
Abstract
The extensive utilization of electronic health records (EHRs) and the growth of enormous open biomedical datasets has readied the area for applications of computational and machine learning techniques to reveal fundamental patterns. This study’s goal is to develop a medical treatment recommendation system using Korean EHRs along with the Markov decision process (MDP). The sharing of EHRs by the National Health Insurance Sharing Service (NHISS) of Korea has made it possible to analyze Koreans’ medical data which include treatments, prescriptions, and medical check-up. After considering the merits and effectiveness of such data, we analyzed patients’ medical information and recommended optimal pharmaceutical prescriptions for diabetes, which is known to be the most burdensome disease for Koreans. We also proposed an MDP-based treatment recommendation system for diabetic patients to help doctors when prescribing diabetes medications. To build the model, we used the 11-year Korean NHISS database. To overcome the challenge of designing an MDP model, we carefully designed the states, actions, reward functions, and transition probability matrices, which were chosen to balance the tradeoffs between reality and the curse of dimensionality issues.
Similar content being viewed by others


Introduction
Medical treatment can be viewed as a series of interactions between patients and doctors. Doctors observe the state of patients through various types of examinations and choose treatments accordingly. The patients’ state changes in response to the treatment. These are called sequential decision processes since a sequence of interrelated decisions must be made over time. At a broad level, modeling of dynamic sequential decision making in medicine has a long and varied history. The Markov-based approach that we have used falls into the category of these modeling techniques, which were originally described in terms of medical decision-making by Beck and Pauker1. Other approaches utilize dynamic influence diagrams2 or decision trees3,4 to model temporal decisions. In all cases, the goal is to determine optimal sequences of decisions over a particular horizon.
Markov decision processes (MDPs) comprise one such efficient technique for determining optimal sequential decisions in dynamic and uncertain environments5,6. However, there have been relatively few applications in healthcare5,6,7,8,9,10,11. MDPs directly address many of the challenges faced in clinical decision-making4,5. Even though clinicians usually decide the treatment regimen taking into account patient's health condition, the effect of treatment for a given patient is unsure and this ambiguity is only exacerbated by an attempt to predict the results of a series of treatments over time.
A challenge in applying MDPs is that they require a data-intensive estimation step to generate reasonable transition and observation models. Large state/action spaces are also computationally expensive to solve, particularly in partially observable settings, and must adhere to specific Markov assumptions that the current time point (t) is dependent only on the previous time point (t − 1). Careful formulation of the problem and state space is necessary to handle such issues4,6.
The sharing of EHRs by the National Health Insurance Service (NHISS) of Korea has made it possible to analyze medical treatments, prescriptions, and medical check-up using Koreans’ Electronic Health Records (EHRs). After considering the merits and effectiveness of such data, we analyzed the medical information of patients and recommended the optimal pharmaceutical prescription for diabetes, known to be the most burdensome disease for Koreans. When prescribing diabetes medications, doctors would consider the patient's state such as complications, period of having diabetes, fasting plasma glucose and more. The initial medication treatment for diabetes starts from single therapy using metformin12,13. The doctors can move to double or triple therapy when patient's condition is not appropriate for single or double therapy respectively14,15,16,17. In previous studies, it is effective to choose multiple (double/triple) therapy as early as possible for maintaining proper glucose level as well as preventing complications14,18,19,20.
The goal of this study was to develop a diabetes treatment recommendation system using the EHRs of Koreans in combination with MDP which addresses the challenges stated above. The system decides to recommend whether to use single, double, or triple therapy of diabetes medication according to the state of diabetes patient. While a few previous studies have evaluated the medical recommendations for diabetes through MDP8,9,10,11,21, despite the challenges of MDP, their models only considered a few states and actions while proposing recommendations. To overcome these challenges, we increased the number of states and actions to as many as possible, so as to contain more information on patients and to provide various choices of recommendations for treating diabetes. In our paper, optimal diabetes medication recommendation by MDP model is the principal outcome. We recommended medication type either single, double, or triple according to the states of patient. Quality-adjusted life year (QALY) is used for reward function to quantify the quality of a year of life with the discomfort due to medical interventions such as diabetic complications. With QALY, MDP model can recommend optimal medication for each state of patient by choosing medication which has highest reward value. For diabetes patients, high blood sugar levels can serious damage many organs of our body leading to diabetic complications. Therefore, it is important to prevent diabetic complications by controlling blood sugar level well. To prevent diabetic complications, we recommended appropriate medication according to the state of patient by our MDP model. Lastly, we proved diabetic complication occurrence can be delayed by our MDP medical recommendations.
Materials and methods
Institutional review board statement
This study was approved by the Institutional Review Board (IRB) of Yonsei University (IRB NO. 7001988-201808-h-444-01E). This is data based research which, data was provided from National Health Insurance Sharing Service (NHISS) of Korea.
The NHISS is a national agency established to enhance the access and convenience of utilization of National Health information on data. The NHISS collects the human data in accordance with relevant guidelines and regulations which includes that informed consent was obtained from all subjects (if subjects are under 18, from a parent and/or legal guardian).
MDP model
We used the MDP model to find the optimal prescription strategy based on patients’ health states over the course of their lifetime. Our model’s objective was to determine the optimal treatment strategy for a single patient that maximizes his/her expected discounted QALY over a planning horizon, t = 1, … , T. We adopted QALY in our model to improve the patients’ expected time in a healthy state by delaying the onset of diabetic complications.
The MDP model consists of four features: [S, A, T, R], where S is a set of states, A is a set of actions, T:S × A × S → [0,1] is a set of state transition probabilities, and R:S × A × S × R → [0,\infty] is a reward function.
State space S
The state space in our model included the following five components of patients’ information:
\({S}_{Chronic}^{t}\) is the state of having chronic complications of diabetes at time t for t = 1,…,T. If a patient has one or more chronic complication(s) at time t it is 1, or else, it is 0. We considered six chronic complications such as diabetic retinopathy, diabetic cataract, and so on, as shown in Table 1. We also stated the International Classification of Diseases (ICD-10) codes which we used to define each symptom in the dataset.
\({S}_{Acute}^{t}\) is the state of having acute complications of diabetes at time t for t = 1,…,T. It is 1, if a patient has one or more of the three acute complications in Table 1, otherwise it is 0.
\({S}_{Risk}^{t}\) represents whether a patient is in severe risk state of diabetes or not. It is 1 when the patient is at a severe risk state, otherwise it is 0. To assess the likelihood of a patient having diabetes, we used the Diabetes Risk Score22, which was designed as a screening tool for identifying high-risk individuals in the population and for increasing awareness relating to modifiable risk factors and healthy lifestyles23. The score is based on seven factors such as sex, age, BMI, family history, smoking, intake of hypertension medication, and intake of steroid medication. If the score is above the threshold (we have used 15 as the median value for the threshold) it is 1, otherwise it is 0. We used the diabetes risk in state space is to compress many information of patient in one state space to avoid curse of dimensionality problem in MDP and also we believed that \({S}_{Risk}^{t}\) can also reflect the severe state of patient who already has diabetes.
\({S}_{Period}^{t}\) represents time elapsed since the occurrence of diabetes. If the time is less than or equal to 4 years, it is 0. If the time ranges between 5 to 8 years, it is 1, otherwise it is 2.
Lastly, \({S}_{FPG}^{t}\) represents the fasting plasma glucose (FPG) level. If the level is below 100 mg/dL, it is 0, between 100 to 125 mg/dL it is 1, and above 125 mg/dL it is 2. These three levels were divided into stages of: normal, impaired FPG level but might not have diabetes, and abnormal.
The total number of states in our model are 72 (2 × 2 × 2 × 3 × 3). Due to the state space explosion and computing power challenges, we tried to keep the model as simple as possible, whilst retaining as much information as possible.
Action space A
The action of our model comprised prescriptions for diabetes patients. We selected eight possible actions as shown in Table 2, which consists of mono, dual, and triple therapies which as their names indicate, imply prescribing one, two, and three medications, respectively. Generally, monotherapy is used for less severe patients while dual and triple therapies are used for more severe patients.
Table 2 shows the popular medications for diabetes with corresponding frequencies. There are eight popular medications for diabetes: Metformin (MET), Sulfonylureas (SUL), Meglitinides (MEG), Thiazolidinediones (TZD), DPP-4 inhibitors (DPP4I), GLP-1 receptor agonists (GLP-1RA), and insulin. Dual therapies combine two medications out of the eight possible medications. Popular dual therapies are MET + SUL, MET + DPP4I, and so on. Popular triple therapies are MET + SUL + AGI, MET + SUL + TZD, and MET + SUL + DPP4I.
Since the number of combinations would have increased exponentially had we considered all possible prescriptions, we decided to limit the number of possible actions to overcome action space explosions. Therefore, in Fig. 1, we sorted the medications by frequency of prescription in our dataset and chose the top two medications for each type and classified other medication as “others.” However, for triple therapy we chose only one specific action (number 7) because, other than that, the other triple therapy prescription frequencies were very low to be taken as actions.

Diabetes medication prescription percentages in the dataset. This figure shows the diabetes medications prescription by frequency in our dataset. We classified the medication by number of medications prescribed (mono, dual, triple-therapy). The poll shows the percentage of each medications.
Transition probability matrices (TPM)
In the MDP model, we needed as many transition probability matrices as the number of actions, which can be denoted by T(s,s′,a) for \(s,{s}^{{\prime}}\in S, a\in A.\) To compute T(s,s′,a), we counted the number of occurrences from state s to state s′ after taking medication denoted by a for all \(s,{s}^{{\prime}}\in S,\) and \(a\in A\).
Once the counting was finished, we divided the number by the sum of the rows, so that the sum of each row becomes 1.
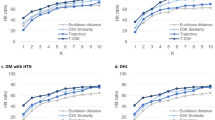
One issue with the TPM model was that some rows did not have any occurrences. In such cases, transition between certain states was rare. To deal with the blank state, we calculated the cosine similarity between each vector by sex, state, and actions to check if we could fill in the blank state with another matrix. Table 3 shows the results of vector similarity.
In Table 3, both gender and actions have similarity values above 0.9 which means they are very similar. Thus, we could obtain the value from between gender and actions to fill blank states in TPM.
Reward R
The reward function \(\mathrm{R}\left(\mathrm{a},{\mathrm{s}}^{{{\prime}}}\right)\) of our model is the patient’s expected discounted QALYs as shown in Eq. (1), where a is an action and s′ is its resulting state. Health services researchers typically use QALYs to quantify the quality of a year of life with the discomfort due to medical interventions. Treating or screening a patient for a chronic disease will offer some reward to the patient, such as a potentially longer life. However, these benefits come at some “cost” to the patient, whether it be a reduction in quality of life, such as side effects due to medications or discomfort due to a screening test, or a financial cost, such as medication or hospitalization expenses. The QALY is also used by many health care researchers21,24,25. We, too, adopted it in our model.
Here, \({R}^{WTP}\) is a willingness to pay for a QALY of 1 which represents a patient being in perfect health for one year without any disutilities caused by medical interventions and side effects of treatment. As the patient’s quality of life decreases due to side effects of medications or disablements from a disease, the QALY value will tend towards 0. We considered four decrement factors—\({d}^{Chronic}\left({s}^{{\prime}}\right)\), \({d}^{Acute}\left({s}^{{\prime}}\right)\), \({d}^{Risk}\left({s}^{{\prime}}\right),\) and \({d}^{Period}\left({s}^{{\prime}}\right)\)—due to chronic diseases, acute diseases, risk factors, and long duration in the model, details of which are shown in Table 4. Lastly \({C}^{MED}\) represents the costs of medication we used for actions26.
The values in the third column are the decrement values that we used in our study, which were taken from other studies26,27,28. For example, the patient with chronic diseases had a QALY of 0.895 (1–0.105).
Data descriptions
We used the National Health and Insurance Service–National Sample Cohort (NHIS–NSC) data—a population-based cohort—established by the NHISS in South Korea (data accessible upon payment)29. The cohort provides representative, useful information regarding citizens’ utilization of health insurance and health examinations. Currently the NHISS maintains and stores national records for healthcare utilization, prescriptions, and medical check-up. Medical check-up database contains major results from medical check-up and behavior and habitual data from questionnaire. Specifically, it includes the following contents: height, weight, waist, systolic and diastolic blood pressure, fasting plasma glucose, total cholesterol, triglyceride, HDL and LDL cholesterol, history (patient him/herself and family) of stroke, heart disease, hypertension, and diabetes, smoke status, drink habit, and exercise frequency. The cohort sampled in the 2002 database was followed until 2013, only if the participants were still eligible for health insurance. For additional information, health care in South Korea is provided by a compulsory National Health Insurance (NHI). Every South Korean is eligible for this insurance until his/her death, immigrant, or working in National Intelligence Service (NIS).
Data cleansing
Figure 2 shows the data cleaning process for maintaining proper records of diabetic patients. We selected diabetic patients’ records from the NSC data of one million that we could access from the NHISS database and filtered the patients with diabetes using the following criteria:
-
1.
Diagnosis of diabetes according to the 10th edition of the ICD-10 codes: E10–E14.
-
2.
Prescribed oral glucose-lowering medications for more than 30 days.

Process of data selection and number of patients included in each step. This figure shows the process of data cleansing for experiment.
Our database finally had 90,047 patients with diabetes which met the criteria.
After filtering out diabetes patients, we also worked on the “wash-out” process. Since we did not know the exact start period of diabetes for the patients in year 2002, we deleted all their data from every other year from 2002 up to 2013, and made year 2003 as the first year of our observation. After all the processing, the total population of diabetes patients was 69,446. All the participants were followed up from January 1, 2003, until the date of their deaths or December 31, 2013, whichever occurred earlier.
Data statistics
Table 5 shows the statistics of the 69,446 diabetes patients used for validation of the treatment recommendation system.
The male and female patients comprised 54% and 46% of the data, respectively, and their mean ages were 58.4 and 61.7, respectively. Female patients’ period of having diabetes was longer than that of the male patients by 0.9 year. For both sexes, BMIs were similar, FPG levels were above the risk level as they exceeded 140 mg/dL, and total cholesterol levels were normal. However, male patients’ blood pressure was in an “elevated” stage while female patients were in the hypertension stage 1. Lastly, the male and female patients who smoked were 65% and 48%, respectively.
Results
Optimal treatment recommendation result
The recommended treatment actions according to each component of the states are shown in Figs. 3 and 4 for males and females, respectively.

MDP recommendation actions on each state for male patients. This figure shows the recommended treatment actions according to each component of the states for male patients. (a) Is the recommended actions on complication states. (b) Is the recommended actions on risk states. (c) Is the recommended actions on period state and (d) is the recommended actions on FPG states. Grey shaded sqaure is for mono therapy recommendations. Open square is for dual therapy recommendations. And striped square is for triple therapy recommendations.

MDP recommendation actions on each state for female patients. This figure shows the recommended treatment actions according to each component of the states for female patients. (a) Is the recommended actions on complication states. (b) Is the recommended actions on risk states. (c) Is the recommended actions on period states and (d) is the recommended actions on FPG states. Grey shaded sqaure is for mono therapy recommendations. Open square is for dual therapy recommendations. And striped square is for triple therapy recommendations.
Our purpose was to observe the changing trends in recommended actions as the states changed. As regards recommended actions on complication states, for the state having no complications, monotherapy and dual therapy were recommended 78% and 22% of the times, respectively, whereas when the states changed to acute, chronic, and both complications, the recommendation level increased by 30%, 28%, and 39%, respectively, for dual therapy, along with a slight increase in triple therapy. For risk states, 56% of low risk patients were recommended monotherapy, but it decreased to 39% as it progressed to high risk, and the recommendations for dual and triple therapies increased by 12% and 6%, respectively, as compared to the low risk state. In the period states, patients in the “1 to 4 years” state were recommended monotherapy and dual therapy 71% and 29% times, respectively. However, when the period state increased to “4 to 8 years” and “9 to 11 years” recommendations for monotherapy reduced to 42% and 33%, respectively, while recommendations for dual-therapy increased to 54% and 63%, respectively, and those for triple therapy increased to 4% for both states. Lastly, in the FPG state, for the normal level patients, the recommendations for monotherapy and dual therapy were 63% and 37%, respectively. For patients whose FPG levels were impaired and abnormal, the recommendations for dual-therapy increased by 12% and 16% as well as 8% and 13% for triple-therapy, as compared to patients with normal levels.
The trends of MDP recommendation results for female patients, shown in Fig. 4 above, were similar to those for male patients. In relation to complication states, monotherapy and dual therapy were recommended 61% and 39% of the times, respectively, for patients without complications, whereas for those with acute, chronic, and both complications, dual therapy was recommended 50%, 67%, and 67% of the times, respectively, and triple-therapy 6%, 11%, and 6% of the times, respectively. For risk states, 72%, 25%, and 3% of low risk patients were recommended mono, dual, and triple therapies, respectively. As it progressed to high risk, the recommendation for monotherapy decreased to 33%, while that for dual and triple therapies increased to 61% and 6%, respectively. For period states, patients in the “1 to 4 years” state were recommended monotherapy and dual-therapy 54% and 46% of the times, respectively. In the “4 to 8 years” and “9 to 11 years” states, recommendations for monotherapy reduced by 4% and 29%, respectively, while recommendations for dual therapy increased by 4% and 19%, respectively, and that for triple therapy increased to 8% for the “9 to 11 years” state. For the FPG states, patients with normal levels were recommended monotherapy and dual therapy 58% and 42% of the times, respectively, while for those whose FPG levels were impaired and abnormal, the recommendations for dual therapy increased to 63% and 54%, respectively, and for triple therapy to 4% and 8%, respectively, compared to patients whose levels were normal.
Discussions
We validated the results of our recommendations by comparing them with doctors’ real life prescriptions. We also checked our recommendation system’s performance by observing the delay in the onset of diabetic complications. Since diabetes is usually accompanied by several complications, well-maintained diabetes could also imply the absence of complications.
Retrospective validation
We compared the optimal recommendations of the MDP model with doctors’ real life prescriptions using the NSC data to check the similarities between the two. Since we proposed an optimal recommendation for each state, our model had 72 optimal actions.
From the NSC database, we calculated the percentage of doctor’s prescriptions for each state. The most frequent prescriptions for each state were compared with the optimal policy of the MDP model. Table 6 shows the results. Of the 72 states, 49 and 44 matched for males and females, respectively. A comparison of the MDP recommendations and doctors’ real life prescriptions revealed matching scores of 68% and 61% for males and females, respectively. The matching percentage represents the count rate which exactly matched the MDP and real life doctors’ prescriptions.
Based on the fact that the prescriptions may vary according to the patients’ specific conditions and doctors’ treatment styles, we believe that the actions that our MDP recommended were acceptable outcomes. To verify this, we also compared the top three real life prescriptions for each state with MDP treatment recommendations. Table 7 shows the scores when the MDP recommendations matched with the top three real life prescriptions in the dataset. Of the 72 states, the scores matched in 63 and 58 states for male and female patients, respectively, and it increased by around 20% when compared to the top three prescriptions.
A comparison of the diabetic complication occurrence periods
Patients with diabetes are at a much higher risk than others of serious complications such as coronary heart disease, stroke, blindness, kidney diseases, amputation of limbs, and neurological disorders. Thus, it is important for these patients to avoid having such complications which in addition to lessening their quality of life, could even cause death.
Accordingly, we checked if MDP recommendations could delay the occurrence of diabetic complications by comparing individuals in the cohort who followed MDP recommendations with those who did not. For research justification, we compared the group who followed MDP recommendations by matching the period of the prescription. If the real life prescription matched the MDP recommendation and its period comprised more than 50% of the patients’ whole data period, we considered them as MDP followers. Their demographics with mean and standard deviation are provided in Table 8.
We computed the average period from the time diabetes was diagnosed to the occurrence of complications, and compared the two groups. The results showed that male and female patients who followed the MDP recommendations appeared to have delayed the onset of diabetic complications by 0.93 year and 0.88 year, respectively, as shown in Fig. 5. This result is meaningful since the main goal of diabetes treatment is lowering glucose levels as well as avoiding complications.

A comparison of the diabetic complication occurrence period between MDP recommendation followers and other prescription users. This figure shows the average period from the time diabetes was diagnosed to the occurrence of complications, and compared the MDP follower groups and other group. Grey shaded sqaure is for MDP follower group and Open square is for other prescription taker group.
The results have been verified as being statistically significant using the t-test. Since we set the alpha value at 0.05, if the p-value is less than 0.05, we can say that there is a statistically significant difference between the means of our two groups. Since both male and female patients had p = 1.46 × 10–33 and p = 7.59 × 10–20, respectively, which is < 0.05, the result is significant.
Conclusions
We proposed an MDP-based treatment recommendation system for diabetic patients. To build the model, we used the 11-year Korean NHISS database of one million patients for each year. To overcome the challenge of designing an MDP model, we carefully designed the states, actions, reward functions, and transition probability matrices, that were chosen to balance the trade-offs between reality and the curse of dimensionality issues.
Our results show that diabetes medication recommended by our MDP system is realistic as it correctly recommends the changing trends from monotherapy to dual and triple therapies, as the patients’ state deteriorates from normal to serious. Doctors, too, increase the number of medications and prescribe them in combination when the patients’ state does not improve. To check the validity of our results, we compared the MDP-based recommendation results with real life prescriptions. Considering that prescription could vary according to the specific condition of patients and treatment styles of doctors, we compared the top three real life prescriptions in each state with MDP treatment recommendations, and obtained 88% and 81% matches for male and female patients, respectively. Lastly, we proved that our MDP recommendation can maintain better health condition by delaying the occurrence of diabetic complications. The patients who followed MDP recommendations were able to delay the onset of complications longer than those who did not follow MDP recommendations. We believe that our proposed MDP recommendation system could help doctors to prescribe appropriate diabetes medications.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to containing potentially identifying patient information collected by National Health Insurance Sharing Service which requires payment for access. But are available from the corresponding author on reasonable request.
References
Beck, J. R. & Pauker, S. G. The Markov process in medical prognosis. Med. Decis. Making. 3(4), 419–458. https://doi.org/10.1177/0272989X8300300403 (1983).
Xiang, Y. & Poh, K. Time-critical dynamic decision modeling in medicine. Comput. Biol. Med. 32(2), 85–97 (2002).
Leong, T.Y. Dynamic decision modeling in medicine: a critique of existing formalisms. In Proc Annu Symp Comput Appl Med Care 478–484 (1993).
Stahl, J. E. Modelling methods for pharmacoeconomics and health technology assessment: An overview and guide. Pharmacoeconomics 26(2), 131–148. https://doi.org/10.2165/00019053-200826020-00004 (2008).
Schaefer, A., Bailey, M., Shechter, S. & Roberts,, M. Modeling medical treatment using Markov decision processes. In Operations Research and Health Care 593–612 (2005).
Alagoz, O., Hsu, H., Schaefer, A. J. & Roberts, M. S. Markov decision processes: A tool for sequential decision making under uncertainty. Med. Decis. Making. 30(4), 474–483. https://doi.org/10.1177/0272989X09353194 (2010) (Epub 2009 Dec 31).
Gocgun, Y., Bresnahan, B. W., Ghate, A. & Gunn, M. L. A Markov decision process approach to multi-category patient scheduling in a diagnostic facility. Artif. Intell. Med. 53(2), 73–81. https://doi.org/10.1016/j.artmed.2011.06.001 (2011) (Epub 2011 Jul 2).
Lobo, J. Treatment optimization for patients with type 2 diabetes. Decis. Anal. Optim. Dis. Prev. Treat. 349–365 (2018).
Kurt, M., Denton, B., Schaefer, A., Shah, N. & Smith, S. The structure of optimal statin initiation policies for patients with type 2 diabetes. Inst. Ind. Eng. Trans. Healthcare Syst. Eng. 1(1), 49–65 (2011).
Denton, B. T., Kurt, M., Shah, N. D., Bryant, S. C. & Smith, S. A. Optimizing the start time of statin therapy for patients with diabetes. Med. Decis. Making. 29(3), 351–367. https://doi.org/10.1177/0272989X08329462 (2009) (Epub 2009 May 8).
Eghbali-Zarch, M., Tavakkoli-Moghaddam, R., Esfahanian, F., Azaron, A. & Sepehri, M. M. A Markov decision process for modeling adverse drug reactions in medication treatment of type 2 diabetes. Proc. Inst. Mech. Eng. H. 233(8), 793–811. https://doi.org/10.1177/0954411919853394 (2019) (Epub 2019 Jun 10).
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 352(9131), 854–865 (1998).
Maruthur, N. M. et al. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 164(11), 740–751 (2016).
Qian, D. et al. Comparison of oral antidiabetic drugs as add-on treatments in patients with type 2 diabetes uncontrolled on metformin: A network meta-analysis. Diabetes Ther. 9, 1945–1958 (2018).
Zaccardi, F. et al. Comparison of glucose-lowering agents after dual therapy failure in type 2 diabetes: A systematic review and network meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 20, 985–997 (2018).
Lee, C. M., Woodward, M. & Colagiuri, S. Triple therapy combinations for the treatment of type 2 diabetes: A network meta-analysis. Diabetes Res. Clin. Pract. 116, 149–158 (2016).
Lozano-Ortega, G. et al. Network meta-analysis of treatments for type 2 diabetes mellitus following failure with metformin plus sulfonylurea. Curr. Med. Res. Opin. 32, 807–816 (2016).
Cai, X., Gao, X., Yang, W., Han, X. & Ji, L. Efficacy and safety of initial combination therapy in treatment-naive type 2 diabetes patients: A systematic review and meta-analysis. Diabetes Ther. 9, 1995–2014 (2018).
Olansky, L. et al. A treatment strategy implementing combination therapy with sitagliptin and metformin results in superior glycaemic control versus metformin monotherapy due to a low rate of addition of antihyperglycaemic agents. Diabetes Obes. Metab. 13, 841–849 (2011).
Hadjadj, S., Rosenstock, J., Meinicke, T., Woerle, H. J. & Broedl, U. C. Initial combination of empagliflozin and metformin in patients with type 2 diabetes. Diabetes Care 39, 1718–1728 (2016).
Steimle, L. & Denton, B. Markov decision processes for screening and treatment of chronic diseases. In International Series in Operations Research & Management Science 189–222 (2017).
Griffin, S. J., Little, P. S., Hales, C. N., Kinmonth, A. L. & Wareham, N. J. Diabetes risk score: Towards earlier detection of type 2 diabetes in general practice. Diabetes Metab. Res. Rev. 16(3), 164–171. https://doi.org/10.1002/1520-7560(200005/06)16:3<164::aid-dmrr103>3.0.co;2-r (2000).
Lindström, J. & Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 26(3), 725–731. https://doi.org/10.2337/diacare.26.3.725 (2003).
Komorowski, M. & Raffa, J. Markov models and cost effectiveness analysis: applications in medical research. Secondary Analysis of Electronic Health Records 351–367 (2016).
Steimle, L. N., Kaufman, D. L. & Denton, B. T. Multi-model Markov decision processes. Optimization Online 2018. http://www.optimization-online.org/DB_FILE/2018/01/6434.pdf.
Centers for Medicare & Medicaid Services. National Average Drug Acquisition Cost (NADAC). 2015. https://data.medicaid.gov/Drug-Pricing-and-Payment/NADAC-as-of-2015-02-11/xgrz-pm3t.
Tengs, T. O. & Wallace, A. One thousand health-related quality-of-life estimates. Med Care. 38(6), 583–637. https://doi.org/10.1097/00005650-200006000-00004 (2000).
Sparring, V. et al. Diabetes duration and health-related quality of life in individuals with onset of diabetes in the age group 15–34 years—a Swedish population-based study using EQ-5D. BMC Public Health 22(13), 377. https://doi.org/10.1186/1471-2458-13-377 (2013).
National Sample Cohort data. National Health Insurance Sharing Service (NHISS). https://nhiss.nhis.or.kr/bd/ab/bdaba013eng.do.
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (MSIP) (No. NRF-2018R1D1A1A02046351). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
S.O. and J.M. conceived and conducted the experiments. S.L. and J.N. verified and advised the experimental outcome. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oh, SH., Lee, S.J., Noh, J. et al. Optimal treatment recommendations for diabetes patients using the Markov decision process along with the South Korean electronic health records. Sci Rep 11, 6920 (2021). https://doi.org/10.1038/s41598-021-86419-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-86419-4
This article is cited by
-
Data-driven meal events detection using blood glucose response patterns
BMC Medical Informatics and Decision Making (2023)
-
Diabetes medication recommendation system using patient similarity analytics
Scientific Reports (2022)
-
An interpretable RL framework for pre-deployment modeling in ICU hypotension management
npj Digital Medicine (2022)
-
Wearable chemical sensors for biomarker discovery in the omics era
Nature Reviews Chemistry (2022)
-
A Promising Approach to Optimizing Sequential Treatment Decisions for Depression: Markov Decision Process
PharmacoEconomics (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
