
Abstract
Multiplicity of infection (MOI) and genetic diversity of P. falciparum infections are important surrogate indicators for assessing malaria transmission intensity in different regions of endemicity. Determination of MOI and diversity of P. falciparum among asymptomatic carriers will enhance our understanding of parasite biology and transmission to mosquito vectors. This study examined the MOI and genetic diversity of P. falciparum parasite populations circulating in Mbita, a region characterized as one of the malaria hotspots in Kenya. The genetic diversity and multiplicity of P. falciparum infections in 95 asymptomatic school children (age 5–15 yrs.) residing in Mbita, western Kenya were assessed using 10 polymorphic microsatellite markers. An average of 79.69% (Range: 54.84–95.74%) of the isolates analysed in this study were polyclonal infections as detected in at least one locus. A high mean MOI of 3.39 (Range: 2.24–4.72) and expected heterozygosity (He) of 0.81 (Range: 0.57–0.95) was reported in the study population. The analysed samples were extensively polyclonal infections leading to circulation of highly genetically diverse parasite populations in the study area. These findings correlated with the expectations of high malaria transmission intensity despite scaling up malaria interventions in the area thereby indicating the need for a robust malaria interventions particularly against asymptomatic carriers in order to attain elimination in the region.
Similar content being viewed by others

Introduction
Malaria continues to be a major public health problem in many parts of the world despite numerous national and international efforts in combatting the ongoing disease transmission. Although enormous success in the fight against the disease has been registered, reports have indicated an insignificant progress in the reduction of global malaria cases for the period 2014–20181. An increase in the global incidence of malaria cases from 219 million in 2017 to 228 million in 2018 with a staggering 405 000 related deaths was registered1,2. Sub-Saharan Africa bears the greatest malaria cases and death rates compared to other regions like South-East Asia, Eastern Mediterranean, Western Pacific, and the Americas with an unprecedented 213 million malaria cases1.
In Kenya, about 74 percent of the total population are reported to be at risk of malaria infection and regions such as the coastal areas and western part of the country records the highest transmission intensity3,4. Children registered the highest prevalence of the disease and recorded an average of 8 percent and 15 percent among younger (<5 years) and older (5–15 years) age categories respectively5. Older children living in endemic environments around lake shores recorded a much higher prevalence of about 38 percent6. In a bid to attain its goal of a “Malaria-free Kenya”, the country has implemented many malaria control and eradication interventions including; the use of Artemisinin based Combination Therapy (ACT) as a first line of treatment, Long-Lasting Insecticidal Net (LLIN), Intermittent Presumptive Treatment in pregnancy (IPTp), Indoor Residual Spraying (IRS) and Rapid Diagnostic Test (RDT) for efficient parasite diagnosis7,8.
A larger proportion of malaria morbidity and mortality studies were centred on preschool-aged children (2–4 years of age). This group contributes a substantial number of incidence to the global malaria burden each year9,10,11. The management and epidemiology of malaria in school-age children as a group has initially received little attention in comparison to the pregnant women and children under the age of five years groups11,12,13,14. In many endemic settings, malaria contributes immensely to the annual school absenteeism and poor academic performance among school children9,13,14. Older children in high malaria transmission areas develop parasite specific immunity against Plasmodium parasite and this contributes to reduction in clinical malaria episodes and high prevalence of asymptomatic parasite carriers15,16,17. As a result, malaria asymptomatic school children might not be absent from school due to clinical malaria episodes but may serve as major reservoir for the transmission of the disease11,18,19.
Overall, progress towards malaria control and elimination has stalled across all World Health Organisation (WHO) regions. The stagnancy in the global fight against the disease is partly due to decreased funding from international donors1,20,21,22,23. However, the high prevalence of asymptomatic carriers especially among older children19,24,25,26,27,28, high recombination rates among distinct P. falciparum clones in endemic settings leading to emergence of highly diverse parasite isolates, rapid emergence and distribution of drug resistant P. falciparum parasite strains29,30,31,32,33, and prevalence of infections characterized by multiple genetically distinct parasite strains are some of the major contributing factors hindering the global malaria control and elimination31,34,35. In highly endemic environments, many individuals carry multiple parasite clones36,37,38. This may have both positive and negative implications in the fight against malaria. The carriage of multiple distinct parasite clones by an individual is reported to enhance the development of multiple strain specific anti-parasite immunity. However, due to an intense intra-host competition, harbouring multiple distinct parasite clones is also implicated in high gametocyte production and emergence of highly virulent and drug resistant parasite strains32,39,40,41,42,43.
Multiplicity of infection (MOI) and genetic diversity of P. falciparum infection are important surrogate tools for the determination of malaria transmission intensity in different regions of endemicity44,45,46. These indices of P. falciparum parasite infections are also used in determining the impact of some key malaria interventions like drug and vaccine efficacy studies29,47,48. Numerous studies about multiplicity and diversity of P. falciparum infections have been carried out in various WHO regions using different tools including size-polymorphic antigens and microsatellite markers followed by agarose gel and capillary electrophoresis respectively, single nucleotide polymorphism genotyping, amplicon ultra-deep sequencing and whole genome sequencing36,49. The use of molecular genotyping of polymorphic antigenic markers like merozoite surface protein (MSP) 1 and 2, glutamate rich protein (Glurp) for parasite diversity studies are faced with some criticisms due to the fact that these genes are implicated to be under strong immune selection44,50,51,52. Amplicon ultra-deep sequencing and whole genome sequencing techniques have high sensitivity and specificity particularly to detect minority clones in case of multiclonal infections52. However, the costs and time factors attached to the use of these techniques are relatively high thereby limiting their application especially in resource scarce settings. Microsatellite markers are highly polymorphic, widely distributed in the Plasmodium genome, perceived to be selection neutral and readily amplifiable using cheap methods like PCR35,53,54. These criteria have made them an ideal tool for the estimation of parasite genetic diversity and MOI36,46,48.
While studies about asymptomatic Plasmodium parasite carriage among school children have been reported18,26,28,55, studies on diversity level and multiplicity of P. falciparum infections among this group still remained scanty. This study was carried out to investigate the diversity and multiplicity of P. falciparum infections among asymptomatic school children (age 5–15 yrs.) in one of the highly malaria endemic regions of Kenya in order to provide an up-to-date critical information for monitoring parasite transmission dynamics and effective evaluation of the impact of currently implemented malaria control interventions in the area.
Materials and Methods
Ethics statement
The Kenya Medical Research Institute (KEMRI) Scientific and Ethics Review Unit (SERU) granted approval for the original study (KEMRI/RES/7/3/1). Consent for sample reuse was part of the original consent form. Study participants were only enrolled after obtaining a written informed consent from their parents or legal guardians. Participants above 12 years also provided assent in addition to parental consent. All experiments were performed in accordance with the relevant guidelines and regulations.
Study site and sample collection
Study site
The study was conducted in Mbita sub-county, situated in the shores of Lake Victoria in Homa Bay County formerly Nyanza Province in western Kenya. The district is bordered from the north, west and south by Lake Victoria and located between latitudes 0° 21′ and 0° 32′ South and longitudes 34° 04′ and 34° 24′ East. The area of the district is about 163.28 km2 and is approximately 400 km west of the capital city of Kenya, Nairobi. Mbita sub-county has a population of about 115,896 and the major economic activities include subsistence farming, fishing, small scale businesses and domestication of animals like sheep, goat, chicken, pig and cattle56. Majority of the residents live in a compound system which comprises of one or more households together. The housing structures range from traditional mud with grass thatched huts to modern concrete and corrugated iron buildings56. The region experiences two periods of rainfall, from March to June and then October to November each year57 and is characterized as one of the HIV hotspots with some of the poorest health indicators in Kenya. Due to the biannual rainfall pattern and the proximity to the shores of Lake Victoria, the region experiences a perennial transmission of malaria thereby making the disease the leading cause of morbidity and mortality among children in the region58.
Sample collection
The study used archived samples that were previously collected from asymptomatic school children in Mbita, western Kenya. The participants were recruited from various primary schools in the region and enrolled between December 2016 and October 2018 as part of a study to evaluate symbiotic microbes and mosquito vector competence using membrane feeding assays in a bid to isolate and characterize potential malaria transmission blocking endosymbiont candidates. Blood samples were obtained from school children aged between 5–15 years and were screened for Plasmodium parasite carriage using SD Bioline malaria Ag Pf/Pan (HRP-II/pLDH) Rapid Diagnostic Test (RDT) and microscopy. A drop of blood from each participant was also obtained for the preparation of thick and thin blood films, stained with 10% Giemsa for 10 minutes and used for the microscopy diagnosis. Two drops of blood were collected from each individual on a filter paper (Whatman 3MM; Whatman, Maidstone, United Kingdom), for genomic DNA extraction. The filter paper dry blood spots (DBS) samples were air dried and sealed in airtight plastic bags containing silica gel and were stored at −20 °C until usage. The blood smear slides were read by a well-trained microscopists and any slide with no observable parasites in 100 microscopic fields were declared negative; gametocytes were counted against 500 white blood cells while the asexual parasites were counted against 200 white blood cells. Slides that were declared negative were all double-read and confirmed to be negative if no parasites are observed in 200 microscopic fields. A second microscopist re-read all the slides for the purpose of quality control. A total of 95 RDT and microscopy positive filter paper dry blood spots (DBS) samples were randomly selected for this study.
Genomic DNA extraction
Single-hole Kangaro punch (No. 376224, India) was used to cut out six circles (3 mm in diameter) from each filter paper dry blood spots (DBS) sample and the punched DBS were placed in 1.5 ml Eppendorf tubes. In order to ensure that there is no cross contamination between samples, the punch was sterilized using sodium hypochlorite (NaClO) and 100% ethanol59.
DNA was extracted using the QIAamp DNA Mini Kit (51304, QIAGEN, Hilden, Germany) following the manufacturer’s protocol. The quality and concentration of each extracted genomic DNA sample was assessed using a Nanodrop 2000C (Thermo Fisher Scientific, Waltham, MA, USA) and samples were stored at −20 °C.
Microsatellite genotyping of P. falciparum
Plasmodium falciparum DNA extracted from each DBS sample was genotyped using ten polymorphic microsatellite markers60. Primer sets targeting specific sequences flanking (TAA)n repeat regions in the P. falciparum genome were used to amplify each locus using a slightly modified published hemi-nested PCR protocol in a SimpliAmp Thermal Cycler (Applied Biosystems, Loughborough, UK)60. The primers were dye labelled using 6-FAM for locus TA1, ARA2, PfPK2, TA87, and TA109; HEX for TA81, TA42, Polyα, TA60 and Pfg377. The hemi-one amplifications were performed in a total PCR reaction volume of 20 µL containing 1× FIREPol Master Mix (Solis BioDyne, Estonia), 0.3 µM of each primer (Macrogen, South Korea) and 3 µL (10 ng/µL) of DNA template. The cycling conditions for nest-one PCR were; initial denaturation for 2 min at 94 °C; 30 cycles of 30 sec at 94 °C, 30 sec at 42 °C, 30 sec at 40 °C and 30 sec at 65 °C; final elongation for 5 min at 65 °C. The total reaction volume of hemi-two PCR was also 20 µL containing 1× FIREPol Master Mix (Solis BioDyne, Estonia), 0.4 µM of each primer (Macrogen, South Korea) (see Supplementary Table S1) and 5 µL of hemi-one PCR amplicons. The PCR conditions were as follows; initial denaturation for 2 min at 94 °C; 30 cycles of 30 sec at 94 °C, 30 sec at 45 °C and 30 sec at 65 °C; final elongation for 5 min at 65 °C.
The PCR amplification for the different loci were confirmed by fragment separation in 2% agarose gels and visualized using ethidium bromide (E1385, Merck, Germany). The amplified products were pooled together as described elsewhere54, wrapped in an aluminium foil then shipped for fragment analysis at the DNA Sequencing Facility, University of Illinois at Urbana-Champaign, Urbana, Illinois, USA. The pooled PCR products were separated on an ABI 3730XL (Applied Biosystems) genetic Analyser using GeneScan 400HD ROX Size Standard (Applied Biosystems, Foster City, CA). Allele sizes scoring and peak height quantification was carried out using GeneMarker V3.0.1 software (SoftGenetics, LLC).
Data analysis
The fact that Plasmodium falciparum parasite stages found in human blood are haploid, the presence of more than one allele at a particular locus per isolate was interpreted as polyclonal or multiple clone infections. That is, samples with more than one allele at any given locus are termed as co-infection with genetically distinct parasite clones. Isolates with minor allele peak heights that are ≥25% of the predominant allele per locus were scored as multiple alleles. DNA samples with only one allele detected at all the genotyped gene loci were scored as monoclonal infections. Multiplicity of P. falciparum infection (MOI) is defined as the number of genetically distinct clones co-infecting a host at any given time. In this study, MOI and average MOI were estimated per locus. The average MOI of all the samples included in this study was estimated as the ratio of the total number of distinct fragments (genetically distinct parasite clones) scored for a given gene loci in relation to the number of samples successfully amplified by that marker locus35.
Descriptive statistics were computed using IBM SPSS Statistics for Windows, version 20 (IBM Corp., Armonk, N.Y., USA). Allelic frequency, expected heterozygosity, number of alleles and number of effective alleles of the study population were determined using a population genetic software, GenAIEx 6.561. The predominant allele in case of multiple alleles or the only allele in the case of single allele at each locus was used to estimate the expected heterozygosity (He) per locus as a measure of genetic diversity using a formula, He = [n/(n − 1)][1 −Σpi2], where n and pi represents the number of isolates analysed and frequency of the ith allele in a given population. Expected heterozygosity (He) values range between 0 and 1 for no genetic diversity and high genetic diversity, respectively60.
Results
Characteristics of study participants
A total of 95 P. falciparum positive samples detected by RDT and microscopy was included in this study. The ages of the study participants ranged from 5 to 15 years. In Table 1, the total number of participants within the age categories 5–9 and 10–15 years were 59 (62.1%) and 36 (37.9%), respectively. The female participants comprised of 42 (44.2%) while 53 (55.8%) were of the male gender. Based on the RDT and microscopy results (data not shown), 77 (81.1%) of the participants were infected with only P. falciparum while 18 (18.9%) of the subjects were infected with P. falciparum plus another Plasmodium species (P. ovale and P. malariae) and 50.5% carried the sexual stage of the parasite (gametocyte).
Multiple clone infections and multiplicity of P. falciparum infection (MOI)
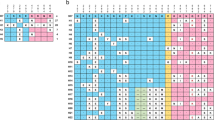
The amplification of the 10 polymorphic microsatellite marker loci was successful in 99% of the isolates. Overall, the Pfg377 locus was the marker with the highest number of missing data in which 3 (3%) of the isolates had a missing data. The full genotype profile and allelic frequencies of the 95 samples were presented as Supplementary Tables S2 and S3, respectively. For this study, samples were grouped into two categories depending on the number of alleles detected per marker loci. Isolates with only one allele per marker locus were classified as monoclonal while those with two or more alleles at either one or more loci were termed polyclonal infections. The percentage of polyclonal infections in the study samples was computed based on the proportion of isolates with multiple genotypes per marker. In Fig. 1 and Table 2, samples analysed in this study contained largely polyclonal parasites [79.69% (Range: 54.84–95.74%)] with high multiplicity of P. falciparum infections [3.39 (Range: 2.24–4.72)] detected at each of the genotyped genetic locus. More than six alleles were found at almost all the genotyped genetic loci (except in the Pfg377 loci) in the study samples indicating an overall complex infections.

Frequency of samples with different number of alleles detected in the study at each of the 10 genotyped P. falciparum microsatellite loci. The various colours in the graph representing the different number of clones: red (1), orange (2), gray (3), gold (4), black (5), green (6), and dark blue (>6).
Overall, based on genotyping of the 10 polymorphic microsatellite marker loci, there were variations in the number of isolates with polyclonal infections detected by each marker locus with TA1 (54.84%) and TA42 (95.74%) markers detecting the lowest and highest number of polyclonal isolates (Fig. 1 and Table 2).
Genetic diversity of P. falciparum infections in the study population
The 10 microsatellite marker loci used in this study were all observed to be highly polymorphic in the study population with total number of distinct observed alleles (Na) per locus ranging from 8 (for locus Pfg377) to 23 (for locus Polyα) and the number of effective alleles (Ne) varied between 2.3 and 15.3. The least and most polymorphic markers were Pfg377 and Polyα respectively. Overall, Na values were much higher than the Ne values indicating that majority of the alleles were present at low frequency (Table 3 and Supplementary Fig. S1 and Table S3).
The expected heterozygosity (He) defined as the probability that two randomly selected clones from a population will carry distinct alleles at each marker loci was used to estimate the allelic diversity per loci based on allelic frequencies computed (See Supplementary files: Table S3) at each of the 10 microsatellite loci. In Table 3, the expected heterozygosity (He) values per locus in the study population varied from 0.57 (TA109) to 0.95 (Polyα) with an average score of 0.81, thereby depicting a high genetic diversity among the isolates.
Discussion
The current study revealed a high level of multiplicity of infections and genetic diversity among the study population. This is illustrated by high level of polyclonal infections and high proportions of locus scores with multiple genotypes. The 79.69% prevalence of polyclonal infections found in the study population is consistent with results from other studies carried out in malaria endemic and high transmission intensity regions where multi-clonal infection rates varied from 50% to 100%, respectively62,63,64,65,66,67. The overall mean MOI of 3.39 in the study population found in our study corroborates with other studies in high malaria transmission areas in Africa like Kenya (2.83)68, Gambia (2.1), Senegal (2.2), Guinea Bissau (2.6), Guinea (4.0)54, Tanzania (3.5)62, Uganda (3.0–3.7)65 and Madagascar (3.72–3.73)66 but higher than results from low malaria transmission regions like Djibouti (1.0–1.4), Dakar (1.0–1.5), Niamey (1.0–1.8)67 and Sudan69. The high MOI found in this study maybe due to the boosted parasite specific immunity in people residing in high malaria transmission regions and the study population as children were reported to carry higher MOI infections compared to adults38,70.
The high number of alleles and high expected heterozygosity of P. falciparum recorded at each of the 10 polymorphic microsatellite marker loci in our study are indications of high genetic diversity among P. falciparum parasites circulating in the study area. This finding could be due to the high malaria transmission and endemicity reported in the area71. Another contributing factor for the high genetic diversity maybe due to the efficient land and water transport networks in the study area facilitating human movements from other malaria endemic regions leading to the introduction of foreign strains to the local parasites gene pool64,68. These results corroborates the findings of previous studies conducted in other parts of western Kenya63,65,66 but different from those of low malaria transmission intensity areas like lowland coastal area of Kenya (Malindi)64, Philippines72 and other regions of South America73,74,75. The high mean He value (0.81) observed in our study was similar to those obtained in high malaria endemic and transmission settings of Africa: Kenya (0.81)64, Congo DRC (0.71)75, Ghana (0.67–0.69)35, Nigeria (0.65–0.79)76, The Gambia (0.75), Senegal (0.72), Guinea Bissau (0.78), Guinea Conakry (0.78)54, Asia: Vietnam (0.52–0.91) and Oceania: Papua New Guinea (0.79)73. However, He values from studies conducted in low malaria transmission intensity regions such as Djibouti (0.41)67, Brazil (0.39–0.52)77, Honduras (0.35) and Nicaragua (0.38)78 were lower than that of our study.
Conclusions
The analysis of genetic diversity and multiplicity of P. falciparum infections among malaria asymptomatic school children (age 5–15 yrs.) in Mbita, western Kenya using 10 polymorphic microsatellite marker loci reveal a high level of multi-clonal infections and high genetic diversity of P. falciparum parasites circulating in the study area. These findings correlated with the expectations of high malaria transmission intensity and endemic region despite the scaling up of malaria control interventions by the government. Therefore, in order to attain ultimate malaria elimination in the region, there is a need for the implementation of more robust and holistic interventions against the parasite particularly the asymptomatic carriers. Furthermore, the findings from our study have pinpointed the need for periodic Plasmodium parasite molecular genetic surveillance studies in the area. This will help maintain up-to-date information about parasite transmission dynamics for effective impact assessment of the currently implemented malaria control interventions. Additionally, it will further guide in the introduction of new malaria control programs whenever needed.
References
WHO. World malaria report 2019. World Health Organization, https://www.who.int/malaria/publications/world-malaria-report-2019/en/ (2019).
WHO. World malaria report 2018. World Health Organization, https://www.who.int/malaria/publications/world-malaria-report-2018/en/ (2018).
Kenya National Bureau of Statistics and ICF Macro. Kenya Demographic and Health Survey 2008–2009. Calverton: Kenya National Bureau of Statistics and ICF Macro. (2010).
Kenya Bureau of Statistics. Kenya Malaria Indicator Survey, 2007. Kenya Malaria Indicator Survey (2007).
Division of Malaria control Ministry of Public Health and Sanitation. (2010) Kenya Malaria Indicator Survey. (2010).
Jenkins, R. et al. Prevalence of malaria parasites in adults and its determinants in malaria endemic area of Kisumu County, Kenya. Malar. J. 14, 1–6 (2015).
Kenya: Ministry of Health, D. of M. C. Government of Kenya. National Malaria Strategy 2009–2017. (2009).
National Malaria Control Programme & Ministry of Health. The Kenya Malaria Communication Strategy 2016-2021. http://www.nmcp.or.ke (2016).
Brooker, S. et al. Situation analysis of malaria in school-aged children in Kenya - What can be done? Parasitol. Today 16, 183–186 (2000).
Carneiro, I. et al. Age-patterns of malaria vary with severity, transmission intensity and seasonality in sub-Saharan Africa: A systematic review and pooled analysis. PLoS One 5 (2010).
Walldorf, J. A. et al. School-age children are a reservoir of malaria infection in Malawi. PLoS One 10, 1–13 (2015).
Nankabirwa, J. et al. Malaria in school-age children in Africa: An increasingly important challenge. Trop. Med. Int. Heal. 19, 1294–1309 (2014).
Vitor-Silva, S., Reyes-Lecca, R. C., Pinheiro, T. R. A. & Lacerda, M. V. G. Malaria is associated with poor school performance in an endemic area of the Brazilian Amazon. Malar. J. 8, 230 (2009).
Mathanga, D. P. et al. The high burden of malaria in primary school children in Southern Malawi. Am. J. Trop. Med. Hyg. 93, 779–789 (2015).
Baliraine, F. N. et al. High Prevalence of Asymptomatic Plasmodium falciparum Infections in a Highland Area of Western Kenya: A Cohort Study. J. Infect. Dis. 200, 66–74 (2009).
Males, S., Gaye, O. & Garcia, A. Long-Term Asymptomatic Carriage of Plasmodium falciparum Protects from Malaria Attacks: a Prospective Study among Senegalese Children. Clin. Infect. Dis. 46, 516–522 (2008).
Chourasia, M. K. et al. Burden of asymptomatic malaria among a tribal population in a forested village of central India: a hidden challenge for malaria control in India. Public Health 147, 92–97 (2017).
Coalson, J. E. et al. High prevalence of Plasmodium falciparum gametocyte infections in school-age children using molecular detection: patterns and predictors of risk from a cross-sectional study in southern Malawi. Malar. J. 15, 1–17 (2016).
Alves, F. P. et al. Asymptomatic Carriers of Plasmodium spp. as Infection Source for Malaria Vector Mosquitoes in the Brazilian Amazon. J. Med. Entomol. 42, 777–779 (2006).
Haakenstad, A. et al. Tracking spending on malaria by source in 106 countries, 2000–16: an economic modelling study. Lancet Infect. Dis. 19, 703–716 (2019).
Sabot, O. et al. Costs and financial feasibility of malaria elimination. Lancet 376, 1604–1615 (2010).
Shretta, R., Avanceña, A. L. V. & Hatefi, A. The economics of malaria control and elimination: a systematic review. Malar. J. 15, 1–14 (2016).
Zelman, B., Melgar, M., Larson, E., Phillips, A. & Shretta, R. Global fund financing to the 34 malaria - eliminating countries under the new funding model 2014–2017: an analysis of national allocations and regional grants. Malar. J. 15, 1–15 (2016).
Amodu, O. K., Olumide, A. O., Uchendu, O. C., Amodu, F. A. & Omotade, O. O. Differences in the Malariometric Indices of Asymptomatic Carriers in Three Communities in Ibadan, Nigeria. Adv. Prev. Med. 2014, 1–4 (2014).
Gbalégba, C. G. N. et al. Distribution of Plasmodium spp. infection in asymptomatic carriers in perennial and low seasonal malaria transmission settings in West Africa. Infect. Dis. Poverty 7, 1–13 (2018).
Sumari, D. et al. Malaria prevalence in asymptomatic and symptomatic children in Kiwangwa, Bagamoyo district, Tanzania. Malar. J. 16, 1–7 (2017).
Pegha Moukandja, I. et al. Marked rise in the prevalence of asymptomatic Plasmodium falciparum infection in Rural Gabon. PLoS One 11, 1–14 (2016).
Orish, V. et al. Asymptomatic Plasmodium falciparum infection and poor school performance in primary school children in the Volta Region of Ghana. Ethiop. J. Health Sci. 28, 749–758 (2018).
Lee, S. A. et al. Complexity of Plasmodium falciparum Infections and Antimalarial Drug Efficacy at 7 Sites in Uganda. J. Infect. Dis. 193, 1160–1163 (2006).
Blasco, B., Leroy, D. & Fidock, D. A. Antimalarial drug resistance: linking Plasmodium falciparum parasite biology to the clinic. Nat. Med. 23, 917–928 (2017).
Talisuna, A. O., Okello, P. E., Erhart, A., Coosemans, M. & Alessandro, U. D. Intensity of Malaria Transmission and the Spread of Plasmodium falciparum – Resistant Malaria: A Review of Epidemiologic Field Evidence. 77, 170–180 (2007).
Sondo, P. et al. Genetically diverse Plasmodium falciparum infections, within-host competition and symptomatic malaria in humans. Sci. Rep. 9, 1–9 (2019).
Lo, E. et al. Transmission dynamics of co-endemic Plasmodium vivax and P. falciparum in Ethiopia and prevalence of antimalarial resistant genotypes. PLoS Negl. Trop. Dis. 11, 1–25 (2017).
Beck, S. et al. Multiplicity of Plasmodium falciparum infection in pregnancy. Am. J. Trop. Med. Hyg. 65, 631–636 (2001).
Abukari, Z. et al. The Diversity, Multiplicity of Infection and Population Structure of P. falciparum Parasites Circulating in Asymptomatic Carriers Living in High and Low Malaria Transmission Settings of Ghana. Genes (Basel). 10, 434 (2019).
Zhong, D., Koepfli, C., Cui, L. & Yan, G. Molecular approaches to determine the multiplicity of Plasmodium infections. Malar. J. 17, 1–9 (2018).
Bereczky, S. et al. Multiclonal asymptomatic Plasmodium falciparum infections predict a reduced risk of malaria disease in a Tanzanian population. Microbes Infect. 9, 103–110 (2007).
Mayor, A. et al. Plasmodium falciparum multiple infections in Mozambique, its relation to other malariological indices and to prospective risk of malaria morbidity. Trop. Med. Int. Heal. 8, 3–11 (2003).
Nassir, E. et al. Impact of genetic complexity on longevity and gametocytogenesis of Plasmodium falciparum during the dry and transmission-free season of eastern Sudan. Int. J. Parasitol. 35, 49–55 (2005).
Bose, J., Kloesener, M. H. & Schulte, R. D. Multiple-genotype infections and their complex effect on virulence. Zoology 119, 339–349 (2016).
Josling, G. A. & Llinás, M. Sexual development in Plasmodium parasites: Knowing when it’s time to commit. Nat. Rev. Microbiol. 13, 573–587 (2015).
Pollitt, L. C. et al. Competition and the evolution of reproductive restraint in malaria parasites. Am. Nat. 177, 358–367 (2011).
Meibalan, E. & Marti, M. The biology of malaria transmission. Cold Spring Harb. Perspect. Med. 7, 1–15 (2017).
Chen, J. T. et al. Genetic diversity and allele frequencies of Plasmodium falciparum msp1 and msp2 in parasite isolates from Bioko Island, Equatorial Guinea. Malar. J. 17, 1–9 (2018).
Mara, S. E. et al. Genetic diversity of Plasmodium falciparum among school-aged children from the Man region, western Côte d’Ivoire. Malar. J. 12, 1–10 (2013).
Arnot, D. Unstable malaria in Sudan: the influence of the dry season: Clone multiplicity of Plasmodium falciparum infections in individuals exposed to variable levels of disease transmission. Trans. R. Soc. Trop. Med. Hyg. 92, 580–585 (1998).
Pringle, J. C. et al. RTS,S/AS01 malaria vaccine mismatch observed among Plasmodium falciparum isolates from southern and central Africa and globally. Sci. Rep. 8, 1–8 (2018).
Apinjoh, T. O., Ouattara, A., Titanji, V. P. K., Djimde, A. & Amambua-Ngwa, A. Genetic diversity and drug resistance surveillance of Plasmodium falciparum for malaria elimination: is there an ideal tool for resource-limited sub-Saharan Africa? Malar. J. 18, 217 (2019).
Murray, L. et al. Microsatellite genotyping and genome - wide single nucleotide polymorphism - based indices of Plasmodium falciparum diversity within clinical infections. Malar. J. 1–6, https://doi.org/10.1186/s12936-016-1324-4 (2016).
Razak, M. R. M. A. et al. Genetic diversity of Plasmodium falciparum populations in malaria declining areas of Sabah, East Malaysia. PLoS One 11, 1–22 (2016).
Viriyakosol, S. et al. Genotyping of Plasmodium falciparum isolates by the polymerase chain reaction and potential uses in epidemiological studies. Bull. World Health Organ. 73, 85–95 (1995).
Nkhoma, S. C. et al. Resolving within-host malaria parasite diversity using single-cell sequencing. bioRxiv 391268, https://doi.org/10.1101/391268 (2018).
Ferreira, M. U., et al Microsatellite Characterization of Plasmodium falciparum from Cerebral and Uncomplicated Malaria Patients in Southern Vietnam. 40, 1854–1857 (2002).
Mobegi, V. A. et al. Population genetic structure of Plasmodum falciparum across a region of diverse endemicity in West Africa. Mala. J. 11, 1–9 (2012).
Worku, L., Damte, D., Endris, M., Tesfa, H. & Aemero, M. Asymptomatic malaria and associated determinant factors among school children in Sanja Town, Northwest Ethiopia. J. Parasitol. Res. 2014, 792536 (2014).
Wanyua, S. et al. Profile: The Mbita Health and Demographic Surveillance System. Int. J. Epidemiol. 42, 1678–1685 (2013).
Minakawa, N., Dida, G. O., Sonye, G. O., Futami, K. & Kaneko, S. Unforeseen misuses of bed nets in fishing villages along Lake Victoria. Malar. J. 7, 5–10 (2008).
Idris, Z. M. et al. High and Heterogeneous Prevalence of Asymptomatic and Sub-microscopic Malaria Infections on Islands in Lake Victoria, Kenya. Sci. Rep. 6, 1–13 (2016).
Strøm, G. E. A., Tellevik, M. G., Fataki, M., Langeland, N. & Blomberg, B. No asymptomatic malaria parasitaemia found among 108 young children at one health facility in Dar es Salaam, Tanzania. Malar. J. 12, 1–5 (2013).
Anderson, T. J., Su, X.-Z., Bockarie, M., Lagog, M. & Day, N. P. Twelve microsatellite markers for characterization of Plasmodium falciparum from finger-prick blood samples. Parasitology 119, 113–125 (1999).
Peakall, R. & Smouse, P. E. GenALEx 6.5: Genetic analysis in Excel. Population genetic software for teaching and research-an update. Bioinformatics 28, 2537–2539 (2012).
Babiker, H. A., Ranford-Cartwright, Lisa, C. & Walliker, D. Genetic structure and dynamics of Plasmodium falciparum infections in the Kilombero region of Tanzania. Trans. R. Soc. Trop. Med. Hyg. 93, 11–14 (1999).
Zhong, D. et al. Plasmodium falciparum genetic diversity in Western Kenya highlands. Am. J. Trop. Med. Hyg. 77, 1043–1050 (2007).
Ingasia, L. A., Cheruiyot, J., Okoth, S. A., Andagalu, B. & Kamau, E. Genetic variability and population structure of Plasmodium falciparum parasite populations from different malaria ecological regions of Kenya. Infect. Genet. Evol. 39, 372–380 (2016).
Kiwuwa, M. S. et al. Genetic diversity of Plasmodium falciparum infections in mild and severe malaria of children from Kampala, Uganda. Parasitol. Res. 112, 1691–1700 (2013).
Durand, R. et al. Analysis of circulating populations of Plasmodium falciparum in mild and severe malaria in two different epidemiological patterns in Madagascar. Trop. Med. Int. Heal. 13, 1392–1399 (2008).
Bogreau, H. et al. Genetic diversity and structure of African Plasmodium falciparum populations in urban and rural areas. Am. J. Trop. Med. Hyg. 74, 953–959 (2006).
Mulenge, F. M. et al. Genetic diversity and population structure of Plasmodium falciparum in lake victoria islands, a region of intense transmission. Am. J. Trop. Med. Hyg. 95, 1077–1085 (2016).
Mustafa, S. O. et al. Genetic diversity and multiplicity of Plasmodium falciparum merozoite surface protein 2 in field isolates from Sudan. F1000Research 6, 1790 (2017).
Smith, T. et al. 4. Age dependence of the multiplicity of Plasmodium falciparum infections and of other malariological indices in an area of high endemicity. Trans. R. Soc. Trop. Med. Hyg. 93, 15–20 (1999).
Bloland, P. B. et al. Longitudinal cohort study of the epidemiology of malaria infections in an area of intense malaria transmission II. Descriptive epidemiology of malaria infection and disease among children. Am. J. Trop. Med. Hyg. 60, 641–648 (1999).
Iwagami, M. et al. Genetic diversity and population structure of Plasmodium falciparum in the Philippines. Malar. J. 8, 1–8 (2009).
Schultz, L. et al. Multilocus haplotypes reveal variable levels of diversity and population structure of Plasmodium falciparum in Papua New Guinea, a region of intense perennial transmission. Malar. J. 9 (2010).
Anderson, T. J. C. et al. Microsatellite markers reveal a spectrum of population structures in the malaria parasite Plasmodium falciparum. Mol. Biol. Evol. 17, 1467–1482 (2000).
Durand, P. et al. Significant linkage disequilibrium and high genetic diversity in a population of Plasmodium falciparum from an area (Republic of the Congo) highly endemic for malaria. Am. J. Trop. Med. Hyg. 68, 345–349 (2003).
Oyebola, M. K. et al. Microsatellite markers reveal low levels of population sub-structuring of Plasmodium falciparum in southwestern Nigeria. Malar. J. 13, 1–8 (2014).
Machado, R. L. D. et al. Genetic Structure of Plasmodium falciparum Populations in the Brazilian Amazon Region. J. Infect. Dis. 190, 1547–1555 (2004).
Larrañaga, N. et al. Genetic structure of Plasmodium falciparum populations across the Honduras-Nicaragua border. Malar. J. 12, 1–10 (2013).
Acknowledgements
We are indebted to all volunteers who partook in this study as well as their parents/guardians for granting consent. The authors are very much grateful to the entire research team of Dr. Jeremy K. Herren and the management of International Centre of Insect Physiology and Ecology (ICIPE) for their help permitting us to use their samples and giving us access to use their research facilities to conduct the study. This study was funded by Pan African University, Institute of Basic Sciences, Technology and Innovation (PAUSTI) under the postgraduate training program awarded to AOT.
Author information
Authors and Affiliations
Contributions
V.A.M., A.O.T. and J.K.H. designed the study; A.O.T., F.W., J.K.H. and V.A.M. were involved in the conduct of the study; J.K.H. provided the study samples; A.O.T., and V.A.M.; were involved in the data analysis; A.O.T., F.W., J.K.H. and V.A.M. wrote the manuscript and all the authors interpreted the data and contributed to writing of the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Touray, A.O., Mobegi, V.A., Wamunyokoli, F. et al. Diversity and Multiplicity of P. falciparum infections among asymptomatic school children in Mbita, Western Kenya. Sci Rep 10, 5924 (2020). https://doi.org/10.1038/s41598-020-62819-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-62819-w
This article is cited by
-
Plasmodium falciparum genetic diversity and multiplicity of infection based on msp-1, msp-2, glurp and microsatellite genetic markers in sub-Saharan Africa: a systematic review and meta-analysis
Malaria Journal (2024)
-
Genotyping Plasmodium falciparum gametocytes using amplicon deep sequencing
Malaria Journal (2024)
-
Recent increase in low complexity polygenomic infections and sialic acid-independent invasion pathways in Plasmodium falciparum from Western Gambia
Parasites & Vectors (2023)
-
Plasmodium falciparum population structure inferred by msp1 amplicon sequencing of parasites collected from febrile patients in Kenya
Malaria Journal (2023)
-
Low genetic diversity of Plasmodium falciparum merozoite surface protein 1 and 2 and multiplicity of infections in western Ethiopia following effective malaria interventions
Malaria Journal (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
