
Abstract
Translation of survival benefits observed in glioblastoma clinical trials to populations and to longer-term survival remains uncertain. We aimed to assess if ≥ 2-year survival has changed in relation to the trial of radiotherapy plus concomitant and adjuvant temozolomide published in 2005. We searched MEDLINE and Embase for population-based studies with ≥ 50 patients published after 2002 reporting survival at ≥ 2 years following glioblastoma diagnosis. Primary endpoints were survival at 2-, 3- and 5-years stratified by recruitment period. We meta-analysed survival estimates using a random effects model stratified according to whether recruitment ended before 2005 (earlier) or started during or after 2005 (later). PROSPERO registration number CRD42019130035. Twenty-three populations from 63 potentially eligible studies contributed to the meta-analyses. Pooled 2-year overall survival estimates for the earlier and later study periods were 9% (95% confidence interval [CI] 6–12%; n/N = 1,488/17,507) and 18% (95% CI 14–22%; n/N = 5,670/32,390), respectively. Similarly, pooled 3-year survival estimates increased from 4% (95% CI 2–6%; n/N = 325/10,556) to 11% (95% CI 9–14%; n/N = 1900/16,397). One study with a within-population comparison showed similar improvement in survival among the older population. Pooled 5-year survival estimates were 3% (95% CI 1–5%; n/N = 401/14,919) and 4% (95% CI 2–5%; n/N = 1,291/28,748) for the earlier and later periods, respectively. Meta-analyses of real-world data suggested a doubling of 2- and 3-year survival in glioblastoma patients since 2005. However, 5-year survival remains poor with no apparent improvement. Detailed clinically annotated population-based data and further molecular characterization of longer-term survivors may explain the unchanged survival beyond 5 years.
Similar content being viewed by others


Introduction
Glioblastoma multiforme is the most common primary malignant brain tumour in adults with an incidence rate of 3.7 per 100,000 person-years, though geographical variation exists1. Despite an increasing understanding of the underlying pathophysiology, glioblastoma remains an incurable disease with high mortality2. A landmark clinical trial in 2005 demonstrated that the addition of concomitant and adjuvant temozolomide to radiotherapy provided an additional survival benefit to patients diagnosed with glioblastoma3. Multiple clinical trials had investigated novel therapies that showed promise in pre-clinical and early phase studies, but to date there have been no major additions to the treatment armamentarium for newly diagnosed patients since 2005. The median survival in the intervention arm of the 2005 trial was 14.6 months3, but there is uncertainty about whether survival benefit from clinical trials is translated to the population4,5. Clinical trial participation itself is associated with better survival6, which may be caused by the preferential inclusion and exclusion criteria into clinical trials. In clinical practice not all patients are eligible for the trial standard of care involving maximal surgical debulking, chemotherapy and radiotherapy, for example because of co-morbidities, poor functional status or tumour location within the brain. There is also a paucity of data on long-term GBM survivors.
We systematically reviewed population-based studies that reported overall survival after glioblastoma to characterize survival beyond 2 years and investigate whether survival has changed since the landmark 2005 trial.
Methods
Protocol and registration
We registered this systematic review in PROSPERO (CRD42019130035) and reported it in accordance with PRISMA and MOOSE guidelines.
Eligibility criteria
We included all population-based studies reporting overall survival at ≥ 2 years in adults with glioblastoma. Studies reporting overall survival in all types of brain tumor from which data could be extracted for glioblastoma were also eligible. There was no language restriction. We excluded conference abstracts, studies without data on overall survival at ≥ 2 years, studies with less than 50 participants, and studies published before 2003 because contemporary imaging facilities and provision, which impact on time of diagnosis and patient management, were generally not available during their recruitment periods.
Information sources and search
We searched MEDLINE and Embase on 15 March 2019 using a combination of search terms for glioma or glioblastoma, population-based, registry, and survival or mortality (Supplementary material Appendix 1). We screened bibliographies of eligible studies for any studies missed by the electronic searches.
Study selection
After removing duplicate records, two reviewers (MTCP and PMB) screened all titles and abstracts. Studies passing the initial screening underwent full eligibility assessment against the inclusion and exclusion criteria. We resolved any disagreements or uncertainties through discussion between the authors.
Data collection process
We developed a data collection tool using a subset of eligible studies. One reviewer (MTCP) extracted data from eligible studies against the data collection tool. A second reviewer (PMB or JDF) resolved uncertainties by discussion.
Data items
We collected data on study characteristics including year of publication, country of population, registry or database used, recruitment period, any study-specific selection criteria, total sample size, median age, gender, number and proportion of patients receiving different treatments (surgical resection, chemotherapy, radiotherapy), and number and proportion of patients surviving at 2, 3, 5, and 10 years. As cancer registries generally do not routinely collect the specific chemotherapy drug and its regimen, we could not quantify the proportion of patients receiving multimodal therapy. If a study reported survival data stratified by recruitment period, we extracted the stratified survival data. Therefore, a study may contribute to meta-analyses of more than one recruitment period. When studies only reported survival data on a graph, we used Plot Digitizer (https://plotdigitizer.sourceforge.net/) to extract data.
Risk of bias assessment
As there is no published risk of bias tool specifically for evaluating population-based observational studies without a pre-defined exposure, we assessed risk of bias based on the preliminary ROBINS-E tool developed by GRADE7, 8. The assessment aimed to evaluate the risk of bias affecting the survival estimate in the study. Categories assessed for bias were patient selection, diagnostic certainty, handling of missing data, and outcome measurement (Supplementary Table S1). Based on risk of bias assessment in each category, we rated the overall risk of bias as low, moderate, serious, or critical.
Summary measures
Summary measures were proportions of patients with glioblastoma surviving at 2, 3, 5, and 10 years.
Synthesis of results
We stratified studies according to whether the recruitment period was before 2005 or during or after 2005 as a proxy to wider use of multimodal treatment in the later period, informed by the 2005 landmark trial. This dichotomy does not imply a definite use of multimodal treatment since not all patients received this treatment and clinical practice of offering this treatment varies. If several publications described the same population, we included the largest sample size. Our target population was all individuals diagnosed with glioblastoma, therefore we excluded studies with selected cohorts—for example, additional exclusion criteria based on age or treatment limit—from the meta-analyses. We meta-analysed survival data at 2, 3, and 5 years from population-based studies stratified by recruitment period using Stata 16.0 (StataCorp) using a random-effects model. We quantified heterogeneity using the I2 statistic.
Additional analyses
By analysing non-overlapping patients stratified by recruitment period, we inevitably excluded some studies from the meta-analyses. Additional analyses of these excluded studies with recruitment period starting before and ending after 2005 allowed us to compare their pooled estimates with the primary analyses. Sensitivity analyses restricting to low risk of bias studies assessed how this affected the meta-analyses.
We observed that survival estimates from East Asian studies appeared higher than European and North American studies. To assess the contribution of the East Asian studies to the heterogeneity observed, we performed sensitivity analyses by meta-analysing the same survival data without studies of East Asian populations.
Further sensitivity analyses included moving the proxy year to 2006 to represent the time-point after which multimodal treatment was likely to be more common. We also meta-analysed studies where patient recruitment started before and ended after 2005. These studies contained some patients also included within populations contributed to the main analyses. However, no patients were included more than once in this additional meta-analysis.
Results
Study selection and characteristics
Our search strategy retrieved 503 records. There were 135 potentially eligible studies, of which 63 were included in this review after full eligibility assessment (Fig. 1)9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37. One study reported two distinct populations14. Therefore, there were 63 eligible studies representing 64 populations from 17 countries that reported overall survival at ≥ 2 year in patients with glioblastoma. Detailed study characteristics are presented in Supplementary Table S2 (p 4–7). The United States was the most frequently reported population (n = 29; 45%). Twenty-seven studies reported survival estimates in Western European populations (including Switzerland and the United Kingdom), and three in Canada. Of the remaining studies, four were from East Asian populations and one from Australia. The median length of recruitment period was 8.5 years (IQR 5–14 years). Median age ranged from 58 to 75 years. In studies that did not use the predominantly male Veterans Health Administration (VA) database, the percentage of females ranged from 32 to 61%. The percentage of patients receiving each of the following treatments ranged from 25 to 100% for resective surgery; 39–100% for radiotherapy; 7–100% for chemotherapy. There were 55 (87%) studies reporting 2-year survival, 31 (49%) reporting 3-year survival, 32 (51%) reporting 5-year survival, and 3 (5%) reporting 10-year survival.

PRISMA flowchart.
Risk of bias
Based on our risk of bias assessment, 29 (46%) studies had low risk of bias (Supplementary Table S2). Nine studies included glioblastoma cases without histological confirmation. Fourteen studies (22%) had a sample size of less than 300. Demographic information (age and gender) were provided in 30 (48%) studies. Only 21 (33%) studies reported the proportion of patients receiving each of resective surgery, radiotherapy, and chemotherapy.
2-year survival
Sixty-seven survival data points stratified by recruitment period were available from 55 studies reporting 2-year survival. There were 16 survival estimates for patients recruited before 2005, 30 for those recruited in studies that spanned across 2005, and 21 for those recruited during or after 2005. After reviewing the information sources for the sample sizes of these studies, survival data from non-overlapping patients were available in eight studies where patient recruitment ended before 2005, and 13 where recruitment started in or after 2005. Table 1 shows the characteristics of these studies. The pooled 2-year survival estimate for the earlier period was 9% (95% confidence interval [CI] 6–12%; n/N = 1,488/17,507; I2 = 97.2%; Fig. 2); the pooled estimate for the later period was 18% (95% CI 14–22%; n/N = 5,670/32,390; I2 = 98.3%; Fig. 2). Seven populations had 2-year survival available at both the earlier and later periods, enabling within-population comparisons: Surveillance, Epidemiology, and End Results (SEER) in the US13,31, Veterans Health Administration (VA) in the US15, Italy26,35, Switzerland18,28, France9,17, Sweden16,24 and Korea22. The survival estimates were higher during the later period compared with the earlier period in all seven populations. Three studies observed at least doubling of survival. The increase in survival ranged from 2 to 8% in the other studies.

Forest plots of 2-year overall survival stratified by recruitment period.
3-year survival
Thirty-five survival data points were available from 31 studies reporting 3-year survival. There were nine survival estimates for patients recruited before 2005, 16 for those where recruitment spanned across 2005, and ten for those recruited during or after 2005. There were seven studies contributing to each meta-analysis for the earlier and later period (Table 1). Pooled 3-year survival was 4% (95% CI 2–6%; n/N = 325/10,556; I2 = 97.9%; Fig. 3) for the earlier period, and 11% (95% CI 9–14%; n/N = 1900/16,397; I2 = 91.8%; Fig. 3) for the later period. There was at least doubling of 3-year survival in all four populations (SEER20,21, VA15, Italy10,26, and Sweden16) that allowed a within-population comparison.

Forest plots of 3-year overall survival stratified by recruitment period.
5-year survival
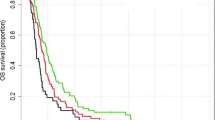
Thirty-seven survival data points were available from 32 studies reporting 5-year survival. There were seven survival estimates for patients recruited before 2005, 22 for those recruited in studies that spanned across 2005, and seven for those recruited during or after 2005. Meta-analyses from five studies (with no duplicated patients) in each time period (Table 1) yielded pooled survival estimate of 3% (95% CI 1–5%; n/N = 401/14,919; I2=96.6%; Fig. 4) for the earlier period, and 4% (95% CI 2–5%; n/N = 1,291/28,748; I2 = 98.0%; Fig. 4) for the later period. The US VA15 and SEER13,31 populations allowed within-population comparison. Survival increased from 213 to 6%31 in the SEER population but remained at 1% in the VA population15.

Forest plots of 5-year overall survival stratified by recruitment period.
10-year survival
Only 3 (5%) studies reported 10-year survival29,33,37. Two studies used the United States SEER database33,37, while one was from Canada using a national cancer registry37. The recruitment periods ranged from 9 to 16 years. Each study had more than 10,000 patients. All three studies had serious or critical risk of bias for their survival estimates. Both studies from the United States included reported survival only in patients who had surgical resection, and one of them excluded those who died within 1 month of surgery. About 25% patients in the Canadian study did not have a histological diagnosis of glioblastoma. The estimate of 10-year survival ranged from 0.333 to 3%37. No comparison in relation to 2005 was possible as all study periods started before and ended after 2005.
Sensitivity analyses
Restricting quantitative analyses to low risk-of-bias studies showed the respective pooled survival estimates for the earlier and later periods were: 11% and 18% at 2 years; 5% and 8% at 3 years; and 3% and 3% at 5 years (Supplementary Fig. S1). Because survival estimates from East Asian populations were consistently higher than the pooled estimate, we carried out sensitivity analyses excluding the East Asian studies from meta-analyses. The respective pooled survival estimates without the East Asian populations for the earlier and later periods were: 8% and 16% at 2 years; 2% and 11% at 3 years; and 2% and 4% at 5 years (Supplementary Fig. S2). Instead of using year 2005 as a proxy time-point after which wider use of multimodal therapy occurred, we stratified studies by their recruitment period into before 2006, and during or after 2006. There was no change to the number of studies available for meta-analyses in the earlier period. In the later period, meta-analyses at 2, 3 and 5 years had 5, 3, and 1 fewer studies, respectively. The respective pooled survival estimates for the earlier and later period using 2006 as the proxy time-point were: 9% and 19% at 2 years; 4% and 12% at 3 years, and 3% and 4% at 5 years (Supplementary Fig. S3).
Meta-analyses of studies that did not contribute to the main analyses are presented in Supplementary Material (Fig. S4). These studies contain some overlapping patients with populations in the main analyses. The pooled estimates of the proportion of patients surviving at 2 and 3 years were 12% and 8%, respectively. Both were between the pooled estimates for the earlier and later periods. At 5 years, the pooled estimate was 4%.
Older populations
Regardless of recruitment period, there were five studies that restricted their cohorts to patients ≥ 65 years20,27,34 and ≥ 70 years of age23,36. Populations in these studies were based in the United States—four from SEER20,27,34,36 and one from the National Cancer Database (NCDB)23. The 2-year survival estimates ranged from 220 to 11%23, and 3-year survival ranged from 0.420,36 to 5%23. The 5-year survival was 0.2% in the only study reporting at this time point20. One study had within-population comparison for the earlier and later recruitment periods and reported an increase in survival estimate at 2 and 3 years from 2 to 7% and from 0.9 to 3%, respectively36.
Discussion
This systematic review of 63 population-based studies of which 22 were included in the primary analyses found that 2-year survival was 18%, 3-year survival was 11%, and 5-year survival was 4% in patients diagnosed with glioblastoma during or after 2005. There was a doubling of 2- and 3-year survival in contemporary populations compared with patients treated prior to 2005. These survival gains were also evident in older (≥ 65 years) patients. However, there was no apparent improvement in 5-year survival.
The most significant development in clinical management of glioblastoma in the past two decades has been the landmark trial of radiotherapy plus concomitant and adjuvant temozolomide3. This clinical trial among 573 patients with a median follow-up of 28 months demonstrated that when compared with radiotherapy alone, the combination therapy improved the median survival from 12.1 to 14.6 months. The reported 2-year survival was 8% in the radiotherapy alone group, and 20% in the combination therapy group. These survival probabilities are very similar to our findings for 2-year survival from the meta-analyses of earlier and later time periods. Within-population comparisons, which should be less prone to confounding, confirmed a higher survival in the later versus earlier period. Although it is not possible to directly examine whether this improvement is secondary to the use of multimodal therapy, there was a rapid increase in the use of adjuvant and concomitant temozolomide with radiotherapy after the trial publication38, at least in the United States. The European39,40 and the United States41 neuro-oncology guidelines have established multimodal treatment for glioblastoma as the standard of care in many countries. Hence, it is possible that the increased use of multimodal therapy contributed to the improvements observed. Our findings also demonstrate the value of using health data to assess the impact of therapeutic advances on a disease at a population level. This approach can evaluate the real-world risk–benefit ratio of treatment at scale for treatments that have significant side-effects.
International variations in incidence of malignant astrocytoma42 and overall survival, may suggest different aetiologies, underlying disease processes, or risk exposure such as ethnicity1. Investigations into these factors may elucidate different underlying pathological mechanisms. Differences in cancer registration practice could also contribute to survival variation. The International Cancer Benchmarking Partnership (ICBP), which comprises 13 jurisdictions from 6 countries, has reported differences in capturing incidence date43. Furthermore, the increased use of brain imaging44 and high prevalence of incidental findings45 may further contribute to the lead-time bias.
There has been significant progress in understanding genomic drivers implicated in glioma tumorigenesis. Multidimensional data from genomics studies such as The Cancer Genome Atlas (TCGA)46, REMBRANDT study47, and the Chinese Glioma Genome Atlas (CGGA)48 have identified molecular signatures associated with glioma subtypes and their prognoses49. Isocitrate dehydrogenase (IDH) mutation and 1p/19q co-deletion are most prominent markers associated with a more favourable prognosis49. The importance of these markers are reflected in the 2016 update of the WHO classification of central nervous system (CNS) tumours50, which incorporates molecular markers into the definition of tumour entities, in addition to histological features. Future studies should examine outcomes and therapy responses amongst these molecular subtypes.
Studying clinical phenotypes can gain knowledge of glioblastoma disease mechanisms. In a recent study using radiographical and transcriptomics data, it was suggested that female and male patients with glioblastoma have different molecular mechanisms51. Studies have suggested that longer-term survivors may have different clinical and tumour characteristics compared to shorter-term survivors. Patients with glioblastoma surviving 5 years or more are younger52,53,54 and have better performance status at the time of diagnosis53,54 compared with shorter-term survivors. Methylation of the O6-methylguanine-DNA-methyltransferase (MGMT)55,56 and IDH55 mutation are more common in patients surviving 3 years compared with those who died before 3 years. However, studies of long-term survivors are challenging given that there are very few subjects, with a varying degree of clinical detail. The observation that the proportion of patients surviving 5 years has not changed, may indicate a molecularly distinct group of patients within this heterogeneous disease. In order to clarify this hypothesis, future studies should include comprehensive clinical details with molecular markers in a large patient cohort.
This systematic review and meta-analysis presented international real-world data drawn from population-based studies. We evaluated longer-term survival beyond the median survival observed in the landmark trial, and we were able to compare survival in the era of contemporary management to an earlier period. Our data also addressed the survival uncertainty in the older population. However, there were some limitations to our study. A high proportion of eligible studies used the same national database. We adopted a strategy to prevent any patient from being included more than once in our analyses. Inevitably this led to the omission of patients recruited in some time periods. However, our sensitivity analyses comparing the pooled estimate of these omitted studies to that of the main analyses showed a confirmatory trend of survival improvement (Supplementary Fig. S4). There was considerable between-study heterogeneity despite excluding studies with a high risk of bias and examining heterogeneity in our sensitivity analyses. Unmeasured factors such as unrecorded variables, missing treatment data, and variations in data coding would contribute to the variation of survival estimates57. Patients in some studies did not have histological confirmation; patients with better prognosis associated with lower grade gliomas or other brain tumours may have been included. This ascertainment bias is unlikely to have significantly affected our findings since studies in the meta-analyses, where some patients did not have histological confirmation, had similar survival to other studies. While this review examines the trend in survival in relation to a landmark clinical trial, we were unable to evaluate directly the pattern of treatment and its impact on survival due to limited treatment information available from eligible studies. Within-population comparison of different time periods, which may partially control for unmeasured factors, was only possible in a few eligible studies. We are, therefore, unable to directly attribute the survival trend observed to a change in treatment patterns. We used the year of 2005 as a proxy time-point for the introduction of wider use of multimodal therapy. Although some studies specified the more prevalent use of multimodal therapy, not all would have taken up recommendations from the clinical trial. However, our sensitivity analysis showed no substantial change in trend and having the cut-off year at 2005 allowed more studies to be included (Supplementary Fig. S3). Survival improvement may be attributable to other factors in addition to the multimodal treatment, such as more prevalent use of neuroimaging leading to earlier diagnosis, strengthening of multidisciplinary neuro-oncology care, and advances in neurosurgical techniques.
Conclusions
Overall estimates of survival among patients with glioblastoma have at least doubled since 2005 to 18% at 2 years and 11% at 3 years. This may reflect treatment response to modern therapeutic approaches. However, longer term survival remains poor and there appears to be a lack of improvement in 5-year survival. Large population-based studies with detailed clinical characteristics would clarify whether there has been an increase in the use of multimodal therapy and whether multimodal therapy affects survival beyond 5 years. Differences in msolecular markers of tumour subtypes may shed light on the underlying disease mechanisms that influence survival.
References
Ostrom, Q. T., Gittleman, H., Stetson, L., Virk, S. & Barnholtz-Sloan, J. S. Epidemiology of intracranial gliomas. Prog. Neurol. Surg. 30, 1–11. https://doi.org/10.1159/000464374 (2018).
Omuro, A. & DeAngelis, L. M. Glioblastoma and other malignant gliomas: A clinical review. JAMA 310, 1842–1850. https://doi.org/10.1001/jama.2013.280319 (2013).
Stupp, R. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 352, 987–996. https://doi.org/10.1056/NEJMoa043330 (2005).
Ray, S., Bonafede, M. M. & Mohile, N. A. Treatment patterns, survival, and healthcare costs of patients with malignant gliomas in a large US commercially insured population. Am. Health Drug Benefits 7, 140–149 (2014).
Dressler, E. V. et al. Patterns and disparities of care in glioblastoma. Neurooncol. Pract. 6, 37–46. https://doi.org/10.1093/nop/npy014 (2019).
Field, K. M. et al. Clinical trial participation and outcome for patients with glioblastoma: multivariate analysis from a comprehensive dataset. J. Clin. Neurosci. 20, 783–789. https://doi.org/10.1016/j.jocn.2012.09.013 (2013).
Morgan, R. L. et al. GRADE: Assessing the quality of evidence in environmental and occupational health. Environ. Int. 92–93, 611–616. https://doi.org/10.1016/j.envint.2016.01.004 (2016).
Morgan, R. L. et al. Evaluation of the risk of bias in non-randomized studies of interventions (ROBINS-I) and the “target experiment” concept in studies of exposures: Rationale and preliminary instrument development. Environ. Int. 120, 382–387. https://doi.org/10.1016/j.envint.2018.08.018 (2018).
Bauchet, L. et al. Oncological patterns of care and outcome for 952 patients with newly diagnosed glioblastoma in 2004. Neurol. Oncol. 12, 725–735. https://doi.org/10.1093/neuonc/noq030 (2010).
Brandes, A. A. et al. Pattern of care and effectiveness of treatment for glioblastoma patients in the real world: Results from a prospective population-based registry. Could survival differ in a high-volume center?. Neuro Oncol. Pract. 1, 166–171. https://doi.org/10.1093/nop/npu021 (2014).
Brodbelt, A. et al. Glioblastoma in England: 2007–2011. Eur. J. Cancer 51, 533–542. https://doi.org/10.1016/j.ejca.2014.12.014 (2015).
Bruhn, H. et al. Improved survival of Swedish glioblastoma patients treated according to Stupp. Acta Neurol. Scand. 138, 332–337. https://doi.org/10.1111/ane.12966 (2018).
Chang, S. M. & Barker, F. G. 2nd. Marital status, treatment, and survival in patients with glioblastoma multiforme: A population based study. Cancer 104, 1975–1984 (2005).
Chien, L.-N. et al. International differences in treatment and clinical outcomes for high grade glioma. PLoS ONE 10, e0129602. https://doi.org/10.1371/journal.pone.0129602 (2015).
Dubrow, R. et al. Time trends in glioblastoma multiforme survival: The role of temozolomide. Neuro-oncology 15, 1750–1761. https://doi.org/10.1093/neuonc/not122 (2013).
Eriksson, M. et al. Improved treatment of glioblastoma—Changes in survival over two decades at a single regional Centre. Acta Oncol. https://doi.org/10.1080/0284186X.2019.1571278 (2019).
Fabbro-Peray, P. et al. Association of patterns of care, prognostic factors, and use of radiotherapy-temozolomide therapy with survival in patients with newly diagnosed glioblastoma: A French national population-based study. J. Neurooncol. https://doi.org/10.1007/s11060-018-03065-z (2018).
Gramatzki, D. et al. Glioblastoma in the Canton of Zurich, Switzerland revisited: 2005–2009. Cancer 122, 2206–2215. https://doi.org/10.1002/cncr.30023 (2016).
Graus, F. et al. Patterns of care and outcome for patients with glioblastoma diagnosed during 2008–2010 in Spain. Neuro Oncol. 15, 797–805. https://doi.org/10.1093/neuonc/not013 (2013).
Iwamoto, F. M., Reiner, A. S., Panageas, K. S., Elkin, E. B. & Abrey, L. E. Patterns of care in elderly glioblastoma patients. Ann. Neurol. 64, 628–634. https://doi.org/10.1002/ana.21521 (2008).
Johnson, D. R. et al. Overall survival in patients with glioblastoma before and after bevacizumab approval. Curr. Med. Res. Opin. 34, 813–820. https://doi.org/10.1080/03007995.2017.1392294 (2018).
Jung, K.-W. et al. Population-based survival data for brain tumors in Korea. J. Neurooncol. 109, 301–307. https://doi.org/10.1007/s11060-012-0893-5 (2012).
Mak, K. S., Agarwal, A., Qureshi, M. M. & Truong, M. T. Hypofractionated short-course radiotherapy in elderly patients with glioblastoma multiforme: An analysis of the National Cancer Database. Cancer Med. 6, 1192–1200. https://doi.org/10.1002/cam4.1070 (2017).
Mathiesen, T., Peredo, I. & Lonn, S. Two-year survival of low-grade and high-grade glioma patients using data from the Swedish Cancer Registry. Acta Neurochir. 153, 467–471. https://doi.org/10.1007/s00701-010-0894-0 (2011).
Morgan, E. R., Norman, A., Laing, K. & Seal, M. D. Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: A population-based study. Curr. Oncol. 24, e92–e98. https://doi.org/10.3747/co.24.3424 (2017).
Nava, F. et al. Survival effect of first- and second-line treatments for patients with primary glioblastoma: A cohort study from a prospective registry, 1997–2010. Neuro-oncology 16, 719–727. https://doi.org/10.1093/neuonc/not316 (2014).
Nuno, M. et al. Does 30-day readmission affect long-term outcome among glioblastoma patients?. Neurosurgery 74, 196–205. https://doi.org/10.1227/NEU.0000000000000243 (2014).
Ohgaki, H. et al. Genetic pathways to glioblastoma: A population-based study. Can. Res. 64, 6892–6899 (2004).
Ostrom, Q. T., Cote, D. J., Ascha, M., Kruchko, C. & Barnholtz-Sloan, J. S. Adult glioma incidence and survival by race or ethnicity in the United States from 2000 to 2014. JAMA Oncol. 4, 1254–1262. https://doi.org/10.1001/jamaoncol.2018.1789 (2018).
Rasmussen, B. K. et al. Epidemiology of glioma: Clinical characteristics, symptoms, and predictors of glioma patients grade I–IV in the the Danish Neuro-Oncology Registry. J. Neurooncol. 135, 571–579. https://doi.org/10.1007/s11060-017-2607-5 (2017).
Rong, X. et al. Influence of insurance status on survival of adults with glioblastoma multiforme: A population-based study. Cancer 122, 3157–3165. https://doi.org/10.1002/cncr.30160 (2016).
Rosenthal, M. A. et al. Management of glioma in Victoria (1998–2000): Retrospective cohort study. Med. J. Aust. 184, 270–273 (2006).
Rusthoven, C. G. et al. The impact of adjuvant radiation therapy for high-grade gliomas by histology in the United States population. Int. J. Radiat. Oncol. Biol. Phys. 90, 894–902. https://doi.org/10.1016/j.ijrobp.2014.07.046 (2014).
Rusthoven, C. G. et al. Combined-modality therapy with radiation and chemotherapy for elderly patients with glioblastoma in the Temozolomide Era: A national cancer database analysis. JAMA Neurol. 73, 821–828. https://doi.org/10.1001/jamaneurol.2016.0839 (2016).
Salmaggi, A. et al. Multicentre prospective collection of newly diagnosed glioblastoma patients: update on the Lombardia experience. Neurol. Sci. 29, 77–83. https://doi.org/10.1007/s10072-008-0865-x (2008).
Shah, B. K., Bista, A. & Sharma, S. Survival trends in elderly patients with glioblastoma in the United States: A population-based study. Anticancer Res. 36, 4883–4886 (2016).
Yuan, Y. et al. Canadian brain cancer survival rates by tumour type and region: 1992–2008. Can. J. Public Health Rev. Can. Sante Publ. 107, e37–e42. https://doi.org/10.17269/cjph.107.5209 (2016).
Yabroff, K. R., Harlan, L., Zeruto, C., Abrams, J. & Mann, B. Patterns of care and survival for patients with glioblastoma multiforme diagnosed during 2006. Neuro Oncol. 14, 351–359. https://doi.org/10.1093/neuonc/nor218 (2012).
NICE Guidance. Brain tumours (primary) and brain metastases in adults [NG99]. Natl. Inst. Health care Excell. (2018).
Weller, M. et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 15, e395-403. https://doi.org/10.1016/S1470-2045(14)70011-7 (2014).
Stupp, R. et al. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 25(Suppl 3), iii93-101. https://doi.org/10.1093/annonc/mdu050 (2014).
Leece, R. et al. Global incidence of malignant brain and other central nervous system tumors by histology, 2003–2007. Neuro Oncol. 19, 1553–1564. https://doi.org/10.1093/neuonc/nox091 (2017).
Eden, M. et al. Impact of variation in cancer registration practice on observed international cancer survival differences between International Cancer Benchmarking Partnership (ICBP) jurisdictions. Cancer Epidemiol. 58, 184–192. https://doi.org/10.1016/j.canep.2018.10.019 (2019).
Korley, F. K., Pham, J. C. & Kirsch, T. D. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998–2007. JAMA 304, 1465–1471. https://doi.org/10.1001/jama.2010.1408 (2010).
Gibson, L. M. et al. Potentially serious incidental findings on brain and body magnetic resonance imaging of apparently asymptomatic adults: Systematic review and meta-analysis. BMJ 363, k4577. https://doi.org/10.1136/bmj.k4577 (2018).
Brennan, C. W. et al. The somatic genomic landscape of glioblastoma. Cell 155, 462–477. https://doi.org/10.1016/j.cell.2013.09.034 (2013).
Gusev, Y. et al. The REMBRANDT study, a large collection of genomic data from brain cancer patients. Sci. Data 5, 180158. https://doi.org/10.1038/sdata.2018.158 (2018).
Zuo, S., Zhang, X. & Wang, L. A RNA sequencing-based six-gene signature for survival prediction in patients with glioblastoma. Sci. Rep. 9, 2615. https://doi.org/10.1038/s41598-019-39273-4 (2019).
Aquilanti, E., Miller, J., Santagata, S., Cahill, D. P. & Brastianos, P. K. Updates in prognostic markers for gliomas. Neuro Oncol. 20, vii17–vii26. https://doi.org/10.1093/neuonc/noy158 (2018).
Louis, D. N. et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 131, 803–820. https://doi.org/10.1007/s00401-016-1545-1 (2016).
Yang, W. et al. Sex differences in GBM revealed by analysis of patient imaging, transcriptome, and survival data. Sci. Transl. Med. https://doi.org/10.1126/scitranslmed.aao5253 (2019).
McLendon, R. E. & Halperin, E. C. Is the long-term survival of patients with intracranial glioblastoma multiforme overstated?. Cancer 98, 1745–1748 (2003).
Shinojima, N. et al. The influence of sex and the presence of giant cells on postoperative long-term survival in adult patients with supratentorial glioblastoma multiforme. J. Neurosurg. 101, 219–226. https://doi.org/10.3171/jns.2004.101.2.0219 (2004).
Nakagawa, Y. et al. Clinical and molecular prognostic factors for long-term survival of patients with glioblastomas in single-institutional consecutive cohort. World Neurosurg. 106, 165–173. https://doi.org/10.1016/j.wneu.2017.06.126 (2017).
Hartmann, C. et al. Long-term survival in primary glioblastoma with versus without isocitrate dehydrogenase mutations. Clin. Cancer Res. 19, 5146–5157. https://doi.org/10.1158/1078-0432.CCR-13-0017 (2013).
Krex, D. et al. Long-term survival with glioblastoma multiforme. Brain 130, 2596–2606. https://doi.org/10.1093/brain/awm204 (2007).
Park, H. S., Lloyd, S., Decker, R. H., Wilson, L. D. & Yu, J. B. Limitations and biases of the surveillance, epidemiology, and end results database. Curr. Probl. Cancer 36, 216–224. https://doi.org/10.1016/j.currproblcancer.2012.03.011 (2012).
Acknowledgements
Mr. Poon is funded by Cancer Research UK Brain Tumour Centre of Excellence Award (C157/A27589).
Author information
Authors and Affiliations
Contributions
M.T.C.P. and P.M.B. conceptualized and designed this study. M.T.C.P. and P.M.B. extracted data from included studies. M.T.C.P. performed statistical analyses. C.L.M.S., J.D.F., P.M.B. and M.T.C.P. interpreted the results. M.T.C.P. drafted the manuscript. C.L.M.S., J.D.F., and P.M.B. critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Poon, M.T.C., Sudlow, C.L.M., Figueroa, J.D. et al. Longer-term (≥ 2 years) survival in patients with glioblastoma in population-based studies pre- and post-2005: a systematic review and meta-analysis. Sci Rep 10, 11622 (2020). https://doi.org/10.1038/s41598-020-68011-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-68011-4
This article is cited by
-
Targeting of REST with rationally-designed small molecule compounds exhibits synergetic therapeutic potential in human glioblastoma cells
BMC Biology (2024)
-
Survival prediction of glioblastoma patients using modern deep learning and machine learning techniques
Scientific Reports (2024)
-
Mutations in glioblastoma proteins do not disrupt epitope presentation and recognition, maintaining a specific CD8 T cell immune response potential
Scientific Reports (2024)
-
Immunotherapy with autologous dendritic cells in the complex treatment of malignant gliomas - results
Journal of Neuro-Oncology (2024)
-
A prognostic model for overall survival in recurrent glioma patients treated with bevacizumab-containing therapy
Discover Oncology (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
