
Abstract
Few studies investigated the respiratory outcomes of metformin use in patients with coexistent type 2 diabetes mellitus (T2DM) and chronic obstructive pulmonary disease (COPD). We want to compare the long-term respiratory endpoints of metformin use and nonuse in patients with T2DM and COPD. This retrospective cohort study enrolled patients with T2DM and COPD from Taiwan’s National Health Insurance Program between January 1, 2000, and December 31, 2012. Main outcomes were hospitalized bacterial pneumonia, hospitalization for COPD, noninvasive positive pressure ventilation (NIPPV), invasive mechanical ventilation (IMV), and lung cancer. In total, 20,644 propensity score-matched metformin users and nonusers were assessed. The adjusted hazard ratios (95% confidence intervals) of metformin use relative to nonuse for bacterial pneumonia, hospitalization for COPD, NIPPV, IMV, and lung cancer were 1.17 (1.11–1.23), 1.34 (1.26–1.43), 0.99 (0.89–1.10), 1.10 (1.03–1.17), and 1.12 (0.96–1.30). Metformin use also exhibited significant dose–response relationship with respect to the risks of bacterial pneumonia, hospitalization for COPD and IMV. Consistent results were found in the sensitivity test. This nationwide cohort study demonstrated that in patients with T2DM and COPD, metformin use was associated with higher risks of pneumonia, hospitalization for COPD, and IMV. If patients with COPD use metformin, vigilance with regard to their pulmonary condition may be required.
Similar content being viewed by others

Introduction
Chronic obstructive pulmonary disease (COPD) is a disease of progressive inflammation in the airway with partially reversible airflow limitation1. Type 2 diabetes mellitus (T2DM) is characterized by insulin resistance and hyperglycemia and is considered a chronic low-grade inflammatory disease2. Globally, approximately 11.7% of adults and nearly 400 million people have COPD3; additionally, it is a leading cause of death4. One in 11 adults and approximately 425 million people have T2DM, making it a leading contributor to the global disease burden5. Approximately 1.6–16% of people with COPD have diabetes. In addition, prevalence of T2DM increases as lung function deteriorates with COPD6, possibly because of the inflammatory process or use of steroids in COPD treatment7. Nearly 10% of patients with T2DM suffer from COPD8. Diabetes can worsen the progression and prognosis of COPD through the consequences of hyperglycemia, including reduced respiratory function, chronic inflammation, and susceptibility to bacterial infection9. Effective treatment of diabetes may improve the prognosis of COPD.
Because only few studies10 have assessed which diabetes treatments are suitable for patients with COPD, most clinicians follow the T2DM guidelines to treat patients with COPD, with metformin typically adopted as the first-line treatment. Metformin, possibly through the activation of AMP-associated protein kinase (AMPK), can reduce the accumulation of advanced glycated end product, oxidative stress, systemic inflammation, and improve insulin resistance11. In addition, it can reduce airway inflammation12 as well as improve respiratory muscle strength13 and forced vital capacity14. One animal study revealed that metformin could reduce airway glucose permeability and limit hyperglycemia-induced bacterial growth15. Several studies have reported that the use of metformin in patients with T2DM and COPD can lower the risk of all-cause mortality16,17,18. Only one randomized clinical trial of metformin use studied nondiabetic patients with exacerbated COPD, and no significant difference in clinical outcomes was observed19; but this study was a short-term (one month) trial with moderate number (n = 52) of patients. Because the evidence regarding metformin use in patients with COPD is so inconclusive, we conducted this retrospective cohort study to evaluate the long-term respiratory outcomes of metformin use in patients with T2DM and COPD.
Results
Participants
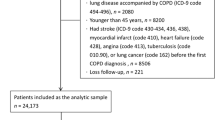
Of the 402,153 patients in the Longitudinal Cohort of Diabetes Patients (LHDB) who were newly diagnosed with T2DM and COPD between January 1, 2000, and December 31, 2012, 61,226 and 71,374 individuals were metformin users and nonusers, respectively. These users and nonusers constituted the cohorts of our study (Fig. 1). After propensity score matching to a 1:1 ratio, 20,644 metformin users and 20,644 nonusers were included in the outcome analysis. The two groups of patients were similar with respect to all covariates (Table 1). Considered jointly, the mean age of patients in these two groups was 63.9 years. The mean follow-up times for metformin users and nonusers were 5.01 years (standard deviation [SD] = 3.26) and 5.19 years (SD = 3.11), respectively.

Flow chart of study design including numbers of patients.
The outcome of hospitalized bacterial pneumonia
During follow-up, 3,133 (15.18%) of the 20,644 metformin users and 3,106 (15.05%) of the 20,644 metformin nonusers were admitted for bacterial pneumonia. The incidence rates (IRs) were 37.8 and 34.5 per 1,000 person-years; the adjusted hazard ratio (aHR) of metformin use vs. nonuse was 1.17, with a 95% confidence interval (CI) of 1.11–1.23 and a p value < 0.0001 (Table 2). The difference in the cumulative incidence of bacterial pneumonia between the metformin users and nonusers was illustrated using a Fine and Gray’s sub-distribution hazard model (Fig. 2A), which showed a higher risk of pneumonia in metformin users relative to nonusers. With respect to the risk of bacterial pneumonia, the aHRs for < 15, 15–29, and ≥ 30 cumulative defined daily dose (DDDs, relative to nonuse) were 1.09, 1.17, and 1.24, respectively (Fig. 3A); the aHRs of the prescribed daily doses of metformin, < 500, 500–749, and ≥ 750 mg/day (relative to nonuse), were 0.88, 1.17, and 1.20, respectively (Fig. 3B).

Cumulative incidence of bacterial pneumonia (A), hospitalization for COPD (B), and invasive mechanical ventilation (IMV, C), between metformin users and nonusers.

Outcomes of various dosages of metformin use relative to nonuse in patients with T2DM and COPD by (A) cumulative DDD and (B) prescribed daily dose (mg/day).
The outcome of hospitalized COPD
The IRs of hospitalization for COPD were 21.5 and 20.5 per 1,000 person-years for metformin users and nonusers, respectively; the aHR was 1.34 (95% CI, 1.26–1.43), with a p value < 0.0001. The cumulative incidence of hospitalization for COPD (Fig. 2B) revealed a higher risk of pneumonia in metformin users relative to nonusers. The aHRs for hospitalization with COPD for < 15, 15–29, and ≥ 30 cumulative DDDs were 1.29, 1.31, and 1.42, respectively (Fig. 3A); the aHRs of the prescribed daily doses of metformin, < 500, 500–749, and ≥ 750 mg/day, were 1.20, 1.33, and 1.69, respectively (Fig. 3B).
The outcomes of invasive and noninvasive ventilation
The IRs of noninvasive positive pressure ventilation (NIPPV) were 7.03 and 6.48 per 1,000 person-years for metformin users and nonusers, respectively; aHR was 0.99, with a 95% CI of 0.89–1.10 and p value of 0.95 (Table 2). The IRs of IMV were 22.2 and 18.4 per 1,000 person-years for metformin users and nonusers, respectively; aHR was 1.10, with a 95% CI of 1.03–1.17 and p value of 0.001. The cumulative incidence of invasive mechanical ventilation (IMV, Fig. 2C) revealed that metformin users had a higher risk of IMV relative to nonusers. With respect to the risk of IMV, the aHRs of the cumulative DDDs of metformin use of < 15, 15–29, and ≥ 30 were 1.10, 1.07, and 1.13, respectively (Fig. 3A); the aHRs of the prescribed daily doses of < 500, 500–749, and ≥ 750 mg/day of metformin were 0.90, 1.12, and 0.96, respectively (Fig. 3B).
The outcome of lung cancer
The IRs of lung cancer were 3.6 and 3.0 per 1,000 person-years for metformin users and nonusers, respectively; the aHR was 1.12 (95% CI of 0.96–1.30), with p = 0.12 (Table 2).
Sensitivity test
We conducted a sensitivity test by defining metformin use ≧ 180 days within 365 days after the new date as metformin users. Marginal structural Cox model was used to compare the outcomes of metformin users vesus matched non-users (Table 3). The metformin users were associated with higher risks of NIPPV [aHR 1.22 (1.20–1.25)], IMV [aHR 1.25 (1.22–1.27)], bacterial pneumonia [aHR 1.25 (1.22–1.28)], hospitalization for COPD [aHR 1.24 (1.21–1.26)], and lung cancer [aHR 1.22 (1.19–1.24)], as compared with non-users.
Discussion
Our study observed that metformin use in patients with T2DM and COPD increased the risks of bacterial pneumonia, hospitalization for COPD and use of IMV. The sensitivity test of metformin use for more than 6 months versus control also disclosed consistent results. The relative risks of the cumulative and prescribed daily dose of metformin seemed to have dose–response relationship.
Patients with T2DM have an increased risk of respiratory infections which could lead to frequent exacerbations of COPD and worse outcomes20. Treatment with corticosteroids is also associated with a higher risk of pneumonia in patients with COPD21. An animal study suggested that the use of metformin could attenuate bacterial growth by reducing the glucose permeability of the airway15. However, our study observed that the use of metformin increased the risk of bacterial pneumonia. In this study, metformin use increased the risk of hospitalization for COPD, this severe exacerbation might increase the use of systemic steroids and add the hazard of bacterial pneumonia.
T2DM has been associated with progression and worse prognosis of COPD9, 17. Greater COPD exacerbation may result in greater airflow limitation, respiratory failure, or hospitalization. Three cohort studies have demonstrated that metformin use could reduce the risk of mortality16,17,18. Bishwakarma et al.22 demonstrated that metformin use in patients with coexistent COPD and T2DM was associated with a lower risk of COPD-specific emergency room (ER) visits and hospitalizations, especially in patients with low-complexity COPD. In another study using randomized control of metformin use in nondiabetic patients with severe exacerbation of COPD, metformin use had no detectable effect on clinical outcomes or C-reactive protein19. Our study demonstrated that metformin users were associated with higher risk of the cumulative incidence of hospitalization for COPD. The Cox proportional hazards with a marginal model indicated that relative to nonuse, metformin use had an aHR of 1.34 (95% CI 1.26–1.43). The cumulative and prescribed daily doses of metformin also had dose–response trends with respect to the risk of hospitalization for COPD. The inconsistency among these 3 studies may be attributed to differences in sample sizes, patient ethnicities, and follow-up periods. Patients with acute exacerbated COPD often have low serum vitamin B12 levels23. Long-term metformin use was associated with lower serum vitamin B12 levels24, which may affect respiratory muscle function25, and have relationship with the exacerbation and hospitalization for COPD.
Oxygen therapy improves survival in patients with severe lung disease and hypoxemia. Mechanical ventilation is essential life-support for respiratory distress; the slow and sustained flow of air to distal airspaces minimizes airflow turbulence, reduces airway resistance, lowers the effort required for breathing, and relieve hypercapnic respiratory failure26. Sexton et al.13 conducted a prospective observational study on 6-month metformin use in 17 participants with moderate to severe COPD and observed that metformin use was associated with reduced symptoms of dyspnea and improved health status. By contrast, our results indicated that metformin use increases the risk of IMV. This inconsistency is probably due to differences in research designs and sample sizes. Mitochondria account for most of the body’s oxygen consumption in their production of adenosine triphosphate (ATP). Metformin can enter cells and inhibit complex I of the mitochondrial electron transport chain through organic cation transporter 1. This inhibition potentially reduces ATP production, which may lead to energy stress and potential mitochondrial dysfunction27. Metformin can diminish mitochondrial respiration in skeletal muscle28. Insufficient energy in respiratory muscle may affect pulmonary function, and the degree of mitochondrial dysfunction in the skeletal muscle was associated with the severity of diseases29. In addition, our study exhibited that metformin use increased the risks of bacterial pneumonia and hospitalization for COPD, both of which are prone to developing into hypercapnic respiratory failure and need the support of invasive mechanical ventilation.
Metformin has been reported have anticancer effects on many types of tumor. A meta-analysis of eight observational studies by Zhu et al.30 suggested that metformin use can yield a significant 16% reduction in the risk of lung cancer. However, in another meta-analysis of 11 cohort and four case–control studies, Nie et al.31 reported a null association between metformin use and lung cancer. Likewise, our study of metformin use in patients with T2DM and COPD revealed no significant association with lung cancer.
This study has some limitations. First, the national health insurance research database (NHIRD) does not provide data regarding family medical history, social economic status, education, body weight, smoking habits, alcohol-drinking habits, or physical activity, all of which may influence our investigated outcomes. Second, because NHIRD claims data do not include symptoms, signs, or the results of pulmonary functional tests, we could not calculate COPD severity scores. Thus, to balance the severity of COPD between metformin users and nonusers, we used clinical records (antibiotics use, oral corticosteroid use, hospitalization or ER visit) to assess the number of moderate and severe exacerbations of COPD. Third, much evidence favors positive roles for long-acting β2 agonists (LABAs) and long-acting muscarinic antagonists (LAMAs) in reducing COPD exacerbations; most of our patients had moderate or severe exacerbations. However, inhaled LABA and LAMA use was not prevalent, which indicated that the treatment was suboptimal. We must educate our physicians, encourage them to adhere to the guideline of COPD treatment, to improve patient’s care. Finally, indication bias might exist in the cohort study because patients and physicians may unconsciously select their preferred method of treatment. Therefore, we balanced multiple variables, such as basic demographics, comorbidity, severity of COPD and T2DM, and the use of various medications to minimize such bias.
In conclusion, our study observed that metformin use in patients with T2DM and COPD was associated with higher risks of bacterial pneumonia, hospitalization for COPD and use of IMV. However, because of some unmeasured or inevitable bias still exist in this cohort study, stringent prospective studies or randomized control clinical trials are warranted to verify our results.
Methods
Study design and participants
The NHIRD comprises health care data from approximately 99% of the population of Taiwan (approximately 23 million people)32. The NHIRD has encrypted data on date of birth; gender; area of residence; disease coding according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM); prescriptions; and clinical procedures. The LHDB is part of the NHIRD. The LHDB selected 120,000 newly diagnosed diabetes patients yearly from 1999 to 2012, and their medical records from 1996 to 2013 were collected.
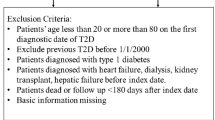
We involved patients who had a record of T2DM and COPD in the LHDB between January 1, 2000 and December 31, 2012. Patients’ study endpoints were withdrawal from the National Health Insurance program, occurrence of the outcome of interest, or December 31, 2013, whichever was earliest. The number of diagnoses of COPD (ICD-9-CM codes: 491, 492, and 496) was ≥ 2 for outpatients within 1 year or ≥ 1 diagnosis for hospitalization or ER visit. The criteria for the definition of COPD that use the ICD-9-CM in the NHIRD was validated in a previous study33. Moderate COPD exacerbation was indicated by prescription of antibiotics and/or oral corticosteroid; severe COPD exacerbation was indicated by hospitalization or an ER visit34. Patients were excluded if they were not between 40 and 100 years old, withdrew from the National Health Insurance program, underwent dialysis (V56.0, V56.8, V45.1), or were diagnosed with type 1 DM (250.1x), hepatic failure (570, 572.2. 572.4, 572.8), or lung cancer (162) before the index date. We also excluded patients who had been diagnosed with T2DM or COPD before January 1, 2000. We confirmed that all methods were performed in accordance to Declaration of Helsinki. This study was approved by the Institutional Review Board of China Medical University in central Taiwan (CMUH104-REC2-115). All information that could be used to identify patients or care providers was encrypted before release to protect participants’ privacy. Therefore, we were granted to waive of the informed consent.
Procedures
The date of concurrent diagnosis of T2DM and COPD was considered the new date. Within 90 days after the new date, patients who took metformin for at least 30 days were considered metformin users. Those who had not used metformin were considered metformin nonusers. The 91st date after the new date was considered the index date (Fig. 4). We identified potential explanatory variables, such as baseline characteristics, moderate or severe exacerbation of COPD, history of bacterial pneumonia, Charlson Comorbidity Index (CCI)35, Diabetes Complications Severity Index (DCSI) score36, and the use of specific classes of drugs (such as antidiabetics other than metformin, antihypertensive drugs, COPD drugs, statins, and aspirin). CCI and DCSI scores were calculated using patients’ status within 1 year before the index date.

We defined patients who have ever taken metformin within 90 days after new date as metformin users; the 91th day after new date as the index date.
Main outcomes
The main outcomes were hospitalized bacterial pneumonia (481, 486, 482.41, and 482.8), hospitalization for COPD, the use of noninvasive positive pressure ventilation (NIPPV, 93.90 and 93.91) or invasive mechanical ventilation (IMV, 96.7), and lung cancer. To preclude insufficient exposure (metformin use) time, patients who were admitted for bacterial pneumonia or COPD, used NIPPV or IMV, developed lung cancer, or died within 180 days after the index date were excluded. We have performed a sensitive test by defining the index date at 366th day after the new date, defining patients who used metformin ≧ 180 days within the 365 days between the new date and index date as metformin users, to compare the respiratory outcomes between the matched metformin users and control.
Statistical analyses
To maximize comparability, a propensity score matching was used to balance user and nonuser groups with respect to known variables37. We determined propensity scores through nonparsimonious multivariable logistic regression, with receipt of metformin as the dependent variable. We incorporated 35 clinically relevant covariates into our analysis as independent variables (Table 1). We applied the nearest-neighbors algorithm to match pairs, assuming that proportions of 0.995–1.0 were acceptable.
For the main outcomes, we censored patients at either the time of events or end of the follow-up on December 31, 2013, whichever came earlier. Using the Fine and Gray’s sub-distribution hazard model, we compared the cumulative incidence of events over time between metformin users and nonusers. We used a marginal structural Cox model, and robust sandwich standard error estimates to compare the outcomes while controlling for baseline covariates38. All analyses were done on the as-treated basis. We stopped following the metformin users when they discontinued metformin after the index date; on the contrary, the metformin non-users were censored when they started to use metformin after the index date. To assess dose effect, we analyzed the relative risks of bacterial pneumonia, hospitalization for COPD and IMV with regard to the cumulative DDD of metformin during the 90-day observational period (< 15, 15–29, and ≥ 30 DDD) and prescribed daily dose (< 500 mg, 500–749 mg, and ≥ 750 mg). DDD is a unit of measurement defined as the assumed average maintenance dose per day as the main indicated drug in an adult; the DDD is 2,000 mg for metformin. We report results as hazard ratios with 95% CI. A two-tailed p value less than 0.05 indicates significance. We used SAS statistical software (Version 9.4 for Windows; SAS Institute, Inc., Cary, NC, USA) for data analysis.
References
Vestbo, J. et al. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease, gold executive summary. Am. J. Respir. Crit. Care Med. 187, 347–365 (2013).
Shu, C. J., Benoist, C. & Mathis, D. The immune system’s involvement in obesity-driven type 2 diabetes. Semin. Immunol. 24, 436–442 (2012).
Adeloye, D. et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J. Glob. Health 5, 020415 (2015).
GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1459–1544 (2016).
International Diabetes Federation. IDF Diabetes Atlas 8th edn. https://diabetesatlas.org/key-messages.html. Accessed October 14, 2019 (2017).
Chatila, W. M., Thomashow, B. M., Minai, O. A., Criner, G. J. & Make, B. J. Comorbidities in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 5, 549–555 (2008).
Rana, J. S. et al. Chronic obstructive pulmonary disease, asthma, and risk of type 2 diabetes in women. Diabetes Care 27, 2478–2484 (2004).
Caughey, G. E. et al. Comorbidity in the elderly with diabetes: identification of areas of potential treatment conflicts. Diabetes Res. Clin. Pract. 87, 385–393 (2010).
Gläser, S., Krüger, S., Merkel, M., Bramlage, P. & Herth, F. J. Chronic obstructive pulmonary disease and diabetes mellitus: a systematic review of the literature. Respiration 89, 253–264. https://doi.org/10.1159/000369863 (2015).
Zhu, A. et al. Role of metformin in treatment of patients with chronic obstructive pulmonary disease: a systematic review. J. Thorac. Dis. 11, 4371–4378 (2019).
Stumvoll, M., Nurjhan, N., Perriello, G., Dailey, G. & Gerich, J. E. Metabolic effects of metformin in non-insulin-dependent diabetes mellitus. N. Engl. J. Med. 333, 550–554 (1995).
Park, C. S. et al. Metformin reduces airway inflammation and remodeling via activation of AMP-activated protein kinase. Biochem. Pharmacol. 84, 1660–1670 (2012).
Sexton, N. P., Metcalf, P. & Kolbe, J. Respiratory effects of insulin sensitization with metformin: a prospective observational study. COPD 11, 133–142 (2014).
Kim, H. J. et al. The impact of insulin sensitisers on lung function in patients with chronic obstructive pulmonary disease and diabetes. Int. J. Tuberc. Lung Dis. 14, 362–367 (2010).
Garnett, J. P. et al. Metformin reduces airway glucose permeability and hyperglycaemia-induced Staphylococcus aureus load independently of effects on blood glucose. Thorax 68, 835–845 (2013).
Yen, F. S., Chen, W., Wei, J. C., Hsu, C. C. & Hwu, C. M. Effects of metformin use on total mortality in patients with type 2 diabetes and chronic obstructive pulmonary disease: a matched-subject design. PLoS ONE 13, e0204859. https://doi.org/10.1371/journal.pone.0204859 (2018).
Ho, T. W. et al. Metformin use mitigates the adverse prognostic effect of diabetes mellitus in chronic obstructive pulmonary disease. Respir. Res. 20, 69. https://doi.org/10.1186/s12931-019-1035-9 (2019).
Mendy, A., Gopal, R., Alcorn, J. F. & Forno, E. Reduced mortality from lower respiratory tract disease in adult diabetic patients treated with metformin. Respirology 24, 646–651 (2019).
Hitchings, A. W., Lai, D., Jones, P. W., Baker, E. H. & Metformin in COPD Trial Team. Metformin in severe exacerbations of chronic obstructive pulmonary disease: a randomised controlled trial. Thorax 71, 587–593 (2016).
Lin, C. S. et al. Diabetes risks and outcomes in chronic obstructive pulmonary disease patients: two nationwide population-based retrospective cohort studies. PLoS ONE 12, e0181815. https://doi.org/10.1371/journal.pone.0181815 (2017).
Nannini, L. J., Lasserson, T. J. & Poole, P. Combined corticosteroid and long-acting beta (2)-agonist in one inhaler versus long-acting beta (2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 8, CD006826 (2013).
Bishwakarma, R. et al. Metformin use and health care utilization in patients with coexisting chronic obstructive pulmonary disease and diabetes mellitus. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 793–800 (2018).
Horadagoda, C., Dinihan, T., Roberts, M. & Kairaitis, K. Body composition and micronutrient deficiencies in patients with an acute exacerbation of chronic obstructive pulmonary disease. Intern. Med. J. 47, 1057–1063 (2017).
Bailey, C. J. Biguanides and NIDDM. Diabetes Care 15, 755–772 (1992).
Paulin, F. V., Zagatto, A. M., Chiappa, G. R. & Muller, P. T. Addition of vitamin B12 to exercise training improves cycle ergometer endurance in advanced COPD patients: a randomized and controlled study. Respir. Med. 122, 23–29 (2017).
Quon, B. S., Gan, W. Q. & Sin, D. D. Contemporary management of acute exacerbations of COPD: a systematic review and meta-analysis. Chest 133, 756–766. https://doi.org/10.1378/chest.07-1207 (2008).
Larsen, S. et al. Metformin-treated patients with type 2 diabetes have normal mitochondrial complex I respiration. Diabetologia 55, 443–449 (2012).
Brunmair, B. et al. Thiazolidinediones, like metformin, inhibit respiratory complex I: a common mechanism contributing to their antidiabetic actions?. Diabetes 53, 1052–1059 (2004).
Brealey, D. et al. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet 360, 219–223 (2002).
Zhu, N., Zhang, Y., Gong, Y. I., He, J. & Chen, X. Metformin and lung cancer risk of patients with type 2 diabetes mellitus: a meta-analysis. Biomed. Rep. 3, 235–241 (2015).
Nie, S. P., Chen, H., Zhuang, M. Q. & Lu, M. Anti-diabetic medications do not influence risk of lung cancer in patients with diabetes mellitus: a systematic review and meta-analysis. Asian Pac. J. Cancer Prev. 15, 6863–6869 (2014).
Cheng, T. M. Taiwan’s new national health insurance program: genesis and experience so far. Health Aff. 22, 61–76 (2003).
Ho, T. W. et al. Validity of ICD9-CM codes to diagnose chronic obstructive pulmonary disease from National Health Insurance claim data in Taiwan. Int. J. Chron. Obstruct. Pulmon. Dis. 13, 3055–3063 (2018).
Rodriguez-Roisin, R. Towards a consensus definition for COPD exacerbations. Chest 117, 398S-401S (2000).
Charlson, M. E., Pompei, P., Ales, K. L. & MAcKenzie, C. R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40, 373–383 (1987).
Young, B. A. et al. Diabetes complications severity index and risk of mortality, hospitalization, and health care utilization. Am. J. Manag. Care 14, 15–23 (2008).
D’Agostino, R. B. Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 17, 2265–2281 (1998).
Lin, D. Y. Cox regression analysis of multivariate failure time data: the marginal approach. Stat. Med. 13, 2233–2247 (1994).
Acknowledgements
We thank Dr. Hsin-Kuo Ko for his influential recommendation of the study design and detailed discussions of the results. This manuscript was edited by Wallace Academic Editing. This work was supported by grants from the Ministry of Health and Welfare, Taiwan (MOHW107-TDU-B-212-123004), China Medical University Hospital, Academia Sinica Stroke Biosignature Project (BM10701010021), Ministry of Science and Technology Clinical Trial Consortium for Stroke (MOST 106-2321-B-039-005)”, Tseng-Lien Lin Foundation in Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds in Japan.
Author information
Authors and Affiliations
Contributions
F.S.Y. and C.M.H designed the study. J.C.W and Y.C.Y collected data and coordinated the study. Y.C.Y and C.C.H participated in the data validation and data analysis, all authors discussed and interpreted the results. F.S.Y, C.C.H, and C.M.H. wrote the manuscript. C.C.H. and C.M.H., who takes responsibility for the content of the manuscript, including the data and analysis. All authors undertook in the revision of this report and approval of the final version. The sponsors had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yen, FS., Wei, J.CC., Yang, YC. et al. Respiratory outcomes of metformin use in patients with type 2 diabetes and chronic obstructive pulmonary disease. Sci Rep 10, 10298 (2020). https://doi.org/10.1038/s41598-020-67338-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-67338-2
This article is cited by
-
Transcriptomic data exploration of consensus genes and molecular mechanisms between chronic obstructive pulmonary disease and lung adenocarcinoma
Scientific Reports (2022)
-
Metformin use and respiratory outcomes in asthma-COPD overlap
Respiratory Research (2021)
-
A geroscience perspective on immune resilience and infectious diseases: a potential case for metformin
GeroScience (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
