
Abstract
The incidence of gestational hypertension (GH) and pre-eclampsia (PE) is increasing. Use of blood pressure (BP) change patterns may improve early detection of BP abnormalities. We used Linear spline random-effects models to estimate BP patterns across pregnancy for white British and Pakistani women. Pakistani women compared to white British women had lower BP during the first two trimesters of pregnancy, irrespective of the development of GH or PE or presence of a risk factor. Pakistani compared to white British women with GH and PE showed steeper BP increases towards the end of pregnancy. Pakistani women were half as likely to develop GH, but as likely to develop PE than white British women. To conclude; BP trajectories differ by ethnicity. Because GH developed evenly from 20 weeks gestation, and PE occurred more commonly after 36 weeks in both ethnic groups, the lower BP up to the third trimester in Pakistani women resulted in a lower GH rate, whereas PE rates, influenced by the steep third trimester BP increase were similar. Criteria for diagnosing GH and PE may benefit from considering ethnic differences in BP change across pregnancy.
Similar content being viewed by others


Introduction
Ten percent of pregnant women will develop gestational hypertension (GH) or pre-eclampsia (PE)1,2,3,4. The incidence of these conditions is increasing and influenced by population characteristics, in particular the rise in overweight and obesity5,6. GH and PE are major causes of maternal and infant perinatal morbidity and mortality7,8,9. There is also growing evidence that the longer-term cardiovascular health of the mother and offspring exposed to GH or PE may be adversely affected10,11. Consequently the burden to the individual and to health services is growing12,13,14. Early detection and treatment of pregnancy hypertension can reduce risks15,16,17, but this early detection is somewhat hampered by the diagnosis of GH or PE being defined as hypertension after 20 weeks of gestation (i.e. after the nadir of early pregnancy decline in BP reported in many previous studies)18,19,20.
Hypertensive disorders of pregnancy (HDP) which includes GH and PE, represents a spectrum of disorders, all of which are characterised by high diastolic (DBP) or systolic (SBP) blood pressure (BP)21. Elevated BP after 20 weeks in women without a history of hypertension is defined as GH; when it occurs with clinically significant levels of proteinuria it is PE21,22. The offspring of women who develop PE, more so than those developing GH, are at greater risk of adverse outcomes including preterm birth and small for gestational age23. Normal pregnancy is characterised by decreasing levels of BP from conception to 20 weeks then a slight and steady increase thereafter to term20. Elevated BP after 20 weeks in all cases of HDP can be reached by different patterns of gestational BP change, including higher than average levels from conception, a smaller decline in BP in early pregnancy and/or a more rapid or pronounced rise following this early pregnancy decline. Whether different patterns of reaching the criteria for GH and PE are helpful in predicting more adverse outcomes, or what risk factors influence them is unclear and this information may be important when considering diagnostic thresholds and treatment of GH and PE in different ethnic groups.
We have shown previously that in white European women without GH or PE, mean BP at the start of pregnancy, the rate of decline in early pregnancy and the steepness of the increase in late pregnancy, differs by established risk factors (age, parity, BMI, multiple pregnancy) in the same direction that those risk factors are associated with HDP18,24. We have further shown that early BP change can be used to predict which women are likely to experience a HDP, and proposed gestational BP centile charts for use in white European women25,26.
South Asians, in comparison to white Europeans, have higher levels of adiposity for a given body mass from birth, and are at increased risk of insulin resistance, diabetes and coronary heart disease27,28,29,30. In pregnancy this is reflected in higher rates of gestational diabetes and mean levels of fasting and post-load glucose29,31. Greater adiposity and gestational diabetes are both associated with an increased risk of a HDP23,32,33, therefore we might expect HDP to be more common in south Asian women. However, the small number of studies that have compared the incidence of HDP between south Asian and white Europeans have found either a lower or similar incidence34,35,36,37. To our knowledge few previous studies have examined ethnic differences in SBP and DBP change across pregnancy. Those that have include few women from ethnic groups other than white European38,39.
The aims of this study were to explore whether: (i) patterns of BP change in pregnancy differed between white British and Pakistani women; (ii) any differences in BP change between these two ethnic groups were related to differences in GH and PE incidence and whether (iii) established risk factors (maternal age, BMI and parity) for GH and PE differed between the ethnic groups in how they relate to BP trajectories and GH and PE incidence.
By addressing these aims we hope to better understand the mechanisms that might lead to ethnic differences in HDP incidence and to provide the foundations for exploring whether different thresholds for diagnosing GH and PE between these different ethnic groups would improve their detection, management and outcomes.
Methods
Participants
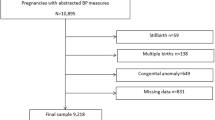
Our analyses were undertaken in two ethnic groups – white British and Pakistani women, because these represent the largest ethnic groups in our cohort study. Data from women participating in the Born in Bradford (BiB) cohort were used. BiB is a prospective birth cohort study including 12,450 women who booked to deliver at the Bradford Royal Infirmary, Bradford, UK, between 2007 and 2011. The cohort is broadly representative of the obstetric population in Bradford and includes equal numbers of Pakistani and white British women. The study methods have been described in full elsewhere40. At recruitment, participants gave informed written consent, height and weight was measured, a questionnaire was administered by trained research assistants and information was abstracted from medical records, informed written consent was also given by participants for the future abstraction of information from medical records. Interviews were conducted in English or in south Asian languages (including Urdu and Mirpuri). Research Ethics Committee approval was obtained (07/H1302/112), all research was performed in accordance with relevant guidelines and regulations. Women were excluded if they did not complete a baseline questionnaire, had one or less BP measurement recorded antenatally or did not have their birth outcomes recorded. Following further exclusions (women with pre-existing hypertension, multiple pregnancies or ‘other’ ethnicities (than white British or Pakistani)), 8212 women were included in these analyses. Figure 1 shows the full inclusion and exclusion criteria of women from BiB for this study.

Study flow chart.
Outcomes
All BP and proteinuria measurements that were recorded as part of routine antenatal care were abstracted from each participant’s medical records (i.e. each woman would have several repeat measurements of SBP, DBP and proteinuria).
These repeat measurements were conducted by midwives, doctors or health care assistants working in the community or hospital clinics, who were trained to measure BP in the seated position using the appropriate cuff size, diastolic BP (DBP) was measured using Korotkoff phase V. Most measurements were scheduled according to UK clinical guideline recommendations (at 10, 16, 28, 34, 36, 38, 41 weeks gestation and additionally at 25, 31 and 40 weeks gestation for women during their first pregnancy)41. Women who were deemed to require additional monitoring by their clinical team or who self-referred for various reasons (for example abdominal pain or reduced fetal movements) had measurements recorded at additional times. A variety of devices were used to measure BP and proteinuria, all devices were calibrated according to standard UK health service practice21. The gestational age on the date of each measurement was derived from the infant’s gestational age at birth and date of measurement, gestational age at birth was derived from the 10 week ultrasound scan and date of birth.
The extraction of BP and proteinuria measurements from paper medical records was undertaken by four trained research assistants. Accuracy of abstractions was checked on 5% of records for all abstracted data; all error rates were less than 1%. The BP and proteinuria repeat measurements were used to derive gestational BP change trajectories across pregnancy and also to define GH and PE in a systematic way for all participants. GH was defined as new-onset hypertension after 20 weeks gestation; DBP equal to or exceeding 90 mmHg and/or SBP equal to or exceeding 140 mmHg on at least two separate occasions. PE was defined as for GH, but also with concurrent (with the elevated blood pressure) clinically significant proteinuria; greater or equal to 1 ‘+’ on the reagent strip reading (the equivalent of ~30 mg/mmol [0.3 mg/mg] on spot urine protein/creatinine ratio)21,22.
Ethnicity, HDP risk factors and other measurements
The woman’s ethnicity, age, education, parity and smoking during pregnancy were obtained from interviewer administered questionnaires at recruitment. Ethnicity was categorised as white British and Pakistani according to UK Office of National Statistics criteria42. Education was equivalized to UK standard attainments and participants were included in one of five mutually exclusive categories (<5 GCSE equivalent, +5 GCSE equivalent, A level equivalent, higher, other)29. Family history of diabetes and hypertension was abstracted from antenatal clinical paper records as described above for the repeat BP and proteinuria measures. Maternal weight as recorded at the first antenatal clinic visit, glucose levels (at the 26–28 week gestation oral glucose tolerance test) and infant sex43 were obtained from hospital electronic records. Gestational diabetes was defined according to modified World Health Organization (WHO) criteria operating at the time of recruitment (either fasting glucose ≥6·1 mmol/L, or 2 h post-load glucose ≥7·8 mmol/L)29,44.
Body mass index (BMI kg/m2) was calculated using height from the recruitment assessment and the first antenatal clinic visit weight, which was generally before 12 weeks gestation, as that would be little influenced by pregnancy or fetal size in comparison to the measure at recruitment (around 28 weeks). BMI was categorised according to WHO definitions of underweight or normal (≤24.9 kg/m2; there being too few women to categorize underweight separately), overweight (≥25.0–29.9 kg/m2) and obese (≥30.0 kg/m2)45. Smoking during pregnancy which was self-reported and categorized as yes or no.
Statistical analysis
Linear spline random-effects models were used to derive SBP and DBP change trajectories across gestation, as previously described18,24. Multilevel modelling (using antenatal visit as level 1 and woman as level 2) was conducted to account for multiple antenatal measurements and clustering (non-independence) of these within each woman. The median, interquartile range, and full range of the number of BP measurements per woman were 10, 8–14 and 1–142 respectively. In order to prevent the small number of women with many repeat measurements overly influencing results we split gestation into two week periods and for any woman who had more than one measure in any of these two-week periods, one measurement was selected at random to remain in the analyses. This was achieved by creating a random number for each record using the invnorm(uniform)) command in Stata, sorting data by participant identifier, gestation period and random number, then choosing the first record within each gestation period. Following this, there was a median of 9 BP measurements per woman (interquartile range, 8–10 and full range 2–16).
The best fitting model was derived using fractional polynomials; we examined these in the whole cohort and for the two ethnic groups, with the appearance of the average cohort trajectory from this modelling used to explore potential knot points. Knot points are the gestational ages at which a change in the direction or magnitude of BP trajectory slopes occurs. We examined the five highest log-likelihoods for SBP and DBP models separately, in the whole cohort and also separately for white British and Pakistani women. Our aim was to identify knot points that were a good reflection (fit) of the observed data and if possible have similar knot points for both SBP and DBP and for both ethnic groups in order to aid comparisons. We set eight weeks gestation as the baseline (intercept) as there were too few measurements before that time to produce meaningful results. The modelling created five measurements of SBP and DBP change for each woman: baseline level at 8 weeks (intercept) and change between 8 and 24, 24 and 30, 30 and 36 weeks and 36 weeks to delivery.
Women with PE have a high risk of preterm delivery, particularly if maternal BP rises rapidly, and earlier delivery may lead to fewer measurements contributing to the models and thus a lower influence from pregnancies with a steeper increase in BP, so underestimating the slope. In order to adust for this, we combined the random-effects spline models for BP change with length of gestation to produce a joint model18. Individual trajectories and trajectories by categorical covariates were obtained from random-intercept and -slope models, which provide a measure of each individual’s deviation from the whole cohort mean BP at 8-weeks and from the average slope in each period of gestation. The following covariates were explored in these models: HDP (normotensive (reference group), GH, PE); age (<25 (reference) 25–29, 30–35, >35); BMI (underweight/normal (reference), overweight, obese); ethnicity (white British (reference), Pakistani); parity (nulliparous (reference), multiparous); smoking in pregnancy (no (reference), yes); gestational diabetes (no (reference), yes); education (<5 GCSE equivalent (reference), 5+ GCSE equivalent, A level equivalent, higher, other) and offspring sex (male (reference), female).
The associations between BP changes and time to delivery were derived from the random effects for BP outcomes and the residual error from the length of gestation. Our initial model (model 1) adjusted for all covariates (described above). In model 2, we additionally adjusted each slope (mean change in BP per gestational week) for the mean BP at 8 weeks, and each proceeding slope(s), so that results were not confounded by the initial BP measure and earlier slope(s) which correlate with subsequent slopes18,24.
Ethics approval
Ethics approval was granted by the Bradford National Health Service Research Ethics Committee (ref 07/H1302/112) on 10 March 2008.
Results
Table 1 shows the distribution of characteristics of all women and by ethnic group; 4345 were Pakistani and 3867 white British. Compared to white British women, Pakistani women were older, were more likely to have attained a higher educational level, to be multiparous, less likely to be obese or to have smoked in pregnancy and more likely to have developed gestational diabetes in the current pregnancy and to have a family history of diabetes or hypertension.
Approximately twice as many white British than Pakistani women developed GH (11% vs 5%), whereas similar proportions of white British and Pakistani women developed PE (3% vs 2%). Of those who developed GH in both ethnic groups approximately half developed it between 20 to 36 weeks of gestation and half at or after 36 weeks, whereas most cases of PE in both groups developed at or after 36 weeks (see Table 2).
Table 3 shows the unadjusted associations between risk factors and GH and PE by ethnicity. Generally, point estimates tended to be closer to the null for Pakistani women than for white British women.
Figure 2a–f show the time to delivery adjusted trajectories (i.e. joint model) of SBP and DBP across pregnancy for Pakistani and white British women who were normotensive (see Fig. 2a,b), and who developed GH (see Fig. 2c,d) or PE (see Fig. 2e,f). Tables 4 and 5 show the corresponding mean differences in SBP and DBP respectively at 8 weeks and the change in BP at each subsequent period. Pakistani women who remained normotensive started pregnancy with lower SBP (−4.00, 95% CI: −4.71 to −3.29) and DBP (−1.92, 95% CI:−2.44 to −1.40) and demonstrated lower BP trajectories across pregnancy compared to white British women.

(a,b) Predicted trajectories of systolic blood and diastolic pressure across pregnancy for Pakistani and white British normotensive women. (c,d) Predicted trajectories of systolic and diastolic blood pressure across pregnancy for Pakistani and white British women with gestational hypertension. (e,f) Predicted trajectories of systolic and diastolic blood pressure across pregnancy for Pakistani and white British women with pre-eclampsia. Footnote to (a to f). − or + Denotes where the mean difference in average BP change in the associated time period between White British and Pakistani women is significantly smaller or larger respectively.
There was no evidence of an early pregnancy decline in SBP or DBP in normotensive women for either ethnic group, with a very slight increase in BP in both groups across pregnancy up to 24 weeks, after which the magnitude of rate of change increased (see Fig. 2a,b and Tables 4 and 5).
As with normotensive Pakistani women, Pakistani women who developed GH had lower SBP (−4.93, 95% CI: −7.74 to −2.12) and DBP (−1.58, 95% CI: −3.60 to 0.44) at the start of pregnancy than white British women who developed this condition, and continued with lower levels until 36 weeks. From 36 weeks onwards, a steeper increase in SBP occurred than the increase demonstrated by white British women, such that by delivery Pakistani women with GH had similar SBP and DBP to white British women with GH (see Fig. 2c,d and Tables 4 and 5).
Pakistani women who developed PE began pregnancy with lower SBP (−2.58, 95% CI: −7.16 to 2.00) but similar DBP (0.48, 95% CI: −2.93 to 3.88) than white British women who developed this condition. Pakistani women demonstrated a steeper increase in BP from 30 weeks gestation than white British women. (see Fig. 2e,f). The steepness of the increase continued to term, which meant that by delivery, Pakistani women’s SBP and DBP were similar to those of white British women. White British women who developed PE showed a decline in BP from 24 weeks, their BP reached a nadir at 30 weeks, after which time both SBP and DBP increased until term. Pakistani women with PE did not show a similar decline in BP.
Supplementary Figures 1a to 7b show the adjusted (Model 2) average shaped SBP trajectories and Supplementary Figures 8a to 14b the adjusted (Model 2) average shaped DBP trajectories for Pakistani and white British women by HDP category and maternal risk factor. These trajectories were consistent with what we would expect from patterns seen with associations of each risk factor with each HDP. Supplementary Tables 1 and 2 show the adjusted mean difference (with 95% CI) in SBP and DBP at eight weeks and change in SBP and DBP in each period of gestation by GH and PE for each ethnic group.
Table 6 shows the associations of BP at eight weeks and changes in BP with time to delivery. SBP and DBP at 8 weeks gestation and BP change in any period of pregnancy was not associated with gestational length in either ethnic group, with the exception of SBP, but not DBP change between 8 and 24 weeks which was weakly associated with a reduction in gestational length for white British women only.
Supplementary Table 3 shows similar predicted lengths of gestation at 2 SDs above and below the average SBP and DBP at 8 weeks and changes in SBP and DBP in each period of gestation for Pakistani and white British women.
Discussion
We found that Pakistani women start pregnancy with lower SBP and DBP than white British women. This is true for women who remain normotensive throughout their pregnancies and for those who go on to develop GH or PE. Generally, normotensive Pakistani and white British women, show gradual increases in BP until 36 weeks when SBP and DBP for both ethnic groups increases more steeply until term. Compared with white British women, Pakistani women who developed either GH or PE had a steeper rise in BP in the third trimester and this difference in BP trajectories influenced the comparison of HDP between the two groups. GH was more common in white British women due to: (a) the combination of the same diagnostic criteria being used across ethnicities, (b) Pakistani women having lower BP levels until the final trimester of pregnancy, and (c) women in both ethnic groups who developed GH doing so evenly between 20–36 and after 36 weeks gestation. By contrast, the proportion with PE was similar in both ethnic groups, because in both groups those developing PE were much more likely to do so after 36 weeks, which meant that the steeper third trimester rise in BP in Pakistani women had a greater impact on their PE rate than their GH rate.
A number of previous studies have reported ethnic differences in the occurrence of GH and PE and the association of risk factors with GH and PE and adverse outcomes for different ethnic groups36,46,47 and one study found similar rates of PE in South Asian and non-Hispanic white Americans36. However, few previous studies have examined ethnic differences in BP trajectories across pregnancy38. A recent study compared Norweigian women with women from eastern Europe, middle east, Africa and south and east Asia, however only 200 south Asian women were included and BP was recorded just twice antenatally39.
The lower rate of GH in Pakistani compared with white British women in our study is not surprising given the lower SBP and DBP of Pakistani women at the start of pregnancy and between 20 and 36 weeks gestation, and that criteria for the diagnosis of HDP are the same in both ethnic groups22.
Our findings provide some evidence for considering the rate of change or trajectory patterns of gestational BP, particularly for understanding ethnic differences in rates of HDP. The use of BP change across pregnancy (usually an increase of >15 mmHg or more from baseline reading) to identify women at increased risk of an adverse outcome has been explored for over 30 years48. However inconsistencies in study methods and their reported findings, together with the complexity of incorporating such measures into clinical guidelines and practice has so far prevented its adoption49,50.
We did not show a decline in BP from early pregnancy to 18/20 weeks that previous studies found18,38,51. This is unlikely to reflect a lack of measurements at 18 to 24 weeks because antenatal measurements were obtained at regular intervals across pregnancy and this did not change over the period of the study22,41. The transitory decline in BP in early pregnancy is thought to reflect the early haemodynamic changes of pregnancy and its end point (around 20 weeks) is used as the marker after which GH and PE are diagnosed. Our finding of a gradual increase in BP in the first two trimesters of pregnancy for normotensive women and women with GH and PE (with the exception of white British women with PE, who showed a decline from 24 to 30 weeks), in both ethnic groups, may reflect the changing characteristics of pregnant women over time and the greater prevalence of risk factors for HDP19. For example, the proportion of women who were overweight and obese included in our previous UK cohort which recruited women in pregnancy in 1990 were 15% and 6%, respectively18,52; in this study, which recruited women 20 years later and from an area of the UK with more deprivation, 29% were overweight and 22% obese40.
Our study is large with many repeated measurements, which allowed a consistent approach to the classification of GH and PE. Use of routinely collected data will introduce a degree of variability, for example use of different BP measurement devices or use of different sized arm cuffs, however all measurements were collected in accordance with clinical care at the time of recruitment and accurately reflect the measurements used to inform clinical decisions related to the diagnosis and treatment of HDP in our study population.
The most recent International Society for the Study of Hypertension in pregnancy (ISSHP) guidance defines PE as high BP on at least two occasions after 20 weeks with concurrent significant proteinuria defined as 2+ on a reagent strip21, the UK NICE do not comment on how many + are appropriate22. Our use of 1+ proteinuria on reagent strip in defining PE reflects the ISSHP criteria for diagnosing PE and what was used in clinical practice in the UK at the time of our study (which preceded the most recent ISSHP guidelines)53.
Compared with the most recent ISSHP criteria our use of 1+ proteinuria may have increased the overall prevalence of PE in our study. However, this will not have altered the ethnic differences in BP trajectories nor the similarity in PE between white British and Pakistani women, which was driven by the steepear increase in BP in Pakistani women. Some of the weaker associations of risk factors with PE compared with GH shown in Table 3 may be because of a lower proteinuria threshold, but given the relatively small numbers with PE and imprecise estimates with wide confidence intervals, we would not be able to distinguish differences in associations with a stricter definition of proteinuria, as the number with PE would be smaller.
Other measures of proteinuria, for example protein-creatinine ratio, may more accurately estimate proteinuria, but they were not consistently recorded at each antenatal visit. Indicators of severe PE, such as evidence of multi-organ involvement were unavailable in our study, so we cannot assess severe PE or eclampsia.
In conclusion, BP trajectories differ by ethnicity. Pakistani women had lower BP at the start of pregnancy and during the first two trimesters, irrespective of the development of a HDP or the presence of a risk factor. Compared to white British women, Pakistani women who developed GH or PE showed steeper increases in BP towards the end of pregnancy. Because GH developed evenly between 20–36 weeks and after 36 weeks gestation and PE occurred more commonly after 36 weeks in both ethnic groups, lower BP up to the third trimester in Pakistani women resulted in a considerably lower GH rate, whereas PE rate, influence by the steep third trimester BP increase is similar in the two groups. Criteria for diagnosing HDP may benefit from considering ethnic differences in BP change across pregnancy.
Data Availability
The Born in Bradford Study allows bone fide researchers to access data. Full details of how to do this are provided on the study web pages (https://borninbradford.nhs.uk/research/how-to-access-data/).
References
Abalos, E., Cuesta, C., Grosso, A. L., Chou, D. & Say, L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Repro Biol 170, 1–7 (2013).
Buchbinder, A. et al. Adverse perinatal outcomes are significantly higher in severe gestational hypertension than in mild preeclampsia. Am J Obstet Gynecol 186, 66–71 (2002).
Hauth, J. C. et al. Pregnancy outcomes in healthy nulliparas who developed hypertension. Calcium for Preeclampsia Prevention Study Group. Obstet Gynecol 95, 24–28 (2000).
Muti, M., Tshimanga, M., Notion, G. T., Bangure, D. & Chonzi, P. Prevalence of pregnancy induced hypertension and pregnancy outcomes among women seeking maternity services in Harare, Zimbabwe. BMC Cardiovasc Disord 15, 111 (2015).
Duckitt, K. & Harrington, D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. BMJ 330, 565 (2005).
Hutcheon, J. A., Lisonkova, S. & Joseph, K. S. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstet Gynaecol 25, 391–403, https://doi.org/10.1016/j.bpobgyn.2011.01.006 (2011).
Cantwell, R. et al. Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer: 2006–08. The Eighth Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG. 118, 1–203 (2011).
Khan, K. S., Wojdyla, D., Say, L., Gülmezoglu, A. M. & Van Look, P. F. A. WHO analysis of causes of maternal death: a systematic review. Lancet 367, 1066–1074, https://doi.org/10.1016/S0140-6736(06)68397-9 (2006).
Bramham, K. et al. Association of Proteinuria Threshold in Pre-Eclampsia with Maternal and Perinatal Outcomes: A Nested Case Control Cohort of High Risk Women. PloS one 8, e76083, https://doi.org/10.1371/journal.pone.0076083 (2013).
Tranquilli, A. L., Landi, B., Giannubilo, S. R. & Sibai, B. M. Preeclampsia: No longer solely a pregnancy disease. Pregnancy Hypertens 2, 350–357, https://doi.org/10.1016/j.preghy.2012.05.006 (2012).
Ayansina, D. et al. Long term effects of gestational hypertension and pre-eclampsia on kidney function: Record linkage study. Pregnancy Hypertens 6, 344–349 (2016).
Ahmed, R. J. et al. The Cost Implications of Less Tight Versus Tight Control of Hypertension in Pregnancy (CHIPS Trial). Hypertension 68, 1049–1055 (2016).
Mistry, H., Dowie, R., Franklin, R. C. G. & Jani, B. R. Costs of neonatal care for low-birthweight babies in English hospitals. Acta Pædiatr 98, 1123–1129 (2009).
Hypertension in Pregnancy: Costing Report: Implementing NICE Guidance. National Collaborating Centre for Women’s and Children’s Health (UK). London: RCOG Press; 2010 Aug.
Cluver, C., Novikova, N., Koopmans, C. M. & West, H. M. Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term. Cochrane Database Syst Revs, https://doi.org/10.1002/14651858.CD009273.pub2 (2017).
Duley, L., Meher, S. & Jones, L. Drugs for treatment of very high blood pressure during pregnancy. Cochrane Database Syst Revis, https://doi.org/10.1002/14651858.CD001449.pub3 (2013).
Duley, L., Gülmezoglu, A. M., Henderson-Smart, D. J. & Chou, D. Magnesium sulphate and other anticonvulsants for women with pre-eclampsia. Cochrane Database Syst Revs, https://doi.org/10.1002/14651858.CD000025.pub2 (2010).
Macdonald-Wallis, C. et al. Blood pressure change in normotensive, gestational hypertensive, preeclamptic, and essential hypertensive pregnancies. Hypertension 59, 1241–1248 (2012).
Magriples, U. et al. Blood pressure changes during pregnancy: impact of race, body mass index, and weight gain. Am J Perinatol 30, 415–424, https://doi.org/10.1055/s-0032-1326987 (2013).
Reiss, R. E., Oshaughnessy, R. W., Quilligan, T. J. & Zuspan, F. P. Retrospective comparison of blood-pressure course during preeclamptic and matched control pregnancies. Am J Obstet Gynecol 156, 894–898 (1987).
Tranquilli, A. L. et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens 4, 97–104 (2014).
Hypertension in Pregnancy: The Management of Hypertensive Disorders During Pregnancy. National Collaborating Centre for Women’s and Children’s Health (UK). London: RCOG Press; 2010 Aug.
Mol, B. W. J. et al. Pre-eclampsia. Lancet 387, 999–1011 (2016).
Macdonald-Wallis, C., Tilling, K., Fraser, A., Nelson, S. M. & Lawlor, D. A. Established preeclampsia risk factors are related to patterns of blood pressure change in normal term pregnancy: findings from the Avon Longitudinal Study of Parents and Children. J Hypertens 29, 1703–1711 (2011).
Macdonald-Wallis, C. et al. Gestational-age-specific reference ranges for blood pressure in pregnancy: findings from a prospective cohort. J hypertens 33, 96–105 (2015).
Macdonald-Wallis, C. et al. Antenatal blood pressure for prediction of pre-eclampsia, preterm birth, and small for gestational age babies: development and validation in two general population cohorts. BMJ 351 (2015).
British Heart Foundation Health Promotion Research Group. Ethnic differences in Cardiovascular disease. Department of Public Health 10th edition (2010).
McKeigue, P. M., Pierpoint, T., Ferrie, J. E. & Marmot, M. G. Relationship of glucose intolerance and hyperinsulinaemia to body fat pattern in South Asians and Europeans. Diabetologia 35, 785–791 (1992).
Lawlor, D. A. et al. Pregnancy glycaemia and cord-blood levels of insulin and leptin in Pakistani and white British mother–offspring pairs: findings from a prospective pregnancy cohort. Diabetologia 57, 2492–2500 (2014).
West, J. et al. UK-born Pakistani-origin infants are relatively more adipose than White British infants: findings from 8704 mother-offspring pairs in the Born-in-Bradford prospective birth cohort. J Epidemiol Community Health 67, 544–551 (2013).
Farrar, D. et al. Association between hyperglycaemia and adverse perinatal outcomes in south Asian and white British women: analysis of data from the Born in Bradford cohort. Lancet Diabetes Endocrinol 3, 795–804 (2015).
Poston, L. et al. Preconceptional and maternal obesity: epidemiology and health consequences. Lancet Diabetes Endocrinol 4, 1025–1036 (2016).
Weissgerber, T. L. & Mudd, L. M. Preeclampsia and Diabetes. Curr Diab Rep 15, 9 (2015).
Naimy, Z., Grytten, J., Monkerud, L. & Eskild, A. The prevalence of pre-eclampsia in migrant relative to native Norwegian women: a population-based study. BJOG 122, 859–865 (2015).
Caughey, A. B., Stotland, N. E., Washington, A. E. & Escobar, G. J. Maternal Ethnicity, Paternal Ethnicity, and Parental Ethnic Discordance: Predictors of Preeclampsia. Obstet Gynecol 106, 156–161 (2005).
Gong, J., Savitz, D. A., Stein, C. R. & Engel, S. M. Maternal ethnicity and pre-eclampsia in New York City, 1995–2003. Paediatr Perinat Epidemiol 26, 45–52 (2012).
Ghosh, G. et al. Racial/ethnic differences in pregnancy-related hypertensive disease in nulliparous women. Ethn Dis 24, 283–289 (2014).
Bouthoorn, S. H. et al. Ethnic Differences in Blood Pressure and Hypertensive Complications During Pregnancy: The Generation R Study. Hypertension 60, 198–205 (2012).
Waage, C. W. et al. Ethnic differences in blood pressure from early pregnancy to postpartum: a Norwegian cohort study. J Hypertension 34, 1151–1159 (2016).
Wright, J. et al. Cohort profile: The Born in Bradford multi-ethnic family cohort study. Int J Epidemiol 4, 1–14 (2012).
Antenatal Care: Routine Care for the Healthy Pregnant Woman. National Collaborating Centre for Women’s and Children’s Health (UK). London: RCOG Press; 2008 Mar.
Office of National Statistics, https://gss.civilservice.gov.uk/wp-content/uploads/2019/04/Ethnic-Group-June-17.pdf.
Di Renzo, G. C., Rosati, A., Sarti, R. D., Cruciani, L. & Cutuli, A. M. Does fetal sex affect pregnancy outcome? Gender Med 4, 19–30 (2007).
World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a WHO consultation. Part 1: diagnosis and classification of diabetes mellitus. (WHO, 1999).
World Health Organization. Body Mass Index – BMI, http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (last accessed January 2018).
Bryant, A. S., Worjoloh, A., Caughey, A. B. & Washington, A. E. Racial/Ethnic Disparities in Obstetrical Outcomes and Care: Prevalence and Determinants. Am J Obs Gynecol 202, 335–343 (2010).
Shahul, S. et al. Racial Disparities in Comorbidities, Complications, and Maternal and Fetal Outcomes in Women with Preeclampsia/Eclampsia. Hypertens Pregnancy 34, 506–515 (2015).
Redman, C. W. G. & Jefferies, M. Revised definition of pre-eclampsia. Lancet 1, 809–812 (1988).
Bullarbo, M. & Rylander, R. Diastolic blood pressure increase is a risk indicator for pre-eclampsia. Arch Gynecol Obstet 291, 819–823 (2015).
Levine, R. J. et al. Should the definition of preeclampsia include a rise in diastolic blood pressure of ≥15 mm Hg to a level <90 mm Hg in association with proteinuria? Am J Obstet Gynecol 183, 787–792 (2000).
Easterling, T. R., Benedetti, T. J., Schmucker, B. C. & Millard, S. P. Maternal Hemodynamics in Normal and Preeclamptic Pregnancies: A Longitudinal Study. Obstet Gynecol 76, 1061–1069 (1990).
Golding, J., Pembrey, M. & Jones, R., The Alspac Study Team. ALSPAC–The Avon Longitudinal Study of Parents and Children. Paediat Perinat Epidemiol 15, 74–87 (2001).
Brown, M. A., Lindheimer, M. D., de Swiet, M., Assche, A. V. & Moutquin, J. M. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy 20 (2001).
Acknowledgements
Born in Bradford is only possible because of the enthusiasm, and commitment of the children, and parents in Born in Bradford. We thank all the participants, health professionals, and researchers who have made Born in Bradford happen. D.F. is supported by a Post-doctoral UK National Institute for Health Research fellowship (PDF-2014-07-019). This report is independent research arising from this Post-doctoral fellowship. The Born in Bradford study is supported by the Wellcome Trust (WT101597MA), UK Medical and Economic and Social Research Councils (MR/N024397/1), and the British Heart Foundation (CS/16/4/32482). Additional support for this work is provided by the European Research Council (DevelopObese; 669545), US National Institute for Health (R01 DK10324), BHF (AA/18/7/34219) and Bristol National Institute for Health Research Biomedical Research Centre. D.A.L. works in a Unit which receives support from the University of Bristol and the UK Medical Research Council (MC_UU_00011/6) and she is a UK National Institute for Health Research Senior Investigator (NF-0616-10102). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
Author information
Authors and Affiliations
Contributions
D.F. and D.A.L. designed this study, with input from other co-authors. D.F. collected the BP measurements, D.F., J.W., D.T. and D.A.L. were involved in the design and data collection of the Born in Bradford study. D.F., C.M.-W., G.S., T.A.S. and D.A.L. developed the analysis protocol and G.S., C.M.-W. and D.F. performed the analyses. D.F. wrote the first draft of the paper with initial further iterations involving all remaining authors and with all authors contributing to the final submitted versions. All authors approved the final version.
Corresponding author
Ethics declarations
Competing Interests
D.A.L. has received support in the last 10 years from National and International governments and charitable funders, Medtronic and Roche Diagnostics for research unrelated to that presented here. The other authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Farrar, D., Santorelli, G., Lawlor, D.A. et al. Blood pressure change across pregnancy in white British and Pakistani women: analysis of data from the Born in Bradford cohort. Sci Rep 9, 13199 (2019). https://doi.org/10.1038/s41598-019-49722-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-49722-9
This article is cited by
-
Social inequalities in pregnancy metabolic profile: findings from the multi-ethnic Born in Bradford cohort study
BMC Pregnancy and Childbirth (2024)
-
Do nuclear magnetic resonance (NMR)-based metabolomics improve the prediction of pregnancy-related disorders? Findings from a UK birth cohort with independent validation
BMC Medicine (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
