
Abstract
Centralized intravenous admixture service (CIVAS) centres, which are pharmaceutical departments found in Chinese hospitals, provide high-quality intravenous fluids and pharmaceutical services for patients, and errors in their working procedures can lead to adverse consequences. Pharmacists, the primary CIVAS centre personnel, play a role in risk control; however, to date, the effect of pharmacists’ participation in risk management has not been reported. The main aim of this study was to evaluate the pharmacist’s role in risk control and evaluate its impact. A retrospective observational study was designed to assess the principal working process in the CIVAS centre of a provincial healthcare setting. Errors in the main working process were identified, and intervention measures were formulated. The pharmacist intervention effect was evaluated by assessing the identification rate of improper prescriptions; the incidence rate of drug preparation, compounding, packaging and delivery process errors; and expenditures on wasteful drugs. There was a higher identification rate for improper prescriptions after the intervention (P < 0.05), while the incidence of drug preparation (P < 0.05), admixture (P < 0.05), and packaging and delivery errors (P < 0.01) was significantly lower; the total wasteful medication expenditure was also dramatically reduced. The potential creativity of pharmacists in error control can provide dependable intravenous drugs for patients and reduce the running expenditures for CIVAS.
Similar content being viewed by others


Introduction
In recent decades, advances in medical therapies have provided patients with more options than ever before; nevertheless, intravenous fluids are the primary clinical treatment due to their rapidity and effectiveness, especially in first aid medication and nutrition support. China, with its large population, consumes a large number of intravenous medicines every year1. Traditionally, intravenous fluids, including chemotherapy drugs, are compounded in an open environment in the ward, which may lead to contaminated intravenous fluids and the staff being exposed to toxic intravenous medication. Gradually, the Ministry of Health of China has become aware that hospital pharmacies serving hospitalized patients should routinely prepare specialized intravenous compounds in a sterile and centralized setting, and the United States Pharmacopeia (USP) Chapter <797> was consulted prior to the construction of centralized intravenous admixture service (CIVAS) centres2. Subsequently, the “Regulations on the Quality Management of Centralized Dispensing of Intravenous Drugs”, which provides a standardization for the establishment and administration of CIVAS centres, were enacted in 20103. Currently, it is estimated that more than 1000 CIVAS centres have been established in first- or second-class Chinese hospitals; these centres have developed into an emerging pharmaceutical industry and a subdiscipline in hospital pharmacy science1.
Generally, Chinese CIVAS centres are characterized as multi-procedure and labour intensive, which is consistent with the fact that a large number of intravenous fluids needs to be produced from prescriptions in a limited time and that operating expenditures must be controlled within a reasonable range. To obtain the intravenous finished product, the doctor’s prescription must go through several stages, including prescription review, drug preparation and compounding, packing and delivery. Unfortunately, the multiple processes and manual operations involved are error-prone and can result in adverse events because of the reliance on human performance4. Worst of all, one error may result in multiple subsequent severe events. For example, unqualified chemotherapeutic fluids have been made from improper drugs or dosages, and patients can exhibit side effects or die when this fluids are administered intravenously; even if the errors are discovered before the intravenous fluid injection, fluid re-preparation will certainly lead to extra drug consumption. In addition, drug container breakage caused by careless operation is a factor in additional drug expenditure increase. Some countries have reduced errors by introducing robotics into their CIVAS centres5. However, this focus on the prevention of errors in the drug admixture process is not a perfect solution because it targets only a single procedure rather than the multiple, successive working processes in Chinese CIVAS centres. Furthermore, it is difficult to calculate the labour and financial costs of running automatic machines because most of the preparation and cleaning jobs have to be performed manually6,7. To date, risks control have not yet been addressed by effective approaches in Chinese CIVAS centres.
Meanwhile, a new round of healthcare reforms aimed at curbing the excessive and rapid growth of patient costs in Chinese public hospitals began in 2017. The minimization of patients’ pharmaceutical expenditures is a top priority for policy intervention8,9. One measure of policy intervention is that all governmental hospitals have an obligation to eliminate drug mark-ups and sell drugs at their purchase price10. Pharmacists used to make a profit for hospitals by drug sales with mark-ups, but now they are no longer the hospital revenue creator following the implementation of this policy, as a result, the remuneration for current pharmacy staff is gradually becoming a great financial burden for hospitals, although China's labour force is relatively cheaper than that of most developed countries may be a reason the majority of CIVAS centres employ labour rather than automation. Salary for pharmacists has declined more common, and pharmacists may be laid off unless they show their abilities as an innovative value generator for the hospital. On the other hand, Chinese CIVAS centres also suffer from a paradoxical dilemma. Specifically, the utilization of multiple working processes poses a significant potential for errors, and additional staff are required to recheck drugs and operations, especially in the intravenous admixture preparation and labelling phase,. Furthermore, the work of CIVAS centres is not only tiring and tedious but also fallible, and technicians easily suffer from stress and anxiety. Extra pharmacy staff members are highly beneficial for alleviating the workload and providing risk control, but staff numbers are strictly limited by hospital costs savings. Therefore, pharmacist competence should be improved to optimize working procedures and decrease risk. This would increase their value and decrease the amount of extra labour required for error management. Therefore, we performed this study to evaluate the effects of pharmacist interventions on risk control in a CIVAS centre in Guangxi.
Methods
This study was approved by the Ethics Committee of People's Hospital of Guangxi Zhuang Autonomous Region (No. KY-ZC-2017-4). All methods were implemented in accordance with the Ethics Committees’ relevant guidelines and regulations. As this study analyzed job method data, patients did not participate in the study, and their consent was not deemed necessary by the Ethics Committee.
Study design
The study site was the CIVAS centre of a large treatment centre in Guangxi Province. The objectives of this study were threefold. First, we sought to identify errors and related causes in the original workflow of the CIVAS centre. Second, we aimed to obtain relevant measures formulated by pharmacists to address these problems. Third, we aimed to evaluate the impact of pharmacists on risk management within the main working procedure by implementation of measures. The main working procedures from January 2018 to December 2018 and from June 2019 to May 2020 were categorized as the control group and practical group, respectively. To ensure the homogeneity of the study, the same pharmacists participated in both periods, and the entire working procedure was recorded by webcam (SONY SSC-SD36P, Sony China limited, Beijing, China) and paper documents. The rate at which improper prescriptions were identified; the incidence of errors in drug preparation, admixture, packaging and delivery processes; and the expenditures of wasteful drugs were used as assessment indexes.
Main workflow of the control group
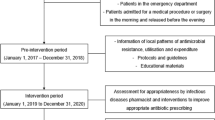
The workflow in our CIVAS centre is generally consistent with that of most Chinese CIVAS centres (Fig. 1). All pharmacists who are employed by the CIVAS centre have passed annual professional technique tests for their position.

Main working process of CIVAS centres.
Prescription review
Doctors’ prescriptions were transmitted to the CIVAS centre by a hospital information system, and pharmacists received prescriptions and charges for drugs. Then, the appropriateness of the prescriptions was automatically reviewed by prescription review software; unqualified prescriptions were rejected and sent back to the doctors’ system, while approved prescriptions were assigned to a batch according to the time at which the pharmacist processed the request (first batch: product delivery at 9:30 AM, second batch: product delivery at 12:00 AM, third batch: product delivery at 5:30 PM). Then, individual patient labels that included medication and batch information, as well as drug summary sheets, were printed.
Preprocessing step
Next, each pharmacist was assigned an equal number of patient labels and drug summary sheets, and they independently completed the following steps for these medications: all drugs were selected from the shelves following the summary sheets, the outer packages were removed, and each infusion bottle/bag was labelled with the patient’s individual information. The same drugs and their corresponding diluent were placed in the same crate. Crates colours were used to distinguish batches. Drug preparation was stopped when a prescription was cancelled due to the doctor or patient, and a full refund was permitted for prepared medicines (e.g., outer package removal, infusion bottle/bag with label) unless the medicine had been mixed with a diluent. Those prepared medicines defined as refunded drugs were put back on the shelf or assigned to other patients to whom they were prescribed. Pharmacists usually focus their attention on successive jobs; hardly anyone notices that refunded drugs have not yet been dealt with. Thus, it is important for medication in the warehouse to be well managed.
Admixing step
Cytotoxic fluids and parenteral nutrition fluids were produced respectively in the biosafety cabinet and laminar flow cabinet in a class 10,000 clean room. The stoppers of each drug and diluent vial/bottle that directly contacted a syringe needle were cleaned with 75% ethanol before the admixing operation. Then, each drug was mixed with the related diluent and injected into an infusion bottle/bag, after which time empty bag(s) or vial(s) were taken away and confirmed outside the clean room as part of the final verification. The workbenches, cabinets and staff gloves were cleaned with 75% ethanol following completion of the compound process of each bottle/bag. The above steps were performed independently by each pharmacist.
Packaging and delivery
A final check of quality and appearance was conducted by the pharmacist. Products that passed the final check were allocated to their wards by scanning the infusion bottle/bag label’s bar code and printing delivery sheets. If the rejected prescription was submitted insistently, the CIVAS centre rejected the mix of drug and diluent. The unmixed drug and label for intravenous fluids were still provided to the wards.
Identification of workflow RISK
Workflow risk was defined as errors that occurred at any step within the main working procedures where the prescription and its related drug were physically handled or manipulated by a healthcare professional and could result in physical injury to the patient, occupational injury to the staff or financial loss to the CIVAS centre. All deviations in the working process that were potentially hazardous to patients, such as deviations in the preparation or combination of drugs from the doctors’ prescriptions, deviations from the hospitals’ intravenous administration policy, or deviations from the manufacturers’ instructions, were also included in the definition of risk. It is worth noting that medications in incorrectly compounded batches were considered a risk because the deviation in administration of finished intravenous fluids at the prescribed drug administration time may result in drug instability or deferred patient treatment. There were no definite indexes with which to evaluate or measure errors due to inadequate aseptic techniques or potential cytotoxic medication leaks; thus, errors or potential errors from these factors were not included in this study. A research panel consisted of one chief pharmacist, one associate chief pharmacist, two pharmacists trained in standardized operations of cytotoxic and parenteral drugs, and two pharmacists with more than 10 years of experience in drug management. The chief pharmacist and associate chief pharmacists reviewed all video and paper records and identified risks or potential risks independently. Acquisition differences were resolved by reviewing the workflow from the video. The identification results were summarized in a table, and each panel member was required to participate in cause analysis. The details are summarized in Table 1.
Main workflow of the practical group
Specific countermeasures (Table 2) had been approved by the director of our CIVAS centre and then incorporated into the original working steps. Every step was signed by the operator, and the person who made an error can be tracked once a risk is discovered. A flexible group that aimed to address two issues was established: (1) heavy workload alleviation in admixing, packing, and delivery steps helped reduce fatigued-related errors, and (2) efficient product completion ensured that patients’ therapeutic plans were not delayed (its four members come from original staff rather than additional employment).
Drug management
Two permanent pharmacists were appointed to perform daily drug management each day. They were responsible for all aspects of medication monitoring, making sure that all medications were manufactured through consistent processes. Distinctive/alert boxes and various pattern label designs were an innovation of this task. Specifically, different coloured boxes (Fig. 2) were used to distinguish cytotoxic from non-cytotoxic drugs; labels (Fig. 3) with sticky material could be placed on shelves, refrigerators or other places to indicate their contents; and cytotoxic and other high-risk medications were placed on independent shelves for identification purposes.

(a) Cytotoxic drugs are stored in red boxes, (b) non- cytotoxic drugs are stored in blue boxes.

Warning sticker for (a) chemotherapeutical medications, (b) dark place storage drugs requiring dark storage, (c) drugs with similar external packaging drugs, (d) drugs with similar names, (e) drugs approached expiry approaching expiration date, (f) drugs with different contents, (g) drugs must store in refrigerator requiring refrigeration, (h) fragile medications. Assemblage of images was derived from version 9.6.45 of Hamrick VueScan (https://www.hamrick.com/).
Prescription review
During the prescription review process, the appropriateness and accuracy of drug employment were assessed by manually reviewing prescriptions that had been approved by the software. If inappropriate prescriptions were found in the review process, the pharmacists not only informed the prescribing physician immediately but also analysed them monthly; then, corresponding analysis results and modification suggestions were given to the physicians. Besides, the prescription submission time was limited to the day before the admixture stage for the purpose of achieving a sufficient handling time. They were received only in cases of urgent prescriptions that needed to be dealt with instantly after submission, and the case submission had to be performed within a certain time window (8:00–10:30 AM, 3:00–4:30 PM) even to have a chance of being accepted. It should be noted that the intelligent review software could not be upgraded automatically; thus, staff periodically renewed the automatic review software. The updated software included adding new legal medical evidence, such as that from drug manufacturers, and various treatment guidelines.
Preprocessing step
Pharmacists performed preparation tasks in teams of two members. One staff member selected medications, removed the outer packaging, and labelled the infusion bottle/bag, while a second person monitored and rechecked these operations. After drug review, this process continued with a “third” pharmacist performing a bottle/bag check, i.e., a check that the medication bottle/bag agreed with the patient’s label, as the first step towards ensuring that the correct medication had been selected. In addition, the pharmacists improved the readability of the patient labels by increasing the font size and marking key points. In terms of refunded drugs, the assigned pharmacists disposed of them to prevent them from being used for the original patients due to carelessness or busyness.
Admixing step
Consistency in medications and labelling were carefully examined in the cabinets before the start of an admixture. Then, a pharmacy technician filled a syringe with the required volume of drug needed for the dosage, and a second pharmacist checked the syringe before injecting it into a bag. The technician then injected the contents of the syringe under the observation of a second staff member, and the final product, along with the used vials and empty syringes, was checked by the second member. After this process, contaminated syringes and vials were disposed of in the biosafety cabinet, avoiding the risk of contaminating other areas of the clean room. An individual leak-proof package for each final cytotoxic product was introduced by the pharmacist. The flexibility group participating in this step helped provide products to the wards on time.
Packaging and delivery
The quality and appearance of final products, as well as delivery sheets, were examined by two pharmacists. When they struggled with a large volume of examination tasks, flexible shift staff shared the workload with them. The update scanning software that be enabled to provide an electronic reminder of missing printouts of scans and delivery orders was introduced by pharmacists. In addition, pharmacists conducted a monthly survey of intravenous fluid usage in the wards, which provided feedback for product improvement.
Statistical analysis
Categorical variables between the two groups were analysed by the chi-square test. Differences in numerical variables between the two groups were analysed by the independent samples T test. P < 0.05 was considered significant. All tests were conducted with SPSS 22.0 software (https://www.ibm.com/cn-zh).
Ethics approval
This study was approved by the Ethics Committee of People's Hospital of Guangxi Zhuang Autonomous Region (No. KY-ZC-2017-4).
Consent to publish
The publication has been approved by all co-authors.
Results
Identification rate of improper prescriptions
Pharmacists rechecked the prescriptions that had been approved by review software, revealing a higher rate of identifying improper prescriptions in the practical group (1%) than in the control group (0.24%) (P < 0.05, Table 3).
Incidence of preprocessing errors
The actual number of prepared drugs was lower in both groups because of cancelled prescriptions and refunded drugs. Error incidence rates were lower in the practical group (0.22%) than in the control group (0.57%) (P < 0.05, Table 4) after intervention with corresponding measures.
Incidence of errors in the admixing process
The number of medications in the admixing process was less than that in the preprocessing phase due to instant prescription cancellations and drug refunds. In this process, the results indicated that the error incidence in the practical group (0.07%) was lower than that in the control group (0.64%) (P < 0.05, Table 5).
Incidence of errors in packaging and delivery
After the measures for the packing and delivery process were implemented by technicians, the error rate in the practical group (0.14%) was significantly lower than that in the control group (0.79%) (P < 0.01, Table 6).
Wasteful drug expenditures
Compared with the cost of wasted drugs before the intervention, the value after the intervention decreased dramatically (P < 0.05, Table 7). Following the pharmacists’ involvement, the total cost of wasted drugs decreased from ¥52,112.20 to ¥9,865.80.
Discussion
CIVAS is an approach that reduces risks and errors related to the preparation and administration of injectable drugs and protects staff from hazardous drug exposure, according to previous literature11,12. Although the error rate was not too high in the control group, which may be attributed to the technicians’ good training and responsibility, a basic competency for each staff member in the CIVAS centre, it was still necessary to strictly control the incidence of procedure errors, which are not only the cause of serious adverse consequences for patients, such as therapeutic failure, physical impairment, and death, but also the trigger of toxic pollution and financial loss at CIVAS centres. The pharmacist-oriented practice outlined here provides an opportunity to control those working procedure risks for patients, the CIVAS centre and its technicians. The incorporation of this practice during regular working procedures allowed its easy implementation in our CIVAS centre.
The implementation of this practice achieved a notable degree of effectiveness from the start, largely due to permanent administrators who were assigned to conduct these tasks. These technicians are familiar with medical examination and inventory management, which resulted in the attainment of several goals: unqualified products were recognized from a large number of drugs before achieving CIVAS centre acceptance, and monthly drug consumption and purchase were estimated accurately to avoid shortages or overstock.
In the control group, selection errors and item return mix-ups were likely because of the close proximity of stored medications with similar names and appearances (e.g., epirubicin and doxorubicin, different medium- and long-chain fat emulsions), the same medications with different specifications (e.g., 10 mg and 50 mg nedaplatin), or the same medications from different manufacturers (oxaliplatin from Sanofi-Aventis, France and Jiangsu Hengrui, China). These issues were resolved through the use of alert labels and different colour storage boxes as well as being placed on separate shelves in the practical group. Furthermore, assigning specific staff to handle refunded drugs helps separate them from the consecutively prepared medications and prevents them from being reassigned to the original patients.
Whereas a fully automated software is able to store manufacturer instructions and medical database information as well as automatic identify improper prescriptions, prescriptions approved by the software still have to be handled manually. It is impractical for software information systems to automatically upgrade to the latest medical knowledge, view prescriptions associated with the patient's laboratory tests, collect imaging and pathological results, or judge certain improper cases. Pharmacists aim to improve such situations through their roles in collecting state-of-the-art medication data, including guidelines, manufacturer instructions, and databases; rebuilding software information systems; taking patients’ examination results into account while reviewing prescriptions; and making decisions regarding special prescriptions based on their expertise. As our practice has shown that manual prescription viewing tasks are extremely time consuming despite being performed by experienced technicians and are highly dependent on the pharmacist’s professional level, we are confident that we could complete this task by curbing the submission of prescriptions made one day prior to the drug admixture, with the exception of certain emergency cases involving chemotherapy regimen adjustments or medications needed for emergency care, to provide sufficient time for review. Hence the increase in identifying improper prescriptions is likely attributed to prescription review software upgrades and appropriate prescription submission times.
The medication preparation and mixture process is the step that is most prone to error, and previous data have revealed that errors are greatly affected by medication administration, the use of robotic drug hybrid devices, and staff training6,7,13. Even if our early drug management practices reduce errors in the subsequent work procedure, electronic medication storage and inventory systems are a better complement to manual error intervention14. Unfortunately, most hospitals may be reluctant to invest large sums of money into electronic devices because 70.1% of the 137 CIVAS centres in China operate at a loss3. Consequently, we adopted a practical method in which the preprocessing and admixing of each bottle/bag of intravenous drug is strictly controlled by two pharmacists for accuracy (process cross-checks and signature label confirmation). If any human error occurred during these or subsequent working procedures, the signature could be traced back to whoever made the error. In addition, the original method for training pharmacists on optimal mixture protocols and standardization continued. In the practical group results, the lower error rate in the preparation and mixture processes may be attributed to the effectiveness of these approaches. The expenditures associated with drug waste in the practical group were lower than those in the control group. We assume that the prevention of workflow errors, such as medication container breakage and incorrect admixing procedures, reduced the quantity of wasted drugs and decreased expenditures and running costs directly15,16,17. In addition, the prevention of medication container breakage, especially for cytotoxic drugs, significantly reduced the occupational exposure of staff. Finally, higher quality and more accurate intravenous fluids were transported to the correct wards in the practical group than in the control group, suggesting the improved effect of pharmacist participation in rechecking the quality of the product and the delivery sheets.
If the same group pharmacists participated in both the control and practical groups, why were their working efficiencies and results so different? There are three possible reasons for this discrepancy. First, the traditional working procedure in the CIVAS centre lacked an effective management approach, which not only posed challenges to risk control but also resulted in a failure to appreciate and exploit the pharmacists’ abilities. Second, the pharmacists in the practical group played a role in optimizing their work steps according to correct management techniques, and the results of their involvement were welcomed by physicians, nurses, and patients, which enabled them to experience a sense of individual importance and value. The sense of achievement, and stress from healthcare reforms thus encouraged the pharmacists to create advanced working methods. Third, staff in flexible group not only are capable of relieving fatigue-triggered errors but also enable intravenous products to be completed in the required time.
This practice was created and conducted by pharmacists focused on the development of their professional skills and may not be applicable to nurse-based CIVAS centres. However, other CIVAS centres may be able to achieve similar effects by modifying these procedures.
Conclusion
A pharmacist-focused practice during working procedures increased the improper prescription identification rate and reduced the incidence of errors in drug preprocessing, admixing, packaging, and delivery processes. This study provides practical information for CIVAS centres in most Chinese hospitals.
Data availability
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided appropriate credit is given to the original author(s) and the source, a link to the Creative Commons license is provided, and any changes are indicated.
References
Mi, W. et al. Chinese centralised intravenous admixture service (CIVAS), an emerging pharmaceutical industry: Survey of the recent advances of CIVAS in China. Eur. J. Hosp. Pharm. 25, 165–168 (2018).
American Society of Health System Pharmacists. ASHP guidelines on compounding sterile preparations. Am. J. Health Syst. Pharm. 71, 145–166 (2014).
Yang, C., Kang, B. Y., Zhang, L. & Yu, D. Construction situation, costs and charges associated with pharmacy intravenous admixture services: Multi-center cross-sectional survey based on 137 medical institutions in mainland China. BMC Health Serv. Res. 20, 577 (2020).
Escrivá Gracia, J., Brage Serrano, R. & Fernández, G. J. Medication errors and drug knowledge gaps among critical-care nurses: A mixed multi-method study. BMC Health Serv. Res. 19, 640 (2019).
Iwamoto, T. et al. Performance evaluation of the compounding robot, APOTECAchemo, for injectable anticancer drugs in a Japanese hospital. J. Pharm. Health Care Sci. 3, 12 (2017).
Parrish, R. H. 2nd. et al. Minimizing medication errors from electronic prescription transmission-digitizing compounded drug preparations. Pharmacy (Basel). 7, 149 (2019).
Schoening, T. et al. Semiautomated aseptic preparation of patient-individual antineoplastic intravenous solutions: First experiences in a German hospital pharmacy. Eur. J. Hosp. Pharm. 23, 44–49 (2016).
Penm, J. et al. The impact of clinical pharmacy services in China on the quality use of medicines: A systematic review in context of China’s current healthcare reform. Health Policy Plan. 29, 849–872 (2014).
Meng, Q. et al. The impact of China’s retail drug price control policy on hospital expenditures: A case study in two Shandong hospitals. Health Policy Plan. 20, 185–196 (2005).
Tang, W. et al. Effects on the medical revenue of comprehensive pricing reform in Chinese urban public hospitals after removing drug markups: Case of Nanjing. J. Med. Econ. 21, 326–339 (2018).
Hecq, J. D. Centralized intravenous additive services (CIVAS): The state of the art in 2010. Ann. Pharm Fr. 69, 30–37 (2011).
da Conceição, A. V. et al. Oncology pharmacy units: A safety policy for handling hazardous drugs and related waste in low- and middle-income African countries-Angolan experience. Ecancermedicalscience. 9, 575 (2015).
Sutherland, A. et al. Incidence and prevalence of intravenous medication errors in the UK: A systematic review. Eur. J. Hosp. Pharm. 27, 3–8 (2020).
Oldland, A. R., Golightly, L. K., May, S. K., Barber, G. R. & Stolpman, N. M. Electronic inventory systems and barcode technology: Impact on pharmacy technical accuracy and error liability. Hosp. Pharm. 50, 34–41 (2015).
Fasola, G. et al. Drug waste minimisation and cost-containment in Medical Oncology: Two-year results of a feasibility study. BMC Health Serv. Res. 8, 70 (2008).
Ranchon, F. et al. Chemotherapeutic errors in hospitalised cancer patients: Attributable damage and extra costs. BMC Cancer 11, 478 (2011).
Hedlund, N., Beer, I., Hoppe-Tichy, T. & Trbovich, P. Systematic evidence review of rates and burden of harm of intravenous admixture drug preparation errors in healthcare settings. BMJ Open. 7, e015912 (2017).
Acknowledgements
The authors acknowledge the financial support from the Guangxi Zhuang Region Health Department (Award No. Z20170382) and Scientific Research and Technology Development Program of Guangxi (Award No. 15277005) for performing the study.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: H.C. and Y.G.; collected the data: Y.G.; analysed the data: H.W. and X.C.; drafted the manuscript: H.C.; commented on the draft of the manuscript: all authors; read and approved the final version of the manuscript: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, H., Guo, Y., Wei, H. et al. The impact of pharmacist oriented mode on risk control in a Chinese centralized intravenous admixture service centre. Sci Rep 11, 5445 (2021). https://doi.org/10.1038/s41598-021-85077-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-85077-w
This article is cited by
-
Development of regional pharmacy intravenous admixture services data reporting and analysis platform for enhanced quality control ability
BMC Health Services Research (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
