
Abstract
The relationship between visceral adiposity index (VAI) and unhealthy metabolic phenotype remained unclear in children and adolescents. This study aimed to investigate their association and compared the ability of VAI and traditional adiposity indicators (body mass index, waist circumference and waist-to-height ratio) to predict metabolically unhealthy phenotype among normal-weight, overweight and obese children and adolescents. In this cross-sectional study, 1722 children and adolescents aged 12–18 years were selected by cluster random sampling, underwent a questionnaire survey, physical examination and biochemical tests. Participants were divided into four phenotypes according to the combination of the weight status determined by body mass index (BMI) and metabolic syndrome components. Receiver operating characteristic (ROC) analysis and multivariate logistic regression were used to compare the predictive capacity between VAI and traditional adiposity indicators and their relationship with metabolically unhealthy phenotype. We found that VAI had better performance in predicting metabolically unhealthy phenotype than traditional adiposity indicators, the area under the receiver-operating characteristic curve (AUC) were 0.808 and 0.763 for boys and girls with normal-weight, 0.829 and 0.816 for boys and girls with overweight and obese (all P < 0.001). VAI was most strongly related to metabolically unhealthy phenotype whether or not to adjust the age, the adjusted OR and 95%CI was 6.15 (4.13–9.14) in boys with normal weight, and 5.90 (3.06–11.36), 4.95 (2.35–10.41) in boys and girls with overweight and obese, respectively (all P < 0.001). Our findings suggested VAI could be used as a comprehensive predictor to identify unhealthy metabolic phenotype in children and adolescents.
Similar content being viewed by others

Introduction
The global prevalence of overweight and obesity among children and adolescents is increasing rapidly and has become a major public health problem1, especially in China2. Childhood obesity was associated with cardiac metabolic disorders, including elevated blood pressure (BP), hyperglycemia and hyperlipidemia3,4, and cardiovascular risk in children could be accompanied into adulthood, aggravating the risk of cardiac metabolism5. However, not all obese individuals had the same metabolic risk, on the contrary, they had favorable metabolic characteristics (such as high insulin sensitivity), which was defined metabolically healthy obesity6,7 and some individuals with normal-weight had metabolic disorders, which was defined metabolically unhealthy normal-weight (MUNW)8. Compared to metabolically healthy normal-weight (MHNW) individuals, metabolically unhealthy obesity and metabolically healthy overweight or obesity individuals had a higher risk of hypertension and cardiovascular disease9,10,11. Thus, early identification of different metabolic phenotypes was important for disease prevention among children and adolescents.
At present, the underlying mechanism for determining different metabolic phenotypes was unclear, which may be related to visceral fat accumulation12, inflammatory factors13, genetics14, dietary intake behaviors and lifestyle habits15. Some studies showed that visceral adipose tissue (VAT) was positively correlated with cardiometabolic risk factors16. As the gold standard for measuring visceral obesity, computed tomography and magnetic resonance imaging were characterized by radiation hazards and high costs, therefore, these techniques were not suitable for large-scale epidemiological investigations17. Visceral adiposity index (VAI), which combined anthropometric (body mass index (BMI) and waist circumference (WC)) and metabolic characteristics (serum triglyceride (TG) and high-density lipoprotein cholesterol (HDL-C)), was considered to be a reliable indicator of visceral fat18.
Studies suggested that compared with traditional adiposity indicators, such as WC and waist-to-height ratio (WHtR), VAI was most strongly related to the metabolically unhealthy phenotype, and showed better power of predicting unhealthy metabolic phenotype in adults17,19. However, the relationship between VAI and metabolically unhealthy phenotype and its predictive value remained unclear among children and adolescents.
Therefore, we aimed to explore the relationship between VAI and unhealthy metabolic phenotype and compare the ability of VAI and traditional adiposity indexes to identify unhealthy metabolic phenotype among normal-weight, overweight and obese children and adolescents, using data from China.
Methods
Study population
Using the method of cluster random sampling, children and adolescents aged 12 to 18 were randomly selected from 13 classes of 3 Junior Middle Schools and 10 classes of 2 Senior High Schools in Yinchuan city, China, from 2017 to 2020. They underwent a questionnaire survey, physical examination and laboratory examination. After excluding participants with missing information, a total of 1722 subjects were enrolled in this study. All subjects and their parents/guardians signed written informed consents. This study was approved by the Ethics Committee of Ningxia Medical University (2016-123) and conducted in accordance with the Declaration of Helsinki.
Questionnaire investigation
The content of the questionnaire included the basic information of the subjects (name, sex, age and date of birth), dietary habits (smoking, drinking and diet) and so on. The basic information of the subjects and the high fat food consumption were used for data analysis. High fat food consumption defined as consumption of at least one meat, fried food or western fast food a week, including poultry meat, Youtiao, fried chicken, hamburger and so on.
Biochemical measurements
After an overnight fast of 12 h, venous blood samples were obtained into the procoagulant tube and centrifuged by 3000 r/min for 15 min after resting for 30 min; then the serum was collected and stored in the refrigerator at – 80 °C. The levels of total cholesterol (TC), TG, HDL-C, low-density lipoprotein cholesterol (LDL-C) and fasting plasma glucose (FPG) were determined using the American AU480 automatic biochemical analyzer.
Anthropometrical data
All anthropometric variables were measured by trained staff in strict accordance with the standard scheme. Height and WC were measured twice for subjects in light clothes without shoes to the nearest 0.1 cm, WC was measured at the midway between the inferior margin of the last rib and iliac crest at the end of normal exhalation, and weight also was measured twice to the nearest 0.1 kg with a lever scale (RGT-140, Wuxi Weigher Factory Co.,Ltd, China), the error of two measurements was no more than 0.5 cm or 0.5 kg. Mean value of weight and height were used to calculate BMI and WHtR. BMI = weight (kg)/height2 (m2), WHtR = WC (cm)/height (cm). For boys, VAI = [WC/(39.68 + 1.88 × BMI)] × (TG/1.03) × (1.31/HDL-C), for girls, VAI = [WC/(36.58 + 1.89 × BMI)] × (TG/0.81) × (1.52/HDL-C), with TG and HDL-C levels expressed as mmol/l. According to the method recommended by the American Hypertension Education Project working Group20, seated systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured continuously for 3 times with at least 1 min between repeated measurements, using an electronic sphygmomanometer (HEM-7012, Omron, Japan), and the difference between the two adjacent measurements was no more than 10 mmHg. The average value of the last two readings was used for analysis.
Definitions
The participants were divided into four metabolically phenotypes as following: (1) metabolically healthy normal-weight (MHNW); (2) metabolically unhealthy normal weight (MUNW); (3) metabolically healthy overweight or obesity (MHO); (4) metabolically unhealthy overweight or obesity (MUO). We used the presence of metabolic syndrome (MetS) components to define metabolic abnormalities, as follows21: (1) WC ≥ 95th percentile for age and sex22; (2) TG levels ≥ 1.24 mmol/L; (3) HDL-C ≤ 1.03 mmol/L; (4) SBP and/or DBP ≥ 90th percentile for age, sex and height23; (5) FPG levels ≥ 5.6 mmol/L. Individuals who meet at least two of the criteria mentioned above were considered metabolically unhealthy. According to the recommendation of the Working Group on obesity (WGOC) in China24, BMI was used to define normal-weight, overweight and obesity in children and adolescents.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median (25th–75th percentiles), and the differences between groups were compared using t-test or the Wilcoxon rank sum test of two independent samples. Categorical variables were presented as percentage, and the chi-square test was used to compare the differences between groups. The Z-scores by age and sex of VAI, BMI, WC and WHtR were calculated and used for receiver operating characteristic (ROC) analysis and multivariate logistic regression, Z-score = (test value-mean value by age and gender) /SD by age and gender. ROC analysis was used to compare the ability of VAI, BMI, WC and WHtR to predict MUNW and MUO; we evaluated the association of VAI, BMI, WC and WHtR with metabolic phenotypes by multivariate logistic regression, with adjustment for age. Epidata3.1 software was used to input data, and data were analyzed using SPSS26.0. Two-sided P < 0.05 was considered to be statistically significant.
Results
Among the 1722 children and adolescent evaluated, the prevalence of MHNW MUNW, MHO and MUO was 65.9%, 12.2%, 5.9% and 16.1%, respectively. Compared to girls, boys showed a lower prevalence of MUNW (9.3% vs 16.9%, P < 0.001), but there was no difference in the prevalence of MUO between the two groups (16.8% vs 14.9%, P = 0.290).
Tables 1 and 2 presented characteristics of subjects according to different phenotypes. Among normal-weight children and adolescents, the prevalence of MUNW was 15.6%, compared with girls, boys had a lower prevalence of MUNW (12.1% vs 21.1%, P < 0.001). Among overweight and obese children and adolescents, the prevalence of MUO was 73.3%, and no difference was found in the prevalence of MUO between boys and girls (72.8% vs 74.2%, P = 0.757). Compared to their metabolically healthy counterparts, metabolically unhealthy subjects showed higher weight, BMI, WC, WHtR, SBP, DBP, TG, FPG and VAI in both normal-weight, overweight and obese children and adolescents (all P < 0.05). In addition, MUNW individuals were older and had higher TC and LDL-C than those with MHNW; MUO individuals had higher height and lower HDL-C than MHO individuals (all P < 0.05). After gender stratification analysis, the results were consistent with the whole population, but no significant differences in FPG were found between MHO and MUO individuals in both genders, there were no significant differences in weight, BMI, WC and WHtR between MHO and MUO girls. Significant differences in consumption of high fat food were only found between MHNW and MUNW boys (P < 0.05).
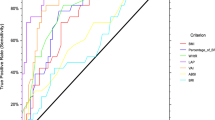
Table 3 and Supplementary Fig. 1 and Fig. 2 showed the ROC curve analysis of the VAI and traditional adiposity indicators for predicting unhealthy metabolic phenotype among normal-weight, overweight and obese individuals. VAI, BMI, WC and WHtR were able to predict MUNW and MUO in the whole population, and both sexes, except BMI and WHtR in overweight and obese girls. VAI presented the greatest diagnostic precision for predicting MUNW in participants with normal-weight (AUC of the whole population, boys and girls were 0.784, 0.808 and 0.763, respectively) and MUO in individuals with overweight and obesity (AUC of the whole population, boys and girls were 0.822, 0.829 and 0.816, respectively, all P < 0.05). In the traditional adiposity indicators, WC showed better ability to predict unhealthy metabolic phenotype in both genders. For boys and girls, the AUC were 0.667 and 0.746 in predicting MUNW, 0.761 and 0.618 in predicting MUNW phenotype, respectively (all P < 0.05).
Table 4 presented the result of multivariate logistic regression analysis. Regardless of whether the analytical model adjusted age or not, VAI and WC were associated with MUNW and MUO. VAI had a stronger association with MUNW and MUO, the adjusted OR and 95% confidence interval (CI) were 4.45 (3.45–5.73) and 5.11 (3.16–8.26), respectively (all P < 0.05). There were similar findings among boys, the adjusted OR and 95%CI were 6.15 (4.13–9.14) and 5.90 (3.06–11.36), respectively (all P < 0.05). However, the association of VAI and BMI with MUNW were found among normal-weight girls, and BMI showed a stronger association, age-adjusted OR and 95%CI was 4.16 (2.53–6.82) (P < 0.05); VAI was the independent determinants of MUO among overweight or obesity girls, the age-adjusted OR and 95%CI was 4.95 (2.35–10.41) (P < 0.05).
Discussion
Our results indicated that among children and adolescents, compared to traditional adiposity indexes (BMI, WC and WHtR), VAI had the greatest power to identify the unhealthy metabolic phenotype and VAI was most strongly related to the MUNW and MUO phenotype. After gender stratification analysis, the results were similar, but except that BMI was most strongly associated with the MUNW phenotype in normal-weight girls. In addition, WC performed better than BMI and WHtR in predicting unhealthy metabolic phenotype in both sexes.
Due to the difference in diagnostic criteria for obesity and metabolic abnormalities, age range and population source, the prevalence of metabolically unhealthy phenotype was different in children and adolescents or adults. Some research suggested that among children and adolescents, the prevalence of MUNW and MUO ranged from 10.6–18.8%25,26,27 to 1.3–15.3%, respectively25,26,28,29,30. Our results were roughly consistent with the above research (12.2% and 16.1%, respectively). What’s more, compared with their metabolically healthy counterparts, individuals with MUNW and MUO showed higher VAI, BMI, WC, WHtR and worse metabolic profiles, which agreed with previous studies19,26.
A cross-section study for Chinese adults suggested that VAI and lipid accumulation product (LAP) were effective markers for identifying MUNW phenotype, the AUC of VAI ranged from 0.611 to 0.835 based on the criteria used for MUNW phenotype17. Data from Brazil indicated that VAI had the better predictive capacity and stronger association with metabolically unhealthy phenotype than other adiposity indexes (BMI, WHtR, waist-to-hip ratios, WC and neck circumference), the AUC for MUNW were 0.865 and 0.847 for men and women with normal weight, the AUC for MUO were 0.830 and 0.903 for men and women with overweight19. Ahmad reported that VAI proved to be superior to other obesity indicators in predicting cardiometabolic risks, VAI showed the largest AUC for men and women (0.79 vs 0.77), followed by waist-to-hip ratios (0.73 vs 0.75), WC (0.69 vs 0.74), WHtR (0.65 vs 0.71) and BMI (0.53 vs 0.51), respectively31. A cohort study followed up for ten years demonstrated that MHO was a transient state, with higher conversion to MUO independently related to VAT, higher fasting insulin level, et al32. Vizzuso found that VAI could be a promising tool to identify MetS in children and adolescents with obesity33. These findings were consistent with our results; VAI showed the strongest prediction ability, it may be due to VAI served as a powerful surrogate marker of visceral adiposity, while these traditional obesity indicators could only provide limited fat distribution information and lack the ability to distinguish between visceral and subcutaneous fat34. These findings suggested that VAI could be a better surrogate index than single traditional adiposity indices to evaluate the adverse metabolic phenotype of children and adolescents. The levels of visceral fat mass were positively associated with elevated BP and dyslipidemia among normal-weight, overweight and obese children and adolescent, which supported our view25.
However, a cohort of obesity children and adolescents aged 4 to 18 evaluated the impact of WHtR, serum Uric Acid and Homeostatic Model Assessment index of insulin resistance on the probability to be MUO, and found that these indexes were independent predictors of the probability of being MUO35. Data from the US National Health and Nutrition Examination Surveys (NHANES, 1999–2012) demonstrated that the AUC of BMI-z score, WHtR-z score and WC-z score to detect at least three cardiovascular risk factors ranged from 0.84 to 0.85 either using the International Diabetes Federation (IDF) or the revised National Cholesterol Education Program Adult Treatment Panel III (ATP III) criteria36. The results of these studies were inconsistent with ours, it may be explained by different standards of metabolic abnormalities, demographic characteristics and variables analyzed.
Chinese visceral adiposity index (CVAI), a novel indicator of visceral obesity, was developed in Chinese adults when considering ethnic differences in body fat characteristics37,38. CVAI increased the factor of the demographic (age) based on VAI39. Some studies indicated that CVAI and its 6-year change were positively related to hypertension risk, CVAI was superior to VAI, BMI, WC and a body shape index (ABSI) in predicting hypertension for both genders40, and CVAI had better performance in predicting diabetes than BMI, WC and ABSI in both sexes41. These results suggested that compared with VAI, CVAI may be more suitable and reliable for predicting metabolically unhealthy phenotype in Chinese adults. Studies from China indicated that the VAT of both boys and girls aged 6–18 years old showed a wavy increase trend with the increase of age42. However, the content of VAT in men firstly increased and then decreased with age, and reached the peak at 30 years old, the VAT content of women increased rapidly from 20 to 50 years old and peaked at 50 years old, after 50 years old, it gradually decreased and stabilized43. Due to the different trend for age of VAT between children and adults, whether CVAI could be used as an effective indicator of VAT in children need to be verified among a large sample population.
At present, the underlying mechanism of VAI and abnormal metabolic phenotype remained unclear. The possible mechanisms were as follows. First, individuals with higher VAT had higher levels of inflammatory cytokines, such as tumour necrosis factor-α, C-reactive protein and interleukin-6, which may lead to insulin resistance and metabolic disorders44. The ectopic fat deposition was also a possible cause45. Second, the increase of VAT was related to the decrease of circulating concentrations of B-type natriuretic peptide, which may diminish natriuresis and vasodilation and lead to hypertension46. In addition, we found WC was positively associated with metabolically unhealthy phenotype in boys, it could be explained by that WC was correlated with increased free fat acid and adipokines, increased oxidative stress, higher activity of inflammation and blunt insulin sensitivity47. We also found that BMI was more strongly correlated with MUNW phenotype than VAI in girls, which may be partly ascribed to the fact that female’s fat mainly accumulated under the skin48, while in girls with normal-weight, the subcutaneous fat might have a greater effect on metabolism than VAT.
Our research had the following limitations. First, the cross-sectional study made it impossible for us to explore the causal relationship between VAI and metabolically unhealthy phenotype. Second, the subjects of our study were limited to children and adolescents aged 12–18 in Yinchuan city, China, and the results may not be generalisable to other populations. Third, confounding factors including physical activity and lifestyle were not assessed in this study, which might have influenced our results. Fourth, our findings may vary depending on the different definition of metabolic phenotype. Nevertheless, we compared the ability of VAI and traditional obesity indicators to identify adverse metabolic phenotypes, so as to provide the scientific basis for the prevention of metabolic diseases in children and adolescents.
Conclusions
In conclusion, the study indicated that compared with traditional adiposity indicators, VAI had the better power of predicting metabolically unhealthy phenotype in both genders, and VAI was most strongly associated with metabolically unhealthy phenotype in boys and MUO phenotype in overweight and obese girls, regardless of whether the age was adjusted or not. VAI might be used as a comprehensive index for predicting adverse metabolic phenotype in children and adolescents. What’s more, in the traditional adiposity indicators, WC was the better index for the screening of metabolically unhealthy phenotype in both genders.
References
Ng, M. et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 384, 766–781. https://doi.org/10.1016/s0140-6736(14)60460-8 (2014).
Ma, S., Zhang, Y., Yang, L., Zhao, M. & Xi, B. Analysis on the trend of overweight and obesity of children and adolescents in 9 provinces of China from 1991 to 2015. Chin. J. Prev. Med. 54, 133–138 (2020).
Chen, F. et al. Association between childhood obesity and metabolic syndrome: Evidence from a large sample of chinese children and adolescents. PLoS ONE 7, 1–7. https://doi.org/10.1371/journal.pone.0047380 (2012).
Ayer, J., Charakida, M., Deanfield, J. E. & Celermajer, D. S. Lifetime risk: Childhood obesity and cardiovascular risk. Eur. Heart J. 36, 1371–1376. https://doi.org/10.1093/eurheartj/ehv089 (2015).
Koskinen, J. et al. Childhood age and associations between childhood metabolic syndrome and adult risk for metabolic syndrome, type 2 diabetes mellitus and carotid intima media thickness: The international childhood cardiovascular cohort consortium. J. Am. Heart Assoc. 6, 1–17. https://doi.org/10.1161/JAHA.117.005632 (2017).
Blüher, M. Mechanisms in endocrinology: Are metabolically healthy obese individuals really healthy?. Eur. J. Endocrinol. 171, R209–R219. https://doi.org/10.1530/EJE-14-0540 (2014).
Prince, R. L., Kuk, J. L., Ambler, K. A., Dhaliwal, J. & Ball, G. D. C. Predictors of metabolically healthy obesity in children. Diabetes Care 37, 1462–1468. https://doi.org/10.2337/dc13-1697 (2014).
Choi, K. M. et al. Higher mortality in metabolically obese normal-weight people than in metabolically healthy obese subjects in elderly Koreans. Clin. Endocrinol. (Oxf) 79, 364–370. https://doi.org/10.1111/cen.12154 (2013).
Mirzababaei, A., Mozaffari, H., Shab-Bidar, S., Milajerdi, A. & Djafarian, K. Risk of hypertension among different metabolic phenotypes: A systematic review and meta-analysis of prospective cohort studies. J. Hum. Hypertens. 33, 365–377. https://doi.org/10.1038/s41371-018-0146-y (2019).
Aung, K. K., Lorenzo, C., Hinojosa, M. A. & Haffner, S. M. Risk of developing diabetes and cardiovascular disease in metabolically unhealthy normal-weight and metabolically healthy obese individuals. J. Clin. Endocrinol. Metab. 99, 462–468. https://doi.org/10.1210/jc.2013-2832 (2014).
Iacobini, C., Pugliese, G., Blasetti Fantauzzi, C., Federici, M. & Menini, S. Metabolically healthy versus metabolically unhealthy obesity. Metabolism 92, 51–60. https://doi.org/10.1016/j.metabol.2018.11.009 (2019).
Xia, L. et al. Association between indices of body composition and abnormal metabolic phenotype in normal-weight Chinese adults. Int. J. Environ. Res. Public Health. 14, 391. https://doi.org/10.3390/ijerph14040391 (2017).
Agostinis-Sobrinho, C. et al. Higher cardiorespiratory fitness levels may attenuate the detrimental association between weight status, metabolic phenotype and c-reactive protein in adolescents—a multi-cohort study. Nutrients 12, 1461. https://doi.org/10.3390/nu12051461 (2020).
Plaza-Florido, A. et al. Distinct whole-blood transcriptome profile of children with metabolic healthy overweight/obesity compared to metabolic unhealthy overweight/obesity. Pediatr. Res. https://doi.org/10.1038/s41390-020-01276-7 (2020).
Qorbani, M. et al. Association of dietary behaviors, biochemical, and lifestyle factors with metabolic phenotypes of obesity in children and adolescents. Diabetol. Metab. Syndr. 12, 1–7. https://doi.org/10.1186/s13098-020-00617-0 (2020).
Demirbas, N. & Kutlu, R. Importance of measured body fat, visceral adiposity index, and lipid accumulation product index in predicting cardiometabolic risk factors. Metab. Syndr. Relat. Disord. 19, 174–179. https://doi.org/10.1089/met.2020.0098 (2021).
Du, T., Yu, X., Zhang, J. & Sun, X. Lipid accumulation product and visceral adiposity index are effective markers for identifying the metabolically obese normal-weight phenotype. Acta Diabetol. 52, 855–863. https://doi.org/10.1007/s00592-015-0715-2 (2015).
Li, R. et al. Visceral adiposity index, lipid accumulation product and intracranial atherosclerotic stenosis in middle-aged and elderly Chinese. Sci. Rep. 7, 1–9. https://doi.org/10.1038/s41598-017-07811-7 (2017).
Ferreira, F. G., Juvanhol, L. L., Da Silva, D. C. G. & Longo, G. Z. Visceral adiposity index is a better predictor of unhealthy metabolic phenotype than traditional adiposity measures: Results from a population-based study. Public Health Nutr. 22, 1545–1554. https://doi.org/10.1017/S136898001800335X (2019).
Falkner, B. & Daniels, S. R. Summary of the fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Hypertension 44, 387–388. https://doi.org/10.1161/01.HYP.0000143545.54637.af (2004).
Wan, N. J. et al. Metabolic syndrome in overweight and obese schoolchildren in Beijing. Chin J Pediatr. 45, 417–421 (2007).
Ma, G. S. et al. Waist circumference reference values for screening cardiovascular risk factors in chinese children and adolescents. Biomed. Environ. Sci. 23, 21–31. https://doi.org/10.1016/S0895-3988(10)60027-X (2010).
Fan, H., Yan, Y. K. & Mi, J. Updating blood pressure references for Chinese children aged 3–17 years. Chin. J. Hypertens. 25, 428–435 (2017).
Ji, C. Y. Working Group on Obesity in China Report on childhood obesity in China (1)—body mass index reference for screening overweight and obesity in Chinese school-age children. Biomed. Environ. Sci. 18, 390–400 (2005).
Chen, F. et al. Abnormal metabolic phenotypes among urban chinese children: Epidemiology and the impact of DXA-measured body composition. Obesity 27, 837–844. https://doi.org/10.1002/oby.22426 (2019).
Ding, W. Q. et al. DXA-measured visceral fat mass and lean body mass reflect abnormal metabolic phenotypes among some obese and nonobese Chinese children and adolescents. Nutr. Metab. Cardiovasc. Dis. 28, 618–628. https://doi.org/10.1016/j.numecd.2018.03.002 (2018).
Li, Y. P. et al. Disease risks of childhood obesity in China. Biomed Environ Sci. 18, 401–410 (2005).
Heshmat, R. et al. Prevalence of different metabolic phenotypes of obesity in Iranian children and adolescents: the CASPIAN V study. J. Diabetes Metab. Disord. 17, 211–221. https://doi.org/10.1007/s40200-018-0363-5 (2018).
Esmaili, H. et al. Association of serum 25-hydroxyvitamin D level with metabolic phenotypes of obesity in children and adolescents: The CASPIAN-V study. Front. Endocrinol. (Lausanne) 11, 1–8. https://doi.org/10.3389/fendo.2020.00310 (2020).
Asghari, G., Hosseinpanah, F., Serahati, S., Haghi, S. & Azizi, F. Association between obesity phenotypes in adolescents and adult metabolic syndrome: Tehran Lipid and Glucose Study. Br. J. Nutr. 122, 1255–1261. https://doi.org/10.1017/S0007114519002344 (2019).
Ahmad, M. N. & Haddad, F. H. Suitability of visceral adiposity index as a marker for cardiometabolic risks in jordanian adults. Nutr. Hosp. 32, 2701–2709. https://doi.org/10.3305/nh.2015.32.6.9543 (2015).
Hwang, Y. C. et al. Visceral abdominal fat accumulation predicts the conversion of metabolically healthy obese subjects to an unhealthy phenotype. Int. J. Obes. 39, 1365–1370. https://doi.org/10.1038/ijo.2015.75 (2015).
Vizzuso, S. et al. Visceral adiposity index (VAI) in children and adolescents with obesity: No association with daily energy intake but promising tool to identify metabolic syndrome (MetS). Nutrients 13, 1–15. https://doi.org/10.3390/nu13020413 (2021).
Dong, H., Xu, Y., Zhang, X. & Tian, S. Visceral adiposity index is strongly associated with hyperuricemia independently of metabolic health and obesity phenotypes. Sci. Rep. 7, 1–13. https://doi.org/10.1038/s41598-017-09455-z (2017).
Genovesi, S. et al. Cardiovascular risk factors associated with the metabolically healthy obese (MHO) phenotype compared to the metabolically unhealthy obese (MUO) phenotype in children. Front. Endocrinol. 11, 27. https://doi.org/10.3389/fendo.2020.00027 (2020).
Zhao, M., Bovet, P., Ma, C. & Xi, B. Performance of different adiposity measures for predicting cardiovascular risk in adolescents. Sci. Rep. 7, 1–6. https://doi.org/10.1038/srep43686 (2017).
Deurenberg, P., Deurenberg-Yap, M. & Guricci, S. Asians are different from Caucasians and from each other in their body mass index/body fat per cent relationship. Obes. Rev. 3, 141–146. https://doi.org/10.1046/j.1467-789X.2002.00065.x (2002).
Camhi, S. M. et al. The relationship of waist circumference and BMI to visceral, subcutaneous, and total body fat: Sex and race differences. Obesity 19, 402–408. https://doi.org/10.1038/oby.2010.248 (2011).
Xia, M. F. et al. A indicator of visceral adipose dysfunction to evaluate metabolic health in adult Chinese. Sci. Rep. 6, 1–8. https://doi.org/10.1038/srep38214 (2016).
Han, M. et al. Chinese visceral adiposity index, a novel indicator of visceral obesity for assessing the risk of incident hypertension in a prospective cohort study. Br. J. Nutr. 1, 1–9. https://doi.org/10.1017/S0007114520004298 (2020).
Wei, J., Liu, X., Xue, H., Wang, Y. & Shi, Z. Comparisons of visceral adiposity index, body shape index, body mass index and waist circumference and their associations with diabetes mellitus in adults. Nutrients 11, 1580. https://doi.org/10.3390/nu11071580 (2019).
Li, K. K. Association between body fat distribution and cardiovascular disease risk factors in school-age children and adolescents in Yinchuan. Ningxia Medical University. https://kns.cnki.net/KCMS/detail/detail.aspx?dbname=CMFD202002&filename=1020753743.nh (2020).
Huang, B. B. et al. Body fat parameters of adult population in Guangxi with the change trend of age. Acat Anat. Sin. 51, 300–305. https://doi.org/10.16098/j.issn.0529-1356.2020.02.025 (2020).
Fontana, L., Eagon, J. C., Trujillo, M. E., Scherer, P. E. & Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 56, 1010–1013. https://doi.org/10.2337/db06-1656 (2007).
Tsatsoulis, A. & Paschou, S. A. Metabolically healthy obesity: Criteria, epidemiology, controversies, and consequences. Curr. Obes. Rep. 9, 109–120. https://doi.org/10.1007/s13679-020-00375-0 (2020).
Seravalle, G. & Grassi, G. Obesity and hypertension. Pharmacol. Res. 122, 1–7. https://doi.org/10.1016/j.phrs.2017.05.013 (2017).
Matsuda, M. & Shimomura, I. Increased oxidative stress in obesity: Implications for metabolic syndrome, diabetes, hypertension, dyslipidemia, atherosclerosis, and cancer. Obes. Res. Clin. Pract. 7, 1–12. https://doi.org/10.1016/j.orcp.2013.05.004 (2013).
Bredella, M. A. Sex differences in body composition. Adv. Exp. Med. Biol. 1043, 9–27. https://doi.org/10.1007/978-3-319-70178-3_2 (2017).
Acknowledgements
The authors greatly appreciate the children and adolescents who participated in the study.
Funding
This work was supported by Ningxia Medical University scientific research project, the National Natural Science Foundation of China (Grant number 81660565) and the National Natural Science Foundation of China (Grant number 82160641).
Author information
Authors and Affiliations
Contributions
Y.D. and W.D. offered the concepts; Y.D. administered the data collection with contributions from R.C., L.B., J.Z. and W.D.; Y.D. performed the data analysis and drafted the manuscript.; Y.D. reviewed the manuscript with contributions from W.D.; all authors designed the study together. And they have accepted responsibility for the entire content of this submitted manuscript and approved submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dong, Y., Bai, L., Cai, R. et al. Visceral adiposity index performed better than traditional adiposity indicators in predicting unhealthy metabolic phenotype among Chinese children and adolescents. Sci Rep 11, 23850 (2021). https://doi.org/10.1038/s41598-021-03311-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-03311-x
This article is cited by
-
Comparison of the ability of HOMA-IR, VAI, and TyG indexes to predict metabolic syndrome in children with obesity: a cross-sectional study
BMC Pediatrics (2023)
-
Bone mineral density saturation as influenced by the visceral adiposity index in adults older than 20 years: a population-based study
Lipids in Health and Disease (2023)
-
Age-specific trend and birth cohort effect on different histologic types of uterine corpus cancers
Scientific Reports (2023)
-
Visceral fat and cardiometabolic future in children and adolescents: a critical update
Pediatric Research (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
