
Abstract
Psychological and mental health consequences of large-scale anti-contagion policies are assuming strong relevance in the COVID-19 pandemic. We proposed a specific focus on a large sample of children with Autism Spectrum Disorder (ASD), developing an ad hoc instrument to investigate changes occurred in specific (sub-)domains during a period of national lockdown (Italy). Our questionnaire, named AutiStress, is both context-specific (being set in the COVID-19 pandemic scenario) and condition-specific (being structured taking into account the autistic functioning peculiarities in the paediatric age). An age- and gender-matched group of neurotypical (TD) controls was also provided. As expected, the severe lockdown policies had a general negative impact both on ASD and TD children, reflecting the obvious burden of the pandemic situation. However, our findings also indicate that children with ASD experienced more positive changes than TD ones. Noteworthy, we report a thought-provoking double dissociation in the context-specific predictor (i.e., accessibility to private outdoor spaces), indicating that it impacts differently on the two groups. Focusing on the ASD group, results suggest a condition-specific impact of the COVID-19 pandemic on core autistic (sub-)domains. Taken together, our data call for a multi-layered, context- and condition-specific analysis of the pandemic burden beyond any oversimplification.
Similar content being viewed by others

Introduction
No doubt that the health, social and economic cost of the COVID-19 pandemic has had a worldwide impact on our lives, and it deeply set the course of biomedical research in 2020 providing extraordinary rapid insights on the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) biology, diagnostics, and treatment1,2,3. Among the most insidious indirect effects of this pandemic, there are psychological and mental health consequences of large-scale anti-contagion policies4,5,6.
Epidemic modelling on virus spread is crucial to balance the significant beneficial health outcomes of extensive anti-contagion policies in slowing the growth rate of infections and their unavoidable psycho-socio-economic cost7,8. Although it is ideally clear that decision-makers should balance health benefits of these policies and psycho-socio-economic consequences of restrictions, how this should be practically provided is extremely challenging and highly debated9,10,11. This balance is even more complex to achieve when we deal with vulnerable populations such as, for example, individuals with previous history of neuropsychiatric conditions that for multifaceted factors may be potentially more affected by the pandemic12. Here, we propose a specific focus on a well-characterized sample of children with Autism Spectrum Disorder (ASD) living in the Northern Italy (Lombardy region), that has been one of the first and major pandemic epicenters in Europe13. This will provide not only additional insights on this extremely complex and multi-layered balance, but it offers the unique possibility to explore the impact of unprecedented restriction measures on children with ASD using a clinically driven approach based on peculiarities of the autistic functioning.
Following the initial mild restrictions circumscribed to specific areas (notably the Lombardy region), in 2 weeks (8th–22nd March, 2020) the Italian government implemented a series of more and more severe public-health measures. These anti-contagion policies took shape a scenario of initially local and then national lockdown8,14. Since May 2020, easing restrictions have been gradually provided allowing for example outdoor workout and the reopening of commercial activities. This scenario circumscribes the so-called COVID-19 first wave, and we limit our analysis to this specific period. Italian anti-contagion policies have been considered among the most stringent by the Oxford COVID-19 Government Response Tracker (OxCGRT), an index collecting information on country-specific governmental responses11.
ASD is an early emerging neurodevelopmental condition characterized by heterogenous phenotypical manifestations in the social domain, restrict and repetitive patterns of behaviours, and peculiarities in the sensory processing15,16. Beyond this largely shared agreement about the generic clinical features, both the pathophysiology and subtler phenotypical aspects of ASD are far to be fully clarified. Noteworthy, recent clinical and experimental approaches raised the hypothesis that inflexibility of learning/thinking/acting may represent a key component in explaining the heterogenous range of autistic behavioural and neurocognitive manifestations17,18,19,20. This phenomenology of the autistic phenotypes helps to overcome the simplistic view of ASD as a condition primarily characterized by social difficulties. In turn, it suggests that the constellation of behavioural “social” symptoms may represent an epiphenomenon of more radical peculiarities in dealing with the social dynamics, potentially reflecting (or reflected by) atypicalities in sensory, perceptual, and motor functioning21,22,23. Most refined clinical approaches on ASD seem to imply that the autistic functioning (i.e., the ASD individuals’ peculiar way of learning/thinking/acting) should be considered to evaluate the impact of potentially stressful situations. Thus, both the unprecedented pandemic COVID-19 scenario and the underestimated peculiarities of the autistic functioning call for a tailored approach in investigating the consequences of severe lockdown policies in our children with ASD sample. For these reasons, we provided an ad hoc questionnaire, named AutiStress, to explore the pandemic impact in a spectrum of domains, each characterized by specific sub-domains ultimately referring to distinct types-of-change (Table S1). Notably, this framework differentiates core Vs. non-core autistic features that basically reflect domains or sub-domains specifically/non-specifically ascribable to the autistic functioning. This aimed to go beyond the largely foreseeable and simplistic conclusions about a generic negative impact of the pandemic. To do it, we tried to control as well as possible the assessment, focusing on a well-characterized sample of children with ASD, with a relatively limited range of age, living in a well-defined geographic area in which the anti-contagion policies applied by the government were identical and the perceived general pandemic burden comparable. In addition, all children with ASD received readapted and personalized remote clinical support during the pandemic by our clinical staff. To minimize confound effects, we limit data collection to an initial tight window in which the anti-contagion policies were most severe (3rd–29th April, 2020). Noteworthy, we considered not only usual variables (e.g., age, cognitive level) but also particular ones taking into account the contextual stay-at-home scenario (e.g., access to private outdoor space). A group of neurotypical children was also provided as control group.
A priori, negative effects of the lockdown policies on our pediatric ASD sample were surely expected, in agreement with seminal perspective views24, and also in line with first empirical reports in the literature25,26,27,28. One may hypothesize that the strict adherence to routines frequently reported in children with ASD may be affected by sudden restrictions, and these may also prevent the access to usual reinforcers (e.g., swimming, going to the playground) with cascade negative effects on children with ASD’s compliance in daily-life activities or homework. However, and going beyond a simplistic and monolithic approach to this complex scenario, children may also benefit from limited contextual/external stimulations. AutiStress tries to tackle this complex and multi-layered scenario without neglecting the peculiarities of the autistic functioning, aiming to provide useful insights to manage the current pandemic, and also unwanted (but unfortunately not unrealistic) future emergency situations.
Methods
Participants
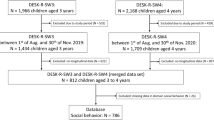
The final sample included 178 children with ASD (mean age ± SD = 5.44 ± 1.81 years, age range 2–9 years, males = 146) and 86 typically developing (TD) children (mean age ± SD = 5.00 ± 1.56 years, age range 2–9 years, males = 63). No differences between the ASD and the age- and gender-matched TD group were found on demographic variables (age: p = 0.06; gender: p = 0.10). Please note that the initial sample consisted of 178 children with ASD and 150 TD children (mean age ± SD = 3.92 ± 1.92 years, males = 81). Due to significant inter-group differences in age and gender variables (both ps < 0.001), we age- and gender-matched the two samples. Being the effects of severe anti-contagion policies on the ASD group our main focus, we chose to keep constant the ASD sample to maximise statistical power in ASD intra-group analyses. All children with ASD were in charge at the Scientific Institute IRCCS Medea (Bosisio Parini, Lecco; Italy) following distinct clinical protocols. Noteworthy, all children included in this sample continued to receive readapted and personalized remote clinical support by our clinical staff also during the most severe pandemic phases. IRCCS Medea is a renowned paediatric research hospital specialized in neurological, neuropsychiatric and neurodevelopmental disorders. Child Psychopathology Unit at the IRCCS Medea represents a unique and privileged observatory for ASD in Italy. It is recognized as “Pivot Center” for early detection and intervention in the Lombardy Region, and it has specific clinical departments using gold-standard clinical procedures for diagnosis (> 250 new ASD diagnosis per year) and behavioural evidence-based protocols for rehabilitation (e.g., NOAH project, New Organization for Autism Healthcare: ≈ 280 children with ASD between 2–6 years old enrolled in a 3-year program). In sum, our inclusion criterion for the ASD sample was the fact to be in charge at the IRCCS Medea in one of the clinical rehabilitative protocols for ASD (being formal diagnosis of ASD the prerequisite for accessing to these protocols). Concerning the TD group, we collected data in an anonymous way, and parents were requested to declare no prior history of psychiatric or neurological disorders in their children. We excluded any subjects for which parents declared any neurological or psychiatric diagnosis.
The study was approved by the IRCCS E.Medea-Ethical Committee, and it was conformed to the principles elucidated in the Declaration of Helsinki. Parents/legal guardians of all patients signed informed consent.
AutiStress questionnaire: structure and coding
AutiStress questionnaire is an ad hoc created parent-report instrument that we originally developed and distributed in Italian (in the interest of international readers, we also provide an English version of the questionnaire in Table S1. Cfr. Supplementary Materials for details). AutiStress was developed to investigate changes occurred in specific domains and sub-domains (also defined as types-of-change) following the severe anti-contagion movement restrictions policies. It is context-specific being set in the COVID-19 pandemic scenario, and condition-specific being structured taking into account the autistic functioning peculiarities in the paediatric age. Thus, we differentiated core Vs. non-core autistic features (both in domains and in sub-domains) according to the idea that ASD is not a condition primarily characterized by phenotypical “social” manifestations. AutiStress was distributed using Google Forms between 3rd and 29th April, 2020.
After a preliminary description of the aims of the study, we collected general basic socio-demographic information. Notably, we asked about the house characteristics considering that accessibility to outdoor spaces may be a critical factor during a period characterized by severe movement restrictions. To maximize statistical power and to avoid misattributions due to ambiguous situations, we merged the four choices using a handy dichotomization between apartment regardless of the presence of the balcony (hereafter, apartment) and home with access to private outdoor spaces (hereafter, private garden).
We structured our requests into seven domains referring both to core autistic features (Sensory Interests; Repetitive Behaviours) and non-core ones (Mood; Play; Eating Behaviour; Circadian Rhythm Sleep; Bowel and Bladder Control). For each domain, parents were asked to report—if any—children’s behavioural changes as compared to pre-pandemic situation (e.g., “Did your child show any change in his/her mood? [yes/no]”). Following a negative answer, the online form moved to the subsequent domain. On the contrary, if parents replied positively in that domain they were asked to rate on a 5-point Likert scale how frequently several domain-related types-of-change occurred. Being a questionnaire that synergistically combined the efforts of clinicians engaged in remote support protocols and researchers, certain AutiStress requests were primarily driven by clinical purposes (notably to provide prompt and comprehensive monitoring for potential behavioural changes, even in less expected spheres). This was the case for example of the Bowel and Bladder Control domain, that was not extensively explored in our analyses due to very limited frequencies (12% in ASD group, 3% in TD group). Similarly, we simplified the Sensory Interests domain focusing exclusively on the main question (related to presence or absence of any change concerning sensory interests), without furtherly analysing sub-domains (i.e., each sense).
Statistical analysis
Given the different nature of dependent variables between domains (dichotomous) and sub-domains/types-of-change (Likert scale), we tested our predictors of interest with different statistical models in Jamovi.
Domains
Generalized linear models were implemented to test main and interaction effects29. Group (ASD Vs. TD) and House-Characteristics (apartment Vs. private garden) entered in the model as dichotomous predictors, and Age as continuous covariate. The Group*House-Characteristics interaction also entered in the model. Moreover, for each sample we tested the effects of House-Characteristics and Age, in order to further assess the specific impact of these predictors within-group. In addition, being available children with ASD’s cognitive functioning measures from pre-pandemic clinical records, in the ASD group we ran the analysis also considering the Cognitive Level as a covariate. This predictor was dichotomized into ‘intellectual-disability’ Vs. ‘no-intellectual-disability’, to overcome variability in instruments used to measure cognitive functioning.
Sub-domains (types-of-change)
Analyses on the sub-domains were performed only on the residual sample of children reporting changes in the correspondent domain. Multiple linear regression models were implemented to test potential change in each sub-domain. Except for the Group*House-Characteristics interaction, which was not included here due to the small number of responses for some combinations of the levels of the two factors, for the analysis of the sub-domains we used the same predictors set that we used for the analysis of the domains. If the assumption of normality (K-S test) of the residuals was violated, then we dichotomized the continuous dependent variable into presence (i.e., from “1” to “4”) or absence (i.e., “0”) of change. Being sub-domains generally characterized by low frequencies in the right side of the Likert scale (i.e., responses “3–4”), we collapsed responses from “1” to “4”. Then a generalized linear model was used. We anticipate that, due to their peculiar nature, the Mood sub-domains were analysed somewhat differently from the other sub-domains (“Changes in non-core autistic features” section).
As we observed missing values, we also tested the hypothesis that missing data were randomly distributed (Missing Completely At Random–MCAR Analysis). If missing values were detected within at least one sub-domain, we ran the MCAR analysis within the correspondent domain. Control analyses confirmed that data are missing completely at random (Circadian Rhythm Sleep: p = 0.09; Eating Behaviour: p = 0.15; Play: p = 0.14; Mood: p = 0.62). No missing values were found in Repetitive Behaviour domain.
Results
Results are presented according to the condition-specific and context-specific hallmarks of AutiStress. Thus, we focus on the core Vs. non-core autistic features distinction, making reference both to specific core autistic domains and sub-domains. In addition, we focus on the House-Characteristics predictor to consider peculiarities of the COVID-19 pandemic scenario. Nevertheless, detailed significant results that do not fall into this conceptual and clinically-driven framework are reported in Tables S2, S3, S4.
Changes in non-core autistic features
Mood domain represents an unspecific and non-core autistic feature that may reliably help in characterizing the burden of the pandemic scenario both for ASD and TD children. We did not find Group difference in reporting changes in this domain (ASD: 50%[88/176]; TD: 48%[41/86]; LRT-χ2 = 0.08, p = 0.78) (Fig. 1a,b), nor any other significant effect of House-Characteristics (LRT-χ2 = 0.10, p = 0.75), Age (LRT-χ2 = 1.86, p = 0.17) or Group*House-Characteristics (LRT-χ2 = 0.62, p = 0.43). Concerning the within-group analyses, no significant effects of any predictor were found neither in the ASD nor in the TD group (ASD group: House-Characteristics LRT-χ2 = 0.75, p = 0.39; Age LRT-χ2 = 0.51, p = 0.48; Cognitive Level LRT-χ2 = 0.12, p = 0.73; TD group: House-Characteristics LRT-χ2 = 0.05, p = 0.83; Age LRT-χ2 = 1.86, p = 0.17).

(a) Graphs illustrating TD children (48% [41/86]) that are reported to show changes in the Mood domain. (b) Graphs illustrating ASD children (50% [88/176]) that are reported to show changes in the Mood domain. (c) Graphs representing intra-group and inter-group comparisons in the mean negative and in the mean positive mood changes. Intra-group comparisons show that both ASD and TD children reported more mean negative than mean positive changes in mood (ASD group: p = 0.005; TD group: p = 0.004). Interestingly, there is no inter-group difference in the mean negative mood changes (ASD group: 1.78 ± 0.87; TD group: 1.49 ± 0.66; p = 0.10), but children with ASD reported more positive mood changes than TD children (ASD group: 1.31 ± 0.86; TD group: 0.97 ± 0.96; p = 0.019).*Statistical significance, p < 0.05; **statistical significance, p < 0.01; ns = no statistical significance. Bars represent standard errors of the mean (SEM).
Considering their peculiar nature, the Mood sub-domains were analysed differently from the other sub-domains. Specifically, instead of analysing separately the types-of-change, we first grouped them based on their positive Vs. negative value (Table S1). In other words, we averaged all the intra-subjects negative and all the intra-subjects positive mood changes. This allowed us to obtain valuable general information about positive and negative mood changes, independently of the specific nature of these changes. Because neither mean positive nor mean negative mood changes were normally distributed (ps < 0.01), we used Wilcoxon Paired Tests to compare ranks of mean positive Vs. mean negative differences in mood changes within each group. The results showed that both ASD and TD children reported more mean negative than mean positive changes in mood (ASD[N = 84]: 1.79 ± 0.86 > 1.30 ± 0.87, W = 2213, p = 0.005; TD[N = 40]: 1.50 ± 0.67 > 0.97 ± 0.96, W = 595, p = 0.004) (Fig. 1c).
In order to test the possible effect of the Group predictor on mean negative and mean positive mood changes, we used two separate Mann Whitney U-tests. If the U-test indicated a statistically significant effect of Group on the mean positive (mean negative) change, then we conducted a regression analysis with predictors Group, House-Characteristics, and Age on each of the positive (negative) type-of-change. Specifically, we used a generalized linear model if the assumption of normality of the residuals was violated and a simple linear model otherwise. In other words, analyses on the positive (negative) types-of-change were performed only if the Group predictor had a statistically significant effect on mean positive (mean negative) mood changes. In line with this post-hoc logic, we adjusted the significance threshold according to Bonferroni correction (Positive mood changes significant threshold: p = 0.05/3 = 0.017; negative mood changes significant threshold: p = 0.05/6 = 0.008). Note that, although these post-hoc analyses were focused on the possible effects of the Group predictor on each type-of-change, we also entered House-Characteristics and Age in the models in order to control for possible spurious correlation effects.
No effect of the Group predictor (ASD Vs. TD) emerged in the mean negative mood changes (ASD[N = 86]: 1.78 ± 0.87; TD[N = 41]: 1.49 ± 0.66; U = 1446, p = 0.10). In contrast, a distinct pattern between the ASD and TD group was found in the mean positive mood changes, with ASD children reporting more positive changes than TD ones (ASD[N = 86]: 1.31 ± 0.86; TD[N = 40]: 0.97 ± 0.96; U = 1279, p = 0.019) (Fig. 1c). In particular, post-hoc analysis on positive types-of-change revealed that ASD children were reported to show more changes than TD children in the more calm (ASD[N = 84]: 1.32 ± 1.02; TD[N = 39]: 0.69 ± 0.86; β = 0.76; p < 0.001), in the more helpful (ASD: 81%[67/83]; TD: 56%[22/39]; LRT-χ2 = 13.42, p < 0.001) and in the more cooperating behaviours (ASD: 73%[62/85]; TD: 63%[25/40]; LRT-χ2 = 4.57, p = 0.032) sub-domains.
The possible effects of the House-Characteristics predictor (private garden Vs. apartment) and of the Age predictor on the mean positive and mean negative mood changes were separately analysed using the same logic as for the Group predictor. The effects of both predictors were tested separately on the TD and ASD group. Consistently with the choice of using the Mann Whitney U-test, the Age predictor was dichotomized (i.e., children ‘ < 6 y.o.’ and ‘ ≥ 6 y.o.’). As for the House-Characteristics factor, in the TD group we found a significant effect in the mean positive mood changes (private garden[N = 18]: 1.41 ± 0.97, apartment[N = 22]: 0.61 ± 0.80; U = 103, p = 0.008), and no significant effect in the mean negative mood changes (private garden[N = 18]: 1.73 ± 0.70, apartment[N = 23]: 1.30 ± 0.58; U = 138, p = 0.068) (Fig. 2a). Post-hoc analysis on positive types-of-change, with predictors House-Characteristics and Age, revealed that TD children having access to private outdoor places were reported to show more changes in the more calm (private garden: 71%[12/17]; apartment: 32%[7/22]; LRT-χ2 = 5.83, p = 0.016) and in the more cooperating behaviours (private garden: 89%[16/18]; apartment 41%[9/22]; LRT-χ2 = 10.60, p = 0.001) sub-domains. Also the more helpful sub-domain showed a comparable trend (private garden: 76%[13/17]; apartment: 41%[9/22]; LRT-χ2 = 5.04, p = 0.025), but it did not survive to the multiple comparison threshold (fixed at p = 0.017). No House-Characteristics significant effects were reported in the ASD group, neither on mean positive (private garden[N = 27]: 1.43 ± 0.97; apartment[N = 59]: 1.26 ± 0.81; U = 710, p = 0.42) nor on mean negative mood changes (private garden[N = 26]: 1.96 ± 0.86; apartment[N = 60]: 1.69 ± 0.87; U = 634, p = 0.17).

(a) Graphs illustrating the effects of House-Characteristics (private garden Vs. apartment) on the mean negative and mean positive mood changes within the TD group (p = 0.008). (b) Graphs illustrating the effects of Age (‘ ≥ 6 y.o.’ Vs. ‘ < 6 y.o.’) on the mean negative and the mean positive mood changes within the ASD group (p = 0.024). *Statistical significance, p < 0.05; **statistical significance, p < 0.01; ns = no statistical significance. Bars represent standard errors of the mean (SEM).
Concerning the Age predictor (‘ < 6 y.o.’ Vs. ‘ ≥ 6 y.o.’), in the ASD group we found a significant effect in the mean positive mood changes (‘ < 6 y.o.’[N = 43]: 1.54 ± 0.75; ‘ ≥ 6 y.o.’[N = 43]: 1.08 ± 0.92; U = 666, p = 0.024), and no significant effect in the mean negative mood changes (‘ < 6 y.o.’[N = 43]: 1.66 ± 0.82; ‘ ≥ 6 y.o.’[N = 43]: 1.89 ± 0.91; U = 789, p = 0.24) (Fig. 2b). In particular, regression analysis on the positive types-of-change with predictors Age (continuous), House-Characteristics, and Cognitive Level revealed that changes in the more helpful (β = -0.37; p < 0.001), in the more calm (β = -0.26; p = 0.015), and in the more cooperating behaviours (β = -0.34; p = 0.002) sub-domains tended to decrease with ASD children’s age. No significant effects of Age were reported in the TD group neither on mean positive (‘ < 6 y.o.’[N = 28]: 1.02 ± 1.04; ‘ ≥ 6 y.o.’[N = 12]: 0.83 ± 0.75; U = 162, p = 0.86) nor on mean negative mood changes (‘ < 6 y.o.’[N = 28]: 1.47 ± 0.64; ‘ ≥ 6 y.o.’[N = 13]: 1.53 ± 0.74; U = 170, p = 0.75).
Finally, concerning the Cognitive Level predictor (‘intellectual-disability’ Vs. ‘no-intellectual-disability’), in the ASD group no significant effects were found neither on mean positive (‘intellectual-disability’[N = 54]: 1.42 ± 0.89; ‘no-intellectual-disability’[N = 32]: 1.14 ± 0.80; U = 699, p = 0.14) nor on mean negative (‘intellectual-disability’[N = 54]: 1.71 ± 0.89; ‘no-intellectual-disability’[N = 32]: 1.88 ± 0.84; U = 770, p = 0.40) mood changes.
Changes in core autistic features
Core autistic features reflect domains and sub-domains ascribable to the autistic functioning. Analyses aimed to test if context-specific critical variables have an impact on condition-specific (sub-)domains.
We found Group (ASD Vs. TD) differences in reporting changes in the Sensory Interests (ASD: 25%[44/176]; TD: 3%[3/86]; LRT-χ2 = 17.31, p < 0.001) and Repetitive Behaviours (ASD: 29%[52/178]; TD: 3%[3/86]; LRT-χ2 = 24.93, p < 0.001) domains. Among the types-of-change more specifically reflecting core autistic characteristics, we found that ASD children were reported to show more changes than TD ones in the food selectivity (ASD: 68%[26/38]; TD: 22%[4/18]; LRT-χ2 = 11.19, p < 0.001), and in the difficulties with transition (ASD[N = 77]: 1.91 ± 1.18; TD[N = 25]: 0.72 ± 1.02; β = 0.84; p < 0.001) sub-domains.
As expected, the number of TD children showing any changes in the autistic core (sub-)domains was basically negligible. Thus, we proposed a specific intra-group focus on the ASD sample. This choice was also justified by the fact that these (sub-)domains refer to aspects taken into account during clinical rehabilitative protocols, therefore children with ASD’s parents are familiar with them. In contrast, they may appear less transparent for neurotypical children’s parents. Although we clinically hypothesized a potential beneficial effect of accessing to private outdoor spaces on core autistic domains, the effect of House-Characteristics (apartment Vs. private garden) did not attain (Repetitive Behaviours, apartment: 32%[38/118]; private garden: 23%[14/60]; LRT-χ2 = 2.12, p = 0.15) or at-best approached the statistical significance level (Sensory Interests, apartment: 29%[34/116]; private garden: 17%[10/60]; LRT-χ2 = 3.35, p = 0.067). Driven by the clinical hypothesis that considers patterns of repetition and sensory processing peculiarities in ASD as potentially related to a common atypical functioning30, we set an additional variable testing the co-occurrence of changes in at-least-one domain (Repetitive Behaviours and/or Sensory Interests). This new variable confirmed that House-Characteristics predictor (apartment Vs. private garden) significantly modulate sensorial and repetitive patterns changes, as ASD children living in apartment were reported to show more changes in Repetitive Behaviours and/or Sensory Interests (apartment: 45%[53/118]; private garden: 30%[18/60]; LRT-χ2 = 4.41, p = 0.036) domains (Fig. 3a).

(a) Graphs illustrating the effects of House-Characteristics (apartment Vs. private garden) on Repetitive Behaviours and/or Sensory Interests domains within the ASD group (p = 0.036). (b) Graphs illustrating the effects of House-Characteristics (apartment Vs. private garden) on the self-stimulation sub-domain within the ASD group (p = 0.029). *Statistical significance, p < 0.05. Bars represent standard errors of the mean (SEM).
Among the types-of-change specifically reflecting core autistic features, the House-Characteristics predictor (apartment Vs private garden) similarly impacted on self-stimulation (apartment[N = 34]: 2.59 ± 0.86; private garden[N = 13]: 1.69 ± 1.11; β = 0.66; p = 0.029), denoting again that children without access to private garden were reported to show more changes (Fig. 3b). Notably, we also found a significant Age effect on self-stimulation (β = 0.36; p = 0.008), indicating that older children were reported to show more changes in this sub-domain.
Discussion
Governments worldwide are trying to face this pandemic providing health policies that balance distinct aspects such as epidemiological situation, socioeconomic and biopolitics factors10,11,31. Although expression “unprecedented times” is becoming a sort of cliché in the COVID-19 era32, are we really transferring this idea and the burden of its implications in the mental health clinical settings? Are we really dealing with the lockdown effects on individuals with ASD taking into account the unique scenario of COVID-19 pandemic? AutiStress tries to tackle this point balancing peculiarities of the current situation, the body of knowledge on ASD (≈ autistic functioning), and notably the interaction of these aspects.
Our first result concerns the Mood domain, that refers to an unspecific and non-core autistic feature. As expected, the severe lockdown policies in Italy had a general negative impact both on children with ASD and neurotypicals controls. This generic and unsurprising result reflects the obvious burden of the pandemic situation, and it was a widely predictable effect of unpleasant (but undelayable) movement restrictions. Notably, we found that mean negative mood changes were higher than mean positive ones in each group (see also Tables S5, S6). This suggests that the effect was not condition-specific for the ASD group whereas it is shared also by our neurotypical pediatric sample, in agreement also with previous reports on clinical/non-clinical populations4,5,6. However, and importantly considering AutiStress aims, children with ASD reported more positive mood changes than TD children (Fig. 1c); notably, they have been reported to show more changes in the more calm, in the more helpful, and in the more cooperating behaviours sub-domains. Although the mainstream view tended to focus on the presumed amplified burden in ASD25,27,28, the possibility that our clinical sample may experience also positive changes during the COVID-19 pandemic cannot be considered totally unexpected. As outlined in the Introduction, children with ASD may have benefited from reduced stressful situations (e.g., public transports, mandatory school activities) and from new more manageable home-based routines. This may be particularly plausible in our ASD sample, considering that all children pursued readapted remote clinical intervention provided also during the more critical period. This may have guaranteed at least basic continuity of care, notably supporting parents in structuring and managing daily activities, and it is consistent with other recent reports describing beneficial effects of remote/telehealth programs in ASD33,34,35. Our data also suggest an interesting double dissociation in modulating positive mood changes between the two groups (Fig. 2). Age seems to explain positive changes in the ASD group, with younger children reported to show more changes in the more calm, in the more helpful, and in the more cooperating behaviours sub-domains. These findings may partially reflect a sort of “protective” role of age, being younger children naturally less aware of the situation, and also the new home-based routines established by caregivers supported by our clinical staff (see also36). In contrast, Age does not seem to play a critical role in explaining positive changes in the TD group. Intriguingly, an additional dissociation emerged for the House-Characteristics predictor that significantly predict positive changes in the TD group. Children with access to private outdoor spaces were reported to show more changes in the more calm and in the more cooperating behaviours sub-domains. In contrast, House-Characteristics does not seem to play a role in explaining positive changes in the ASD group. Taken together, results on the Mood domain depict a scenario largely consistent with the previous literature, with obvious negative effects of the severe anti-contagion policies impacting both on ASD and TD children. However, the double dissociation on positive changes may assume strong theoretical and clinical significance taking into account the autistic functioning peculiarities, and notably the distinction between core Vs. non-core autistic features.
A very timely report faced the challenge of setting up remotely readapted protocols37. This report has the merit of pushing readers in considering the peculiar core of the autistic phenotype, and nicely fits with the AutiStress purpose of differentiating changes in core Vs. non-core autistic features. Thus, our second major finding concerns a condition-related impact of severe anti-contagion policies on specific core autistic features. We found that children with ASD reported changes more often than TD controls in the Sensory Interests and Repetitive Behaviours domains. In addition, children with ASD reported significantly more changes than controls in food selectivity and in difficulties with transitions, that represent two prototypical sub-domains related to the autistic functioning (i.e., inflexibility, rigidity). From the one side, it is not surprising that neurotypical children basically did not present any changes in these aspects, and likely these requests may have appeared less transparent for neurotypical children’s parents. However, percentages and rough proportion in the ASD sample clearly indicate relevant changes compared to pre-pandemic period in these condition-specific aspects. Intriguingly, a subtler and deeper analysis of our ASD sample suggests an additional thought-provoking dissociation with the neurotypical control group. Considering ASD children reporting changes in at-least-one of the autistic core domains (Sensory Interests and/or Repetitive Behaviours), a significant effect of House-Characteristics emerged. Moreover, House-Characteristics significantly impacts on a sub-domain distinctive of the autistic functioning such as self-stimulation (Fig. 3). Results on House-Characteristics in the ASD sample hint at refined and clinically insightful perspective-shift. Our suggestion is that a context-specific critical variable may have a relevant impact on condition-specific (sub-)domains (i.e., core autistic features for the ASD group), whereas it would impact on a more general and unspecific domain such as Mood in neurotypical controls. A provocative hypothesis is that Mood domain for TD children corresponds to core autistic domains for the ASD group, as it was the “core neurotypical domain”. Although this remains a rather speculative hypothesis, our results clearly indicate a different effect of context-specific protective factors, and implicitly call for a multi-layered, condition-specific and less simplistic analyses of complex phenomena. Having access to private outdoor places reasonably represents a critical variable during severe lockdown. Potential mental health and well-being benefits of time spent outside in natural environments have been largely hypothesized in the literature38, notably in coping with strict movement restrictions39. Countries such as Italy and Spain promoted very restrictive lockdown policies in which people basically were not allowed to leave their homes except for healthy (e.g., brief outside walks were permitted in the Lombardy region for people with severe mental health disorders or intellectual disabilities, provided that the caregiver presented a written certificate signed by the clinical mental health specialist, see37), emergency or essential job reasons, for buying food and medicines, or—in certain cases—walking the dog. Even in a scenario of national lockdown, other countries permitted at least limited access to nature or public outdoor spaces for recreational activities (e.g., France, UK). Thus, accessibility to private outdoor spaces (e.g., private garden) is likely more critical in areas, such as Italy or Spain, in which not even limited access to public park or greenspace was permitted. This hypothesis not only drove our choices in AutiStress of controlling house characteristics, but it also nicely fits with the findings recently reported in a large sample of 3403 individuals from Spain39. The authors tested the potential resilient effect of the residual contact with the nature, and results suggest that having access to private outdoor spaces and window views of natural features (as a proxy of indirect contact with nature, see40) can act as a protective factor against negative consequences of severe stay-at-home restrictions. Without underestimating or even neglecting the role of other critical moderators (e.g., socio-demographic factors, personal circumstances), accessibility to private outdoor places may effectively represent a relevant factor in this pandemic. Accordingly, also our results indicate that private garden availability plays a role in coping the strict movement restrictions policies. More interestingly for our aims, we showed that children with ASD and neurotypical controls seem to be impacted differently from this modulator factor, as if it acted primarily on each individual’s more “sensible” spheres. Here again, no doubt that House-Characteristics is not the only ingredient modulating individual reaction to the pandemic. For children with ASD a primary role was also played by familiar coping strategies, eventually supported by remote programs guaranteeing continuity of cares.
Finally, a methodological point deserves to be underlined. It would be virtually meaningless considering each (sub-)domain per se, without a within-subject pre-/post-pandemic comparison. Two distinct approaches may solve this concern. The first one consists in the comparison of results on standardized questionnaires used during periodic clinical follow-up (as proxy of pre-pandemic timepoint) with a new re-evaluation ideally administered just before the relaxing of restrictions (as proxy of post-lockdown timepoint)41,42,43. This strategy has the undeniable advantage of using standardized instruments, however these instruments are not context-specific and usually not even condition-specific. A second alternative approach consists in ad hoc questionnaires. AutiStress clearly accompanied the respondents to not consider absolute rate for each (sub-)domain, whereas we drove them in focusing on potential changes in relation to pre-pandemic period. Noteworthy, AutiStress is context-specific: it is tailored to the COVID-19 pandemic situation (e.g. effects of enforced stay-at-home orders), and this inspired us in using ad hoc predictor (e.g., House-Characteristics) that would not be so befitting in other emergency contexts such as wars or natural disasters areas. AutiStress is also condition-specific: it is based on a renovated clinical framework that considers sensory processing and behavioural rigidity as the key components of ASD (≈ autistic functioning) that, in turn, inspired us in differentiating core Vs. non-core autistic features. Finally, asking for changes we implicitly “controlled” for a sort of individual threshold, and this helps to explain the modest impact of ASD children’s cognitive level in our results. At first glance this result may appear weird, being clinically well-established that certain components are normally more pronounced in ASD children with lower cognitive abilities (e.g., self-stimulation for which—indeed—results indicate a non-significant trend). Thus, we speculate that the emphasis on reporting changes may explain the absence of any significant results of the cognitive level (domains, all ps > 0.22; sub-domains, all ps > 0.11).
Conclusion
The health, social and economic cost of COVID-19 pandemic is impressive4,5,6,7,8,9,12,24,25,26,27,28,33,34,35,36,37,41,42,43,44, and by now no one can fully evaluate neither short- nor long-term effects in a reliable way. Although our work offers only a very specific and circumscribed view, we hope this may contribute to improve global attention also to the (a)typical mental health impact of COVID-19 pandemic.
We intended AutiStress both as a case-specific instrument and a potentially replicable tool, as long as specific (but finally minimal) adaptations are provided. AutiStress strengthens the idea that we would benefit from an approach that considers seriously the autistic functioning and its learning/thinking/acting peculiarities, since extraordinary situations may selectively impact on them. This does not imply that more classical works focusing on general mental health symptoms regardless of the specificities of the clinical population are less informative, in light for example of the clear benefit of having access to standardized instruments. We simply state that they are not enough, and we should promote convergent/combined approaches that consider both perspectives. Similarly, facing an “unprecedented” emergency scenario we need peculiar contextual constraints (e.g., access to outdoor space). How we act and interact in the world is a puzzle even during golden age periods. Promoting the best possible equilibrium between safe and effective social dynamics during this pandemic time seems to be a matter of titanic importance both for neurotypical and autistic population. We are all main characters of this challenge.
Data availability
Materials and data generated during the current study and supporting the findings of this article are available from the corresponding authors upon reasonable request.
References
Callaway, E., Ledford, H., Viglione, G., Watson, T. & Witze, A. COVID and 2020: An extraordinary year for science. Nature 588(7839), 550–552 (2020).
Meyerowitz, E. A., Richterman, A., Bogoch, I. I., Low, N. & Cevik, M. Towards an accurate and systematic characterisation of persistently asymptomatic infection with SARS-CoV-2. Lancet Infect. Dis. 2, 1–7 (2020).
Viner, R. M. et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: A systematic review and meta-analysis. JAMA Pediatr. 175(2), 143–156 (2021).
Shi, L. et al. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA Netw. Open 3(7), e2014053 (2020).
Ettman, C. K. et al. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw. Open. 3(9), e2019686 (2020).
Xie, X. et al. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei province, China. JAMA Pediatr. 174(9), 898–900 (2020).
Flaxman, S. et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 584(7820), 257–261 (2020).
Hsiang, S. et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 584, 262–267 (2020).
Han, E. et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 396, 1525–1534 (2020).
Benzell, S. G., Collis, A. & Nicolaides, C. Rationing social contact during the COVID-19 pandemic: Transmission risk and social benefits of US locations. Proc. Natl. Acad. Sci. USA. 117, 14642–14644 (2020).
Li, Y. et al. The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (R) of SARS-CoV-2: A modelling study across 131 countries. Lancet Infect. Dis 21(2), 193–202 (2021).
Moreno, C. et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 7, 813–824 (2020).
Villani, L., McKee, M., Cascini, F., Ricciardi, W. & Boccia, S. Comparison of deaths rates for COVID-19 across Europe during the first wave of the COVID-19 pandemic. Front. Public Health 8, 620416 (2020).
Farina, M. & Lavazza, A. Lessons from Italy’s and Sweden’s policies in fighting COVID-19: The contribution of biomedical and social competences. Front. Public Health 8, 1–6 (2020).
Lai, M., Anagnostou, E., Wiznitzer, M., Allison, C. & Baron-Cohen, S. Evidence-based support for autistic people across the lifespan: Maximising potential, minimising barriers, and optimising the person—environment fit. Lancet Neurol. 4422, 1–18 (2020).
Hyman, S. L., Levy, S. E. & Myers, S. M. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics 145(1), e20193447 (2020).
Black, K. R. et al. Linking anxiety and insistence on sameness in autistic children: The role of sensory hypersensitivity. J. Autism Dev. Disord. 47, 2459–2470 (2017).
Lawson, R. P., Mathys, C. & Rees, G. Adults with autism overestimate the volatility of the sensory environment. Nat. Neurosci. 20, 1293–1299 (2017).
Casartelli, L., Riva, M., Villa, L. & Borgatti, R. Insights from perceptual, sensory, and motor functioning in autism and cerebellar primary disturbances: Are there reliable markers for these disorders?. Neurosci. Biobehav. Rev. 95, 263–279 (2018).
Ronconi, L. et al. Altered neural oscillations and connectivity in the beta band underlie detail-oriented visual processing in autism. NeuroImage Clin. 28, 102484 (2020).
Wang, S. et al. Atypical visual saliency in autism spectrum disorder quantified through model-based eye tracking. Neuron 88, 604–616 (2015).
Robertson, C. E. & Baron-Cohen, S. Sensory perception in autism. Nat. Rev. Neurosci. 18(11), 671–684 (2017).
Casartelli, L., Federici, A., Biffi, E., Molteni, M. & Ronconi, L. Are we “motorically” wired to others? High-level motor computations and their role in autism. Neuroscientist 24, 568–581 (2018).
Narzisi, A. Handle the autism spectrum condition during coronavirus (COVID-19) stay at home period: Ten tips for helping parents and caregivers of young children. Brain Sci. 10(4), 207 (2020).
Colizzi, M. et al. Psychosocial and behavioral impact of COVID-19 in autism spectrum disorder: An online parent survey. Brain Sci. 10(6), 341 (2020).
Mutluer, T., Doenyas, C. & Aslan, G. H. Behavioral implications of the Covid-19 process for autism spectrum disorder, and individuals’ comprehension of and reactions to the pandemic conditions. Front. Psychiatry 11, 561882 (2020).
Bal, V. H. et al. Early pandemic experiences of autistic adults: Predictors of psychological distress. Autism Res. 14(6), 1209–1219 (2021).
White, L. C. et al. Brief report: Impact of COVID-19 on individuals with ASD and their caregivers: A perspective from the SPARK cohort. J. Autism Dev. Disord. 2, 1–8 (2021).
Gallucci, M. GAMLj: General analyses for linear models. [jamovi module] (2019).
Schulz, S. E. & Stevenson, R. A. Sensory hypersensitivity predicts repetitive behaviours in autistic and typically-developing children. Autism 23(4), 1028–1041 (2019).
Maxmen, A. Why did the world’s pandemic warning fail when COVID hit?. Nature 589(7843), 499–500 (2021).
Major, C. Unprecedented times and innovation. Innov. High Educ. 23, 1–2 (2020).
Brondino, N., Damiani, S. & Politi, P. Effective strategies for managing COVID-19 emergency restrictions for adults with severe ASD in a daycare center in Italy. Brain Sci. 10(7), 436 (2020).
Pollard, J. S., LeBlanc, L. A., Griffin, C. A. & Baker, J. M. The effects of transition to technician-delivered telehealth ABA treatment during the COVID-19 crisis: A preliminary analysis. J. Appl. Behav. Anal. 54, 87–102 (2021).
Tokatly Latzer, I., Leitner, Y. & Karnieli-Miller, O. Core experiences of parents of children with autism during the COVID-19 pandemic lockdown. Autism 25, 1047–1059 (2021).
Berard, M. et al. Impact of containment and mitigation measures on children and youth with ASD during the COVID-19 pandemic: Report from the ELENA cohort. J. Psychiatr. Res. 137, 73–80 (2021).
degli Espinosa, F., Metko, A., Raimondi, M., Impenna, M. & Scognamiglio, E. A. Model of support for families of children with autism living in the COVID-19 lockdown: Lessons from Italy. Behav. Anal. Pract. 13(3), 1–9 (2020).
White, M. P. et al. Spending at least 120 minutes a week in nature is associated with good health and wellbeing. Sci. Rep. 9(1), 7730 (2019).
Pouso, S. et al. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 756, 143984 (2021).
Keniger, L. E., Gaston, K. J., Irvine, K. N. & Fuller, R. A. What are the benefits of interacting with nature?. Int. J. Environ. Res. Public Health 10(3), 913–935 (2013).
Di Renzo, M. et al. Parent-reported behavioural changes in children with autism spectrum disorder during the COVID-19 lockdown in Italy. Continuity Educ. 1(1), 117–125 (2020).
Siracusano, M. et al. The impact of COVID-19 on the adaptive functioning, behavioral problems, and repetitive behaviors of Italian children with autism spectrum disorder: An observational study. Children 8, 96 (2021).
Siracusano, M. et al. COVID-19 and social responsiveness: A comparison between children with Sotos syndrome and autism. Psychiatry Res. 299, 113851 (2021).
TMGH-Global COVID-19 Collaborative. Perceived stress of quarantine and isolation during COVID-19 pandemic: A global survey. Front. Psychiatry. 12, 651 (2021).
Acknowledgements
This work was supported by the “5per1000” funds for biomedical research (Scientific Institute IRCCS Medea) to LC. The funders did not participate in the conception and development of this work. The contribution of the clinical staff of the Scientific Institute IRCCS Medea as well as of children and their families are gratefully acknowledged. The authors would like to thank Elisa Pini for her contribution.
Author information
Authors and Affiliations
Contributions
Conceptualization: L.F., L.V., L.C.; Data curation: L.F., M.N., V.R., M.V., L.C.; Formal analysis: M.N., V.R., M.V.; Methodology: L.F., M.V., L.C.; Clinical supervision: L.V.; General supervision: M.V., L.C.; Visualization: M.N.; Writing—original draft: M.N., M.V., L.C.; Writing—review and editing: L.F., L.V., V.R.; all authors read and approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fumagalli, L., Nicoli, M., Villa, L. et al. The (a)typical burden of COVID-19 pandemic scenario in Autism Spectrum Disorder. Sci Rep 11, 22655 (2021). https://doi.org/10.1038/s41598-021-01907-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-01907-x
This article is cited by
-
The Impact of COVID-19 on the Mental Health and Wellbeing of Children with Special Education Needs and Disabilities: A Systematic Review
Review Journal of Autism and Developmental Disorders (2024)
-
Distance learning during the COVID-19 pandemic for children with ADHD and/or ASD: a European multi-center study examining the role of executive function deficits and age
Child and Adolescent Psychiatry and Mental Health (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
