by the Institutional Review Board at Augusta University. All measurements were performed on the morning of the health fair at the plant nursery at CL Farm. All methods were carried out in accordance with relevant guidelines and regulations.
Handgrip strength measurement
Isometric handgrip strength was measured using a Jamar Hydraulic Hand Dynamometer (Jamar; Bolingbrook, IL). Grip strength was measured in both hands in a seated position with the arm at a 90-degree angle according to the National Health and Nutrition Examination Survey (NHANES) guidelines for hand dynamometry16. Handgrip strength was measured three times, and the highest score was used for each hand. The combined strength (in kilograms) of the right and left hands were used to create the absolute handgrip value. The relative handgrip was then calculated as the absolute handgrip divided by their BMI (kg/BMI)6,12. Handgrip strength asymmetry ratio is calculated as non-dominant/dominant handgrip strength. Those with handgrip strength ratio < 0.90 or > 1.10 have handgrip strength asymmetry.
Anthropometry measurements
Height and weight were obtained according to standard procedures, using a wall-mounted stadiometer (Tanita Corporation of American, Arlington Heights, IL) and calibrated electronic scale (model CN2OL; Cardinal Detecto, Webb City, MO). BMI as weight (kg)/height (m2) was calculated using the CDC formula. Waist and hip circumferences (inches) were measured with minimal clothing at the level of umbilicus, and around the widest portion of the buttocks, respectively. The waist/hip circumference (W/Hip) ratio was calculated as the waist circumference divided by the hip circumference. After 5 min of rest, systolic (SBP) and diastolic blood pressures (DBP) were measured twice, each at least 1 min apart, in sitting position using manual mercury sphygmomanometer. The averages of two measurements were reported and used for analyses.
Laboratory measurements
As previously described26, venous blood was collected after an overnight fast, and all blood samples were centrifuged immediately and stored at − 80 °C for analysis. Fasting plasma glucose (FPG) and lipid profile (total cholesterol, low-density lipoprotein cholesterol [LDL-cholesterol], high-density lipoprotein cholesterol [HDL-cholesterol], and triglycerides) were assessed by standard clinical laboratory methods at Premier Medical Laboratory Services (Greenville, SC). Fasting glucose was measured using hexokinase and glucose-6-phosphate dehydrogenase enzymatic method. Lipid parameters were measured by an enzymatic colorimetric method, using an automated analyzer (Cobas c 311/501 and Cobas c 502) and Cobas enzymatic reagents.
Outcome variables
The outcome variables included BMI, LDL cholesterol, HDL cholesterol, cholesterol, triglycerides, BP, and blood glucose. In addition, these continuous variables were further classified to at risk or not using definitions from the American Diabetes Association (Table 1)25.
Statistical analysis
Normal distribution and homogeneity of variances were confirmed by Shapiro-Wilks W and Leven’s tests, respectively27,28. Partial Pearson’s correlation coefficients were used to examine the associations between absolute and relative handgrip as the independent variables and CMR factors as the dependent variables, with control for age. Similar statistical analyses were carried out in males and in females separately to investigate the sex-specific associations between handgrip strength and CMR factors. Absolute and relative handgrip strength measures were compared between each CMR factor at risk and not at risk using t-test. The cumulative associations of the composite CMR factors with absolute and relative handgrip measures were calculated using stepwise regression models, and backward-selection estimation was performed to select CMR factors correlated with handgrip strength with the backward selection at the significance level of 0.2 for removal from the model. Statistical analyses were carried out using SPSS software (version 23, IBM SPSS Statistics, Chicago, IL). A P-value < 0.05 was considered statistically significant.
Results
General characteristics of the participants
The population was composed of 173 Hispanic/Latino farmworkers (49% female) and the mean (± SEM) age was 35.1 ± 0.7 years. The clinical characteristics of the participants are presented in Table 2.
Variations in handgrip strength by participant characteristics
In the total sample, the means of absolute and relative handgrip strength were 73.1 ± 1.6 kg, 2.6 ± 0.1 kg/BMI, respectively. On average, absolute and relative handgrip strengths were 32.7 kg and 1.4 kg/BMI higher respectively in males than in females (p < 0.01, Table 2). Age was inversely correlated with absolute (r = − 0.17, p = 0.03) and relative handgrip strengths (r = − 0.28, p < 0.01). The differences in handgrip strength asymmetry and ratio between the male and the female were not statistically significant (p > 0.05).
Associations between absolute handgrip strength and cardiometabolic risk factors
Supplementary Table S1 shows the partial correlations (adjusting for age) between absolute handgrip strength and CMR factors. A significant but weak inverse association was observed between absolute handgrip strength and triglycerides among males (r = − 0.25, p = 0.03). Likewise, there was a significant but weak inverse association between absolute handgrip strength and FPG among females (r = − 0.27, p = 0.01). Handgrip strength ratio was not correlated with any of the CMR factors in males or in females (p > 0.05).
Associations between relative handgrip strength and cardiometabolic risk factors
Supplementary Table S2 reports the partial correlations (adjusting for age) between relative handgrip strength and CMR factors. In males, lower relative handgrip strength was significantly but weakly correlated with higher waist circumference (r = − 0.32, p < 0.01), W/Hip ratio (r = − 0.34, p < 0.01), and triglycerides (r = − 0.35, p < 0.01), while higher relative handgrip strength was significantly but weakly associated with higher HDL-cholesterol (r = 0.24, p = 0.04). In females, lower relative handgrip strength was significantly but weakly correlated with higher waist circumference (r = − 0.38, p < 0.01), and FPG (r = − 0.22, p < 0.01) (Supplementary Table S2). There were inverse trends of the correlations of relative handgrip with SBP and DBP among males and females, and an inverse trend for the correlation between relative handgrip and low-density lipoprotein among males only; however, none reached statistical significance.
Comparisons of handgrip strength between cardiometabolic risk factor categories
Table 3 showed that males had lower absolute handgrip strength when their triglycerides levels were at risk (p = 0.021), and lower relative handgrip strength when their FPG (p = 0.034) and triglycerides (p = 0.002) levels were at risk. Females had lower relative handgrip strength when their FPG (p = 0.001) and BP (p = 0.004) were at risk.
Cumulative association of cardiometabolic risk factors with handgrip strength
The absolute handgrip strengths were explained by cumulative variations of age, BMI, and triglycerides (adjusted R-squared = 0.09) in males, and by FPG and SBP (adjusted R-squared = 0.11) in females (Table 4). The relative handgrip strengths were explained by cumulative variations of FPG, LDL-cholesterol, total cholesterol, and triglycerides (adjusted R-squared = 0.17) in males, and by age, FPG, DBP, LDL-cholesterol, total cholesterol, and triglycerides (adjusted R-squared = 0.13) in females (Table 4).
Discussion
To our knowledge, this is the first study to characterize the values of absolute and relative handgrip strengths and to investigate their associations with CMR factors in a Hispanic/Latino migrant farmworker population. To date, mean values of absolute and relative handgrip strengths have not been studied in the Hispanic adult population in general, and especially Hispanic/Latino migrant farmworkers. Data from 2011–2012 NHANES showed that the means of absolute and relative handgrip strengths in the U.S. adult population were similar to our Hispanic farmworkers in both sexes16. In males, the combined absolute handgrip strengths reported in the NHANES population in comparison with our study participants were 89.7 ± 0.8 kg and 89.2 ± 1.8 kg, respectively. The relative handgrip strength in the NHANES and our population were 3.2 ± 0.1 kg/BMI and 3.3 ± 0.1 kg/BMI, respectively. In females, the combined absolute handgrip strength in NHANES and our population were 56.1 ± 0.5 kg and 56.5 ± 1.9 kg, respectively. The means of relative handgrip strength in NHANES and our population were 2.0 ± 0.02 kg/BMI and 1.9 ± 0.1 kg/BMI, respectively. Multiple studies have shown that handgrip strength was relatively stable from 20–59 years, but decreased from 60 to 79 years29,30. The average ages of our population (35.1 ± 0.7 years) and NHANES population (47.5 ± 0.8 years) were both below age 50, which might explain the similar finding of absolute and relative handgrip strength in both populations.
This study found that in Hispanic/Latino farmworkers, lower handgrip strength is correlated with greater CMR factors in a sex-specific manner. In both males and females, relative handgrip strength was coupled with obesity and abdominal obesity markers, which is consistent with previous research31 indicating that obesity is associated with decreased muscle activity and strength. Higher relative handgrip strength was associated with lower waist circumference and W/Hip ratio in males, and lower waist circumference in females. A large population study found that grip strength was inversely associated with all-cause mortality, myocardial infarction, and stroke, and was a stronger predictor of all-cause and cardiovascular mortality than SBP32.
It has been postulated that the underlying mechanisms which could explain the relationship between obesity and reduced handgrip strength are inflammation and insulin resistance33,34,35. First, in the state of obesity, the inflammatory responses are activated through the production of proinflammatory cytokines and adipokines from adipose tissue36,37. Chronic inflammation and increased oxidative stress could contribute to the decline of muscle mass and strength38,39. Second, obesity is linked to insulin resistance, and the most crucial factor in modifying insulin sensitivity is the release of non-esterified fatty acids which diminish insulin receptor signaling40. Also, decreased insulin secretion due to the defect of the β-cell in the pancreas could explain the association between obesity and insulin resistance35. Barzilay et al. observed that insulin resistance could be related to the reduction in muscle strength of quadriceps muscle in elderly41. A possible physiological mechanism underlying diabetes and handgrip strength may be that the decreased muscle mass can lead to less efficient glucose uptake, which stimulates insulin resistance that can progress to diabetes23. Abbatecola et al. did not only find that insulin resistance was not linked to lower handgrip strength, but also observed that this relationship was significant in women while it was not significant in men, which is consistent with our finding42. However, other previous research indicated that handgrip strength was associated with dysglycemia43, prediabetes23, and type 2 diabetes in males19. It has been postulated that the difference in muscle strength between males and females from early adulthood may elucidate the difference in the association between handgrip strength and FPG44.
The lipid profile was also associated with handgrip strength for males. The inverse correlation between relative handgrip strength and HDL-cholesterol and triglycerides is comparable to the results of previous research that CVD risk was associated with lower handgrip in both male and female participants16. Other research supports that greater muscle strength affects the levels of lipoproteins45,46. However, we did not find the same relationship in females in our population. It may be plausible that the variation in the association between handgrip strength and CMR factors among both male and female participants may be due to differences in sex hormones47,48. A study by Michael and colleagues found that hormone therapy in postmenopausal women did not enhance their handgrip strength49, while a study by Page and colleagues showed that the administration of exogenous testosterone to older men enhanced their handgrip strength50. Future studies with larger sample sizes are warranted to unravel the underlying mechanism for these sex differences.
Limitations of the study should be acknowledged. This study is observational, which does not provide a causal explanation for the findings. Also, the current study has a relatively small sample size and only one single measure of muscle strength. Third, our participants were relatively young, and most of them were in their young adulthood. Therefore, our results of the relationship between handgrip strength and CMR factors cannot be generalized to other age groups. Similarly, only Hispanic/Latino farmworkers were included in this analysis, thus the appliance of our results to other race groups needs caution. Lastly, some relevant confounders were not collected in this study, such as dietary intake, physical activity, socioeconomic status, and family history.
Conclusions
In conclusion, this is the first study to report the values of absolute and the relative handgrip strengths, and their associations with sex-specific CMR factors among the Hispanic/Latino farmworkers. Handgrip strength is not only a marker of whole-body strength but also appears to be an indicator of CMR. As such, routine testing of handgrip strength should be considered when assessing the CMR of Hispanics in the clinical setting. Further research is required for studying potential underlying mechanisms.
References
Hernandez, T., Gabbard, S. & Carroll, D. Findings from the National Agricultural Workers Survey (NAWS) 2013–2014: A demographic and employment profile of United States farmworkers (US Department of Labor, 2016).
Chaney, B. H. & Torres, E. Covariates of identified stress and depression among seasonal farmworkers. Int. J. Environ. Res. Publ. Health. 14(7), 711 (2017).
Ramos, A. K., Su, D., Lander, L. & Rivera, R. Stress factors contributing to depression among latino migrant farmworkers in Nebraska. J. Immigr. Minor. Health 17(6), 1627–1634 (2015).
Bail, K. M. et al. The impact of invisibility on the health of migrant farmworkers in the southeastern United States: a case study from georgia. Nutr. Res. Pract. 2012, 760418 (2012).
Benjamin, E. J. et al. Heart disease and stroke statistics-2018 update: a report from the American heart association. Circulation 137(12), e67–e492 (2018).
Nowbar, A. N., Howard, J. P., Finegold, J. A., Asaria, P. & Francis, D. P. 2014 global geographic analysis of mortality from ischaemic heart disease by country, age and income: statistics from World Health Organisation and United Nations. Int. J. Cardiol. 174(2), 293–298 (2014).
González, H. M. et al. Cardiovascular health among diverse Hispanics/Latinos: Hispanic Community Health Study/Study of Latinos (HCHS/SOL) results. Am. Heart J. 176, 134–144 (2016).
Mattei, J. & Sotres-Alvarez, D. Diet Quality and Its Association with Cardiometabolic Risk Factors Vary by Hispanic and Latino Ethnic Background in the Hispanic Community Health Study/Study of Latinos. J. Nutr. 146(10), 2035–2044 (2016).
Rosales, C. et al. The US/Mexico border: a binational approach to framing challenges and constructing solutions for improving farmworkers’ lives. Int. J. Environ. Res. Publ. Health. 9(6), 2159–2174 (2012).
Castañeda, S. F., Rosenbaum, R. P., Holscher, J. T., Madanat, H. & Talavera, G. A. Cardiovascular disease risk factors among Latino migrant and seasonal farmworkers. J. Agromed. 20(2), 95–104 (2015).
Raed A, Bhagatwala J, Cromer PR, et al. Obesity and related cardiometabolic risk in young US Hispanic farmworkers: a neglected public health problem. Jacobs J. Commun. Med. 2017;3(1).
Laukkanen, J. A. et al. Handgrip strength is inversely associated with sudden cardiac death. Mayo Clin. Proc. 95(4), 825–828 (2020).
Ramírez-Vélez, R. et al. Association between ideal cardiovascular health score and relative handgrip strength of community-dwelling older adults in Colombia. J. Am. Med. Dir. Assoc. 21(3), 434-436.e432 (2020).
Jang, S. K., Kim, J. H. & Lee, Y. Effect of relative handgrip strength on cardiovascular disease among Korean adults aged 45 years and older: results from the Korean Longitudinal Study of Aging (2006–2016). Arch. Gerontol. Geriatr. 86, 103937 (2020).
Lee, W. J., Peng, L. N., Chiou, S. T. & Chen, L. K. Relative handgrip strength is a simple indicator of cardiometabolic risk among middle-aged and older people: a nationwide population-based study in Taiwan. PLoS ONE 11(8), e0160876 (2016).
Lawman, H. G. et al. Associations of relative handgrip strength and cardiovascular disease biomarkers in U.S. Adults, 2011–2012. Am. J. Prev. Med. 50(6), 677–683 (2016).
Kishimoto, H. et al. Midlife and late-life handgrip strength and risk of cause-specific death in a general Japanese population: the Hisayama Study. J. Epidemiol. Community Health 68(7), 663–668 (2014).
An KO, Kim J. Associations between handgrip strength with adverse cardiometabolic health among representative Korean adults. 2019;17(1).
Li, J. J. et al. Muscle grip strength predicts incident type 2 diabetes: population-based cohort study. Metabolism Clin. Exp. 65(6), 883–892 (2016).
Peterson, M. D. et al. Low normalized grip strength is a biomarker for cardiometabolic disease and physical disabilities among US and Chinese adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 72(11), 1525–1531 (2017).
Stenholm, S. et al. Association between obesity history and hand grip strength in older adults–exploring the roles of inflammation and insulin resistance as mediating factors. J. Gerontol. A Biol. Sci. Med. Sci. 66(3), 341–348 (2011).
Mainous, A. G. 3rd., Tanner, R. J., Anton, S. D. & Jo, A. Grip strength as a marker of hypertension and diabetes in healthy weight adults. Am. J. Prev. Med. 49(6), 850–858 (2015).
Mainous, A. G. 3rd., Tanner, R. J., Anton, S. D. & Jo, A. Low grip strength and prediabetes in normal-weight adults. J. Am. Board Fam. Med. 29(2), 280–282 (2016).
McGrath, R. P. et al. The association between handgrip strength and diabetes on activities of daily living disability in older Mexican Americans. J. Aging Health 30(8), 1305–1318 (2018).
Armani, A. M. Check up America: reduce cardiometabolic risk: clinical tools of the american diabetes association. Crit. Pathw. Cardiol. 6(2), 60–63 (2007).
Dong Y. Alanine aminotrans-ferase levels are associated with cardiometabolic risk markers in hispanic. Latino Farmwork-ers. 2018:20–25.
Shapiro, S. S. & Wilk, M. B. An analysis of variance test for normality (complete samples). Biometrika 52(3/4), 591–611 (1965).
Levene H. Robust tests for equality of variances. Contributions to probability and statistics Essays in honor of Harold Hotelling. 1961:279–292.
Mathiowetz, V. et al. Grip and pinch strength: normative data for adults. Arch. Phys. Med. Rehabil. 66(2), 69–74 (1985).
Luna-Heredia, E., Martin-Pena, G. & Ruiz-Galiana, J. Handgrip dynamometry in healthy adults. Clin. Nutr. 24(2), 250–258 (2005).
Tomlinson, D. J., Erskine, R. M., Morse, C. I., Winwood, K. & Onambele-Pearson, G. The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology 17(3), 467–483 (2016).
Leong, D. P. et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet (London, England). 386(9990), 266–273 (2015).
Roubenoff, R. Sarcopenic obesity: the confluence of two epidemics. Obes. Res. 12(6), 887–888 (2004).
Fontana, L., Eagon, J. C., Trujillo, M. E., Scherer, P. E. & Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 56(4), 1010–1013 (2007).
Kahn, S. E., Hull, R. L. & Utzschneider, K. M. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 444(7121), 840–846 (2006).
Keevil, V. L. et al. Cross-sectional associations between different measures of obesity and muscle strength in men and women in a British cohort study. J. Nutr. Health Aging. 19(1), 3–11 (2015).
Choi, K. M. The Impact of Organokines on Insulin Resistance, Inflammation, and Atherosclerosis. Endocrinol. Metab (Seoul). 31(1), 1–6 (2016).
Meng, S. J. & Yu, L. J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci. 11(4), 1509–1526 (2010).
Visser, M. et al. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: the Health ABC Study. J. Gerontol. A Biol. Sci. Med. Sci. 57(5), M326-332 (2002).
Shulman, G. I. Cellular mechanisms of insulin resistance. J. Clin. Investig. 106(2), 171–176 (2000).
Barzilay, J. I. et al. Insulin resistance is associated with decreased quadriceps muscle strength in nondiabetic adults aged >or=70 years. Diabetes Care 32(4), 736–738 (2009).
Abbatecola, A. M. et al. Insulin resistance and muscle strength in older persons. J. Gerontol. A Biol. Sci. Med. Sci. 60(10), 1278–1282 (2005).
Kalyani, R. R. et al. Sex differences in the association of fasting and postchallenge glucose levels with grip strength among older adults: the Rancho Bernardo Study. BMJ Open Diabetes Res Care. 3(1), e000086 (2015).
Aoyama, T. et al. Association between muscular strength and metabolic risk in Japanese women, but not in men. J. Physiol. Anthropol. 30(4), 133–139 (2011).
Tambalis, K., Panagiotakos, D. B., Kavouras, S. A. & Sidossis, L. S. Responses of blood lipids to aerobic, resistance, and combined aerobic with resistance exercise training: a systematic review of current evidence. Angiology 60(5), 614–632 (2009).
Williams, M. A. et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 116(5), 572–584 (2007).
Cheung, C. L., Nguyen, U. S., Au, E., Tan, K. C. & Kung, A. W. Association of handgrip strength with chronic diseases and multimorbidity: a cross-sectional study. Age 35(3), 929–941 (2013).
Amaral Cde, A. et al. Association of handgrip strength with self-reported diseases in adults in Rio Branco, Acre State, Brazil: a population-based study. Cad Saude Publica. 31(6), 1313–1325 (2015).
Michael, Y. L. et al. Hormone therapy and physical function change among older women in the Women’s Health Initiative: a randomized controlled trial. Menopause 17(2), 295–302 (2010).
Page, S. T. et al. Exogenous testosterone (T) alone or with finasteride increases physical performance, grip strength, and lean body mass in older men with low serum T. J. Clin. Endocrinol. Metab. 90(3), 1502–1510 (2005).
Funding
This study was supported in part by Community Partnership Study Award to DL and YD from Institute of Preventative and Public Health at Augusta University.
Author information
Authors and Affiliations
Contributions
A.R. and J.B. developed the study theory, performed the formal analysis, and drafted the manuscript. M.C., P.C., H.Z., A.M., D.L., S.P., J.B., YT.D., Z.S., and Y.D. carried out the investigation and collected data. L.Y., L.C., H.Z., A.M., and Y.D. revised the manuscript. H.Z. and Y.D. acquired the funding.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Raed, A., Bilz, J., Cortez-Cooper, M. et al. Handgrip and sex-specific cardiometabolic risk factors in Hispanic/Latino migrant farmworkers. Sci Rep 11, 10272 (2021). https://doi.org/10.1038/s41598-021-89138-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-89138-y
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
