
Abstract
Besides clinical characteristics, easy-accessible laboratory markers could be of value to refine risk stratification in peripheral artery disease. In the current study, we investigated whether α-hydroxybutyrate dehydrogenase (HBDH) is associated with atherothrombotic events in 83 stable patients undergoing infrainguinal angioplasty and stenting. The primary endpoint was defined as the composite of the first occurrence of nonfatal myocardial infarction, nonfatal stroke or transient ischemic attack and cardiovascular death within 2 years after angioplasty and stenting, and occurred in 6 patients (7.2%). HBDH levels at baseline were significantly higher in patients who subsequently developed the primary endpoint (126 U/L [116–137 U/L] vs. 105 U/L [95–120 U/L]; p = 0.04). ROC curve analysis revealed that HBDH could distinguish between patients without and with future atherothrombotic events. A HBDH concentration ≥ 115 U/L was identified as the best threshold to predict the composite endpoint, providing a sensitivity of 83.3% and a specificity of 71.4%, and was therefore defined as high HBDH. High HBDH was seen in 28 patients (33.7%). Ischemic events occurred significantly more often in patients with high HBDH than in patients with lower HBDH levels (5 vs. 1 patients, p = 0.007). In conclusion, HBDH is associated with the occurrence of atherothrombotic events after infrainguinal angioplasty with stent implantation. Future trials are warranted to study the predictive role of HBDH for ischemic outcomes and to investigate underlying mechanisms.
Similar content being viewed by others
Introduction
Patients with peripheral artery disease (PAD) are at an increased risk of atherothrombotic events like myocardial infarction and stroke1. Moreover, previous studies have shown that those undergoing angioplasty and stenting for PAD frequently suffer target vessel restenosis or reocclusion2,3,4. While the latter are predominantly a consequence of intimal hyperplasia5, atherothrombotic events are often initiated by plaque rupture with subsequent platelet and coagulation activation6, and may therefore be prevented by more intense antithrombotic therapy7,8. Indeed, a new antithrombotic regimen consisting of platelet inhibition with low-dose aspirin and inhibition of thrombin generation with a very low dose of the factor Xa antagonist rivaroxaban recently yielded promising results in patients with stable PAD9. In detail, rivaroxaban 2.5 mg twice daily in additon to 100 mg aspirin significantly reduced the occurrence of atherothrombotic events compared to 100 mg aspirin alone in 7470 PAD patients of the COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial. However, the decrease in ischemic outcomes was achieved at the cost of an increased major bleeding risk9. Consequently, the new treatment regimen should only be prescribed in PAD patients at high risk of atherothrombotic events. In order to optimally select PAD patients in need of intensified antithrombotic therapy, it seems crucial to identify factors associated with adverse ischemic outcomes. Besides clinical characteristics, easy-accessible laboratory markers could be of value to refine risk stratification in PAD.
α-Hydroxybutyrate dehydrogenase (HBDH) is a marker of cell death particularly reflecting renal, red blood cell and myocardial damage10,11,12,13,14. Since chronic kidney disease, anemia and myocardial injury predispose patients to adverse events following percutaneous coronary intervention10,15,16,17,18,19,20, we hypothesized that HBDH may be associated with ischemic outcomes following infrainguinal angioplasty and stenting for stable PAD.
Methods
Patients
In this prospective cohort study, 83 patients undergoing successful infrainguinal angioplasty with endovascular stent implantation were enrolled consecutively at the Division of Vascular Medicine of the Medical University of Vienna21. All patients had intermittent claudication classified as Rutherford stages of PAD 2–3 due to sonographically confirmed infrainguinal artery stenosis and occlusion, respectively. All patients received long-term aspirin therapy (100 mg/day), and 75 mg of clopidogrel per day for three months following angioplasty and stenting. Clinical follow-up was assessed 1 and 2 years after the percutaneous intervention.
Exclusion criteria were a known aspirin or clopidogrel intolerance (allergic reactions, gastrointestinal bleeding), a therapy with vitamin K antagonists (warfarin, phenprocoumon, acenocoumarol) or direct oral anticoagulants (dabigatran, rivaroxaban, apixaban and edoxaban), a treatment with ticlopidine, dipyridamol or nonsteroidal antiinflammatory drugs, a family or personal history of bleeding disorders, malignant paraproteinemias, myeloproliferative disorders or heparin-induced thrombocytopenia, severe hepatic failure, known qualitative defects in thrombocyte function, a major surgical procedure within one week before enrollment, a platelet count <100.000 or >450.000/µl and a haematocrit <30%22.
The study protocol was approved by the Ethics Committee of the Medical University of Vienna in accordance with the Declaration of Helsinki and written informed consent was obtained from all study participants.
Blood sampling
As previously described22, blood was drawn by aseptic venipuncture from an antecubital vein using a 21-gauge butterfly needle (0.8 × 19 mm; Greiner Bio-One, Kremsmünster, Austria) one day after the percutaneous intervention. To avoid procedural deviations all blood samples were taken by the same physician applying a light tourniquet, which was immediately released and the samples were mixed adequately by gently inverting the tubes.
Measurement of HBDH, lactate dehydrogenase (LDH) and free haemoglobin
HBDH, LDH and free haemoglobin were measured in the central laboratory of the Medical University of Vienna according to standardized protocols.
Clinical endpoints
Clinical follow-up was assessed at regular visits of the study participants to the outpatient department of the Division of Vascular Medicine at the Medical University of Vienna and via telephone calls, respectively. The primary endpoint was defined as the composite of the first occurrence of nonfatal myocardial infarction, nonfatal stroke or transient ischemic attack, and cardiovascular death within 2 years after angioplasty and stenting21. Target vessel restenosis > 80% or reocclusion as assessed by duplex sonography was defined as secondary endpoint.
Sample size calculation and statistical analysis
A sample size calculation was based on the observed mean ± SD (108 ± 26 U/L) of HBDH in a former population of 30 stable PAD patients (15 male, 15 female; age 64 years (58–71 years)) 24 hours after angioplasty and stenting23,24,25. We calculated that we needed to include 80 patients to be able to detect a 30% relative difference of HBDH between patients without and with the primary endpoint with a power of 83% (using a two-sided alpha level of 0.05). To compensate for loss to follow-up we included 3 additional patients24.
Statistical analysis was performed using the Statistical Package for Social Sciences (IBM SPSS version 25, Armonk, New York, USA). Median and interquartile range of continuous variables are shown. Categorical variables are given as number (%). We performed Mann Whitney U tests to detect differences of continuous variables. The chi-square test and the Fisher´s exact test were used to detect differences in categorical variables, respectively24. Receiver operating characteristic (ROC) curve analysis was used to determine the ability of HBDH to distinguish between patients without and with the primary endpoint25. The p-value was determined using the DeLong test. The optimal cut-off value was calculated by determining the HBDH level that provided the greatest sum of sensitivity and specificity. A survival curve was generated using the Kaplan-Meier method, and the difference between the groups was assessed by the log-rank test. Two-sided p-values < 0.05 were considered statistically significant21,24,25.
Results
Characteristics of the overall study population and of patients without and with the primary endpoint are shown in Table 1. HBDH in the overall study population was 106 U/L (95–123 U/L). Of note, none of the included patients had suffered myocardial infarction within 6 months prior to infrainguinal angioplasty and stenting. Moreover, a history of myocardial infarction was present in 18.2% and 16.7% of patients without and with the primary endpoint, respectively (Table 1; p = 1). Twenty-eight (33.7%) and 23 (27.7%) patients of the study population had documented stable coronary artery disease (CAD) and cerebrovascular disease (CVD) at study inclusion, respectively. The presence of stable CAD and CVD at baseline did not differ significantly between patients without and with the primary endpoint (Table 1; both p ≥ 0.7). Polyvascular disease was documented in 41 patients (49.4%) at study inclusion (10 patients with PAD, CAD and CVD; 18 patients with PAD and CAD; 13 patients with PAD and CVD; Table 1). The presence of polyvascular disease at baseline did not differ significantly between patients without and with the primary endpoint (38 (49.4%) vs. 3 (50%) patients; p = 1).
The primary endpoint occurred in 6 patients (7.2% of the study population) within 2 years after peripheral angioplasty with stent implantation and comprised 2 nonfatal myocardial infarctions, 2 nonfatal strokes, 1 transient ischemic attack and 1 cardiovascular death. Target vessel restenosis or reocclusion occurred in 28 patients (33.7%) during follow-up.
HBDH levels at baseline were significantly higher in patients who subsequently developed the primary endpoint (Fig. 1; Table 1; 126 U/L [116–137 U/L] vs. 105 U/L [95–120 U/L]; p = 0.04). In contrast, LDH and free haemoglobin levels did not differ significantly between patients without and with atherothrombotic events during follow-up (Table 1; LDH: 167 U/L [145–187 U/L] vs. 179 U/L [166–229 U/L]; free haemoglobin: 2.1 mg/dL [1.4–3.4 mg/dL] vs. 1.7 mg/dL [1.3–2 mg/dL]; both p ≥ 0.2). HBDH, LDH and free haemoglobin were similar in patients without and with target vessel restenosis or reocclusion within 2 years after angioplasty and stenting (all p > 0.6).

α-Hydroxybutyrate dehydrogenase (HBDH) in patients without and with the primary endpoint. The boundaries of the box show the lower and upper quartile of data, and the line inside the box represents the median. Whiskers are drawn from the edge of the box to the highest and lowest values that are outside the box but within 1.5 times the box length.
ROC curve analysis revealed that HBDH could distinguish between patients without and with future atherothrombotic events (Fig. 2; area under the curve = 0.753, 95% CI 0.61–0.9; p = 0.04). A HBDH concentration ≥ 115 U/L was identified as the best threshold to predict the composite endpoint, providing a sensitivity of 83.3% and a specificity of 71.4%, and was therefore defined as high HBDH. High HBDH was seen in 28 patients (33.7% of the study population). Ischemic events occurred significantly more often in patients with high HBDH than in patients with lower HBDH levels (Fig. 3; 5 vs. 1 patients, p = 0.007 with the log-rank test).

Receiver-operating characteristic curve for the analysis of the predictive value of α-hydroxybutyrate dehydrogenase (HBDH) for the primary endpoint. An area under the curve of 0.753 was observed (95% CI 0.61–0.9; p = 0.04). The cut-off value for high HBDH is shown as vertical dotted line originating from the x-axis.

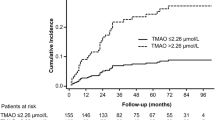
Kaplan-Meier analysis for the cumulative incidence of the primary endpoint in patients with high and low α-hydroxybutyrate dehydrogenase (HBDH). High HBDH is indicated by the dotted line, low HBDH is indicated by the solid line.
Discussion
Our study is the first to investigate the association of markers of cell death with clinical outcomes following infrainguinal angioplasty and stenting for PAD. High levels of HBDH were linked to an increased risk of atherothrombotic events over 2 years, whereas target lesion restenosis and reocclusion did not occur more frequently in patients with high HBDH. Plasma concentrations of LDH and free haemoglobin were not linked to atherothrombotic events and target lesion restenosis or reocclusion, respectively.
HBDH was investigated as a potential risk marker because it reflects renal, red blood cell and myocardial injury10,11,12,13,14. In order to study whether cell death in general or red cell damage alone are linked to ischemic outcomes, we decided to also measure LDH and free haemoglobin concentrations, respectively. Our results, however, point towards HBDH as most promising risk predictor of atherothrombotic events among these 3 markers of cell injury. Of note, serum creatinine, haemoglobin and haematocrit alone did not differ significantly between patients without and with the primary endpoint in our study (Table 1). However, serum creatinine was numerically higher and both haemoglobin and haematocrit were numerically lower in patients who subsequently developed the primary endpoint. It may therefore be speculated that by combining information on subclinical kidney, red blood cell and myocardial injury, HBDH may represent a more sensitive risk marker for atherothrombotic outcomes than the respective laboratory values alone.
Considering the inclusion of patients with manifest atherosclerotic cardiovascular disease, we observed a rather low rate of atherothrombotic events during follow-up. This may be due to 1. the inclusion of stable PAD patients undergoing elective infrainguinal angioplasty and stenting because of intermittent claudication and 2. optimal medical treatment and risk factor management following the percutaneous intervention. In detail, all patients received state-of-the-art antiplatelet, antihypertensive and lipid-lowering therapy and had regular check-ups at the outpatient department every 6 months2. As a next step, it would be interesting to study the predictive value of HBDH for atherothrombotic outcomes in high-risk patients. Among PAD patients, especially those suffering critical limb ischemia may benefit from adequate risk stratification in order to receive an individually tailored treatment approach and follow-up strategy. Finally, HBDH may also be linked to the prognosis of patients with chronic or acute ischemic heart disease and cerebrovascular disease, respectively.
The lack of a significant association between HBDH levels and target vessel restenosis or reocclusion may be explained by differences in the underlying pathomechanisms: Target vessel restenosis usually occurs due to intimal hyperplasia potentially resulting from chronic inflammation26. In contrast, myocardial infarction, stroke and cardiovascular death primarily arise from a prothrombotic environment6. Our finding of an association between HBDH and atherothrombotic events suggests that HBDH levels might mirror the latter. However, large clinical trials confirming HBDH as predictor of thrombotic outcomes are needed before HBDH can be considered for risk stratification in PAD.
Due to the small sample size, our study should be considered hypothesis-generating only. Moreover, we exclusively enrolled stable PAD patients who underwent elective infrainguinal angioplasty and stenting due to intermittent claudication. Therefore, our results cannot be extrapolated to patients with critical limb ischemia. Elevated HBDH levels may be attributable to individual reactions to the peripheral interventions. Alternatively, HBDH might have already been increased before angioplasty and stenting in some patients, reflecting increased cell turnover or damage. Unfortunately, all markers of cell death were only determined 24 hours after the intervention. Consequently, we cannot provide preprocedural HBDH values or data on the variability of HBDH levels over time. This time point was chosen because (1) 24 hours after the elective procedures, all patients were still at the inpatient ward, and (2) we sought to investigate whether or not a single postprocedural HBDH measurement may be used for risk stratification. Further, the AUC of 0.753 observed in the ROC curve cannot be considered a strong classifier. Finally, we do not provide mechanistic data supporting the above-discussed speculations.
In conclusion, HBDH is associated with the occurrence of atherothrombotic events after infrainguinal angioplasty with stent implantation. Future trials are warranted to study the predictive role of HBDH for adverse outcomes in patients with critical limb ischemia and other manifestations of cardiovascular disease, and to investigate underlying mechanisms.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
References
Welten, G. M. et al. Long-term prognosis of patients with peripheral arterial disease: a comparison in patients with coronary artery disease. J Am Coll Cardiol 51, 1588–1596, https://doi.org/10.1016/j.jacc.2007.11.077 (2008).
Aboyans, V. et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J 39, 763–816, https://doi.org/10.1093/eurheartj/ehx095 (2018).
Norgren, L. et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg 45(Suppl S), S5–67, https://doi.org/10.1016/j.jvs.2006.12.037 (2007).
Schillinger, M. et al. Balloon angioplasty versus implantation of nitinol stents in the superficial femoral artery. N Engl J Med 354, 1879–1888, https://doi.org/10.1056/NEJMoa051303 (2006).
Gur, I. et al. Clinical outcomes and implications of failed infrainguinal endovascular stents. J Vasc Surg 53(discussion 667), 658–666, https://doi.org/10.1016/j.jvs.2010.09.069 (2011).
Davi, G. & Patrono, C. Platelet activation and atherothrombosis. N Engl J Med 357, 2482–2494, https://doi.org/10.1056/NEJMra071014 (2007).
Pultar, J., Wadowski, P. P., Panzer, S. & Gremmel, T. Oral antiplatelet agents in cardiovascular disease. Vasa, 1–12, https://doi.org/10.1024/0301-1526/a000753 (2018).
Gremmel, T., Michelson, A. D., Frelinger, A. L. III & Bhatt, D. L. Novel aspects of antiplatelet therapy in cardiovascular disease. Res Pract Thromb Haemost 2, 439–449, https://doi.org/10.1002/rth2.12115 (2018).
Anand, S. S. et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet, https://doi.org/10.1016/S0140-6736(17)32409-1 (2017).
Ohlmann, P. et al. Prognostic value of C-reactive protein and cardiac troponin I in primary percutaneous interventions for ST-elevation myocardial infarction. Am Heart J 152, 1161–1167, https://doi.org/10.1016/j.ahj.2006.07.016 (2006).
Dissmann, R., Linderer, T. & Schroder, R. Estimation of enzymatic infarct size: direct comparison of the marker enzymes creatine kinase and alpha-hydroxybutyrate dehydrogenase. Am Heart J 135, 1–9 (1998).
Kemp, M., Donovan, J., Higham, H. & Hooper, J. Biochemical markers of myocardial injury. Br J Anaesth 93, 63–73, https://doi.org/10.1093/bja/aeh148 (2004).
Karayalcin, G., Lanzkowsky, P. & Kari, A. B. Serum alpha-hydroxybutyrate dehydrogenase levels in children with sickle cell disease. Am J Pediatr Hematol Oncol 3, 169–171 (1981).
Apostolov, I. et al. Acute changes of serum markers for tissue damage after ESWL of kidney stones. Int Urol Nephrol 23, 215–220 (1991).
Fox, C. S. et al. Use of evidence-based therapies in short-term outcomes of ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction in patients with chronic kidney disease: a report from the National Cardiovascular Data Acute Coronary Treatment and Intervention Outcomes Network registry. Circulation 121, 357–365, https://doi.org/10.1161/CIRCULATIONAHA.109.865352 (2010).
Surana, S. P., Riella, L. V., Keithi-Reddy, S. R., Charytan, D. M. & Singh, A. K. Acute coronary syndrome in ESRD patients. Kidney Int 75, 558–562, https://doi.org/10.1038/ki.2008.233 (2009).
Stigant, C., Izadnegahdar, M., Levin, A., Buller, C. E. & Humphries, K. H. Outcomes after percutaneous coronary interventions in patients with CKD: improved outcome in the stenting era. Am J Kidney Dis 45, 1002–1009 (2005).
Giustino, G. et al. Impact of Anemia on Platelet Reactivity and Ischemic and Bleeding Risk: From the Assessment of Dual Antiplatelet Therapy With Drug-Eluting Stents Study. Am J Cardiol 117, 1877–1883, https://doi.org/10.1016/j.amjcard.2016.03.034 (2016).
Pilgrim, T. et al. Additive effect of anemia and renal impairment on long-term outcome after percutaneous coronary intervention. PLoS One 9, e114846, https://doi.org/10.1371/journal.pone.0114846 (2014).
Wang, X. et al. Impact of anemia on long-term ischemic events and bleeding events in patients undergoing percutaneous coronary intervention: a system review and meta-analysis. J Thorac Dis 7, 2041–2052, https://doi.org/10.3978/j.issn.2072-1439.2015.11.56 (2015).
Gremmel, T., Koppensteiner, R., Ay, C. & Panzer, S. Residual thrombin generation potential is inversely linked to the occurrence of atherothrombotic events in patients with peripheral arterial disease. Eur J Clin Invest, https://doi.org/10.1111/eci.12236 (2014).
Lee, S., Ay, C., Kopp, C. W., Panzer, S. & Gremmel, T. Impaired glucose metabolism is associated with increased thrombin generation potential in patients undergoing angioplasty and stenting. Cardiovasc Diabetol 17, 131, https://doi.org/10.1186/s12933-018-0774-0 (2018).
Gremmel, T. et al. Response to antiplatelet therapy and platelet reactivity to thrombin receptor activating peptide-6 in cardiovascular interventions: Differences between peripheral and coronary angioplasty. Atherosclerosis 232, 119–124, https://doi.org/10.1016/j.atherosclerosis.2013.10.027 (2014).
Gremmel, T. et al. In vivo and protease-activated receptor-1-mediated platelet activation but not response to antiplatelet therapy predict two-year outcomes after peripheral angioplasty with stent implantation. Thromb Haemost 111, 474–482, https://doi.org/10.1160/TH13-07-0558 (2014).
Gremmel, T. et al. Serum Cholinesterase Levels Are Associated With 2-Year Ischemic Outcomes After Angioplasty and Stenting for Peripheral Artery Disease. J Endovasc Ther 23, 738–743, https://doi.org/10.1177/1526602816655521 (2016).
Ross, R. Atherosclerosis–an inflammatory disease. N Engl J Med 340, 115–126 (1999).
Author information
Authors and Affiliations
Contributions
Silvia Lee: statistical analysis, writing the manuscript. Renate Koppensteiner: critical revision and final approval. Christoph W. Kopp: critical revision and final approval. Thomas Gremmel: study design, patient enrollment, statistical analysis, writing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lee, S., Koppensteiner, R., Kopp, C.W. et al. α-Hydroxybutyrate dehydrogenase is associated with atherothrombotic events following infrainguinal angioplasty and stenting. Sci Rep 9, 18200 (2019). https://doi.org/10.1038/s41598-019-54899-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-54899-0
This article is cited by
-
Serum α-hydroxybutyrate dehydrogenase as a biomarker for predicting survival outcomes in patients with UTUC after radical nephroureterectomy
BMC Urology (2024)
-
Serum hydroxybutyrate dehydrogenase as an early predictive marker of the severity of acute pancreatitis: a retrospective study
BMC Gastroenterology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
