
Abstract
This study aimed to determine the factors related to intraoperative extension gap (EG) in patients who underwent posterior-stabilized total knee arthroplasty (TKA). A total of 106 TKAs in 84 patients were retrospectively reviewed. Only patients who underwent the same method of bone resection were included consecutively. Bilateral popliteal angle (BPA) was used as an indicator of hamstring tightness. EG and extension space angle were measured using an offset type tensor. The associations between patient variables and EG were analyzed using multivariable linear regression and Pearson's correlation coefficients. The average EG was 12.9 ± 2.1 mm, and the average extension space angle was 2.8° ± 3.2°. BPA was greater than flexion contracture in most cases (94.3%), and no difference was found in only six cases (5.7%). According to multivariable linear regression analysis which was conducted after modifying the BPA into a categorical variable by 5°, EG was correlated with BPA (p < 0.001). Pearson’s correlation coefficient between EG and BPA was − 0.674 (p < 0.001). No other factors were significantly correlated with intraoperative EG. The present study found that popliteal angle is a different entity from flexion contracture, and that it is a predictable factor for EG in osteoarthritis patients. Smaller BPAs led to larger EG in patients who underwent the same degree of bone resection.
Similar content being viewed by others
Introduction
The size of proper extension gap (EG) and balance with the flexion gap are essential for achieving successful clinical outcomes in total knee arthroplasty (TKA)1. However, unexpected large EG can occur, even if the surgery is performed in the same way. The EG comprises the distance between distal femur and proximal tibia, as well as the laxity of soft tissue, including collateral ligaments and posterior structures of the knee. Since bone resection level can be controlled by the surgeon, unexpected gap differences between patients mainly occur due to the soft tissue laxity. When the knee joint is extended in the posterior stabilized TKA setting, cruciate ligaments are resected and the extensor mechanism is loose, leading the posterior structures of the knee and collateral ligaments to mainly affect the soft tissue laxity and the EG.
The anatomy of the posterior knee consists of a complicated network of dynamic and static stabilizers. Among them, the posterior semimembranosus complex was described as one of the major anatomical structures in the posterior aspect of the knee, according to LaPrade et al.2. Moreover, many studies have reported releasing hamstring musculature as a technique for adjusting the EG3,4. Taken together, it can be considered that the hamstring musculature is one of the major structures that could affect soft tissue laxity around the extended knee. If the hamstring tightness, which reflects the laxity of posterior structures of the knee, can be predicted in advance, the EG can be expected, and additional procedures or unnecessary bone resection can be avoided. However, to the best of our knowledge, the method for predicting the hamstring tightness and EG in elderly patients undergoing TKA is not yet known5. Base on this idea, we hypothesized that the EG can be predicted by measuring the hamstring tightness in elderly patients undergoing TKA. Therefore, the aim of this study was to determine whether factors such as hamstring tightness were related to intraoperative extension gap in patients who underwent the same amount of bone resection.
Materials and methods
Patient recruitment
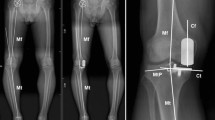
After receiving the approval from our Institutional Review Board, we retrospectively reviewed 186 knees of 121 patients who underwent primary TKA for degenerative osteoarthritis consecutively. Since the purpose of this study was to analyze the effect of soft tissue on the gap, only patients who underwent the same method of bone resection were included. The same method of bone resection was defined as follows: (1) distal femur resection was performed perpendicular to the femoral mechanical axis and at a distance of 9 mm from the most distal femoral condyle (mainly medial femoral condyle); and (2) proximal tibial resection was performed perpendicular to the tibial mechanical axis and at a distance of 8 mm from the most proximal tibial plateau (mainly lateral tibial condyle) (Fig. 1A). Exclusion criteria were as follows: (1) patients who did not undergo physical examinations or image studies; (2) patients who had a history of previous unicompartmental knee arthroplasty, high tibial osteotomy (HTO), infection, trauma, or rheumatoid arthritis; (3) patients who had a history of spinal fusion; (4) patients with bone defects in medial femoral condyle and lateral tibial condyle that cannot be used as a reference; (5) patients with motor weakness of lower extremity; and (6) patients who did not have bone resection, as mentioned above. A total of 80 TKAs were excluded for various reasons; and finally, a total of 106 TKAs of 84 patients were enrolled in this study (Fig. 1B). Demographic data and radiographic parameters are shown in Table 1.

(A) The method of bone resection of patients enrolled in this study. (B) Flowchart of patient inclusion.
Popliteal angles and generalized joint laxity
Popliteal angles, range of motion (ROM), and generalized joint laxity of each patient were routinely measured to evaluate the soft tissue laxity. The flexion contracture measurements were made using a digital goniometer with reference to the lateral femoral epicondyle, greater trochanter, and lateral malleolus with the passively extended knee in the supine position of the patient. Popliteal angles are generally used to identify hamstring tightness in pediatric patients with cerebral palsy6,7. Popliteal angle was defined as the acute angle between tibia and femur when the knee joint was passively extended with the hip flexed 90 degrees. Unilateral popliteal angle (UPA) was measured with the contralateral hips and knees extended, indicating functional hamstring tightness (Fig. 2A). Bilateral popliteal angle (BPA) was measured with the contralateral hips and knees flexed to neutralize the anterior pelvic tilt, indicating true hamstring tightness (Fig. 2B). Among the two popliteal angles, Thomson et al. reported that the BPA neutralizing anterior pelvic tilting was an indicator of semimembranosus8. For this reason, our study used BPA as an indicator of hamstring tightness and excluded patients who had a history of spinal fusion, as there may be limitations of neutralization of pelvic tilt. Measurements were made with a digital goniometer similar to the flexion contracture measurements. Since the origin of hamstring muscles is located in the posterior-inferior aspect relative to the hip joint, hip joint flexion makes hamstrings tighter than extension; as a result, UPA is always larger than BPA.

Popliteal angle was defined as the angle between the femoral extended line and tibia. (A) UPA was measured with the contralateral hips and knees extended. (B) BPA was measured with the contralateral hips and knees flexed to neutralize the anterior pelvic tilt.
The generalized joint laxity was also evaluated using the Beighton and Horan criteria9, which are widely used in the field of sports medicine. The Beighton and Horan criteria are as follows: (1) hyperextension of the little finger (5th digit) beyond 90°, (2) passive apposition of the thumb to the flexor aspect of the forearm, (3) hyperextension of the elbow beyond 10°, (4) hyperextension of the knee beyond 10°, and (5) forward flexion of the trunk so that the palms of the hands rest easily upon the floor. Items 1–4 are scored as either 1 or 0 for each side, right and left. The fifth item is scored as either 1 or 0. The total sum is the final score, ranging from 0 to 9. Generalized joint laxity is defined as a score ≥ 4 points. Higher scores indicate higher degrees of joint laxity. In the present study, none of the patients satisfied the fourth item due to arthritic flexion contracture.
Gap measurement
An offset type tensor was used in this study to measure the distance and angle between the resected bone planes. The offset type tensor FuZion (Zimmer Biomet, Warsaw, IN) makes it easy to measure the EG and extension space angle without the use of a navigation system. This device consists of three parts: femoral assembly, tibial assembly, and femoral paddle (Fig. 3A). The distance between the center of the femoral paddle and tibial assembly is the EG, and the angle between the two parts is the extension space angle. The EG is equal to the mean of the medial compartment gap (MCG) and the lateral compartment gap (LCG) (Fig. 3B). The offset type tensor was placed between the resection plane of distal femur and proximal tibia. Since the measurements could vary depending on the position of the offset type tensor, the anterior border of proximal tibia and tibial tuberosity were used as reference to obtain a constant position. Then, the EG was measured with patella reduction and temporary joint closure with towel clips. In the present study, joint distraction force was 40 lbf with toque driver.

(A) Offset type tensor. (B) EG was defined as the distance between each center of tibial assembly and femoral paddle with distraction by the torque driver; and it was equal to the average value of LCG and MCG.
Surgical procedure
All patients underwent posterior stabilized TKA through the midvastus approach by one experienced surgeon (WSL) using the Persona Knee System (Zimmer Biomet, Warsaw, IN). All surgeries used the technique of mechanical alignment in TKA. After the removal of anterior cruciate ligament and posterior cruciate ligament, 9-mm resection of distal femur was performed perpendicular to the femoral mechanical axis using intramedullary guide. Since there was no varus femoral anatomy in this study, all distal femoral bone resection had been made from the medial femoral condyle. Then, proximal tibial resection was performed perpendicular to the tibial mechanical axis and with 3° of posterior slope at a distance of 8 mm from the least involved tibial condyle. In most patients, there were various forms of bone defects in medial tibial condyle, which made it difficult to set a consistent resection level from the medial tibial condyle. Therefore, tibial resection was performed based on lateral tibial condyle, and only the patients on which it was performed were enrolled in this study. The resection thickness of distal femur (9 mm) and proximal tibial (8 mm) did not include cartilage thickness. Afterward, EG and extension space angle were measured using the offset type tensor. At this time, only meniscectomy and deep medial collateral ligament release were performed, while other soft tissues that could affect the gap were not manipulated.
Radiographic parameters
The Kellgren-Lawrence grade was evaluated using true anterior–posterior standing radiographs of the knee. The medial proximal tibial angles (MPTA) were evaluated by preoperative scanograms. As knee flexion compensates for the spinal sagittal imbalance10, we evaluated the pelvic parameters in elderly patients that might affect the tissue contracture around the knee. EOS imaging system11 was used to measure the pelvic parameters (pelvic incidence, sacral slope, and pelvic tilt) and hip-knee-ankle angle (HKA). Posterior slopes and tibial component coronal angle to anatomical axis were measured from postoperative radiographs for the evaluation of tibial bone resection.
Statistical analysis
The associations between patient variables and EG were analyzed using multivariable linear regression and Pearson's correlation coefficients. The intra- and inter-observer reliability of measurements were assessed using intra-class correlation coefficients. Statistical analysis was performed using SPSS software for Windows (version 25.0; IBM Corp., Armonk, NY). The level of significance was set as p-value < 0.05. The statistical software G*Power (version 3.1.9.4; Heinrich Heine Universität Düsseldorf, DE) was used to calculate statistical power12. An effect size for statistical power calculation was obtained from the result of a linear regression analysis in a pilot study that included 40 subjects. Using α of 0.05 and the sample size of this study, the calculated statistical power was 0.99.
Ethical approval
This retrospective study was approved by the Gangnam Severance Hospital Institutional Review Board (IRB # 3-2019-0228) and all methods were performed in accordance with the guidelines and regulations of Gangnam Severance Hospital IRB. A wavier of consent was obtained by Gangnam Severance Hospital IRB for retrospective collection and analysis for deidentified demographic and medical data.
Results
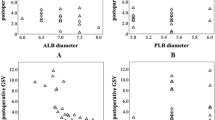
The average EG was 12.9 ± 2.1 mm, and the average extension space angle was 2.8° ± 3.2° (Table 2). BPA was greater than flexion contracture in most cases (94.3%), and no difference was found in only six cases (5.7%) (Fig. 4A). According to multivariable linear regression analysis which was conducted after modifying the BPA into a categorical variable by 5° (Fig. 4B), EG was correlated with BPA without variance inflation factor issue (p < 0.001) (Table 3). Pearson’s correlation coefficient between EG and BPA was − 0.674 (p < 0.001) (Fig. 4C). No other factors were significantly correlated with intraoperative EG.

(A) Histogram for differences between BPA and flexion contracture angle (FCA). (B) Histogram for BPA divided into 7 categories by 5°. (C) Scatterplots of the correlation between EG and BPA (r = − 0.674, p < 0.001).
Intra- and inter-observer reliability for the variables were as follows: 0.940–0.943 and 0.937–0.942 for ROM, 0.974 and 0.964 for BPAs, 0.901 and 0.850 for posterior slopes, 0.977 and 0.893 for tibial component coronal angle, 0.931 and 0.937 for MPTA at the 95% confidence interval, respectively.
Discussion
The present study identified that BPA reflecting hamstring tightness was related to EG. The tighter the hamstring muscles, the smaller the EG. In addition, it was suggested that popliteal angle has its own meaning in the adult group without neuromuscular disease.
Flexion contracture is caused by a combination of bone impingement and soft tissue contracture13,14. Popliteal angle is similar with flexion contracture in view of the limitation of the knee joint extension, but the proportions affected by bone impingement and soft tissue contracture are different. If there is an osteophyte that induces flexion contracture in the posterior femoral condyle, the degree of soft tissue tenting is affected not only by the size of the osteophyte15, but also by the knee flexion angle. As the knee flexion angle is increased, posterior structures and their insertion sites move further backwards than the osteophyte16, so the effect of osteophyte decreases. Therefore, it can be considered that BPA, whose extension is restricted at an angle greater than flexion contracture angle, is less affected by osteophyte. According to Moon et al., the average flexion contracture was 1.0 (-0.1 to 2.5) and the average BPA was 24.6 degrees (18.7 to 30.3) in normal people aged 13–50 without OA6. The BPA value of this study was greater than that of the OA patient group in our study. If osteophyte had a greater effect on BPA, it would be more likely to have a greater BPA value in the OA group. Taken together, it can be concluded that the soft tissue laxity due to the distraction of the offset type tensor would have a greater correlation with BPA than with flexion contracture, and our multivariable linear regression results support this.
Anatomical structures of the posterior aspect of the knee resisted hyperextension and distraction force (gap measurement). Among these structures, the oblique popliteal ligament (OPL) was the most important structure to resist knee hyperextension biomechanically17. LaPrade et al. described OPL as one of eight distal attachments of the semimembranosus tendon and the largest structure over the posterior aspect of the knee2. Then, Thomson et al. reported that BPA is an indicator of short medial hamstrings (semimembranosus)8. In conclusion, BPA reflects the tightness of posterior semimembranosus complex, including its distal attachment OPL, and it seems to affect the EG.
The size of the EG itself, as well as the balance between extension and flexion gaps, are important in TKA. If the EG is too small, more bone resection is required, and this is not technically difficult18,19. However, if it is too large, thick bearings may be needed to avoid instability or recurvatum, and as such, surgeons should be more cautious about performing this procedure. According to Greco et al., the use of thick bearings equal to or larger than 16 mm does not have a higher failure rate compared to thin bearings20. However, large gaps with unnecessary bone resection may induce negative results. Adding distal femoral resection can result in joint line elevation21, and adding proximal tibial resection can lead to increased strain on the tibia22. In addition, it is necessary to minimize unnecessary bone resection, even in view of the possibility of future revisions23.
The Beighton and Horan criteria reflecting generalized joint laxity, which is also known to reflect the soft tissue laxity and joint hypermobility of the whole body, did not appear to affect the EG in elderly patients. Kwon et al. reported that two groups divided by generalized joint laxity showed difference in insert thickness24, but the choice of insert could be affected by the surgeon’s intentions, and this was not reproduced in this study. Unlike young patients, joint mobility of elderly patients is disrupted by joint degeneration and osteophyte apart from soft tissue laxity. To evaluate the generalized joint laxity, hyperextension of the knee joint should be measured. However, as most elderly patients with knee osteoarthritis tend to have flexion contracture, it is impossible to measure knee hyperextension. Instead, since popliteal angle is mostly measured before reaching the flexion contracture angle, it is advantageous to measure the soft tissue laxity around the knee joint in elderly patients.
This study had some limitations. First, there was a lack of previous studies on the significance of popliteal angle in adult patients. We tried to prove that the popliteal angle is an independent entity from flexion contracture in normal adults, but further study would be needed. Second, the results of this study may not be applied quantitatively, due to the differences in surgical methods and instruments used by different surgeons. However, this study is valuable in that it provides a rough trend of the EG in advance using a simple examination. Third, it was impossible to conduct a separate evaluation of collateral ligaments affecting the EG through physical examination alone. However, collateral ligaments are also stretched out by distractions like in the posterior structures25, so BPA seems to reflect not only the laxity of hamstring, but also the generalized soft tissue laxity around the knee. Just as the Beighton and Horan criteria is considered to reflect generalized joint laxity in the sports medicine field, hamstring tightness can reflect the soft tissue laxity around the knee including collateral ligaments in OA patients who cannot be applied the Beighton and Horan criteria, and statistical results of our study support this. Nevertheless, this study is still meaningful as it is the first to identify the relationship between hamstring tightness and extension gap. Moreover, it is the first to demonstrate that popliteal angle can be used as a method to measure hamstring tightness. Since BPA is a non-invasive and simple method, TKA surgeons would have no difficulty in applying this method for evaluation. Therefore, if BPA is performed preoperatively, it could be very helpful for both the surgery and the patient's prognosis, with only little effort.
Conclusion
The present study found that popliteal angle is a different entity from flexion contracture, and that it is a predictable factor for EG in osteoarthritis patients. Smaller BPAs lead to larger EG among patients who underwent the same degree of bone resection. This finding would allow surgeons to predict the approximate soft tissue laxity and reduce unnecessary bone resection, thereby making it possible to determine an adequate EG.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Bottros, J., Gad, B., Krebs, V. & Barsoum, W. K. Gap balancing in total knee arthroplasty. J Arthroplasty 21, 11–15 (2006).
LaPrade, R. F., Morgan, P. M., Wentorf, F. A., Johansen, S. & Engebretsen, L. The anatomy of the posterior aspect of the knee. An anatomic study. J Bone Jt. Surg Am 89, 758–764 (2007).
Koh, H. S. & In, Y. Semimembranosus release as the second step of soft tissue balancing in varus total knee arthroplasty. J. Arthroplasty 28, 273–278 (2013).
Peters, C. L., Mohr, R. A. & Bachus, K. N. Primary total knee arthroplasty in the valgus knee: Creating a balanced soft tissue envelope. J. Arthroplasty 16, 721–729 (2001).
Kappel, A., Laursen, M., Nielsen, P. T. & Odgaard, A. Relationship between outcome scores and knee laxity following total knee arthroplasty: A systematic review. Acta Orthop. 90, 46–52 (2019).
Moon, S. J. et al. Normative values of physical examinations commonly used for cerebral palsy. Yonsei Med. J. 58, 1170–1176 (2017).
Katz, K., Rosenthal, A. & Yosipovitch, Z. Normal ranges of popliteal angle in children. J. Pediatr. Orthop. 12, 229–231 (1992).
Thompson, N. S., Baker, R. J., Cosgrove, A. P., Saunders, J. L. & Taylor, T. C. Relevance of the popliteal angle to hamstring length in cerebral palsy crouch gait. J. Pediatr. Orthop. 21, 383–387 (2001).
Beighton, P. & Horan, F. Orthopaedic aspects of the Ehlers-Danlos syndrome. J. Bone Jt. Surg. Br. 51, 444–453 (1969).
Obeid, I. et al. Global analysis of sagittal spinal alignment in major deformities: Correlation between lack of lumbar lordosis and flexion of the knee. Eur. Spine J. 20(Suppl 5), 681–685 (2011).
Demzik, A. L. et al. Inter-rater and intra-rater repeatability and reliability of EOS 3-dimensional imaging analysis software. J. Arthroplasty 31, 1091–1095 (2016).
Faul, F., Erdfelder, E., Lang, A. G. & Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191 (2007).
Bellemans, J., Vandenneucker, H., Victor, J. & Vanlauwe, J. Flexion contracture in total knee arthroplasty. Clin. Orthop. Relat. Res. 452, 78–82 (2006).
Scuderi, G. R. & Kochhar, T. Management of flexion contracture in total knee arthroplasty. J. Arthroplasty 22, 20–24 (2007).
Leie, M. A. et al. Large osteophyte removal from the posterior femoral condyle significantly improves extension at the time of surgery in a total knee arthroplasty. J. Orthop. 19, 76–83 (2020).
Choi, C. H. et al. Adequate protection rather than knee flexion prevents popliteal vascular injury during high tibial osteotomy: Analysis of three-dimensional knee models in relation to knee flexion and osteotomy techniques. Knee Surg. Sports Traumatol. Arthrosc. 28, 1425–1435 (2020).
Morgan, P. M., LaPrade, R. F., Wentorf, F. A., Cook, J. W. & Bianco, A. The role of the oblique popliteal ligament and other structures in preventing knee hyperextension. Am. J. Sports Med. 38, 550–557 (2010).
Mihalko, W. M. & Whiteside, L. A. Bone resection and ligament treatment for flexion contracture in knee arthroplasty. Clin. Orthop. Relat. Res. 141–147 (2003).
Athwal, K. K., Milner, P. E., Bellier, G. & Amis, A. A. Posterior capsular release is a biomechanically safe procedure to perform in total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 27, 1587–1594 (2019).
Greco, N. J., Crawford, D. A., Berend, K. R., Adams, J. B. & Lombardi, A. V. Jr. “Thicker” polyethylene bearings are not associated with higher failure rates in primary total knee arthroplasty. J. Arthroplasty 33, 2810–2814 (2018).
van Lieshout, W. A. M. et al. The negative effect of joint line elevation after total knee arthroplasty on outcome. Knee Surg. Sports Traumatol. Arthrosc. 27, 1477–1486 (2019).
Berend, M. E., Small, S. R., Ritter, M. A. & Buckley, C. A. The effects of bone resection depth and malalignment on strain in the proximal tibia after total knee arthroplasty. J. Arthroplasty 25, 314–318 (2010).
Schnurr, C., Csecsei, G., Nessler, J., Eysel, P. & Konig, D. P. How much tibial resection is required in total knee arthroplasty?. Int. Orthop. 35, 989–994 (2011).
Kwon, S. K., Kwon, H. M., Kong, Y. & Park, K. K. The impact of generalized joint laxity on clinical outcomes of total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 25, 3360–3365 (2017).
Nagai, K. et al. The influence of joint distraction force on the soft-tissue balance using modified gap-balancing technique in posterior-stabilized total knee arthroplasty. J. Arthroplasty 32, 2995–2999 (2017).
Acknowledgements
The authors would like to thank MID (Medical Illustration & Design) for helping to design the figures.
Author information
Authors and Affiliations
Contributions
B.W.C.: Formal analysis, Writing—original draft. I.H.Y.: Methodology. W.S.L.: Validation. B.W.C. and H.M.K.: Data curation, Resources. K.Y.L.: Data curation. W.S.L. and K.K.P.: Supervision, Writing—review and editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cho, B.W., Kwon, H.M., Lee, K.Y. et al. The effect of hamstring tightness on intraoperative extension gap in posterior stabilized total knee arthroplasty. Sci Rep 11, 3655 (2021). https://doi.org/10.1038/s41598-021-83221-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-83221-0
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
