
Abstract
Due to the symptoms, patients with acute type A aortic dissection are first seen by the ambulance service and diagnosed at the emergency department. How often an aortic dissection occurs in an emergency department per year has been studied. The incidence in the emergency department may be used as a quality marker of differential diagnostics of acute chest pain. A multi-institutional retrospective study with the municipal Berlin hospital chain Vivantes and its Department of Pathology and the Charité - University Medicine Berlin was performed. From the Berlin Hospital Society, the annual numbers of publicly insured emergency patients were obtained. Between 2006 and 2016, 631 aortic dissections were identified. The total number of patients treated in the emergency departments (n = 12,790,577) was used to calculate the “emergency department incidence.” The autopsy data from six clinics allowed an estimate on how many acute type A aortic dissections remained undetected. Across all Berlin hospitals, the emergency department incidence of acute type A aortic dissection was 5.24 cases in 100,000 patients per year. In tertiary referral hospitals and, particularly, in university hospitals the respective incidences were markedly higher (6.7 and 12.4, respectively). Based on the autopsy results, about 50% of the acute type A aortic dissection may remain undetected, which would double the reported incidences. Among different hospital types the emergency department incidences of acute type A aortic dissection vary between 5.93/100,000 and 24.92/100,000. Aortic dissection; Incidence; Emergency Department; Epidemiology
Similar content being viewed by others


Introduction
Acute type A aortic dissection (ATAAD) is part of the preclinical differential diagnosis of acute chest pain. According to the current literature, the population-based incidence of ATAAD is stated between 2.1 and 16.3 per 100,000 persons1,2,3,4,5,6,7,8,9,10,11,12. It is associated with a high mortality ranging from 26% in surgically treated patients to 58% in medically treated patients13. ATAAD is associated with a high risk for post-traumatic stress disorder and has negative effects on the patients’ physical and mental health14. Aortic dissection usually manifests with sudden thoracic or back pain13,15. Increased awareness may further accelerate the diagnostic workup16. As the majority of patients with symptoms of an ATAAD are admitted through the emergency department (ED), the emergency staff needs to be aware of the expected incidence of ATAAD. Surgical care of an ATAAD is a time critical event and can only be carried out in specialized clinics17. Immediate transportation with a ground-based rescue device to the target hospital is the quickest option and is also necessary from a medical law perspective18,19. According to the Federal Statistical office, Berlin has 3,613,495 inhabitants and 83 hospitals. The aim of this study was to gather the current knowledge on the incidence of ATAAD among different populations and to determine the true incidence among patients treated in an ED in the region of Berlin.
Results
Emergency department incidence und pathology data
With 12,734,308 ED patients from 2006 to 2016 in Berlin and 631 ATAADs, an ED incidence of 4.96/100,000 was calculated. During the observation period from 2006 to 2016, all these 631 clinical cases of ATAAD were transferred to and treated at the German Heart Center Berlin or the cardiac surgery department of Charité-University Medicine Berlin. Of these, 410 (65%) were men and 221 (35%) were women. The average age was 61.4 ± 13.8 years. The youngest patient was 23 and the oldest patient was 90 years old. The mean body mass index (BMI) was 27.2 ± 4.9 kg/m2 and ranged from 16.3 to 55.56 kg/m2. In 425 (67.8%) cases, a pre-existing arterial hypertension was detected. Eighty-one (12.8%) patients had coronary artery disease. In 43 (6.8%) patients, type 2 diabetes mellitus was detected. Pre-existing aortic diseases such as aortic aneurysm or ectasia of the aorta were found in 86 (13.6%) of the patients. Fifteen (2.4%) patients had a Stanford type B dissection in their clinical history. One hundred ninety (30.1%) had a history of nicotine abuse, and 32 (5.1%) patients were alcohol addicted. Arteriosclerosis was found in 51 (8.1%) of the patients. A hereditary connective tissue disorder (Marfan or Ehlers-Danlos) was found in 18 (2.9%) patients. 66 (10.5%) patients were known to have hypothyroidism. There were only three (0.5%) cases of pregnancy and five (0.8%) cases of cocaine abuse.
The Charité and the Vivantes clinics play a major role in the care of critically ill patients. We assigned all patients to the respective clinics in Berlin. We divided them into three groups. The first group includes all Charité patients, the ED group patients from Vivantes clinics formed the second group. The third and last group includes all other EDs in Berlin. Detailed data including the distribution of patient characteristics among different types of hospitals are shown in Table 1. The Charité and the Vivantes clinics provided us with their own ED patient numbers. With our data, it was possible to calculate the exact incidence in the ED for the respective observation periods.
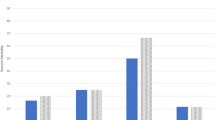
In Table 2 the cases of ATAAD, the population and the incidence are compared for the congruent period from 2010–2016. The first column contains all patients in the Berlin region.
The following columns compare the Charité clinics, the Vivantes clinics and all other hospitals in terms of cases, the emergency department incidence and the extrapolated data.The Charité has 131 ATAAD cases and an ED population of 1,050,994. This results in an incidence of 12.46/100,000. At the Vivantes hospitals, 153 cases of ATAAD were found among 2,112,610 ED patients resulting in an ED incidence of 7.24/100,000. The remaining Berlin hospitals had 5,195,208 ED patients and 154 ATAAD cases. The ED incidence was 2.96/100,000. (Table 2).The information of the pathology department of six Vivantes clinics was used to estimate how many ATAADs went undetected. The ATAAD was not known prior to the autopsy. Compared with the data from the German Heart Institute and the Vivantes clinics, this suggests that only one of every two ATAAD cases was detected. The details are shown in Table 3. Extrapolating this assumption to all hospitals, the incidence of ATAAD in the EDs all over Berlin would increase to 10.48/100,000, to 14.48/100,000 at Vivantes, to 24.92/100,000 at the Charité, and to 5.93/100,000 at all other hospitals in Berlin (Table 2).
Discussion
The literature review has shown that the data on the incidence of ATAAD vary substantially. The study characteristics are summarized in Table 4. It is important to provide an accurate estimation of the incidence and also to consider its development over the years. This may serve as a quality indicator for emergency services, statistical offices, public health offices, legal medicine, and other healthcare providers. The total population of the 14 studies included 1,733,937,352 person years. The indicated incidences of all population-based studies were very heterogeneous and ranged from 2.1 to 16.3/100,000 inhabitants1,2,3,4,5,6,7,8,9,10,11,12.
A retrospective study from Rogers et al. 2011 roughly estimated an ED incidence for acute aortic dissection in the United States. They assumed 10,000 cases of AAD annually and 100,000,000 ED visits in the same time period. This led to an ED incidence of 10/100,000 patients20.
Our study confirmed this assumption using exact numbers of ED patients and ATAAD cases.
Another study analyzed the incidence in clinical and forensic autopsies in the regions of Berlin and Brandenburg. The analysis provided 1150.5 cases of ATAAD per 100,000 autopsies2. In a retrospective study from Mollo et al. in 1983, autopsy reports were analyzed from 1932 to 1981. They could show a relative frequency of 1/168 or an incidence of 595/100,000 autopsies21. The incidence rates in the population-based studies were related to AADs without distinction between type A and type B. For this reason, we calculated the incidence for the ATAADs from the given data. A population-based incidence of 2.3/100,000 for all population-based studies was obtained. Due to the high preclinical mortality and missing forensic and clinical autopsy data, the number of unreported cases can safely be assumed to be very high. 26% of the patients who received surgical treatment due to a type A dissection died within the clinic. The mortality of the conservatively treated patients was 58%13. The ED incidence in the Berlin area varied over the years, but no sustained increase occurred. Across all 83 hospitals in Berlin, an ED incidence of 4.96/100,000 was calculated for the period from 2006 to 2016. The German Heart Center is responsible for the surgical care of nearly 90% of acute type A aortic dissections in the Berlin region. Looking separately at the largest hospital companies, the incidence at the Vivantes clinics was 7.24/100,000, and at the Charité hospitals it was 12.46/100,000 emergency patients. Hospitals with a higher level of care and a simultaneous “Chest Pain Unit” qualification are increasingly being approached by the ambulance service for the symptom of chest pain. With greater expertise and better occupation in the ED, these institutions generate larger numbers of cases and have a higher incidence of ATAAD in the ED. The study showed higher prevalence with lower incidence of ATAAD in the Vivantes clinics compared to the Charité clinics. This is due to the different number of EDs (Vivantes n = 9, Charité n = 3). The autopsy results and these data led to the conclusion that probably only one in two ATAADs was diagnosed. Following this assumption for the time period from 2010 to 2016, the incidence for all Vivantes clinics increased from 7.24/100,000 to 14.48/100,000. Extrapolating this assumption, the incidence in the Charité increased from 12.46/100,000 to 24.92/100,000. There is only one study that assessed the incidence in EDs in the United States of America. It provides a rough estimateof 10 AAD cases of any type among 100,000 ED patients20. We calculated an ED incidence of 5.24 ATAAD/100,000 for Berlin. Under the assumption that only one out of two cases are actually detected, the incidence increases to 10.48/100,000, which is almost identical to the United States of America. This incidence is higher than the average extrapolated population-based incidence in Berlin. In relation to the Berlin population during the study period (37,843,130 person years) and 1262 extrapolated cases of ATAAD, the population-based incidence was 3.3/100,000. The examination of the section material shows a very high number of unreported cases. In all deceased patients undergoing autopsy, the ATAAD was not known prior to the autopsy. Whether or not ATAAD was causal for death is not known, but, considering the high in-hospital mortality of untreated ATAAD we can assume that it was the cause of death in the majority of cases22. To reduce this number, it would be necessary to take a closer look at the deceased patients of each hospital. A study by Modelmog et al. could show that the autopsy findings are not in line with the diagnosis given on the death certificate in 45% of the cases23. Burton et al. from 2003 pointed out that an autopsy can reveal important and unsuspected diagnoses. The discrepancy between the clinical diagnosis and the findings of the autopsy has decreased over time. But, it remains so high that a continuation of the autopsies is indicated24.Brinkmann et al. provides data on the development of clinicopathologic and forensic autopsy rates between 1994 and 1999. Especially in Berlin, the autopsy rate decreased by 3.9% within 5 years, from 15.3% in 1994 to 11.4% in 199925.
The study periods vary between Charité (2010–2016), Vivantes and Berlin (2006–2016). Unfortunately, it was not possible to gather data on the missing years to get equal study periods. The ED population for 2016 was missing and had to be estimated based on the evolution of patient numbers. As a result, the numbers could be under- or overestimated. The autopsy data was provided only from the Vivantes clinics. The overall autopsy rate was 5.95%. This is not enough to provide reliable numbers on undetected cases of ATAAD. Therefore, the extrapolation of these undetected numbers to all Berlin hospitals should be considered with care. For a more detailed assessment, autopsy data from all hospitals in Berlin and the Charité would be necessary. The new data on incidence in EDs should sensitize the hospitals and ambulance services to this acute disease. The goal in preclinical care should be the establishment of a standard operating procedure for the symptom complex of chest pain in which the aortic dissection detection risk score is firmly anchored. There, a special focus should be on patients who are delivered by the ambulance or the rescue service.
Conclusion
Our results underline a higher incidence in the EDs compared with the population-based incidence in the general population of Berlin. The ED incidence in the period from 2010 to 2016 varies between 2.96/100,000 and 12.46/100,000 among different types of hospitals. The population-based incidence for the entire Berlin population from 2010 to 2016 is 3.45/100,000. Specialized clinics show significantly higher case numbers. The ATAAD is a severe disease and it is one of the four differential diagnoses of acute chest pain. Lower than expected incidences may mean that ATAAD remains undetected in a considerable number of patients. The pathology department information showed, that only one in two cases of ATAAD is detected. Under this assumption, the ED incidences and the population-based incidence would be twice as large.
Material and Methods
Study design
The databases PubMed und Google Scholar were used to search for studies on the subject of incidence of aortic dissection. Incidences in the fields of population, ED, pathology autopsies, and forensic medicine were considered. “Acute aortic dissection type A incidence” and “acute aortic dissection at autopsy” were used as search terms. The search on Pubmed and Google Scholar yielded 23,056 studies. The abstracts were screened, and studies were excluded if they dealt with other topics, full-text was not available, or language was different than English or German. Based on these criteria, 23,020 studies were excluded. Twenty-two of the remaining 34 full-text studies fulfilled all criteria for eligibility and met all criteria. The bibliographies of the included studies were explored for further relevant studies. In an additional search, six more relevant studies were identified. Fourteen articles that deal with autopsy-, population-, forensic medicine incidence, and ED incidence of ATAAD are summarized in Table 4, which includes the following information: kind of incidence, author, date, study type, population size and incidence. The study from Kurz et al. was considered twice, for a population based incidence and a forensic medicine incidence of ATAAD2.
Data collection
The only two institutions surgically treating ATAAD in Berlin are the German heart Centre and the Department of Cardiovascular Surgery, Charité- University Medicine Berlin. Thus the number of 631 patients was taken from the archives of these hospitals covering the years 2006 to 2016. To estimate a population of ED patients in Berlin for the years 2006 to 2016, we contacted the two major health care providers, the municipal Berlin hospital chain Vivantes, running nine large hospitals, and the Charité-University Medicine Berlin, with three hospital sites. For Charité-University Medicine hospitals, we received the numbers of ED patients for the years 2010 to 2016 directly from the heads of the respective departments. The Vivantes clinics provided us with the data from 2006 to 2015. The missing data from 2016 had to be calculated based on the annual increase. From the Berlin Hospital Society, we received the annual numbers of publicly insured emergency patients for the years 1998 to 2015. Estimating the rate of privately insured patients at 10%, we added the respective numbers. For the year 2016, no data were available. We therefore extrapolated the number for this year according to the average yearly increment of patient numbers, resulting in a total of 1,268,507 patients in 2016, including private patients.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Charité-Universitätsmedizin Berlin (Ethics Subcommittee 2 of Campus Virchow-Klinikum, registration number: EA2/126/14) and complies with the Declaration of Helsinki. An informed consent by the patient to participate in the study was not necessary on the part of the ethics committee.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
References
Reutersberg, B. et al. Hospital Incidence and In-Hospital Mortality of Surgically and Interventionally Treated Aortic Dissections: Secondary Data Analysis of the Nationwide German Diagnosis-Related Group Statistics From 2006 to 2014. J. Am. Heart Assoc. 8, 5–12 (2019).
Kurz, S. D. et al. Insight into the incidence of acute aortic dissection in the German region of Berlin and Brandenburg. Int. J. Cardiol. 241, 326–329 (2017).
Yeh, T.-Y. et al. Epidemiology and Medication Utilization Pattern of Aortic Dissection in Taiwan. Medicine (Baltimore). 94, e1522 (2015).
Olsson, C., Thelin, S., Stahle, E., Ekbom, A. & Granath, F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 114, 2611–2618 (2006).
Landenhed, M. et al. Risk profiles for aortic dissection and ruptured or surgically treated aneurysms: a prospective cohort study. J Am Hear. Assoc 4, e001513 (2015).
Sato, F. et al. Newly diagnosed acute aortic dissection: characteristics, treatment modifications, and outcomes. Int. Heart J. 46, 1083–1098 (2005).
Howard, D. P. J. et al. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the oxford vascular study. Circulation 127, 2031–2037 (2013).
Clouse, W. D. et al. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc 79, 176–180 (2004).
Melvinsdottir, I. H. et al. The incidence and mortality of acute thoracic aortic dissection: results from a whole nation study. Eur. J. Cardiothorac. Surg. https://doi.org/10.1093/ejcts/ezw235 (2016).
Mody, P. S. et al. Trends in aortic dissection hospitalizations, interventions, and outcomes among medicare beneficiaries in the United States, 2000-2011. Circ. Cardiovasc. Qual. Outcomes 7, 920–928 (2014).
Pacini, D. et al. Acute aortic dissection: epidemiology and outcomes. Int J Cardiol 167, 2806–2812 (2013).
McClure, R. S. et al. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: A population-based study. J. Thorac. Cardiovasc. Surg. 155, 2254–2264.e4 (2018).
Hagan, P. G. et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 283, 897–903 (2000).
Adam, U. et al. Health-related quality of life of patients after surgery for acute Type A aortic dissection. Interact. Cardiovasc. Thorac. Surg. 1–6. https://doi.org/10.1093/icvts/ivy036 (2018).
Hennessy, T. G., Smith, D., McCann, H. A., McCarthy, C. & Sugrue, D. D. Thoracic aortic dissection or aneurysm: clinical presentation, diagnostic imaging and initial management in a tertiary referral centre. Ir J Med Sci 165, 259–262 (1996).
Kurz, S., Gieb, M., Kuppe, H., Tsokos, M. & Buschmann, C. Die akute Typ-A-Dissektion nach Stanford – Fallstricke und Implikationen für die notfallmedizinische Praxis TT - Stanford’s Acute Aortic Dissection Type A – Pitfalls and Implications for Emergency Medical Practice. Der Notarzt 33, 20–24 (2017).
Zaschke, L. et al. Acute type A aortic dissection: Aortic Dissection Detection Risk Score in emergency care – surgical delay because of initial misdiagnosis. https://doi.org/10.1177/2048872620914931 (2020).
Kurz, S. D., Falk, V., Buschmann, C. T. & Peters, M. Medikolegale Aspekte des präklinischen Managements von „akuten Aortensyndromen“. Der Notarzt, https://doi.org/10.1055/a-1075-1868 (2020).
Matschilles, C., Mochmann, H.-C., Syrmas, G., Zaschke, L. & Kurz, S. Interhospital transfer of patients suffering from acute aortic dissection by helicopter and ground-based emergency medical services. Resuscitation 130, e136 (2018).
Rogers, A. M. et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circulation 123, 2213–2218 (2011).
Mollo, F., Comino, A. & Passarino, G. Incidence of acute aortic dissection at autopsy. Chest 83, 712 (1983).
Mehta, R. H. et al. Predicting death in patients with acute type a aortic dissection. Circulation 105, 200–206 (2002).
Modelmog, D. & Goertchen, R. Der Stellenwert von Obduktionsergebnissen in Beziehung zu Sektionsfrequenz und amtlicher Todesursachenstatistik (Görlitzer Studie). Dtsch. Arztebl. 89, 33–37 (1992).
Burton, E. C., Mcdonald, K. M., Goldman, L. & Page, P. Changes in Rates of Autopsy-Detected. Jama 289, 2849–2856 (2014).
Brinkmann, B., Du Chesne, A. & Vennemann, B. Aktuelle daten zur obduktionsfrequenz in Deutschland. Dtsch. Medizinische Wochenschrift 127, 791–795 (2002).
Author information
Authors and Affiliations
Contributions
M.W., H.H., S.D.K. were responsible for the study concept and design. M.W., V.F., H.H., J.T., B.L., E.G., W.B., S.D.K. performed the acquisition of the data. M.W., H.H., S.D.K. analyzed and interpreted the data. M.W., H.H., S.D.K. wrote the manuscript.M.W., V.F., J.J.E.G., H.H., J.T., B.L., E.G., W.B. H.H., S.D.K. performed a critical revision of the manuscript for important intellectual content. The statistical expertise, and acquisition of funding was performed by M.W., H.H. and S.D.K. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wundram, M., Falk, V., Eulert-Grehn, JJ. et al. Incidence of acute type A aortic dissection in emergency departments. Sci Rep 10, 7434 (2020). https://doi.org/10.1038/s41598-020-64299-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-64299-4
This article is cited by
-
Acute Lung Injury in aortic dissection : new insights in anesthetic management strategies
Journal of Cardiothoracic Surgery (2023)
-
Morbid obesity impacts mortality among inpatients with type a aortic dissection: an analysis of the national inpatient sample
Journal of Cardiothoracic Surgery (2023)
-
Predictive value of admission CO2 combining power combined with serum sodium for the prognosis in acute Stanford type A aortic dissection patients
Scientific Reports (2023)
-
Interdisciplinary German clinical practice guidelines on the management of type B aortic dissection
Gefässchirurgie (2023)
-
A retrospective observational study of serum uric acid and in-hospital mortality in acute type A aortic dissection
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
