
Abstract
We aimed to evaluate the influence of shift work rotation, circadian misalignment and being overweight/obese on psychomotor performance throughout a complete shift rotation schedule. The study was conducted with 30 males working rotating shifts from a mining company under real life conditions. Individuals were evaluated over seven days in a shift schedule carried out as follow: two shifts in the morning (D1 and D2), two shifts in the afternoon (D3 and D4), 24 hour free day (D5) and two shifts at night (D6 and D7). Work performance was evaluated by psychomotor vigilance task tests (PVT), and actigraphy was used to characterise the rest-activity rhythm based on intradaily variability (IV) and interdaily stability (IS) of nonparametric functions. We found a significant effect of the shift, body mass index (BMI), IS and IV on lapses in attention. More lapses occurred on D7 than D1, D2, D3 and D4 of the schedule shift. The obese group presented a higher number of lapses in attention than eutrophic. The interaction between day and IS showed that less synchronised individuals presented a higher number of lapses in attention on D7 than D1 and, for the interaction between day and IV, more fragmented individuals presented a higher number of lapses in attention on D7 than D6. We conclude that higher BMI, lower synchronisation and higher fragmentation of the rest-activity pattern influenced lapses in attention throughout the shift rotation.
Similar content being viewed by others

Introduction
Shift work is characterised by 24 hours of operations and presents a wide variety of working time arrangements, including all working hours that are outside the normal daytime ones1. In industrialised society it is estimated that this type of work represents more than 20% of employees2, in the USA it is 28.7%3 and in Brazil the percentage for shift work has not yet been calculated, but specific data for night work shows a percentage of 15%4. Among the different types of shift work arrangements, the rotating shift – characterised by constant alternation of working hours and free days within a pre-established period5 – is quite common among companies6. The direction of shift schedule rotation (clockwise or counterclockwise) and rotation speed (fast or slow) also presents variation among shift work schedules7.
The physiology and behaviour of human beings are coordinated by an intrinsic molecular clock into rhythms that are synchronised with the 24 hour solar day. The suprachiasmatic nucleus (SCN), the primary synchroniser, works with various peripheral synchronisers8, and both are influenced by external time cues – such as light-dark, meals and social interaction9. Shift work, mainly night shifts, is impacted by most of these external synchronisers – such as the daytime pattern of exposure to light and the exposure time to synchronisers10. Thereby, adjustments in the phase of endogenous circadian rhythms are compromised in shift workers9, which leads to desynchronisation between the circadian clock and the sleep cycle, known as circadian misalignment11. Currently it is possible to quantify circadian misalignment by assessing variables such as interdaily stability (IS, i.e. the stability of the rhythm over days) and intradaily variability (IV, i.e. the fragmentation of the rhythm relative to its 24 hour amplitude) by actigraphy12.
Circadian misalignment may negatively affect psychomotor performance, since cognitive functions such as vigilance level and, consequently, the development of lapses in attention are directly linked to circadian and homeostatic influences, which in turn suffer fluctuations throughout the day13. The physiological mechanism involving wakefulness levels is determined by responses generated by the parasympathetic and sympathetic nervous systems through environmental stimuli14. Therefore, the vigilance level of individuals fluctuates over the course of a day14 and may be impacted by misalignment. This can lead to an inappropriate response, indicating a state of decompensation and failure of physiological functions15. It has been documented that approximately 10% to 30% of fatal traffic deaths are due to sleepiness and fatigue, which are directly associated with lapses in attention16. In addition, variables such as the workload and the nutritional status of individuals have been shown to be possible variables that can alter psychomotor performance17,18.
Previous studies showed that circadian misalignment also leads to losses in physiologic functions, which show a 24 hour rhythmicity and are ruled by the light/dark cycle, such as the sleep/awake cycle19 and macronutrients metabolism20,21. In this condition, the release of hormones associated with food consumption, such as leptin and ghrelin, may be altered, which establishes a link between circadian misalignment and obesity22. Cook et al.23 postulated that even in situations where there is no apparent circadian misalignment, obesity is capable of interfering with psychomotor performance23. However, the relationship between psychomotor performance, circadian misalignment and obesity is little explored among shift workers.
Rotating shift workers experience a large variation in working times over a short period. In this sense, it is reasonable to assume that circadian misalignment leads to diminished work performance, and in obese subjects this situation could be worse24. This study aimed to evaluate the influence of a rotating shift, circadian misalignment and being overweight/obese on the performance of rotative shift workers. We hypothesised that excessive body weight, lower synchronisation and higher fragmentation of the rest and activity pattern can lead to an increase in the number of lapses in attention throughout the scheduled shift days in rotative shift workers.
Methods
Participants and ethics
This prospective, observational study was conducted with 30 males that worked for a mining company located in a city in the midwest of Brazil, on a rotative shift work schedule. The shift workers were informed about the objectives and procedures, and after that they were invited to join the study. This study was approved by the Human Research Ethics Committee of the Federal University of Uberlândia (CAAE: 49689115.0.0000.5152), all methods were performed in accordance with the relevant guidelines and regulations and all subjects signed an informed consent form.
Participants were selected if they met the following criteria: works a clockwise rotating shift (morning-afternoon-night); works in an operations control panel or leadership position; is able to wear actigraphy monitors and to perform the psychomotor performance tests (PVT); has not done trans-meridian travel in the three months prior to the start of the study. Participants were excluded if they had a sleep disorder or other comorbities (heart and metabolic diseases, cancer, neurological and degenerative brain diseases), hearing and visual impairments, had loss of consciousness or used medication capable of inducing sleep or wakefulness. This information was obtained from the occupational medicine area of the company where the study was conducted and by the initial questionnaire and sleep diary. From the company’s total workforce, 30 subjects (aged between 25 and 52 years old) met the inclusion and exclusion criteria and agreed to participate in the study.
On the first day of the study, initial evaluations such as questionnaires regarding sociodemographic and health behaviours, as well as anthropometric and biochemical analyses, were conducted. Then, individuals were evaluated over seven days regarding their work performance (PVT) and rhythm rest-activity pattern (actigraphy).
Initial Evaluation
Sociodemographic data and health behaviours
All subjects answered a questionnaire about sociodemographic aspects, such as age, marital status, presence of children, level of education and years of shift work, as well as health behaviours such as frequency of physical activity, alcohol intake, smoking habits, diseases diagnosed and use of medicines.
Blood parameters
The subjects were instructed to fast overnight for 12 hours before blood sample collection. All procedures occurred at the company’s ambulatory clinic. The biochemical analyses measured were: fasting blood glucose, fasting insulin, insulin resistance index (HOMA-IR), total cholesterol, low density lipoprotein (LDL-c), high density lipoprotein (HDL-c) and triglycerides (TG).
The glucose-oxidase method (Siemens, Chicago, IL, USA) was used to determine the glucose serum concentrations. Insulin concentrations were accessed using a commercial enzyme-linked immunosorbent assay kit (ELISA) (Siemens). Homeostasis model for the assessment of insulin resistance (HOMA-IR) was determined using the following formula described by Matthews et al.25, fasting serum insulin (μIU/L) × fasting serum glucose (mmol/L)/22.5. The concentrations of cholesterol, triglycerides and HDL-cholesterol were determined by means of coupled reactions. The products of this reaction are a coloured complex that can be measured by spectrophotometry. Each of the specific analyses was accessed using a commercial kit from Biosystems® (cholesterol - Ref. 21505, triglycerides - Ref. 11828, HDL-cholesterol - Ref. 11648). The value of LDL-cholesterol was determined using the formula described by Friedewald26.
Anthropometric variables
Weight and height measurements were performed according to the standardisation method proposed by Lohman et al.27 Weight was measured with a high precision scale accurate to 0.1 kg (Toledo Scale Corp., Toledo, Ohio). To measure height, a stadiometer coupled to a scale with an accuracy of 0.1 cm (Toledo Scale Corp., Toledo, Ohio) was used. Waist circumference (WC) was measured as the midpoint between the last rib and the iliac crest using an inelastic measuring tape28. According to World Health Organization recommendations, a WC ≥ 102 cm was considered abdominal obesity29. Body mass index (BMI, kg/m²) was calculated as the weight (kg) divided by the height squared (m2). A BMI <25 kg/m² was considered eutrophic, ≥25 to <30 kg/m² overweight and ≥30 kg/m² obese29.
Evaluations conducted over shift schedule
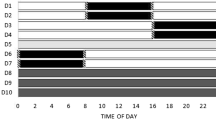
Individuals were followed for seven consecutive days carried out as follows: two days (D1 and D2) working during the morning (08:00–16:00); two days (D3 and D4) working during the evening (16:00–00:00); two days (D6 and D7) working during the night (00:00–08:00). On the 24 hours of rest (D5) between the last day of evening shift and the first one at night, as well as on free days (D8, D9 and D10), the psychomotor vigilance test (PVT) was not performed (Fig. 1).

Shift schedule days. D = shift days; working times of each shift = morning (D1 and D2) – 08:00 to 16:00; afternoon (D3 and D4) – 16:00 to 00:00; 24 h free day (D5) – 00:00 to 00:00; and night (D6 and D7) – 00:00 to 08:00.
Actigraphy
The actigraphy data were collected using the actigraph - Act trust (Condor Instruments®). This tool was configured for collecting information every 24 hours over the period of 15 consecutive days. The information was downloaded through the software ActStudio (Condor Instruments® - version 1.0.0.0050.2015). The volunteers wore the actigraph on their non-dominant wrist. Use of the actigraph was recommended during two complete shift schedules and volunteers filled out a sleep diary with information on their activity during this period30. For this paper we analysed only data from the period between D1–D7 (on the first shift rotation). The correct use of actigraphy were certificated by cellphone messages. The actigraph is a tool validated to identify the patterns of circadian rhythm during shift work31. Through the analysis of circadian rhythm variables by the cosinor method it is possible to obtain information about parametrical (acrophase, mesor, period and amplitude) and nonparametric variables for quantifying the stability and fragmentation of the rest-activity rhythm32.
In this research, rhythm fragmentation was measured by intradaily variability (IV), while synchronisation to the 24 hours light-dark cycle was measured by interdaily stability (IS)33. The IV provides information on rest activity rhythm fragmentation. The IV calculation is based on the first derivate of the hourly clustered actimetry data (Eq. (1)). The first derivate is the result of subtracting the previous element (Xi_1) from the posterior element (Xi) of the raw data. From the first derivate, the root mean square is calculated and the result normalized by the raw data population variance. Large hourly differences such as daytime sleep or nighttime awakenings increase the value of IV. High IV values indicate a fragmented rhythm, such as the presence of daytime sleep and/or nocturnal awakenings (Witting et al., 1990).
Interdaily stability (IS), which yields information about the rest activity rhythm synchronization with the light dark cycle, is calculated from the mean 24-h profile (24 points represent the hours of the day). In Eq. 2, N corresponds to the total number of data items, p is the number of data items per day (24 in this case), Xm is the average of all data, Xh corresponds to each hour of the mean profile, while Xi represents each given hour of raw data. IS is calculated as the variance of the average daily profile divided by the total variance.
We used the median values of IS (0.23) and IV (0.66) to create two groups: for IS, less synchronised (≤0.23) or more synchronised (>0.23); and for IV, less fragmented (≤0.66) or more fragmented (>0.66). Fragmentation (IV) may be derived from daytime sleepiness and/or nocturnal arousals. Higher IV values are related to worse sleep efficiency. The variable IS indicated it was synchronised with the 24 hour zeitgeber. High values show that the subject was synchronised. This reflects good functioning of the CTS components related to photic and nonphotic synchronisation (social effects and schedule shifts33).
Psychomotor vigilance performance
Psychomotor vigilance performance was measured using a portable psychomotor vigilance task (PVT) model 192 (Ambulatory Monitoring, Inc., NY). The PVT tests had durations of five minutes and occurred just before and after the work period, over six days of shift work (corresponding to a complete work schedule) at the workplace. The participant performed the test alone in a quiet room (before the PVT test all partipants were trained to use the machine). The PVT-5 min was used to measure sustained attention and psychomotor vigilance of participants. The variable analysed for this study was mean number of lapses of attention. Lapses of attention are disruptions in performance that typically last reaction time (RT) > 500 ms34. The protocol adopted only used visual response tests, during which bright red visual stimuli (from a light-emitting diode [LED] digital counter) were flashed at intervals of 2 to 10 seconds on the screen of the device. The participants were instructed to press a response button, located on the right side of the device, as soon as the visual stimuli appeared35. The PVT test scores (pre and post work) were summed up and we got the number of lapses of attention (number of lapses of attention = number of lapses of attention pre work + number of lapses of attention post work). The values obtained were analysed using the software Microsoft Excel®.
Statistical analysis
The Shapiro-Wilk test was performed to test the normality of the data. Data are presented as mean and standard error or median and interquartile range. The Spearman correlation test was used to analyse the correlation between lapses in attention and BMI and between IS and IV. The linear regression test was used for continuous variables such as IS, IV and BMI.
Generalised estimating equations (GEE) were used to analyse the single and interacting effects of independent variables (day of the shift schedule, BMI, IS and IV) on the dependent variable (number of lapses of attention). In the present study, an exchangeable correlation structure was used in two models for analysis of the interactions. Model 1 - dependent variable: lapses of attention; independent variables: day of shift work, BMI and IS. Model 2 - dependent variable: lapses of attention; independent variables: day of shift work, BMI and IV. The isolated effects of the independent variables and the interactions between them were tested in both models. Both models were adjusted for age, period of shift work and presence of children at home. Gamma distribution and Sidak sequential test were performed for pairwise comparisons.
Data was assessed for outliers by a visual assessment via scatter plot and SDs from the mean. Three participants with extreme values of lapses were considered as outliers (Outlier 1, Σ number of lapses of attention = 109.0; Outlier 2, Σ number of lapses of attention = 85.1; Outlier 3, Σ number of lapses of attention = 38).
We performed a paired t-test to compare the values between pre- and post-work PVT scores. As we did not find significant differences (p = 0.56), the two values were summed, and total number of lapses of attention of each shift day was considered for the comparisons throughout the complete shift schedule.
In the analysis involving the variables IS and IV, the n sample was 25. The reason for missing data regarding IS and IV variables (n = 5) is because some volunteers did not use the actigraph during the established period and in the correct way as described in the experimental protocol.
Statistical analyses were performed using SPSS version 23.0 (SPSS Inc., Chicago, IL). For statistical significance, α error was set at 5%.
Results
Population
Data regarding sociodemographics, clinic, occupational, anthropometric, blood parameters, sleep duration, circadian and psychomotor characteristics are presented in Table 1. Among the thirty individuals evaluated, the majority were married (90%), had children at home (63.3%) and had worked in shifts for 10 years or more (66.7%). Ninety percent of participants did not smoke, while fifty percent drank alcoholic beverages at least once a week and most of the subjects did physical activities at least once a week (63.3%). In regards to anthropometric parameters, the majority of subjects had BMI ≥ 25 kg/m2 (76.7%), and 30.0% had abdominal obesity (WC ≥ 102 cm). The individuals had a shorter sleep duration on D5 and during the night shifts (D6 and D7), when compared with morning shifts (D1 and D2), afternoon shifts (D3 and D4) and free days (D8, D9 and D10) (Table 1).
Correlation between total number of lapses and BMI
We found a significant positive correlation between the total number of lapses in attention during the complete shift schedule (seven days) and BMI (Fig. 2; r = 0.331, P < 0.001).

Correlation between total number of lapses in attention in schedule shift and BMI (n = 27; 3 outliers were excluded from this analysis).
The variables IS and IV usually did not correlate mathematically, which also occurred with the IS and IV data for this study. We performed the correlation test and found no significant results (r = 0.75, p = 0.36).
We compared the PVT scores before and after the work shift and found no significant results to difference between pre- and post- work (p = 0.56).
Effect of BMI on the number of lapses of attention
GEE analysis showed the effect of BMI on the number of lapses in attention. The analysis was conducted through two statistical models: 1) including as independent variables: day of shift, BMI and IS; and 2) including as independent variables: day of shift, BMI and IV. In Fig. 3A (Model 1, including the IS variable), the obese individuals presented a greater number of lapses in attention than eutrophic ones (2.51 ± 0.52 and 1.07 ± 0.68, respectively; P < 0.001). In Fig. 3B (Model 2, including IV variable), eutrophic individuals (0.56 ± 0.72) also had a lower number of lapses in attention when compared to overweight and obese individuals (1.65 ± 0.26 and 2.49 ± 0.49, respectively; P < 0.001 for all) (Fig. 3B).

Effect of BMI on number of lapses in attention. (A) Model 1 - Effect of BMI on number of lapses in attention through the analysis of GEE and (B) Model 2 - Effect of BMI on number of lapses through the analysis of GEE. Data correspond to mean ± standard error of the mean (n = 30). The bars with different letters are significantly different; P < 0.001. All analysis were adjusted for age, period of shift work and presence of children in the house (see results for statistics).
The results of Model 1 showed isolated effects of the variables as well as their interactions. In relation to the day of the shift rotation, the highest value of lapses in attention was found on D7 (2.68 ± 0.35; night shift), which was significantly higher than D1, D2, D3 and D4 (0.56 ± 0.77, 1.84 ± 0.34, 1.99 ± 0.29 and 1.69 ± 0.28, respectively; P < 0.05 for all). For the effect of synchronisation of the rest-activity rhythm (IS) on the number of lapses in attention, we found that poorly synchronised subjects presented mean number of lapses of 1.69 ± 0.24 and the most synchronised ones of 1.53 ± 0.20 without significant differences (P = 0.61).
Interaction between shift day and IS and between the shift day and BMI
Table 2 shows the effect of interactions between the shift day and IS and between the shift day and BMI on the number of lapses in attention over the seven days evaluation period (Model 1). In the analysis between day of shift work and IS, less synchronised individuals had a greater number of lapses in attention on D7 than D1 (2.60 ± 0.54 and 0.46 ± 0.10, respectively; P < 0.001). Also, in the more synchronised group, the highest number of lapses in attention occurred on D7 (2.77 ± 0.43), significantly higher than D1, D2 and D3 (0.67 ± 0.09, 1.66 ± 0.31 and 1.60 ± 0.27, respectively; P < 0.001) (Table 2).
Throughout the work schedule, eutrophic individuals had higher values of lapses in attention on D7 (3.00 ± 0.35) than D1, D2 and D3 (0.18 ± 0.05, 0.74 ± 0.21 and 1.24 ± 0.15, respectively; P < 0.001) (Table 2). We did not find differences in the overweight group in the lapses in attention values throughout the work schedule (P > 0.05). Also, the number of lapses in attention of the obese individuals was higher on D1 than the eutrophic ones (0.54 ± 0.00 and 0.18 ± 0.05, respectively; P < 0.001).
Obese individuals with low synchronisation had a mean number of lapses in attention of 3.41 ± 1.20, while obese ones that were more synchronised presented a mean of 1.85 ± 0.42 (P = 0.86). In the less synchronised eutrophic group, the mean was 0.79 ± 0.10 and for the more synchronised group the value was 1.45 ± 0.00 (P = 0.17). Less synchronised overweight individuals presented a mean of 1.79 ± 0.39 and more synchronised a mean of 1.34 ± 0.44 (P = 0.92).
The analysis of Model 2 found a significant effect of the variables day of the shift rotation, BMI and IV on number of lapses in attention (P < 0.001). In relation to the day of the shift schedule, the volunteers had a higher value of lapses in attention on D7 – the last day of the schedule and the night shift (2.19 ± 0.42) – than the first day of the schedule (0.60 ± 0.10, P < 0.001). D1 was also lower than D2 and D3 (1.71 ± 0.29 and 2.08 ± 0.34, respectively; P < 0.05). No significant isolated effect of activity-rest fragmentation (IV) on the number of lapses in attention was found; less fragmented individuals presented mean lapses of 1.33 ± 0.17 and the more fragmented of 1.38 ± 0.19 (P = 0.86).
Interaction between shift day and IV and between the shift day and BMI
The analysis of the interaction between day and BMI showed that the eutrophic group presented higher values of lapses in attention on D3 (1.01 ± 0.16) compared to days D1, D4 and D6 (0.18 ± 0.54, 0.5 ± 0.04 and 0.35 ± 0.05, respectively; P < 0.001) (Table 3). The number of lapses in attention in the overweight group did not present a significant difference between the days analysed. Obese subjects presented higher values of lapses in attention on D3 (5.64 ± 1.41), with a significant difference in comparison with D1 (0.45 ± 0.08; P < 0.001) (Table 3).
The results of Model 2 for the interaction between day and IV showed, for the more fragmented group, that D7 was significantly higher than D6 (4.94 ± 1.33 and 0.83 ± 0.17, respectively, P < 0.001) (Table 3). In less fragmented individuals, no significant differences were found (P > 0.05) (Table 3).
We also found in Model 2 that the group of more fragmented obese individuals presented a mean number of lapses in attention of 3.83 ± 1.29 and among less fragmented individuals the mean was 1.61 ± 0.34 (P = 0.51). For the less fragmented eutrophic group, we found a mean of 1.09 ± 0.25 and in more fragmented individuals the value was 0.25 ± 0.00 (P = 0.11). In less fragmented overweight individuals mean lapses in attention were 1.33 ± 0.30 and for more fragmented overweight it was 2.05 ± 0.77 (P = 0.70).
Discussion
This study evaluated the effect of rotating shift work, circadian misalignment and nutritional status on psychomotor performance throughout a complete shift schedule under real life conditions. We found that the shift, obesity, synchronisation and fragmentation of the rest and activity pattern had a significant effect on lapses of attention throughout the scheduled shift days, which supports the hypothesis of the present study. In addition, we found a moderate correlation between lapses in attention in the total shift schedule and BMI. Overall, eutrophic subjects – both less and more synchronised, as well as less or more fragmented activity rhythm – presented a lower number of lapses in attention on several days of the rotating shift schedule when compared with obese/overweight ones. Taken together, the above results demonstrate that psychomotor performance may be influenced by nutritional, work and circadian aspects of the shift worker, which demonstrates the need for a multifactorial approach in interventions aimed at improving the performance and safety of these individuals.
In our study, the number of lapses of attention did not differ between the beginning and end of each day of the schedule, but rather with the advancement of the rotation, and especially when the work was performed at night. In this regard, the second day of night shift and the last day of the shift schedule (D7) presented the most impairment in terms of psychomotor performance compared to other days (Tables 2 and 3). The negative effects of night work on performance have already been recognised in previous studies36,37,38,39. Magee et al.36 showed a greater deleterious effect on alertness and neurobehavioural performance when individuals worked consecutive night shifts. Folkard and Lombardi37 found that during the second day of night shift the risk of work accidents increased by 6% compared to the first day of the night shift. A study conducted by Keith et al.38 found a decrease in workers’ cognitive performance during the night shift when compared with the morning shift. Reinke et al.39 also observed that the occurrence of lapses in attention increased during night shifts. Our results corroborate previous studies, which reaffirmed the deleterious effect of night shift on performance. Given that the number of lapses in attention can be influenced by “time of day” and be impacted by sleepiness and fatigue, it is important to consider the impact of these results on human errors and, consequently, the high levels of occupational accidents40. Therefore, intervention strategies should be adopted in individuals working at night to prevent deleterious effects on psychomotor performance and ensuring the safety of these workers.
The results from this study showed that the second day of night work (D7) represented the worst day in terms of psychomotor performance for both groups. It is also worth noting that the values of lapses of attention oscillated more along the rotation of shifts in the more synchronized group (>IS) than in the less synchronized group (<IS) (see results-Table 2). Less synchronization - in other words, low values of IS - is a repercussion of a possible misalignment between photic and non-photic synchronisers (eg shift work) with circadian functions (eg sleep-wake cycle)33, and this mechanism may explain the largest fluctuations in the number of lapses in the more synchronized group. This is because individuals with higher IS have their activity-rest rhythm more synchronized to the light-dark cycle, which results in better established sleeping and waking times9. Thus, these individuals may have more difficult adapting to quick time alerting on a rotating shift schedule9,41,42. In addition, it should be noted that we use the median IS values to determine the group division and we haven’t determined if this value is the most appropriate to classify individuals as more or less synchronized. So far, it has not been described what would be an ideal cutoff point for this analysis, and further studies on this subject are needed.
The rhythmicity of some physiological functions may impact cognitive perfomance, such as some hormones functions, which are related to mediating information from the central nervous system, including the SCN, to the peripheral tissues. Many of these hormones have a daytime secretion pattern, thus in misalignment situations the transmission of these biochemical signals compromises the mechanism called clock-hormone-interaction, so different circadian oscillators, present in tissues, can impact cognitive performance19,21,43. A similar mechanism occurs in more fragmented individuals – with higher values of IV – in this case, the fragmentation of the wake-sleep cycle negatively compromises sleep efficiency33. Since this cycle is also influenced by the circadian timing system, the misalignment caused by the evening ‘wake-maintenance zone’ (WMZ) and ‘sleep-promoting zone’ (SPZ) leads to an abrupt deterioration of cognitive performance and both situations compromise cognitive performance12,44. We predicted that the rotating worker would generally present a lower IS value, but we observed that some volunteers presented a more regular level of synchronization than others, and this may result in better parameters in psychomotor performance. We predicted that the rotating worker would generally present a lower IS value, but we observed that some volunteers presented a more regular level of synchronization than others, and this may result in better parameters in psychomotor performance. We emphasize that new studies are necessary to confirm these findings.
The results from the present study corroborate the study of Chellapa et al.45, who performed a protocol of circadian misalignment/alignment in night shift workers. The authors showed the effect of the “circadian misalignment condition” on the decrease in cognitive performance when comparing the first day of evaluations (T1) with the others (T2, T3 and T4)45. This data can be considered relevant because, although night work leads to circadian desynchronisation, as explained previously, the effect of night work on cognitive performance seems to occur independently of circadian misalignment. Nonetheless, it is important to recognise the potential interaction between night shift work and circadian effects on psychomotor performance, since all these changes related to misalignment drastically impact all physiological functions that have circadian rhythmicity40.
Our results also showed that obese individuals presented higher values of lapses in attention throughout the shift schedule compared with eutrophic ones (Figs. 2, 3A,B). Cook et al.23 also found that obese individuals had a decrease in psychomotor performance when compared to non-obese. Tsai, Huang and Tsai46 presented evidence that the group of obese volunteers presented a slower reaction time (PVT) compared with the control group, which impacts the decrease in cognitive performance of obese individuals. Although we believe that eating habits can affect cognitive performance17, other studies23,47 suggested that the possible mechanisms that lead to a reduction in cognitive performance in obese individuals are linked to increased oxidative stress, metabolic dysfunctions and systemic inflammation that are capable of interfering with brain functions linked to cognitive performance23. In this sense, there is increasing evidence linking neuroinflammation with the pathogenesis of obesity and, consequently, with cognitive decline47. Another possible explanation for the relationship between obesity and impaired cognitive performance found in the present study may be the increased risk in sleep-disordered breathing48 and poorer sleep quality49 in obese individuals. Considering the role of sleep on the psychomotor performance already documented in the literature48 we might assume that such sleep disorders - and not directly obesity - could mediate impairments in cognitive performance. In the present study, having sleep disorders was considered an exclusion criterion, but this identification may have failed because volunteers did not perform the polysomnography. Further studies should assess whether the effect of BMI on the number of lapses can be mediated by the sleep pattern.
In the present study we did not find significant effects of interaction between IS/IV and BMI on psychomotor performance (Table 4). There is little evidence that components of cognitive function such as vigilance and the number of lapses of attention may also be impacted by the association between circadian misalignment50 and obesity23. As recent evidence shows that shift work34 is related to negative effects on psychomotor performance51, we postulated that these variables – shift work, obesity and circadian misalignment - could interact to produce a worse psychomotor performance, but perhaps the isolated impact of other factors common to shift work- such as sleep deprivation itself- may have hampered this identification. Future research that should be done to elucidate this issue.
This study has limitations. The study was conducted within a sample composed of only male workers; a study including women and with a more relevant sample size is necessary for better understanding of the association between alternating shift work and work performance in the general population. Although the data collected were objective, they were dependent on the collaboration of the participants, since the correct use of the devices and the performance of the tests at all times can determine the quality of the data. Furthermore, the performance tasks were applied in a quiet and empty room to minimise the influence of psychological and behavioural determinants.
Conclusion
The psychomotor performance of workers was affected by shift rotation, especially in the group of workers that were less desynchronised, with fragmented rhythm and overweight and/or obese. Also, eutrophic individuals – both synchronised and with low fragmentation – performed better than overweight/obese ones; the eutrophic group was impacted only by the night shift, increasing the lapses in attention on those days. Additional studies should be performed to confirm these findings.
References
Dall’Ora, C., Ball, J., Recio-Saucedo, A. & Griffiths, P. Characteristics of shift work and their impact on employee performance and wellbeing: A literature review. Int. J. Nurs. Stud. 57, 12–27 (2016).
Akerstedt, T. & Wright, K. P. Jr. Sleep loss and fatigue in shift work and shift work disorder. Sleep Med. Clin. 4, 257–271 (2009).
Alterman, T. et al. Prevalence rates of work organization characteristics among workers in the U.S.: data from the 2010 National Health Interview Survey. Am. J. Ind. Med. 56, 647–59 (2013).
IBGE, https://biblioteca.ibge.gov.br/visualizacao/livros/liv97329.pdf (2016).
Knauth, P. Designing better shift systems. Appl. Ergon. 27, 39–44 (1996).
Waage, S. et al. Subjective and objective sleepiness among oil rig workers during three different shift schedules. Sleep Med. 13, 64–72 (2012).
Kantermann, T. et al. The direction of shift-work rotation impacts metabolic risk independent of chronotype and social jetlag–an exploratory pilot study. Chronobiol. Int. 31, 1139–1145 (2014).
Partch, C. L., Green, C. B. & Takahashi, J. S. Molecular architecture of the mammalian circadian clock. Trends Cell Biol. 24, 90–99 (2014).
Jin, Y., Hur, T. Y. & Hong, Y. Circadian rhythm disruption and subsequent neurological disorders in night-shift workers. J. Lifestyle Med. 7, 45–50 (2017).
James, S. M., Honn, K. A., Gaddameedhi, S. & Van Dongen, H. P. A. Shift work: disrupted circadian rhythms and sleep-implications for health and well-being. Curr. Sleep Med. Rep. 3, 104–112 (2017).
West, A. C. et al. Misalignment with the external light environment drives metabolic and cardiac dysfunction. Nat. Commun. 8, 417 (2017).
Luik, A. I., Zuurbier, L. A., Hofman, A., Van Someren, E. J. & Tiemeier, H. Stability and fragmentation of the activity rhythm across the sleep-wake cycle: the importance of age, lifestyle, and mental health. Chronobiol. Int. 30, 1223–1230 (2013).
Correa, A., Molina, E. & Sanabria, D. Effects of chronotype and time of day on the vigilance decrement during simulated driving. Accid. Anal. Prev. 67, 113–118 (2014).
Lara, T., Madrid, J. A. & Correa, Á. The vigilance decrement in executive function is attenuated when individual chronotypes perform at their optimal time of day. Plos One 9, e88820 (2014).
Posada-Quintero, H. F., Bolkhovsky, J. B., Reljin, N. & Chon, K. H. Sleep deprivation in young and healthy subjects is more sensitively identified by higher frequencies of electrodermal activity than by skin conductance level evaluated in the time domain. Front. Physiol. 8, 1–9 (2017).
Akerstedt, T., Axelsson, J., Lekander, M., Orsini, N. & Kecklund, G. The daily variation in sleepiness and its relation to the preceding sleep episode—a prospective study across 42 days of normal living. J. Sleep Res. 22, 258–265 (2013).
Leedo, E., Beck, A. M., Astrup, A. & Lassen, A. D. The effectiveness of healthy meals at work on reaction time, mood and dietary intake: a randomised cross-over study in daytime and shift workers at an university hospital. Br. J. Nutr. 118, 121–129 (2017).
Grant, C. L. et al. The impact of meal timing on performance, sleepiness, gastric upset, and hunger during simulated night shift. Ind. Health 55, 423436 (2017).
Vetter, C., Fischer, D., Matera, J. L. & Roenneberg, T. Aligning work and circadian time in shift workers improves sleep and reduces circadian disruption. Curr. Biol. 25, 907–911 (2015).
Crispim, C. A. et al. The influence of sleep and sleep loss upon food intake and metabolism. Nutr. Res. Rev. 20, 195–212 (2007).
McHill, A. W. et al. Impact of circadian misalignment on energy metabolism during simulated nightshift work. Proc. Natl. Acad. Sci. USA 111, 1730217307 (2014).
Taheri, S., Lin, L., Austin, D., Young, T. & Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 1, e62 (2004).
Cook, R. L. et al. Relationship between obesity and cognitive function in young women: the food, mood and mind study. J. Obes. 2017, 5923862 (2017).
Gupta, C. C. et al. It’s not just what you eat but when: the impact of eating a meal during simulated shift work on driving performance. Chronobiol. Int. 34, 66–77 (2017).
Matthews, D. R. et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Friedewald, W. T., Levy, R. I. & Fredrickson, D. S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 18, 499–502 (1972).
Lohman, T. G., Roche, A. F. & Martorell, R. Anthropometric Standardization Reference Manual (Human Kinetics Books, Champaign, IL, 1988).
Heyward, V. & Stolarczyk, L. Avaliação da Composição Corporal Aplicada (Editora Manole, 2000).
WHO. Obesity: preventing and managing the global epidemic. World Health Organ. Tech. Rep. Ser. 894, 1–253 (2000).
Martin, J. L. & Hakim, A. D. Wrist actigraphy. Chest 139, 1514–1527 (2011).
Marino, M. et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep 36, 1747–1755 (2013).
Mitchell, J. A. et al. Variation in actigraphy-estimated rest-activity patterns by demographic factors. Chronobiol. Int. 34, 1042–1056 (2017).
Gonçalves, B. S. B., Adamowicz, T., Louzada, F. M., Moreno, C. R. & Araujo, J. F. A fresh look at the use of nonparametric analysis in actimetry. Sleep Med. Rev. 20, 84–91 (2015).
Basner, M. & Dinges, D. F. Maximizing sensitivity of the psychomotor vigilance test (PVT) to sleep loss. Sleep. 34, 581–91 (2011).
Narciso, F. V. et al. Effects of shift work on the postural and psychomotor performance of night workers. PLoS One 11, e0151609 (2016).
Magee, M. et al. Associations between number of consecutive night shifts and impairment of neurobehavioral performance during a subsequent simulated night shift. Scand. J. Work Environ. Health 42, 217–227 (2016).
Folkard, S. & Lombardi, D. A. Modeling the impact of the components of long work hours on injuries and “accidents”. Am. J. Ind. Med. 49, 953–963 (2006).
Keith, D. R., Gunderson, E. W., Haney, M., Foltin, R. W. & Hart, C. L. Smoked marijuana attenuates performance and mood disruptions during simulated night shift work. Drug Alcohol Depend. 178, 534–543 (2017).
Reinke, L., Ozbay, Y., Dieperink, W. & Tulleken, J. E. The effect of chronotype on sleepiness, fatigue, and psychomotor vigilance of ICU nurses during the night shift. Intensive Care Med. 41, 657–666 (2015).
Oriyama, S. & Miyakoshi, Y. The effects of nighttime napping on sleep, sleep inertia, and performance during simulated 16 h night work: a pilot study. J. Occup. Health 60, 172–181 (2018).
Short, M. A., Agostini, A., Lushington, K. & Dorrian, J. A systematic review of the sleep, sleepiness, and performance implications of limited wake shift work schedules. Scand. J. Work Environ. Health 41, 425–440 (2015).
Chinoy, E. D., Harris, M. P., Kim, M. J., Wang, W. & Duffy, J. F. Scheduled evening sleep and enhanced lighting improve adaptation to night shift work in older adults. Occup. Environ. Med. 73, 869–876 (2016).
Tsang, A. H., Barclay, J. L. & Oster, H. Interactions between endocrine and circadian systems. J. Mol. Endocrinol. 52, R1–16 (2014).
Ly, J. Q. et al. Circadian regulation of human cortical excitability. Nat. Commun. 7, 11828 (2016).
Chellappa, S. L., Morris, C. J. & Scheer, F. Daily circadian misalignment impairs human cognitive performance task-dependently. Sci. Rep. 8, 3041 (2018).
Tsai, C. L., Huang, T. H. & Tsai, M. C. Neurocognitive performances of visuospatial attention and the correlations with metabolic and inflammatory biomarkers in adults with obesity. Exp. Physiol. 102, 1683–1699 (2017).
Moreno-Navarrete, J. M. et al. Neuroinflammation in obesity: circulating lipopolysaccharide-binding protein associates with brain structure and cognitive performance. Int. J. Obes. (Lond) 41, 1627–1635 (2017).
Cori, J. M. et al. The Differential Effects of Regular Shift Work and Obstructive Sleep Apnea on Sleepiness, Mood and Neurocognitive Function. Journal of Clinical Sleep Medicine 14, 6 (2018).
Kim, B.-il et al. Factors related with quality on sleep of daytime workers. Annals of Occupational and Environmental Medicine 30, 63 (2018).
Cheng, P., Tallent, G., Bender, T. J., Tran, K. M. & Drake, C. L. Shift Work and Cognitive Flexibility: Decomposing Task Performance. J. Biol. Rhythms 32, 143–153 (2017).
Fisk, A. S. et al. Light and Cognition: Roles for Circadian Rhythms, Sleep, and Arousal. Frontiers in Neurology 9, 56 (2018).
Author information
Authors and Affiliations
Contributions
D.E.R. and L.P.M. designed the study, researched the data and wrote the manuscript. M.T.M, F.V.N., B.S.B.G. and E.C.M. contributed to the analytical plan, discussion, reviewed and edited the manuscript. C.A.C. designed the study, contributed to the analytical plan, discussion, reviewed and edited the manuscript. All authors contributed to the discussion of the results and reviewed the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rosa, D.E., Marot, L.P., de Mello, M.T. et al. Shift rotation, circadian misalignment and excessive body weight influence psychomotor performance: a prospective and observational study under real life conditions. Sci Rep 9, 19333 (2019). https://doi.org/10.1038/s41598-019-55114-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-55114-w
This article is cited by
-
Impaired psychomotor vigilance associated with sleep-disordered breathing in women working in the care of older adults in Japan
Sleep and Breathing (2022)
-
Association between chronotype and psychomotor performance of rotating shift workers
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
