
Abstract
This study aimed to investigate the accuracy of cup placement and determine the predictive risk factors for inaccurate cup positioning in robot-assisted total hip arthroplasty (THA). We retrospectively analyzed 115 patients who underwent robot-assisted THA between August 2018 and November 2019. Acetabular cup alignment and three-dimensional (3D) position were measured using pre- or postoperative computed tomography (CT) data. Absolute differences in cup inclination, anteversion, and 3D position were assessed, and their relation to preoperative factors was evaluated. The average measurement of the absolute differences was 1.8° ± 2.0° (inclination) and 1.9° ± 2.3° (anteversion). The average absolute difference in the 3D cup position was 1.1 ± 1.2 mm (coronal plane) and 0.9 ± 1.0 mm (axial plane). Multivariate analysis revealed that a posterior pelvic tilt [odds ratio (OR, 1.1; 95% confidence interval (CI), 1.00–1.23] and anterior surgical approach (OR, 5.1; 95% CI, 1.69–15.38) were predictive factors for inaccurate cup positioning with robot-assisted THA. This is the first study to demonstrate the predictive risk factors (posterior pelvic tilt and anterior surgical approach) for inaccurate cup position in robot-assisted THA.
Similar content being viewed by others

Introduction
Acetabular cup positioning is important for early and long-term outcomes of total hip arthroplasty (THA), and malposition is recognized as a risk factor for postoperative complications, such as impingement, dislocation, and accelerated polyethylene wear, after THA1,2,3. However, even experienced surgeons find it difficult to achieve accurate target cup positioning4. Previous reports have demonstrated several factors that lead to inaccurate cup positioning. The factors included patient characteristics comprising body mass index (BMI)5, age6, gender6, and primary diagnosis for THA7 or surgery including the performing surgeon's experience6, the surgical approach8, and the prosthetic components9. To resolve this difficulty, various techniques, such as manual guides, intraoperative landmarks, intraoperative X-ray or fluoroscopy, computer navigation, and robotics, were developed to improve the accuracy and precision of acetabular cup positioning in THA10. Although computed tomography (CT)-free, fluoroscopy-based, and CT-based navigation systems were developed to improve component positioning in THA11,12,13, several risk factors for inaccurate cup positioning with navigation-assisted THA, such as high BMI and posterior pelvic tilt, persisted14,15.
Recently, a new generation of robots was created for assistance during THA and accurate cup positioning16,17,18. Kanawade et al. reported that robot-assisted THA achieved precise cup inclination in 88% and anteversion in 84% within a 10° discrepancy between intraoperative planning angles and postoperative CT validation18. Nodzo et al. reported a significant correlation in inclination and anteversion between intraoperative angles and postoperative CT validation17.
However, to the best of our knowledge, no study has analyzed the predictive risk factors for inaccurate cup position in robot-assisted THA. This is important because it is difficult to notice an inaccurate cup location and adjust positioning during robot-assisted THA. We hypothesize that robot-assisted THA can achieve accurate cup placement. However, we believe that several predictive risk factors for inaccurate cup positioning may exist. Therefore, this study aimed to investigate the accuracy of cup placement and determine the predictive risk factors for inaccurate cup positioning in robot-assisted THA.
Patients and methods
Patients
In this retrospective cohort study, we enrolled 121 consecutive patients (121 joints). Of the 121 joints, 6 were excluded from this study because of missing data sets, including postoperative CT data; finally, 115 patients (115 joints) were analyzed in this study. All patients were diagnosed with osteoarthritis (grade 4 according to the Tönnis classification system) or avascular necrosis of the femoral head (stage 4, 5, or 6 according to the Steinberg staging of avascular necrosis) and underwent robot-assisted THA (MAKO Rio Robot, Ft. Lauderdale, FL) between August 2018 and November 2019. Thirty-one patients had developmental dysplasia of the hip (DDH), which was defined as a lateral center-edge (CE) angle of Wiberg less than 20°19. All surgical procedures were performed using a mini-anterolateral approach in the supine position20 or posterior approach in the lateral position by three senior surgeons. One surgeon usually used the MIS-anterior lateral supine approach; however, a posterior approach was used when the patient’s BMI was over 35 kg/m2 or in severe DDH cases. Conversely, two other surgeons used the posterior approach for all patients.
The demographic data of patients are shown in Table 1.
Preoperative plan and surgery
Preoperative CT scans from the level of the iliac wing to the femoral condyle were obtained. The slice thickness was 1 mm, and the CT data were transferred to the MAKO planning module. Subsequently, preoperative planning was performed to determine the optimal component size, angle, and position using the three-dimensional (3D) templating software of the MAKO robotic hip system before surgery. The target cup inclination angle was usually fixed at 40°, and the anteversion angle was determined preoperatively according to Widmer’s combined anteversion theory21 with respect to the functional pelvic plane22. Pelvic tilt was defined as the inclination angle of the anterior pelvic plane, determined by both the anterior superior iliac spines and the pubic tubercles, relative to the table plane. The patients underwent THA with a Trident hemispherical cup and Accolade II or Exeter v40 stems (Stryker Orthopaedics, Mahwah, NJ, USA).
The robot-assisted THA procedures were performed with the MAKO robotic hip system, which is a robot-assisted computer navigation system that uses the RIO robotic arm (MAKO Rio Robot) to ream the acetabulum and place the acetabular component. After placement of the acetabular cup, one or two screws were inserted, and the intraoperative cup alignment was confirmed by touching five points at the cup edge using the navigation pointer. Full-weight bearing was allowed 1 day after surgery in all patients.
Postoperative evaluation
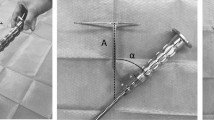
Postoperative CT scans were obtained 1 week after surgery, and the data were transferred to the OrthoMap 3D Navigation System (Stryker Orthopaedics). The computer-aided design models of the implants were manually adjusted for postoperative multi-planar reconstruction of the CT images (Fig. 1). Cup inclination and anteversion angles were measured with respect to the functional pelvic plane. To analyze the accuracy of cup alignment, we compared the absolute differences in cup alignment between the postoperative measurements, navigation records, and preoperative plans. To assess the cup position in the axial axis, a normal vector line passing through the cup center was drawn in the axial views of the preoperative plans on the MAKO workstation (Fig. 2) and the postoperative reconstruction image on the OrthoMap 3D workstation (Fig. 3). To assess the cup position in the coronal axis, a horizontal line passing through the cup center was drawn in the coronal views on the preoperative plans and postoperative images (Figs. 2 and 3). The distance between the outer edge of the cup and the medial edge of the acetabulum on the line was measured, and the absolute differences in distance between that assessed in the preoperative plan and the postoperative measurement were calculated in the axial and coronal views (Figs. 2 and 3).

Acetabular cup angles are measured by superimposing the templates of the acetabular cup on postoperative images of the acetabular component.

Preoperative cup positions are measured on the MAKO workstation. White lines indicate the distance between the outer edge of the cup and the medial edge of the acetabulum in axial and coronal views.

Postoperative cup positions are measured on the OrthoMap 3D Navigation System workstation. White lines indicate the distance between the outer edge of the cup and the medial edge of the acetabulum in axial and coronal views.
Statistics
All data are expressed as mean ± standard deviation (SD) unless otherwise indicated. The differences in cup angles between that evaluated in preoperative plans and postoperative CT measurements were analyzed by paired t-test (Table 2). The average measurements of the absolute differences in cup alignment in cases where the posterior approach was used by the surgeons were analyzed using one-way analysis of variance. The outliers of accurate acetabular cup placement were defined as an absolute difference in inclination or anteversion of more than 5° and a difference in distance between preoperative plans and postoperative CT measurements of more than 3 mm, according to previous reports18,23,24. To identify predictive factors of the outliers in postoperative cup malposition with robot-assisted THA, outliers and non-outliers were compared using the Fisher’s exact test for nominal variables (Tables 3 and 5) and the unpaired t-test for continuous variables (Tables 4 and 6). Additionally, we performed a multivariate analysis to test the association between acetabular shape, surgical approach, and pelvic tilt with outliers of cup placement (Table 7). Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated using the Fisher’s exact test and multivariate analysis. The database was analyzed using SPSS version 16.0 (IBM Corp., Armonk, NY, USA), and p-values < 0.05 were considered statistically significant.
For Fisher’s exact test, a power calculation using G*Power 325 determined that a minimum total sample size of 114 patients would be sufficient to ascertain whether there was a significant difference. A power of 0.8, prespecified significance level of α < 0.05, and allocation ratio (N1/N2) based on the preliminary study with 30 cases (with an OR of 5 or more) was set as a clinically meaningful difference. For the unpaired t-test, we calculated the effect size using means and SDs based on the Hedges’ g for each parameter and a 95% CI for effect sizes26.
Ethics
This study complies with the Declaration of Helsinki, study protocols were approved by the ethics committee of the Kobe University Graduate School of Medicine, and all participants provided informed consent for participation.
Results
Robot-assisted THA accurately reproduced the preoperative plan of cup angles and positions
Table 2 provides the average angles of cup inclination and anteversion documented in the preoperative plans, intra-operative navigation records, and postoperative measurements. The average inclination angle in the preoperative plan was 40°, and the average anteversion angle was 19.2°. The average angles did not reveal any remarkable change between the preoperative plans and postoperative measurements (Table 2). The average measurements of absolute differences in cup alignment (postoperative CT measurement-preoperative plan) were 1.8° ± 2.0° (inclination) and 1.9° ± 2.3° (anteversion) for all cases (Table 2). Additionally, we compared the average measurements of the absolute differences in cup alignment in cases where the posterior approach was used, and no significant difference in cup alignment was observed among the three surgeons (p = 0.518).
Reproducibility of cup angles using robot-assisted THA with changes in the pelvic tilt
No notable differences were observed in the frequencies of cup inclination or anteversion outliers on treated sides, surgical approaches, and acetabular shape (Table 3).
Table 4 presents the mean values of BMI, age, and pelvic tilt angles of patients in the outlier and non-outlier groups. The average BMI and age of the patients revealed no significant differences for inclination and anteversion angles. However, the mean pelvic tilt angle was significantly different between the outlier and non-outlier groups for anteversion (p = 0.029) (Table 4).
Reproducibility of 3D cup positions using robot-assisted THA with variations in surgical approaches
The accuracy of 3D cup positioning was estimated, and the average absolute differences in the distance (postoperative CT-preoperative plan) were 1.1 ± 1.2 mm (coronal plane) and 0.9 ± 1.0 mm (axial plane). No significant differences were observed in the frequency of 3D cup position outliers on the treated sides and acetabular shapes. However, we observed a significant difference in the frequency of 3D cup position outliers between patients who underwent surgery via an anterior or posterior approach (p-value = 0.004) (Table 5).
Table 6 presents the mean values of BMI, age, and pelvic tilt angles of patients in the outlier and non-outlier groups. The average BMI, age, and pelvic tilt were not significantly different between the outlier and non-outlier groups regarding the 3D cup position.
Predictive factors for outliers of postoperative cup placement with robot-assisted THA
We noted that two predictive factors (surgical approach and pelvic tilt) were related to postoperative cup malposition with robot-assisted THA based on unpaired t-test results for continuous variables and Fisher’s exact test results for nominal observations. However, the predictive factors for outliers could be dependent on multiple confounders. Therefore, these two significant predictive factors were used as covariates for multivariate analysis. We discerned that outliers of postoperative cup anteversion with robot-assisted THA were significantly associated with posterior pelvic tilt (OR, 1.1; 95% CI, 1.00–1.23), and the outliers of cup position were associated with an anterior approach (OR, 5.1; 95% CI, 1.69–15.38) (Table 7).
Discussion
We examined the reproducibility of cup placement with robot-assisted THA in this study. This is the first study to demonstrate that a posterior pelvic tilt and anterior surgical approach were significantly associated with postoperative inaccurate cup positioning.
Several reports have analyzed the various factors associated with inaccurate cup positioning with robot-assisted THA23,27. Gupta et al. conducted a study in obese patients and found no significant correlation between BMI and acetabular anteversion/ inclination27. Their results support our findings that BMI did not affect the accuracy of cup inclination, anteversion, or 3D cup position with robot-assisted THA.
Previous studies have demonstrated a higher complication rate comprising loosening of the acetabular component and postoperative dislocation after THA in DDH patients28,29,30. The reason for the higher complication rate is inaccurate acetabular cup positioning due to an inadequate acetabular roof, a double acetabular floor, the presence of osteophytes, and a difficulty in identifying the accurate orientation of the acetabulum28,29,30. However, several studies described an accurate cup placement with CT-based navigation in DDH cases12,31,32. Similarly, we demonstrated no differences in the accuracy of cup positioning between DDH and non-DDH patients after robot-assisted THA.
Several reports demonstrated that the posterior approach could achieve accurate 3D cup positions with navigation THA33,34. Nakahara et al. demonstrated in a case series using the posterior approach that the CT-based navigation accuracy of the implant position, which was defined as differences between the postoperative measurements on CT images and intraoperative records on the navigation system, was within a 2-mm difference34. However, we did not find any literature focused on 3D cup positions of the mini-anterior surgical approach with robot-assisted THA. In this study, we observed that a mini-anterior approach affected 3D implant position with robot-assisted THA. Minimally invasive surgical approaches are currently used for THA. Mini-incision THA reduces postoperative pain and blood loss, leads to a speedy recovery, and reduces hospital stay compared to THA performed using a standard approach35. However, some researchers are concerned that mini-incision THA may introduce new potential problems related to a reduced visual field during surgery, such as implant malposition, neurovascular injury, and poor implant fixation36. The visual field during manual registration of landmarks during a mini-anterior approach in the supine position was much smaller than that during a posterior approach, with difficulty in the registration of the anterior and posterior wall edges (Fig. 4). A sufficient visualization of the surgical field is essential for the registration of the cup positioning, and the idea of improving accuracy despite the approach is needed for robot-assisted THA implantation.

Photographs of the acetabular visual field during registration. (a) Mini-anterolateral approach, (b) posterior approach.
We also determined that a posterior pelvic tilt affected the accuracy of postoperative cup anteversion with robot-assisted THA. Previous simulation studies suggest that changes in pelvic tilt would lead to changes in the acetabular anteversion37. Yamada et al. reported that the accuracy of cup anteversion in CT-based navigation was lower in patients with a greater posterior pelvic tilt15. Hasegawa et al. also stated that posterior pelvic tilt affected the accuracy of postoperative cup anteversion angle in a mini-anterolateral approach using an accelerometer-based portable navigation system38. We had previously reported that preoperative posterior pelvic tilt was significantly associated with greater pelvic motion on the axial axis during surgery39, and the greater motion could cause anteversion errors even with robot-assisted THA.
Our study had some limitations. First, the number of patients included in the study was too small to analyze all the aspects of robot-assisted THA. Secondly, this was not a randomized trial but a retrospective cohort study with inherent limitations.
Conclusion
This is the first study to determine the predictive risk factors of inaccurate cup position in robot-assisted THA. Posterior pelvic tilt and anterior surgical approach were significantly associated with postoperative inaccurate cup positioning in robot-assisted THA. Thus, it is imperative to pay attention to these findings in THA cases to reduce errors.
References
Hedlundh, U. & Fredin, H. Patient characteristics in dislocations after primary total hip arthroplasty. 60 patients compared with a control group. Acta Orthop. Scand. 66(3), 225–228 (1995).
Lewinnek, G. E., Lewis, J. L., Tarr, R., Compere, C. L. & Zimmerman, J. R. Dislocations after total hip-replacement arthroplasties. J. Bone Joint Surg. Am. 60(2), 217–220 (1978).
Kennedy, J. G. et al. Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J. Arthroplasty. 13(5), 530–534 (1998).
Saxler, G. et al. The accuracy of free-hand cup positioning—A CT based measurement of cup placement in 105 total hip arthroplasties. Int. Orthop. 28(4), 198–201 (2004).
Azodi, O. S. et al. High body mass index is associated with increased risk of implant dislocation following primary total hip replacement—2,106 patients followed for up to 8 years. Acta Orthop. 79(1), 141–147 (2008).
Sanchez-Sotelo, J. & Berry, D. J. Epidemiology of instability after total hip replacement. Orthop. Clin. N. Am. 32(4), 543 (2001).
Conroy, J. L. et al. Risk factors for revision for early dislocation in total hip arthroplasty. J. Arthroplasty 23(6), 867–872 (2008).
Arthursson, A. J., Furnes, O., Espehaug, B., Havelin, L. I. & Soreide, J. A. Prosthesis survival after total hip arthroplasty—Does surgical approach matter? Analysis of 19,304 Charnley and 6,002 Exeter primary total hip arthroplasties reported to the Norwegian Arthroplasty Register. Acta Orthop. 78(6), 719–729 (2007).
Jasty, M. et al. Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J. Bone Joint Surg. Am. 79(3), 349–358 (1997).
Sugano, N. Computer-assisted orthopaedic surgery and robotic surgery in total hip arthroplasty. Clin. Orthop. Surg. 5(1), 1–9 (2013).
Kalteis, T. et al. Greater accuracy in positioning of the acetabular cup by using an image-free navigation system. Int. Orthop. 29(5), 272–276 (2005).
Jingushi, S. et al. Computed tomography-based navigation to determine the socket location in total hip arthroplasty of an osteoarthritis hip with a large leg length discrepancy due to severe acetabular dysplasia. J. Arthroplasty. 22(7), 1074–1078 (2007).
Kalteis, T. et al. Imageless navigation for insertion of the acetabular component in total hip arthroplasty: Is it as accurate as CT-based navigation?. J. Bone Joint Surg. Br. 88(2), 163–167 (2006).
Buller, L. T., McLawhorn, A. S., Romero, J. A., Sculco, P. K. & Mayman, D. J. Accuracy and precision of acetabular component placement with imageless navigation in obese patients. J. Arthroplasty 34(4), 693–699 (2019).
Yamada, K. et al. Accuracy of cup positioning with the computed tomography-based two-dimensional to three-dimensional matched navigation system: A prospective, randomized controlled study. J. Arthroplasty 33(1), 136–143 (2018).
Kamara, E., Robinson, J., Bas, M. A., Rodriguez, J. A. & Hepinstall, M. S. Adoption of robotic vs fluoroscopic guidance in total hip arthroplasty: Is acetabular positioning improved in the learning curve?. J. Arthroplasty. 32(1), 125–130 (2017).
Nodzo, S. R. et al. Intraoperative placement of total hip arthroplasty components with robotic-arm assisted technology correlates with postoperative implant position: A CT-based study. Bone Joint J. 100-B(10), 1303–1309 (2018).
Kanawade, V., Dorr, L. D., Banks, S. A., Zhang, Z. & Wan, Z. Precision of robotic guided instrumentation for acetabular component positioning. J. Arthroplasty. 30(3), 392–397 (2015).
Wiberg, G., Frey, H. Studies on Dysplastic Acetabula and Congenital Subluxation of the Hip Joint, with Special Reference to the Complication of Osteo-arthritis. 135 (P. A. Norstedt & Söner; 1939).
Hayashi, S. et al. Evaluation of the accuracy of acetabular cup orientation using the accelerometer-based portable navigation system. J. Orthop. Sci. 25(4), 612–617 (2020).
Widmer, K. H. & Zurfluh, B. Compliant positioning of total hip components for optimal range of motion. J. Orthop. Res. 22(4), 815–821 (2004).
Miki, H. et al. Anatomic hip range of motion after implantation during total hip arthroplasty as measured by a navigation system. J. Arthroplasty. 22(7), 946–952 (2007).
Redmond, J. M. et al. Accuracy of component placement in robotic-assisted total hip arthroplasty. Orthopedics 39(3), 193–199 (2016).
Kajino, Y. et al. Does degree of the pelvic deformity affect the accuracy of computed tomography-based hip navigation?. J. Arthroplasty. 27(9), 1651–1657 (2012).
Faul, F., Erdfelder, E., Buchner, A. & Lang, A. G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods. 41(4), 1149–1160 (2009).
Durlak, J. A. How to select, calculate, and interpret effect sizes. J. Pediatr. Psychol. 34(9), 917–928 (2009).
Gupta, A. et al. Does robotic-assisted computer navigation affect acetabular cup positioning in total hip arthroplasty in the obese patient? A comparison study. J. Arthroplasty. 30(12), 2204–2207 (2015).
Stans, A. A., Pagnano, M. W., Shaughnessy, W. J. & Hanssen, A. D. Results of total hip arthroplasty for Crowe type III developmental hip dysplasia. Clin. Orthop. Relat. Res. 348, 149–157 (1998).
Rogers, B. A. et al. Total hip arthroplasty for adult hip dysplasia. J. Bone Joint Surg. Am. 94(19), 1809–1821 (2012).
Argenson, J. N., Flecher, X., Parratte, S. & Aubaniac, J. M. Anatomy of the dysplastic hip and consequences for total hip arthroplasty. Clin. Orthop. Relat. Res. 465, 40–45 (2007).
Yamada, K. et al. Accuracy of cup positioning with the computed tomography-based two-dimensional to three-dimensional matched navigation system: A prospective, randomized controlled study. J. Arthroplasty. 33(1), 136–143 (2018).
Tsutsui, T. et al. Efficacy of a computed tomography-based navigation system for placement of the acetabular component in total hip arthroplasty for developmental dysplasia of the hip. J. Orthop. Surg. (Hong Kong). 25(3), 2309499017727954 (2017).
Iwana, D. et al. Accuracy of angle and position of the cup using computed tomography-based navigation systems in total hip arthroplasty. Comput. Aided Surg. 18(5–6), 187–194 (2013).
Nakahara, I., Kyo, T., Kuroda, Y. & Miki, H. Effect of improved navigation performance on the accuracy of implant placement in total hip arthroplasty with a CT-based navigation system. J. Artif. Organs. 21(3), 340–347 (2018).
Mayr, E. et al. A prospective randomized assessment of earlier functional recovery in THA patients treated by minimally invasive direct anterior approach: A gait analysis study. Clin. Biomech. 24(10), 812–818 (2009).
Woolson, S. T., Mow, C. S., Syquia, J. F., Lannin, J. V. & Schurman, D. J. Comparison of primary total hip replacements performed with a standard incision or a mini-incision. J. Bone Jt. Surg. Am. Vol. 86(7), 1353–1358 (2004).
Buckland, A. J. et al. Acetabular anteversion changes due to spinal deformity correction: Bridging the gap between hip and spine surgeons. J Bone Joint Surg. Am. 97(23), 1913–1920 (2015).
Hasegawa, M., Naito, Y., Tone, S., Wakabayashi, H., Sudo, A. Accuracy of acetabular cup insertion in an anterolateral supine approach using an accelerometer-based portable navigation system. J. Artif. Organs. (2020).
Kamenaga, T. et al. Intraoperative pelvic movement is associated with the body mass index in patients undergoing total hip arthroplasty in the supine position. J. Orthop. Sci. 25(3), 446–451 (2020).
Author information
Authors and Affiliations
Contributions
S.Hay. participated in the study design, drafting of the manuscript, and data collection. S.Has. carried out data collection and drafting of the manuscript. Y.K. participated in the data collection and drafting of the manuscript. N.N. participated in the study design and helped to revised the manuscript. TM participated in the data collection and drafting of the manuscript. K.I. carried out data collection and drafting of the manuscript. N.S. participated in the data collection and drafting of the manuscript. T.K. participated in the data collection and drafting of the manuscript. R.K. participated in the study design and helped to revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hayashi, S., Hashimoto, S., Kuroda, Y. et al. Accuracy of cup position following robot-assisted total hip arthroplasty may be associated with surgical approach and pelvic tilt. Sci Rep 11, 7578 (2021). https://doi.org/10.1038/s41598-021-86849-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-86849-0
This article is cited by
-
A novel imageless accelerometer-based navigation system improves acetabular cup placement accuracy during total hip arthroplasty in the lateral decubitus position
Archives of Orthopaedic and Trauma Surgery (2024)
-
Accuracy comparison of cup positioning during total hip arthroplasty using Hip Align and AR-Hip in the supine position
Archives of Orthopaedic and Trauma Surgery (2023)
-
Comparing the accuracy of three-dimensional mini-optical portable navigation and accelerometer-based portable navigation system for acetabular cup placement during total hip arthroplasty
Archives of Orthopaedic and Trauma Surgery (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
