
Abstract
Lower limb amputation highly impacts the lives of individuals. The inability to walk due to difficulties in adapting to wearing prosthesis can potentially result in physical degeneration and comorbidity in this population. In this randomized clinical trial study, we investigated if a low-cost and easily implementable physiotherapy intervention was effective in improving gait performance and adaptation to lower limb prosthesis in individuals with an amputation. A total of 26 individuals participated in the study, 16 with lower limb amputation and 10 without amputation. Participants with amputation were further divided in intervention and control groups. The intervention group underwent a rehabilitation protocol aimed at strengthening muscles and improving prosthesis adaptation. Muscle strengthening targeted the hip segment, prioritizing the abdominal muscles, hip flexors, extensors, adductors and abductors, followed by cicatricial mobilization and weight-bearing on the stump for desensitization. Assessment and measures were performed across the kinetic and kinematic parameters of gait. In the comparison between pre-and post-intervention, a significant increase in gait speed (0.68—2.98, 95% CI, 1.83, effect size ES) and cadence (0.56—2.69, 95% CI, 1.63, ES) was found between groups and time points. Step (0.73—3.11, 95% CI, 1.92, ES) and stride length (0.62—2.84, 95% CI, 1.73) increased between pre- and post-intervention, while in the control group both variables remained smaller. The intervention group decreased stance phase as a percentage of gait cycle between pre- and post-intervention (− 1.33—0.62, 95% CI, − 36, ES), while it increased in the control group. Improvement in a combination of important gait parameters indicates that the intervention protocol promoted the adaptation to prosthesis and the functional independence of individuals with lower limb amputation. It is recommended that the participants continue receiving follow-up assessments and rehabilitation interventions.
Similar content being viewed by others

Introduction
Lower limb amputation (LLA) highly impacts the lives of individuals. Psychological, physical and social well-being are directly affected. Care centers for individuals with amputation, composed of multidisciplinary rehabilitation teams, are responsible for the recovery and functional maintenance of patients, as well as for their reintegration to work, sports and social activities1. One important factor that influences the quality of life of this population is adequate adaptation to prosthesis. Despite not being the only contributor, the inability to walk due to difficulties in adapting to wearing prosthesis can potentially result in physical degeneration and comorbidity in this population2,3. Inadequate adaptation to prosthesis is also considered one of the factors related to the high incidence of falls and fear of falling among them4, and should therefore be one of the focuses of rehabilitation programs directed at this population. Some studies report that confidence and balance during walking and the execution of specific tasks are factors that benefit the quality of life and socialization of these individuals, a prevalent dependency found in the lives of individuals with LLA5,6,7.
According to a systematic review about physiotherapy rehabilitation programs for individuals with amputations wearing prosthesis, there is no consensus regarding the types and quality of exercises and evaluations more suitable for this population. In general, the studies show the importance of strengthening exercises as well as gait training for prosthesis use. However, only 9 out of 10,393 studies met the inclusion criteria of this systematic review, and no clear conclusions were obtained on how to better assist this population with rehabilitation interventions8.
Furthermore, more clinical quantitative and qualitative assessments are needed to better understand the performance of gait in these individuals when wearing prosthesis following intervention. Among the different types of assessment, temporal-spatial, kinetic and kinematic analyses offer a quantitative approach that can precisely detect differences in performance9,10,11,12.
The objective of this study was to develop a simple and low-cost rehabilitation protocol, taking into account the wide-spread use of a functionally poor type of prosthesis offered by rehabilitation units from the public sector of many countries, and verifying the potential of applying this protocol in those units with few resources. The intervention prioritized the strengthening of the hip segment and gait training with the objective of stabilizing the pelvic girdle, optimizing gait performance and attaining good adaptation to prosthesis. It was elaborated and adjusted to last for the same amount of time reserved by the public hospital for prosthesis adaptation, 4 months in total. The purpose was to meet the functional needs of these individuals after amputation. The justification of the study is based on the difficulty in finding rehabilitation protocols in the literature that meet the primary needs of individuals with lower limb amputations that rely on care offered by public sectors with few resources, to verify if assistance could be satisfactorily provided without the need for expensive equipment, often also more difficult to manipulate. Temporal-spatial, kinetic and kinematic analyses were performed pre- and post-intervention.
Method
Design
This study is a randomized clinical trial registered with the Brazilian Clinical Trials Registration Identifier RBR-4s5nkh with the registration date 20/05/2020 (https://ensaiosclinicos.gov.br/metis/search/query), conducted in accordance with the Declaration of Helsinki guidelines, and approved by the State University of Campinas Research Ethics Committee (Nº. 2.349.249). Written informed consent was obtained from each participant before the study began.
Participants
Data were collected with a total of 26 participants, including 16 participants with amputation and 10 able-bodied individuals. The clinical population, including the intervention and control groups, was recruited from the Specialization and Assistance Center for Individuals with Amputations at the Clinics Hospital. Sample selection was based on the following inclusion criteria: age between 18 and 60 years, physically inactive, intellectually capable, having undergone unilateral vascular or traumatic amputation at the transtibial (TT) or transfemoral (TF) levels, suitable for prosthesis. Able-bodied individuals were recruited from the hospital staff if met with the inclusion criteria: age between 18 and 60 years, physically inactive, intellectually capable, having no amputations or musculoskeletal injuries related to the locomotor system. Able-bodied individuals were submitted to the same kinetic and kinematic gait assessment performed by the groups of individuals with amputation. Its evaluation aimed to ensure that a ‘standard’ gait parameter was attained from able-bodied individuals undergoing this study’s experimental setup and procedure, comparable to the normative data already found in the literature, in view of the large variability found from one instrument to another.
Initial screening was performed from medical records, followed by interviews. All interviewed individuals with amputation agreed to take part in the study and were blindly randomized during recruitment. An independent researcher divided the sample into control and intervention groups by handling them blindly chosen envelopes containing the assigned group. The intervention group underwent the rehabilitation described below (Table 1).
Intervention
The intervention protocol was designed to be low-cost and easy to apply. The use of accessible materials, such as ice, sponges, elastic resistance bands and band loops (TheraBand), balls, cones, benches, mini-trampolines, parallel bars, electrotherapy (Model: ENDOPHASYS MMS-050, Manufacturer / distributor: KLD Biosistemas Equipamentos Eletrônicos Ltda, Amparo-SP, Brazil), and the outdoor environment, were chosen so that public rehabilitation centers, with few resources, could use it as a first step in post-amputation care. The intervention protocol aimed at promoting adaptation to prosthesis use and functional and social independence. The exercises focused on core exercises, predominantly in the abdominal region, and on the activation of hip muscles13,14. The protocol was designed to meet capacity and demand needs, i.e., juggle between developing the necessary physical capacity and adapting to wearing prosthesis, ultimately minimizing the high physical demand required for this adaptation15.
The intervention group underwent the rehabilitation exercise protocol, divided in two phases: pre- and post-prosthesis. The pre-prosthesis phase was carried out for 12 weeks, with 2 sessions of 1 h each week, totalling 24 sessions. The post-prosthesis phase was carried out for 4 weeks, with 2 sessions of 1 h each week, totalling 8 sessions. The intervention period was set for 4 months in accordance with the time frame that the hospital normally takes to perform prosthesis preparations and adjustments. The prostheses were created according to the model provided by the public health service (Table 1). During the post-prosthesis period, adjustments and alignment of prostheses were performed by specialized technical professionals to comply with the participant comfort and needs.
Outcome measures
Data used to characterize the sample was collected and filled in an evaluation sheet containing the items: sex, height, weight, age, body mass index (BMI), type of amputation, cause of amputation, and amputation time. Type, cause, and amputation time were obtained from the participants’ medical records.
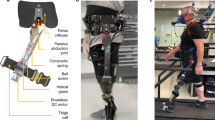
The gait cycle evaluation protocol, including kinetic and kinematic evaluations, was performed by asking the participant to walk along an 8-m-long walkway, at a self-selected gait speed considered comfortable by each individual. Three valid attempts from each participant in all groups were recorded. Twelve high- speed cameras operating at 100 Hz (Vero 1.3, Vicon Motion Systems Ltd., Oxford, United Kingdom), and 2 force platforms at 1000 Hz (AMTI, Watertown, United States) were used to capture kinematic and kinetic data, respectively. The kinematic model used was a six degrees-of-freedom model created with the Motion Monitor X Gen software (v. 2019, Innsport Inc., Chicago Illinois, USA). Marker positions from a static trial were used to define joint centres. Calibration of the participant body segments were performed with clusters with 4 retro-reflective marks fixed on a rigid plate and placed over the lumbar-sacral region, thighs, legs and dorsal surface of the feet (Fig. 1). Kinetic and kinematic data were processed and analyzed with the Motion Monitor X Gen software. The phases of the gait cycle were defined as: initial contact, loading response, mid stance, terminal stance, pre-swing, initial swing, mid swing and terminal swing. Data from amputated and contralateral limbs were analysed in participants with amputation, but only data from the dominant limb in able-bodied participants were used for analysis. Data were analysed from the hips, knees and bilateral ankle joints in the sagittal plane. The temporal-spatial data of each group were also analysed. Data was filtered with a 4th order, zero-lag low-pass Butterworth filter with 10 Hz cut-off frequency. Gait analysis was performed in all individuals with amputation, after the pre-prosthesis intervention phase was completed by the intervention group and 12 weeks after recruitment of the control group. Two assessments were recorded, as soon as the participant received the prosthesis and 4 weeks after (post gait training for the intervention group). The group of able-bodied participants was tested once.

Positioning of clusters with retro-reflective marks fixed on the rigid plate.
Statistical analysis
All statistical analyses were conducted with PASW Statistics software (v. 18.0, SPSS Inc., Chicago, USA). Initially we performed a characterization of the sample by amputation level (transtibial or transfemoral) and for able-bodied individuals. Participants with amputation were then further characterized in control and intervention groups (Fig. 2). Data distribution and homogeneity of variance were verified with Shapiro–Wilk and Levene’s test. For the comparison of continuous variables between groups of individuals with transtibial amputation, transfemoral amputation and able-bodied individuals, one-way repeated measures ANOVA, followed by Tukey post hot test was used when data presented normal distribution and homogeneity of variances; Kruskal Wallis test, followed by Bonferroni post hot test, was used when the data did not show normal distribution or homogeneity of variances.

CONSORT flow chart (CONSORT, Consolidated Standards of Reporting Trials).
For the comparison of the amputation time (pre- versus post-intervention) and amputation cause between TT and TF amputation groups, the Mann Whitney U-test and the Fisher exact test were used, respectively. The analyses were conducted independently between amputated and contralateral limbs. For the comparison of the sample characterization parameters between control and intervention groups pre-prosthesis, Student's t-test were used for continuous variables and Fisher's exact test for categorical variables. For the analysis of angle, moment and temporal-spatial variables, Mixed Linear Models were applied, assuming group (intervention x control), limb (amputated x contralateral) and time (pre x post-intervention) as fixed effects, and subject as a random effect. Additionally, time and limb effects were assumed as repeated measures and the injury level as covariable. When major effects or significant interactions were found, Sidak's post hoc test was used to point out the differences.
Due to the large number of possible comparisons, interactions were analyzed from largest (triple) to smallest (main effect) complexity, and only significant results composed by the largest number of factors were described in the final results. Additionally, the clinical effects of the intervention were further analyzed by calculating the effect size (ES, d Cohen), defined as the mean difference divided by the combined standard deviation (DPpooled) from pre- vs. post-intervention results, and interpreted as: small (│d│ ≤ 0.30), moderate (0.31 < │d│ < 0.8) and large (│d│ ≥ 0.8)16. Thereafter, to minimize the bias caused by the small sample size, a Hedges correction was applied to obtain ES and estimates of unbiased confidence limits17. A 5% (P ≤ 0.05) significance criterion was adopted.
Results
Characterization of the sample
There was no significant difference between groups of participants with TT and TF amputation and able-bodied adults with regards to age, height, body mass and body mass index. Moreover, no difference was found in amputation time and amputation cause between individuals with amputation groups. For the intervention and control groups at the start of the experiment before intervention, no statistical difference was found for age, height, body mass index, amputation time, cause of amputation and type of amputation. Although no significant difference was observed between groups in the sample characterization variables, it was decided to include the amputation type as a covariable in the subsequent analyses to minimize possible bias caused by the imbalance in the proportion of participants with TF and TT amputation in intervention and control groups (Table 2).
Kinematics: control vs intervention
Between amputated and contralateral limbs, it was observed differences in the ankle joint, knee joint and hip joint. Between groups of individuals with amputation, it was observed higher plantar flexion in the intervention group during initial contact compared to the control group (Table 3).
The magnitude of the effects can be seen in Table 4. Ankle, knee and hip joint angular variation during different gait phases pre- and post-intervention can be visualized in the representation of the gait cycle in Fig. 3.

Ankle, knee and hip joint angular variation in the sagittal plane during different phases of gait cycle, in each group of individuals with amputation pre- and post-intervention. Able-bodied group parameter from their dominant limb is added for reference.
Kinetics: intervention vs. control
In the comparison between limbs and groups, for the ankle joint, lower plantar flexion moment during initial contact, and lower dorsiflexion moment during mid stance in the contralateral limb were found in the intervention group.
For the knee joint, between limbs, higher flexion moment during loading response, mid stance and terminal stance was found in the contralateral limb; between time points, lower flexion moment during initial contact was found post-intervention.
For the hip joint, between limbs, lower flexion moment during pre-swing was found in the contralateral limb; between groups, lower extension moment during initial contact was found in the intervention group; pre-intervention between limbs, higher extension moment during initial was found in the contralateral limb; post-intervention between groups, higher flexion moment during mid stance was found in the intervention group; within the control group between time points, higher extension moment was found during mid stance (Table 5).
The magnitude of the effects for different groups, limbs and time points can be seen in Table 6. Average joint moments can be visualized in the representation of the gait cycle in Fig. 4.

Ankle, knee and hip joint moment variation in the sagittal plane during gait cycle, in each group with amputation pre- and post-intervention. Able-bodied group parameter from their dominant limb is added for reference.
Temporal-spatial: intervention vs. control
Both mean gait speed and cadence increased at the post-intervention compared to pre-intervention, while for stride length, both groups increased (Table 7). The interpretation of effect magnitude can be seen in Table 8.
Discussion
The 16-week physiotherapy intervention protocol presented in this study demonstrated to be effective as the first stage of a post-amputation rehabilitation process. With regards to the magnitude of the intervention effect on temporal-spatial parameters, for the intervention group, the results demonstrated an increase in gait speed, cadence, and step length, with a large effect size, when compared to the control group. Stride length increased in both groups. However, the intervention group had a large effect size, while the control group had a moderate effect size (Table 8). From the combination of multiple gait parameters, it can be inferred that the intervention protocol promoted improvement in gait parameters, especially in temporal-spatial variables, and prosthesis adaptation. Despite the improvement in kinematic and kinetic parameters of gait, the study showed that both groups adopted adaptive gait strategies, presenting variability and asymmetry between limbs.
Previous studies showed that individuals who received intervention after amputation, not only tended to improve musculoskeletal resistance, gait speed, and the capacity to adjust to the prosthesis, but the intervention also reverberated in an increase of the survival rate by 1 year, when compared to people who did not receive any treatment18,19,20,21. Other studies, such as the present one, pointed out the adoption of adaptive patterns and the asymmetry between limbs, persisting during gait, also when sitting, getting up, and climbing stairs and ramps22,23,24. Although the origin of gait variability in individuals with amputation is not well defined, studies showed that it is related to multisystemic issues such as neuromotor control dysfunction, peripheral and central nervous system function, autonomic nervous system, and cardiac, musculoskeletal and psychological adaptation25,26,27.
In the stance phase, the main differences between intervention and control groups were in ankle (group and limb) and hip (group and time) joint angle during initial contact. For the ankle joint, the intervention group presented higher plantar flexion for both limbs, amputated and contralateral. For the hip joint, the intervention group presented higher flexion pre- and post-intervention. During mid stance, the hip showed a significant difference between interaction*group, limb and time, with a large effect size for the contralateral limb. In other words, there was a greater hip extension for contralateral limb post-intervention. During terminal stance, for the intervention group, there was an increase of knee flexion in the amputated limb, and greater hip extension in the amputated and contralateral limbs post-intervention. In the control group, there was a smaller hip extension and no difference between limbs or times. In the swing phase, the data did not present differences between the groups, only between limbs, as shown by a knee angle difference between limbs and times in the mid and terminal swing.
For the sagittal plane kinetic data, considered as propellants of the movement, the main difference observed by the study between intervention and control groups regarding moments, were for ankle plantarflexion moment during initial contact. The intervention group demonstrated a neutral tendency for ankle moment, for the amputated and contralateral limbs, and the control group demonstrated a tendency for a plantarflexion moment, mainly for the amputated limb. Differences between groups during initial contact were also for hip moment, showing a lower flexor tendency for the intervention when compared to control group. During mid stance, also in the hip segment, the intervention group presented a moment with extensor tendency, while the control group presented a moment with flexor tendency.
A previous study also investigating individuals with TT and TF amputation obtained similar adaptations at the hip joint to compensate for the loss of the ankle joint. Accordingly, differences at the knee joint were observed depending on amputation level, also similar to the findings of the present study28. Another study showed that the proposed rehabilitation exercise program promoted stability during gait phases, and the number of falls were reduced29. A study carried out with individuals with TT amputation showed positive results, with 66.7% improvement in functional mobility after undergoing a rehabilitation protocol30.
A limitation of this study was the small sample size; it prevented the separation of groups by level of amputation and cause of amputation. In addition, the different types and models of footwear wore by the participants during the process of adaptation to prosthesis, rehabilitation and gait assessments were also configured as possible limitations of the study.
In conclusion, this study showed that a low-cost and easily implementable physiotherapy intervention was relevant as the very first stage of a post-amputation rehabilitation procedure to aid in an individual’s adaptation to wearing prosthesis. There was improvement of kinetic and kinematic variables resulting in better gait performance by increasing speed, stride and step size. In addition, there was a decrease in stance contact time of the amputated limb, thus demonstrating a greater fluidity of gait after the intervention. However, asymmetry was observed between lower limb in both groups.
Additionally, it confirmed the importance of ensuring the continuity of rehabilitation and monitoring of individuals by a multidisciplinary team post-prosthesis fitting, mainly because this population is more susceptible to falls, requiring more neuromotor training to improve the performance of gait and daily activities.
References
Roffman, C. E., Buchanan, J. & Allison, G. T. Predictors of non-use of prostheses by people with lower limb amputation after discharge from rehabilitation: development and validation of clinical prediction rules. J. Physiother. 60(4), 224–231 (2014).
Dobson, A., El-Gamil, A., Shimer, M. & DaVanzo, J. E. Economic value of prosthetic services among Medicare beneficiaries: a claims-based retrospective cohort study. Mil. Med. 181(2 Suppl.), 18–22 (2016).
Samuelsson, K. A., Toytari, O., Salminen, A. L. & Brandt, A. Effects of lower limb prosthesis on activity, participation, and quality of life: a systematic review. Prosthet. Orthot. Int. 36(2), 145–158 (2012).
Miller, W. C., Speechley, M. & Deathe, B. The prevalence and risk factors of falling and fear of falling among lower extremity amputees. Arch. Phys. Med. Rehabil. 82(8), 1031–1037 (2001).
Bize, R., Johnson, J. A. & Plotnikoff, R. C. Physical activity level and health-related quality of life in the general adult population: a systematic review. Prev. Med. 45(6), 401–415 (2007).
Haskell WL, et al. Heath GW, Thompson PD, Bauman A; American College of Sports Medicine; American Heart Association. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 116(9):1081–93 (2007).
Balboa-Castillo T, León-Muñoz LM, Graciani A, Rodríguez-Artalejo F, Guallar-Castillón P. Longitudinal association of physical activity and sedentary behavior during leisure time with health-related quality of life in community-dwelling older adults. Health Qual Life Outcomes. 27; 9:47 (2011).
Ülger, Ö., Yıldırım Şahan, T. & Çelik, S. E. A systematic literature review of physiotherapy and rehabilitation approaches to lower-limb amputation. Physiother. Theory Pract. 34(11), 821–834 (2018).
Esquenazi, A. Gait analysis in lower-limb amputation and prosthetic rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 25(1), 153–167 (2014).
Sagawa, Y. Jr. et al. Biomechanics and physiological parameters during gait in lower-limb amputees: a systematic review. Gait. Post. 33(4), 511–526 (2011).
Rusaw, D. & Ramstrand, N. Motion-analysis studies of transtibial prosthesis users: a systematic review. Prosthet. Orthot. Int. 35(1), 8–19 (2011).
Rietman, J. S., Postema, K. & Geertzen, J. H. Gait analysis in prosthetics: opinions, ideas and conclusions. Prosthet. Orthot. Int. 26(1), 50–57 (2002).
Chan, M. K. et al. The effects of therapeutic hip exercise with abdominal core activation on recruitment of the hip muscles. BMC Musculoskelet. Disord. 18(1), 313 (2017).
Chiarotto, A., Ostelo, R. W., Turk, D. C., Buchbinder, R. & Boers, M. Core outcome sets for research and clinical practice. Braz. J. Phys. Ther. 21(2), 77–84 (2017).
Bittencourt, N. F. N. et al. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br. J. Sports Med. 50(21), 1309–1314 (2016).
Cohen, J. The concepts of power analysis. Statistical power analysis for the behavioral sciences. (Academic Press, 1988).
Nakagawa, S. & Cuthill, I. C. Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol. Rev. Camb. Philos. Soc. 82, 591–605 (2007).
Geertzen J, et al. Dutch evidence-based guidelines for amputation and prosthetics of the lower extremity: rehabilitation process and prosthetics. Part 2. Prosthetics and Orthot Int. 39:361–371 (2015).
Kahle, J. T. et al. Predicting walking ability following lower limb amputation: an updated systematic literature review. Technol. Innov. 18, 125–137 (2016).
Christiansen, C. L., Fields, T., Lev, G., Stephenson, R. O. & Stevens-Lapsley, J. E. Functional outcomes after the prosthetic training phase of rehabilitation after dysvascular lower extremity amputation. PMR. 7, 1118–1126 (2015).
Madsen, U. R., Baath, C., Berthelsen, C. B. & Hommel, A. A prospective study of short-term functional outcome after dysvascular major lower limb amputation. Int. J. Orthop. Trauma Nurs. 28, 22–29 (2018).
Agrawal, V., Gailey, R., O’Toole, C., Gaunaurd, I. & Dowell, T. Weight distribution symmetry during the sit-to-stand movement of unilateral transtibial amputees. Ergonomics 54, 656–664 (2011).
Agrawal, V. et al. Comparison of four different categories of prosthetic feet during ramp ambulation in unilateral transtibial amputees. Prosthet. Orthot. Int. 39, 380–389 (2015).
Agrawal, V., Gailey, R. S., Gaunaurd, I. A., O’Toole, C. & Finnieston, A. A. Comparison between microprocessor-controlled ankle/foot and conventional prosthetic feet during stair negotiation in people with unilateral transtibial amputation. J. Rehabil. Res. Dev. 50, 941–950 (2013).
Hausdorff, J. M. Gait variability: methods, modeling and meaning. J. Neuroeng. Rehabil. 20, 2–19 (2005).
Beauchet, O. et al. Higher gait variability is associated with decreased parietal gray matter volume among healthy older adults. Brain Topogr. 27, 293–295 (2014).
Martinikorena, I. et al. Gait variability related to muscle quality and muscle power output in frail nonagenarian older adults. J. Am. Med. Dir. Assoc. 17(2), 162–167 (2016).
Prinsen, E. C., Nederhand, M. J. & Rietman, J. S. Adaptation strategies of the lower extremities of patients with a transtibial or transfemoral amputation during level walking: a systematic review. Arch. Phys. Med. Rehabil. 92(8), 1311–1325 (2011).
Schafer, Z. A., Perry, J. L. & Vanicek, N. A personalised exercise programme for individuals with lower limb amputation reduces falls and improves gait biomechanics: A block randomised controlled trial. Gait Post. 63, 282–289 (2018).
Gailey, R. et al. Effectiveness of an evidence-based amputee rehabilitation program: a pilot randomized controlled trial. Phys. Ther. 100(5), 773–787 (2020).
Acknowledgements
The authors thank the support by grants from FAPESP-São Paulo Research Foundation [2018/02420-0].
Author information
Authors and Affiliations
Contributions
The first author wrote the main manuscript text and prepared the figures and tables. All authors assisted in data analysis. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Almeida, L.V., Fukuchi, C.A., Sakanaka, T. et al. A low-cost easily implementable physiotherapy intervention clinically improves gait implying better adaptation to lower limb prosthesis: a randomized clinical trial. Sci Rep 11, 21228 (2021). https://doi.org/10.1038/s41598-021-00686-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-00686-9
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
