
Abstract
Several studies have evaluated the association between serum adiponectin levels and knee and hand osteoarthritis (OA); mixed results have been reported. We investigated the relationship between OA and serum adiponectin levels according to the radiographic features of knee and hand OA. A total of 2402 subjects was recruited from the Dong-gu Study. Baseline characteristics were collected via a questionnaire, and X-rays of knee and hand joints were scored using a semi-quantitative grading system. The relationship between serum adiponectin levels and radiographic severity was evaluated by linear and logistic regression analysis. Subjects in the higher serum adiponectin levels tertiles were older and had a lower body mass index (BMI) than those in the lower tertiles. Regarding knee joint scores, serum adiponectin levels was positively associated with the total (P < 0.001), osteophyte (P = 0.003), and joint space narrowing (JSN) scores (P < 0.001) after adjustment for age, sex, BMI, smoking, alcohol consumption, education, and physical activity. In terms of hand joint scores, no association was found between serum adiponectin levels and the total, osteophyte, JSN, subchondral cyst, sclerosis, erosion, or malalignment score after the above-mentioned adjustments. Similarly, subjects with serum adiponectin levels above the median had higher total radiographic scores in the knee joints, but not in the hand joints, after adjustment. An increased serum adiponectin levels was associated with a higher radiographic score in the knee joint, but not in the hand joint, suggesting the involvement of different pathophysiologic mechanisms in the development of OA between those joints.
Similar content being viewed by others


Introduction
Osteoarthritis (OA) is the most common form of arthritis, affecting the knees, hips, and hands in the appendicular joints1. OA is characterized by progressive cartilage degradation, bone remodeling, osteophyte formation, and synovial inflammation, which lead to pain, stiffness, swelling, and disability. Although the risk factors for the occurrence and progression of OA differ on the basis of the joints involved, obesity, age, sex, physical activity, previous injury, and genetic factors are implicated in its development and progression in all joints2. Obesity is the most important risk factor because it not only plays a mechanical role by increasing joint load, but also metabolic and inflammatory roles as a result of the secretion by adipose tissue of proinflammatory factors, such as adipokines, cytokines, and chemokines3.
Adipokines are soluble factors that predominantly originate from adipocytes and are associated with obesity-related inflammation. Adiponectin is secreted in large quantities by adipose tissue and plays important roles in the regulation of glucose and lipid metabolism4. In arthritis models and joint tissues, adiponectin plays roles in the initiation and progression of OA, and exerts pro- or anti-inflammatory effects depending on the tissue and cell types5. Although the circulating adiponectin level was reported be elevated in patients with OA compared to healthy controls in two recent meta-analyses6,7, the role of adiponectin in the pathogenesis of OA is controversial. Several studies have evaluated the association between plasma and synovial fluid adiponectin levels and the severity of OA in the knee and hand based on radiographic findings. Studies examining the correlation of the adiponectin level with the severity of knee joint OA based on the Kellgren-Lawrence grade have yielded inconsistent results (positive associations in two studies8,9, negative associations in two others10,11, and no association in three studies12,13,14. Similarly, two studies found an inverse association between the adiponectin level and radiographic hand OA15,16, but two others found no such association17,18. These varying results may be attributable to the small numbers of subjects and use of a low-accuracy radiographic grading method, such as the Kellgren-Lawrence grade. To overcome these limitations of previous studies, we took advantage of the availability of a large, population-based cohort to evaluate the relationship between the adiponectin level and radiographic severity of knee and hand OA using a novel, semi-quantitative grading system19. The aim of this study was to investigate the association of serum adiponectin levels with the radiographic features of knee and hand OA.
Methods
Population and study design
The subjects were from the Dong-gu Study, a population-based cohort study performed in South Korea. The study was conducted from 2007 to 2010 in the Dong-gu area of Gwangju Metropolitan City; 9260 subjects aged ≥ 50 years participated in the study20. To identify risk factors for OA, an ancillary study was conducted on 2516 subjects who participated in the Dong-gu Study in 2009. X-rays of the knees and hands of 2489 subjects were obtained. We included 2402 subjects in the final analysis after excluding 51 subjects with a history of total knee arthroplasty surgery or knee amputation, 15 with missing data on smoking and drinking status, and 21 with missing data on adiponectin levels. The study was approved by the Institutional Review Board of Chonnam National University Hospital (IRB approval no. CNUH-2019-335), and all patients provided written informed consent at the time of enrollment. This study was conducted in accordance with the Declaration of Helsinki and the Good Clinical Practice guidelines.
Covariates
We collected information on the subjects’ baseline characteristics—including smoking, alcohol drinking, education and physical activity—by means of questionnaires. Body mass index (BMI) was calculated as the weight in kilograms divided by the height in meters squared. Smoking status was categorized as never smoker (< 100 lifetime cigarettes and not smoking currently), ex-smoker (> 100 lifetime cigarettes and not smoking currently), or current smoker (> 100 lifetime cigarettes and smoking now). Alcohol consumption in the past 12 months was used as the criterion to distinguish current alcohol drinkers from non-drinkers. Educational attainment was classified as high school or above high school. Physical activity was classified as regular or irregular according to the frequency of engagement in physical training/leisure activities during a typical week.
Assay of serum adiponectin levels
Serum adiponectin levels were measured by enzyme-linked immunosorbent assay (AdipoGen, Incheon, South Korea) and divided into three tertiles: < 12.08 μg/mL, 12.09–19.69 μg/mL, and ≥ 19.72 μg/mL. The intra-assay coefficient was 5.2% and the inter-assay coefficient of variance was 7.2%.
Radiographic assessment
Anteroposterior X-rays of the hands and knees were obtained with the subject in the standing position. The X-ray images were evaluated by two independent observers using a semi-quantitative grading system21. The intraobserver (kappa, 0.85–0.92) and interobserver (kappa, 0.79–0.89) reliability were both good.
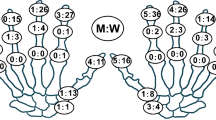
We described the semi-quantitative grading system previously22. In brief, radiographic features were noted for the hand (distal interphalangeal joint [DIP], proximal interphalangeal joint [PIP], carpometacarpal joint [CMC], interphalangeal joint of the thumb [IP], and naviculotrapezial joint [NTJ]) and knee (medial compartment, lateral compartment, tibial component, and femoral component). The degree of damage was graded as 0 to 3 (0, normal; 1, mild; 2, moderate; 3, severe), or as absent (0) or present (1). For the hand, osteophyte and joint space narrowing (JSN) scores were obtained for the DIP (0–3), PIP (0–3), CMC (0–3), IP (0/1), and NTJ (0/1); sclerosis and malalignment scores were obtained for the DIP (0/1), PIP (0/1), and CMC (0/1); subchondral cyst scores were obtained for the PIP (0/1) and CMC (0/1); and erosion scores were obtained for the DIP (0/1), DIP—central erosion (0/1), DIP—pseudowidening (0/1), PIP (0/1), and CMC (0/1). For the knee, osteophyte scores were obtained for the medial femoral condyle (0–3), medial tibial plateau (0–3), lateral femoral condyle (0–3), and lateral tibial plateau (0–3); JSN scores were obtained for the medial compartment (0–3) and lateral compartment (0–3); a medial tibial attrition score was also obtained (0–3, as well as medial tibial sclerosis (0–3) and lateral femoral sclerosis scores (0–3). The total score (max = 70) of the hand joint was given by the sum of the scores on the six subscales: the osteophyte score (max = 22), JSN score (max = 22), subchondral cysts score (max = 4), sclerosis score (max = 6), erosion score (max = 10), and malalignment score (max = 6). The total score (max = 42) of the knee joint was given by the sum of the scores on the four subscales: osteophyte score (max = 24), JSN score (max = 12), tibial attrition score (max = 2), and sclerosis score (max = 4).
Statistical analysis
The general characteristics of the subjects are presented as means and standard deviation (SD) for continuous variables and as number (%) for categorical variables. Continuous variables were compared by one-way analysis of variance, and categorical variables by chi-squared test. Linear regression analysis was performed to assess the relationship between serum adiponectin levels and radiographic scores of the knee and hand joints after adjusting for age, sex, BMI, smoking, alcohol consumption, education, and physical activity. P-values for paired comparisons among adiponectin tertiles were adjusted using the Bonferroni correction. Values are provided as adjusted means ± SD. In addition, dichotomous logistic regression analyses were conducted to determine whether values above the median adiponectin levels were associated with increased radiographic severity based on the median radiographic scores. A value of P < 0.05 was taken to indicate statistical significance. Statistical analysis was performed using Stata software (version 14.2; Stata Corporation, College Station, TX, USA).
Results
Baseline characteristics stratified by serum adiponectin levels
The baseline characteristics and radiographic features of the knee and hand joints according to serum adiponectin levels tertile are presented in Table 1. Among the 2402 subjects, the mean age was 64 years (SD, 8.2 years) and the mean BMI was 24.4 kg/m2 (SD, 2.9 kg/m2); 1042 subjects (43.4%) were male. Subjects in the higher serum adiponectin tertiles were older (mean age, 64.9 years) and had a lower BMI (mean, 23.8 kg/m2) than those in the lower tertiles. In addition, the proportions of subjects who were male (24.3%), current smokers (8.1%), current alcohol drinkers (40.1%), had an educational level of above high school (26.0%), and partook in regular physical activity (13.9%) were lower in subjects in the higher serum adiponectin tertiles than in those in the lower tertiles.
Regarding the radiographic scores of the knee joints, subjects in the higher serum adiponectin tertiles had a significantly higher total score (P < 0.001), osteophyte score (P < 0.001), JSN score (P < 0.001) and sclerosis score (P = 0.010) than those in the lower tertiles. However, the tibial attrition score did not differ among serum adiponectin tertiles (P = 0.136). Regarding the hand joint scores, subjects in the higher serum adiponectin tertiles had a significantly higher total score, JSN score, and subchondral cyst score than those in the lower tertiles (all P < 0.001). However, the osteophyte, sclerosis, erosion, and malalignment scores did not differ among serum adiponectin tertiles.
Association between the tertiles of serum adiponectin levels and knee and hand OA
Table 2 shows the relationships between serum adiponectin levels and total and individual radiographic scores of the knee and hand joints. In multiple linear regression analyses adjusted for age, sex, BMI, smoking, alcohol consumption, education level, and physical activity, serum adiponectin levels were positively associated with the total (P < 0.001), osteophyte (P = 0.003), and JSN (P < 0.001) scores in knee joints. However, in multiple linear regression analyses, there was no significant difference in the score for any hand joint parameter among the serum adiponectin tertiles after adjusting for age, sex, BMI, smoking, alcohol consumption, education level, and physical activity.
Associations of serum adiponectin levels above and below the median with knee and hand OA
Table 3 shows the relationships of serum adiponectin levels above and below the median with the total radiographic scores of the knee and hand joints based on the median radiographic scores. In multivariate logistic regression analysis adjusted for age, sex, BMI, smoking, alcohol consumption, education level, and physical activity, subjects with serum adiponectin levels above the median had higher total radiographic scores in the knee joints (P = 0.049), but not in the hand joints. Regarding the individual radiographic scores (Supplementary Table S1), adiponectin levels above the median were associated with the osteophyte (P = 0.018) and JSN (P = 0.022) scores in knee joints, and erosion (P = 0.026) and malalignment (P = 0.046) scores in hand joints, after adjustment.
Discussion
In this cross-sectional study, serum adiponectin levels were positively associated with the radiographic severity of OA in the knee joints, but not in the hand joints. Among the knee OA parameters, the adiponectin level was associated with the osteophyte, JSN, and total scores. To our knowledge, this is the largest study to investigate the relationship between serum adiponectin levels and radiographic severity of OA using a semi-quantitative grading system.
In this study, serum adiponectin levels were positively associated with the radiographic severity of OA of the knee joints, and particularly with the osteophyte and JSN scores. Prior studies of the association between the blood adiponectin level and radiographic severity of knee OA produced conflicting results. In a Finish study of 35 male patients with knee OA, the plasma adiponectin level was significantly higher in patients with radiographically severe OA than in those with mild OA8. In a Turkish study of 60 patients with knee OA, serum adiponectin levels were positively correlated with the Kellgren-Lawrence grade9. However, in a Thai study10 and the Anhui OA study11, the circulating adiponectin level was negatively associated with disease severity, as measured by the Kellgren-Lawrence grade, suggesting a protective role for adiponectin against knee OA. Interestingly, no association was found between the blood adiponectin level and severity of knee OA in the Framingham Offspring cohort study14, nor in Greek12, and Dutch studies13. These conflicting results may be attributable to small numbers of OA patients, use of radiographic grading systems with low accuracy (such as the Kellgren-Lawrence grade), inadequate control for confounding variables in the statistical analysis, and the use of different methods to measure isoforms of adiponectin. In comparison with previous studies, we recruited a large number (2402) of subjects from the Dong-gu study, obtained detailed information on the radiographic features of OA using a semi-quantitative grading system, and adjusted for relevant confounding variables in the statistical analysis. Although our finding of a positive association of adiponectin with the radiographic severity of knee OA requires confirmation in a prospective study, it provides insight into the role of adiponectin in the initiation and progression of knee OA.
Serum adiponectin levels were not associated with the radiographic severity of OA of the hand joints. A longitudinal study of 164 patients with hand OA reported that a higher level of adiponectin was associated with a lower risk of radiographic progression15. Another longitudinal study of 224 patients with hand OA investigated the associations between total and high-molecular-weight (HMW) adiponectin levels with the radiographic severity of hand OA16. The total adiponectin level was inversely associated with radiographic progression, but the HMW adiponectin level was not associated with progression. In contrast, in two cross-sectional studies17,18, serum adiponectin levels were not associated with the radiographic severity of hand OA. Our findings are in accordance with the results of cross-sectional studies, but not with those of longitudinal studies; this suggests that the differences are attributable to period and cohort effects23. Further studies are needed to determine if there is a causal relationship between serum adiponectin levels and radiographic severity of OA of the hand.
In this study, serum adiponectin levels were associated with the radiographic severity of OA in the knee joints, but not in the hand joints. Two hypotheses can be formulated that may explain the difference. First, obesity has a greater effect on knee OA than on hand OA24. In our previous study of the Dong-gu cohort, body weight was significantly associated with the radiographic severity of knee, but not hand, OA25. Because adiponectin originates predominantly from adipose tissue, it can be postulated that weight-bearing knee joints are more closely associated with the adiponectin level than are non-weight-bearing hand joints. Second, the expression level of adiponectin receptors differs among the joints. Adiponectin acts via two receptors: AdipoR1, predominantly found in skeletal muscle; and AdipoR2, mainly present in the liver26. The skeletal muscle mass of knee joints is greater than that of hand joints, so the role of adiponectin may differ among joints.
The strengths of our study included its inclusion of a large population-based cohort, detailed radiographic grading, and simultaneous evaluation of knee and hand joints. However, the study also had several limitations. First, the design was cross-sectional rather than longitudinal; therefore, the results are correlational and causality cannot be determined. Second, although many potential confounding factors were adjusted for, residual confounding effects of unmeasured variables may have introduced bias. Third, the adiponectin level was measured systemically, so may not reflect the intraarticular adiponectin level.
Conclusion
In this population-based study, serum adiponectin levels were positively associated with the radiographic severity of OA in knee joints, but not in hand joints. Our findings indicate that different pathophysiologic mechanisms underlie the initiation and progression of OA of the knee and hand joints.
Data availability
Full original protocol and dataset can be accessed upon request for academic researchers by contacting Professor Shin-Seok Lee (shinseok@chonnam.ac.kr).
References
Cisternas, M. G. et al. Alternative methods for defining osteoarthritis and the impact on estimating prevalence in a US population-based survey. Arthritis Care Res. (Hoboken) 68, 574–580 (2016).
Bijlsma, J. W., Berenbaum, F. & Lafeber, F. P. Osteoarthritis: An update with relevance for clinical practice. Lancet 377, 2115–2126 (2011).
Urban, H. & Little, C. B. The role of fat and inflammation in the pathogenesis and management of osteoarthritis. Rheumatology (Oxford) 57, 10–21 (2018).
Yamauchi, T. et al. Targeted disruption of AdipoR1 and AdipoR2 causes abrogation of adiponectin binding and metabolic actions. Nat. Med. 13, 332–339 (2007).
Xie, C. & Chen, Q. Adipokines: New therapeutic target for osteoarthritis?. Curr. Rheumatol. Rep. 21, 71 (2019).
Lee, Y. H. & Song, G. G. Association between circulating adiponectin levels and osteoarthritis: A meta-analysis. J. Rheum. Dis. 25, 231–238 (2018).
Tang, Q. et al. Association of osteoarthritis and circulating adiponectin levels: A systematic review and meta-analysis. Lipids Health Dis. 17, 189 (2018).
Koskinen, A. et al. Adiponectin associates with markers of cartilage degradation in osteoarthritis and induces production of proinflammatory and catabolic factors through mitogen-activated protein kinase pathways. Arthritis Res. Ther. 13, R184 (2011).
Cuzdan Coskun, N., Ay, S., Evcik, F. D. & Oztuna, D. Adiponectin: is it a biomarker for assessing the disease severity in knee osteoarthritis patients?. Int. J. Rheum. Dis. 20, 1942–1949 (2017).
Honsawek, S. & Chayanupatkul, M. Correlation of plasma and synovial fluid adiponectin with knee osteoarthritis severity. Arch. Med. Res. 41, 593–598 (2010).
Zheng, S. et al. Association between circulating adipokines, radiographic changes, and knee cartilage volume in patients with knee osteoarthritis. Scand. J. Rheumatol. 45, 224–229 (2016).
Staikos, C. et al. The association of adipokine levels in plasma and synovial fluid with the severity of knee osteoarthritis. Rheumatology (Oxford) 52, 1077–1083 (2013).
Van Spil, W. E. et al. Cross-sectional and predictive associations between plasma adipokines and radiographic signs of early-stage knee osteoarthritis: Data from CHECK. Osteoarthritis Cartilage 20, 1278–1285 (2012).
Vlad, S. C., Neogi, T., Aliabadi, P., Fontes, J. D. & Felson, D. T. No association between markers of inflammation and osteoarthritis of the hands and knees. J. Rheumatol. 38, 1665–1670 (2011).
Yusuf, E. et al. Association between leptin, adiponectin and resistin and long-term progression of hand osteoarthritis. Ann. Rheum. Dis. 70, 1282–1284 (2011).
Klein-Wieringa, I. R. et al. Are baseline high molecular weight adiponectin levels associated with radiographic progression in rheumatoid arthritis and osteoarthritis?. J. Rheumatol. 41, 853–857 (2014).
Choe, J. Y. et al. Serum resistin level is associated with radiographic changes in hand osteoarthritis: Cross-sectional study. Joint Bone Spine 79, 160–165 (2012).
Massengale, M., Lu, B., Pan, J. J., Katz, J. N. & Solomon, D. H. Adipokine hormones and hand osteoarthritis: Radiographic severity and pain. PLoS ONE 7, e47860 (2012).
Wen, L. et al. The relationships between bone mineral density and radiographic features of hand or knee osteoarthritis in older adults: Data from the Dong-gu Study. Rheumatology (Oxford) 55, 495–503 (2016).
Kweon, S. S. et al. Cohort profile: The Namwon Study and the Dong-gu Study. Int. J. Epidemiol. 43, 558–567 (2014).
Altman, R. D. & Gold, G. E. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthritis Cartilage 15(Suppl A), A1-56 (2007).
Wen, L. et al. Association between grip strength and hand and knee radiographic osteoarthritis in Korean adults: Data from the Dong-gu study. PLoS ONE 12, e0185343 (2017).
Louis, T. A., Robins, J., Dockery, D. W., Spiro, A. 3rd. & Ware, J. H. Explaining discrepancies between longitudinal and cross-sectional models. J. Chronic Dis. 39, 831–839 (1986).
Felson, D. T. Does excess weight cause osteoarthritis and if so, why?. Ann. Rheum. Dis. 55, 668–670 (1996).
Wen, L. et al. Associations between body composition measurements of obesity and radiographic osteoarthritis in older adults: Data from the Dong-gu Study. BMC Musculoskelet. Disord. 17, 192 (2016).
Yamauchi, T. & Kadowaki, T. Adiponectin receptor as a key player in healthy longevity and obesity-related diseases. Cell Metab. 17, 185–196 (2013).
Acknowledgements
This study was supported by a grant (BCRI20047) from Chonnam National University Hospital Biomedical Research Institute. The authors also thank the patients and their families for their participation.
Author information
Authors and Affiliations
Contributions
H.X., M.-H.S. and S.-S.L. conceived and designed the study. J.-H.K., S.-E.C., D.-J.P., S.-S.K., Y.-H.L., H.-Y.K. and J.-K.L. acquired data. H.X., M.-H.S. and S.-S.L. performed statistical analysis and drafted the manuscript. All authors critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xu, H., Kang, JH., Choi, SE. et al. Increased adiponectin levels are associated with higher radiographic scores in the knee joint, but not in the hand joint. Sci Rep 11, 1842 (2021). https://doi.org/10.1038/s41598-021-81513-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-81513-z
This article is cited by
-
Specific-cytokine associations with outcomes in knee osteoarthritis subgroups: breaking down disease heterogeneity with phenotyping
Arthritis Research & Therapy (2024)
-
Obesity, Metabolic Syndrome, and Osteoarthritis—An Updated Review
Current Obesity Reports (2023)
-
mtDNA haplogroup A enhances the effect of obesity on the risk of knee OA in a Mexican population
Scientific Reports (2022)
-
Elevated resting heart rate is associated with increased radiographic severity of knee but not hand joints
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
