
Abstract
Neuroimaging research increasingly suggests there are biological features related to suicidal risk, including brain morphometric features, leading to an elaborate suicide risk assessment. However, few studies have focused on the severity of suicidal ideation and its association with subcortical anatomy in patients with major depressive disorder (MDD). Here, we mainly investigated whether specific structural differences were present in MDD patients with and without suicidal ideation; and supplemented comparison with and without suicidal attempt. We hypothesized that structures associated with suicidal ideation would be derived from a combination of depression and impulsivity. Local atrophy of subcortical structures in 48 patients with MDD (24 with suicidal ideation and 24 without) and 25 age- and sex-matched healthy controls were compared using a surface-based shape analysis method. There was no difference in brain volume between MDD patients with or without suicidal ideations; or MDD patients with or without suicidal attempt. However, the atrophy level in the left pallidum showed a positive correlation with severity of suicidal risk in MDD patients with suicidal ideation. Local atrophy of the left hippocampus, right caudate, and right pallidum had a positive correlation with total impulsivity. These findings possibly suggest that vulnerability to suicidal attempt can be derived from suicidal ideation combined with depression and impulsivity, related to reduced motivational control.
Similar content being viewed by others

Introduction
Although suicide prevention has been thoroughly studied, suicide remains a major cause of morbidity and mortality worldwide. Worldwide, suicide resulted in 800,000 deaths in 2018. Every 40 seconds, the suicide death rate increases; it has risen 4% internationally in the past 10 years1. Major depressive disorder (MDD) is an important illness associated with suicidal ideation and completed suicide2,3,4. However, it is unclear why many patients with MDD have suicidal ideation.
Suicidal risk has been considered as a continuum5 that includes suicidal ideation, plans, attempts, and completion. Growing findings from large cohorts investigating the prevalence of suicidality support the presence of these phenomena across diagnostic entities6,7. Previous studies have reported that many risk factors for suicidal behaviors can predict suicidal ideation, but not the transition from ideation to attempt8,9. However, considering the associations between suicidal ideation, behaviors, and completed suicide10,11, examination of biological correlations of suicidal ideation is important. Recent studies suggest that brain dysfunctions such as impairment in functional connectivity12,13, reduced white matter tracts14, and decreased gray matter density15 in the frontal-subcortical network may impact suicidal ideation in patients with MDD.
Magnetic resonance imaging (MRI), frequently used in studies of structural and functional characteristics, is a noninvasive method to explore the neural correlates of suicidal risk in vivo. Only a few structural brain imaging studies have examined the relationship between subcortical structures and suicidal ideation in patients with MDD, and a recent meta-analysis reported small and non-significant reductions in subcortical and intracranial volumes in MDD16. Subcortical volumetric correlation with suicidal risk, including a history of suicidal ideation to attempt, has been reported. Findings include reduced volumes of the orbitofrontal cortex, caudate, and pallidum17, and increased volume in the right hippocampus18 and amygdala19 in patients with MDD compared to healthy controls. However, few previous studies have focused on the severity of suicidal ideation and its association with subcortical anatomy in MDD patients.
Therefore, the objective of the present study was to elaborate on the neural basis of suicidal ideation in patients with MDD. We compared participants with or without suicidal ideation, and MDD patients with or without suicidal ideation, to adjust for structural characteristics of MDD. We hypothesized that MDD patients with suicidal ideation would display different regional brain volumes than MDD patients without suicidal ideation. We expected the volumes of these brains regions to be positively correlated with severity of suicidal ideation and impulsivity, which could be validated by suicidal attempt. We also hypothesized that structural regions correlated with suicidal ideation would be independent of those correlated with MDD; such differences may be responsible for the decision-making impairment that accompanied to depression leading to suicidal attempt20,21.
Methods
Subjects
A total of 48 patients (5 males and 43 females) with MDD were recruited from the outpatient clinic of the Depression Center of Samsung Medical Center, from April 2011 through April 2013. All patients were clinically referred, and none had received psychotropic medications within 2 weeks of the study or fluoxetine within 4 weeks. Inclusion criteria were: 18 years of age or older and experiencing a current unipolar major depressive episode as verified by the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for MDD22,23. The diagnosis was based on clinical evaluation by a board certified psychiatrist and the full version of the Mini-International Neuropsychiatric Interview (MINI)24. The baseline minimum 17-item Hamilton Scale for Depression (HAM-D)25 score required for enrollment was 16. Exclusion criteria were psychotic disorders (e.g., schizophrenia or delusional disorder), bipolar affective disorder, neurological illness including significant cognitive impairment or Parkinson’s disease, mental retardation, significant medical conditions, epilepsy, history of alcohol or drug dependence, personality disorders, or brain injury.
Additionally, 25 healthy volunteers with no history of psychiatric disease were recruited by advertisement as a control group. Volunteers with a positive family history of mood disorder were excluded. The study protocol was approved by the Ethics Review Board of Samsung Medical Center, Seoul, Korea. All research was performed in accordance with relevant guidelines. Signed informed consent was obtained from all participants.
Clinical evaluation
We divided the MDD group into participants with and without suicidal ideation. We also compared MDD participants with and without suicidal attempt. Participants with suicidal attempt included those with a self-injury history within 1 month and those with a previous lifetime suicide attempt. At entry, the intensity of suicidal ideation was assessed with the Beck Scale for Suicide Ideation (SSI)26. The SSI is a 19-item self-report measure designed to assess the current attitude, behaviors, and plan to commit suicide over the past week. All items are rated on a 3-point scale of intensity and generate a total score between 0 and 38. The results of the SSI were confirmed by a psychiatrist through a clinical interview. The Korean version of the SSI shows acceptable reliability and validity27. Among the 48 patients, 24 were classified as being part of the ‘suicidal ideation group,’ and 24 age/sex-matched patients with MDD who had no suicidal ideation were designated as the ‘no suicidal ideation group.’ Participants were also classified into two groups based on suicidal attempt: 13 had suicidal attempt including self-injury, defined as a self-injury history within 1 month or a previous lifetime suicide attempt; and 35 did not have suicidal attempt. Note that the number of participants in the ‘suicidal attempt’ group is lower than the number in the ‘suicidal ideation’ group because some participants with suicidal ideation had no history of suicide attempt (categorized as ‘non-suicidal attempt’). The severity of suicidal risk was measured by both the MINI-Suicidality Scale28 and SSI29. The severity of depression and anxiety was measured using the 17-item HAM-D25 and the Hamilton Anxiety Rating Scale (HAM-A)30. In addition, the Mood Disorder Questionnaire (MDQ)31 was used to detect symptoms of bipolarity in depressed patients32. The SSI, HAM-D, and HAM-A were administered by a single trained rater at baseline, after 1 month, and after 3 months.
Image acquisition
Structural images of the brain were acquired from all 48 patients and 25 healthy subjects at the Samsung Medical Center using the same 3.0-T MRI scanner (Philips 3.0 T Achieva) within 1 week after the baseline visit. T1-weighted MRI data were recorded using the following imaging parameters: 1-mm sagittal slice thickness, over contiguous slices with 50% overlap, no gap, repetition time (TR) of 9.9 ms, echo time (TE) of 4.6 ms, flip angle of 8°, and matrix size of 240 × 240 pixels. Images were reconstructed to 480 × 480 over a 240-mm field of view.
Image processing
To construct surface meshes of subcortical structures, the T1 images were processed to obtain anatomical parcellations using the FreeSurfer software package (version 5.1.0, http://surfer.nmr.mgh.harvard.edu). After parcellation, the labeled images were transformed to the native anatomical space of the input MR data. The subcortical surface meshes were then extracted from the labeled images for each subject by employing a Laplacian-based surface modeling system33. Surface-based registration was achieved by adopting a previously developed method to establish the vertex correspondence of subcortical surface meshes across all samples34. For given vertices on a subcortical surface mesh, we measured local shape volume (LSV), employing the method proposed by Shapira et al.35,36,37. By definition, the LSV measures the amount of local shape volume at each vertex, which can be used to analyze surface-based atrophy of subcortical structures. Each subcortical structure was composed of 2,562 vertices.
Statistical analysis
Clinical and demographic profiles are presented as categorical variables and continuous variables, as appropriate. Categorical variables included frequencies and proportions. Continuous variables included mean ± standard deviation (SD) or median and interquartile range. Depending on the normality of the distribution, Student t tests, one-way ANOVAs, Wilcoxon rank-sum tests, or Kruskal-Wallis tests were used.
To compare the local shape volumes of subcortical structures among the three groups, we used permutation-based ANCOVA, controlling for the effects of age, sex, level of education38, and intracranial volume (ICV)39. We re-populated the datasets N-1 times by random re-assignment (permutation) of all subjects into one of the three groups, where N is the number of permutations. We computed F-values for the original dataset and N-1 permuted sets through a simple ANCOVA to form a null distribution of group difference. Then we estimated the significance level of group difference as the fraction of the occurrences whose F-values were not less than the F-value of the original dataset. We used 5,000 as N. We also performed pairwise comparisons for the three groups using permutation-based ANCOVA and the False Discovery Rate (FDR) procedure.
We further performed the correlation test between clinical measurements and the LSV of each subcortical structure. Since the LSV often does not follow a normal distribution, we used Spearman partial correlation to control for the effects of age, sex, level of education, and ICV. For multiple comparison correction, we used cluster-based statistics40.
Results
Demographic results
Table 1 summarizes the demographic and clinical characteristics of the participants. Forty-eight had moderate to severe depression based on an initial median HAM-D score of 19. Eight of the 13 (33.3%) patients in the MDD group with suicidal ideation had a history of previous suicide attempts. Patients with suicidal ideation had much higher suicidal risk scores as measured by the MINI Suicidality Scale than patients without suicidal ideation, and six patients without suicidal ideation had a suicidality score of 1. The median score of the MINI suicidality scale was 3.5 in all MDD patients. Patients with suicidal ideation had more previous suicide attempts and higher SSI scores than patients without suicidal ideation. There was no significant difference in gender, age, education, number of episodes of MDD, duration of current episode, BIS score, HAM-A score, HAM-D score, and MDQ score between the patient groups. There was also no significant difference in demographic profiles between the two depressive groups and the healthy control group.
LSV differences in the between-group comparisons
Differences in the LSV between MDD patients with or without suicidal ideation using permutation-based ANCOVA are presented in Table 2. Twelve local regions in the subcortical hemispheres showed differences between the two groups, including the left and right amygdala, caudate, hippocampus, pallidum, putamen, and thalamus. Comparison of the LSV between MDD patients with or without suicidal attempt is presented in Table 3. As shown in Tables 2 and 3, the local regions that showed a difference in LSV with the presence of suicidal ideation partially corresponded to the regions that showed a difference in LSV with the presence of suicidal attempt except both amygdala and pallidum Both amygdala and pallidum showed no difference in LSV with the presence of suicidal attempt. However, these regions showed no significant association with MDD accompanying suicidal ideation after post hoc analysis (covariates of age, sex, ICV, and years of education).
Independent of suicidal risk, an LSV comparison between the MDD patients and healthy participants is presented in Table 2. Compared with the healthy participants, MDD patients showed significantly different right and left putamen volumes. Among these regions, only the bilateral putamen showed significant volume differences between the MDD patients and normal participants.
Correlations between LSV and clinical measurements
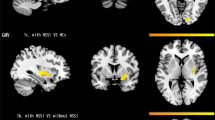
Local regions that showed significant correlations with severity of suicidal ideation and impulsivity are presented in Fig. 1 and Table 4. Both thalamus volumes were positively correlated with non-planning impulsivity and lack of future planning and forethought. Both hippocampi were positively correlated with attentional impulsivity, while the volume of the right hippocampus was positively correlated with motor impulsivity, the tendency to act without thinking. The left hippocampus, right caudate, and right pallidum were positively correlated with total impulsivity (Fig. 1A). Interestingly, regions correlated with non-planning impulsivity, motor impulsivity, attentional impulsivity, and total impulsivity were observed with no overlap, except the left hippocampus and right caudate. The left hippocampus volume showed opposite directional correlation with attentional impulsivity and total impulsivity in MDD patients with and without suicidal ideation. The right caudate showed the same directional correlation with total impulsivity in both groups of MDD patients with and without suicidal ideation. The LSV of the left pallidum showed a positive correlation with severity of suicidal risk in MDD patients with suicidal ideation (Fig. 1B). It also showed a negative correlation with severity of suicidal risk in MDD patients without suicidal ideation. However, these regional volumes were not significantly different between MDD patients with or without suicidal ideation after post-hoc analysis.

Subcortical structures associated with impulsivity and suicidal ideation. (A,B) Subcortical structures associated with total impulsivity and structures associated with severity of suicidal ideation are depicted in A and B with negative correlation represented as blue color and positive correlation represented as red color.
In the MDD group, irrespective of the presence of suicidal ideation, the left putamen and right thalamus were positively correlated with non-planning impulsivity. The right caudate was positively correlated with motor impulsivity in the same group. Considering the results from group comparisons between the MDD and normal participants, the correlation between the LSV of the left putamen and non-planning impulsivity was significant. Subcortical structures including the left thalamus, right amygdala, right putamen, and right pallidum showed no significant correlation with depression severity in the MDD group. However, the right amygdala and right putamen were positively correlated with depression severity in MDD patients with suicidal ideation and inversely correlated with depression severity in MDD patients without suicidal ideation. The left thalamus showed a significant negative correlation with depression severity in MDD patients without suicidal ideation.
Discussion
Our study showed distinct LSV differences between brain regions correlated with the presence of MDD and of suicidal ideation. There was no significant difference in LSV between MDD patients with or without suicidal ideation. Likewise, there was no significant LSV difference between MDD patients with or without suicidal attempt, defined as a self-injury history within 1 month or a previous lifetime suicide attempt. Although a significant group difference was not observed in total subcortical volume, subcortical volumes of specific regions, including the left pallidum, were correlated with suicidal risk severity in MDD patients with suicidal ideation. This directional correlation was positive in the group of participants with suicidal ideation and negative in the group without suicidal ideation. Left hippocampal volume also showed a positive correlation with attentional impulsivity in the group of participants with suicidal ideation and a negative correlation in participants without suicidal ideation.
Our findings agree with a recent meta-analysis that reported no significant differences for any regional brain volume measures between MDD patients with or without suicidal symptoms16. The negative correlation between LSV and suicidal ideation may be explained by different components of suicidal risk, including impulsivity, hopelessness, and dysfunction in cognitive flexibility, originating from different brain structures. The small sample size of the current study could also have affected the results. Nonetheless, the finding of differences in the shape of the left pallidum in relation to suicidal ideation may have clinical relevance, if we consider suicidal risk as a continuum. Regions that differed between groups with and without suicidal ideation mostly corresponded to the same regions that differed between groups with and without suicidal attempt except both amygdala and pallidus. This finding supports the validity of previous work relating suicidal ideation to suicidal attempts with negative finding on participants with suicidal attempt especially in amygdala and pallidus41,42. Numerous studies have reported the complexity of suicidal risk43, in which suicidal ideation and behaviors are transdiagnostic phenomena that can present without distinct diagnosable mental disorders44,45. The globus pallidus has been reported to contribute to abnormal temperament, supported by the structural links between parts of the globus pallidus and the reward circuits of the ventral striatum46. Among heterogenous suicidal subtypes that reflect various patterns of suicidal thinking and stress responsivity47,48, there are consistent findings supporting the importance of the globus pallidus. Recent findings from an animal study49 demonstrated the crucial role of the pallidum in top-down control of the cortico-striato-thalamo-cortical circuit to influence perception, attention, and emotion at downstream cortical levels. Thus, even there is limitation to interpret this finding connected to features related to suicidal attempt due to its low sample size, function of top-down control in pallidum would have been correlated to suicidal ideation which lost its correlation after one’s behavior realization through suicidal attempt. However, this study mainly focused on comparison between MDD with suicidal ideation and without, whether than MDD with suicidal attempt and without, which could have lack of evidence to support actual progress from ideation to attempt. There are some of researches reporting volume change of pallidus in suicidal attempt. Increased delay discounting was found to be related to suicide attempts that were poorly planned, of low-lethality, and repetitive. Increased delay discounting was also comorbid with substance use disorders. This behavioral tendency was explained by altered integrity of the basal ganglia50,51,52 and decreased pallidum volume in those attempting suicide17. A positive correlation in the left lateralized pallidum with suicidal risk is supported by left lateralization of activity related to cognitive processing53. An asymmetric model has also been studied in relation to impulsivity54. Increased volume of the right caudate was correlated with increased total impulsivity, consistent with previous findings. The caudate is primarily associated with impulsive, stimulation-seeking features and is observed to contribute to poor decision-making55. Considering the pathway supporting adaptive cognitive control, projecting from the anterior cingulate cortex to the striatum and caudate, the same directional correlation observed with total impulsivity in MDD patients with and without suicidal ideation can be understood56. We also found that hippocampal volume was correlated with attentional impulsivity, and with left laterality in total impulsivity, consistent with recent research57. The relationship between left lateralization and cognitive processing also supports the inverse directional correlations of the left hippocampus between MDD patients with and without suicidal ideation in attentional impulsivity and total impulsivity. Considering the subdomains of impulsivity, a positive correlation with both the thalamus and non-planning impulsivity is in line with previous findings showing a correlation between risk taking and activity in subcortical regions58. Likewise, the directional correlation between motor impulsivity and reduced right hippocampal volume is in line with a previous report, showing that dysfunction in this region59,60 impacts hyperactivity and impulsivity61. However, careful interpretation is needed because our study was not designed to assess asymmetry or altered basal ganglia-thalamo-cortical structure in impulsivity.
Impairment in subcortical structures could facilitate depressive symptoms accompanied by dysfunctional cognitive processes such as poor impulse control. Suicidal ideation with increased intensity could be derived from a combination of depression severity and impulsivity. Top-down control from the pallidus and amygdala which showed volume difference with presence of suicidal ideation could be diminished after realization of suicidal attempt, represented with no difference. Altered paralimbic reward signals and impulsivity with carelessness have been suggested to facilitate unplanned suicidal acts through a disruptive process in the cortico-striato-thalamic circuits50. As a result, these findings might suggest that suicidal attempt derived from suicidal ideation can be provoked by reduced motivational control over intentional behavioral reactions to salient negative stimuli in depression62. However, limited sample size on participants with suicidal ideation but no history of suicidal attempt and on participants with suicidal ideation with suicidal attempt history, we should be careful to infer these theses. Altered activity in the hippocampal-basal ganglia-midbrain circuit during the salience process has been reported to be correlated with severity of abnormal belief 63. Problems related to decision-making and ruminative brooding associated with the salience network are also reported to contribute to suicidal ideation64. In the current study, both putamens were demonstrated to show volume changes in MDD. This might reflect deficits in the reward circuit in MDD, which is consistent with recent findings65,66. A positive correlation between the right caudate and motor impulsivity in MDD patients and a positive correlation between the left putamen and non-planning impulsivity in MDD patients are consistent with previous reports showing that diminished reward sensitivity is associated with volumetric and functional changes in the nucleus accumbens in MDD67,68,69. Our findings of right laterality in the caudate nucleus and left laterality in the putamen are also in line with previous research66,70. Our finding that the left putamen showed significant differences in volume between MDD patients and healthy controls is consistent with recent findings showing that this relationship remains even when controlling for participant age or subtype of depression66,71. The lack of a significant difference in caudate volume in MDD patients may have occurred because we excluded cognitively impaired participants, as previous studies have shown an association between smaller caudates and cognitive impairment and dementia72. Complete discordance in local volume differences between MDD patients and healthy controls, and volume differences between participants with and without suicidal ideation, agree with previous reports12,14.
This study had several limitations. The relatively small number of participants limits the generalizability of the findings. Because we used a cross-sectional design, it was not possible to determine the causal relationships among regional volume changes in MDD patients with suicidal ideation. Despite these limitations, the present study identified differences in regional brain volumes with clinical correlation between participants with or without suicidal ideation in MDD. In addition, corresponding brain regions except amygdala and pallidus differed between MDD patients with or without suicidal ideation also differed between MDD patients with or without suicidal attempt. A strength of this study was the determination of the impact of depression on structural volume between MDD patients with or without suicidal ideation. Although significant group differences were not found in simple group comparisons, a positive correlation between severity of suicidal ideation and impulsivity in structures related to decision-making and reward processes provides evidence for neurobiological markers of suicidal risk in MDD. Thus, consistent with a previous report, the combination of depression with impulsivity related to decision making and the reward process could facilitate suicidal ideation and lead to suicidal attempt73. Further study is necessary to elaborate on these findings and to investigate suicide related behavior as a continuum in a transdiagnostic approach. Identification of MDD subjects at particular risk for suicidal ideation and behavior may guide clinicians to use adjunctive psychotherapeutic strategies such as acceptance and commitment therapy, aimed specifically at reducing suicide risk74.
References
Haagsma, J. A. et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj Prev 22, 3–18, https://doi.org/10.1136/injuryprev-2015-041616 (2016).
Jeon, H. J. et al. Unplanned versus planned suicide attempters, precipitants, methods, and an association with mental disorders in a Korea-based community sample. J Affect Disord 127, 274–280, https://doi.org/10.1016/j.jad.2010.05.027 (2010).
Jeon, H. J. et al. Lifetime prevalence and correlates of suicidal ideation, plan, and single and multiple attempts in a Korean nationwide study. J Nerv Ment Dis 198, 643–646, https://doi.org/10.1097/NMD.0b013e3181ef3ecf (2010).
Bertolote, J. M. & Fleischmann, A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry 1, 181–185 (2002).
Sveticic, J. & De Leo, D. The hypothesis of a continuum in suicidality: a discussion on its validity and practical implications. Ment Illn 4, e15, https://doi.org/10.4081/mi.2012.e15 (2012).
Nock, M. K. et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 192, 98–105, https://doi.org/10.1192/bjp.bp.107.040113 (2008).
Bertolote, J. M. et al. Suicide attempts, plans, and ideation in culturally diverse sites: the WHO SUPRE-MISS community survey. Psychol Med 35, 1457–1465, https://doi.org/10.1017/S0033291705005404 (2005).
Nock, M. K. et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry 70, 300–310, https://doi.org/10.1001/2013.jamapsychiatry.55 (2013).
Borges, G., Angst, J., Nock, M. K., Ruscio, A. M. & Kessler, R. C. Risk factors for the incidence and persistence of suicide-related outcomes: a 10-year follow-up study using the National Comorbidity Surveys. J Affect Disord 105, 25–33, https://doi.org/10.1016/j.jad.2007.01.036 (2008).
Ribeiro, J. D. et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med 46, 225–236, https://doi.org/10.1017/S0033291715001804 (2016).
Prinstein, M. J. et al. Longitudinal trajectories and predictors of adolescent suicidal ideation and attempts following inpatient hospitalization. J Consult Clin Psychol 76, 92–103, https://doi.org/10.1037/0022-006X.76.1.92 (2008).
Kim, K. et al. Reduced orbitofrontal-thalamic functional connectivity related to suicidal ideation in patients with major depressive disorder. Sci Rep 7, 15772, https://doi.org/10.1038/s41598-017-15926-0 (2017).
Kang, S. G. et al. Resting-state functional connectivity of the amygdala in suicide attempters with major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry 77, 222–227, https://doi.org/10.1016/j.pnpbp.2017.04.029 (2017).
Myung, W. et al. Reduced frontal-subcortical white matter connectivity in association with suicidal ideation in major depressive disorder. Transl Psychiatry 6, e835, https://doi.org/10.1038/tp.2016.110 (2016).
Wagner, G. et al. Structural brain alterations in patients with major depressive disorder and high risk for suicide: evidence for a distinct neurobiological entity? Neuroimage 54, 1607–1614, https://doi.org/10.1016/j.neuroimage.2010.08.082 (2011).
Renteria, M. E. et al. Subcortical brain structure and suicidal behaviour in major depressive disorder: a meta-analysis from the ENIGMA-MDD working group. Transl Psychiatry 7, e1116, https://doi.org/10.1038/tp.2017.84 (2017).
Vang, F. J., Ryding, E., Traskman-Bendz, L., van Westen, D. & Lindstrom, M. B. Size of basal ganglia in suicide attempters, and its association with temperament and serotonin transporter density. Psychiatry Res 183, 177–179, https://doi.org/10.1016/j.pscychresns.2010.05.007 (2010).
Gosnell, S. N. et al. Prefrontal cortex, temporal cortex, and hippocampus volume are affected in suicidal psychiatric patients. Psychiatry Res Neuroimaging 256, 50–56, https://doi.org/10.1016/j.pscychresns.2016.09.005 (2016).
Monkul, E. S. et al. Fronto-limbic brain structures in suicidal and non-suicidal female patients with major depressive disorder. Mol Psychiatry 12, 360–366, https://doi.org/10.1038/sj.mp.4001919 (2007).
Dumais, A. et al. Risk factors for suicide completion in major depression: a case-control study of impulsive and aggressive behaviors in men. Am J Psychiatry 162, 2116–2124, https://doi.org/10.1176/appi.ajp.162.11.2116 (2005).
Dombrovski, A. Y. & Hallquist, M. N. The decision neuroscience perspective on suicidal behavior: evidence and hypotheses. Curr Opin Psychiatry 30, 7–14, https://doi.org/10.1097/YCO.0000000000000297 (2017).
Kim, H. et al. Monoamine transporter gene polymorphisms and antidepressant response in koreans with late-life depression. JAMA 296, 1609–1618, https://doi.org/10.1001/jama.296.13.1609 (2006).
Association., A. P. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR®. 4th edition edn, (American Psychiatric Association, 2000).
van Vliet, I. M. & de Beurs, E. The MINI-International Neuropsychiatric Interview. A brief structured diagnostic psychiatric interview for DSM-IV en ICD-10 psychiatric disorders. Tijdschr Psychiatr 49, 393–397 (2007).
Hamilton, M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol 6, 278–296 (1967).
Park, S. W. et al. Development of the Suicide Risk Scale for Medical Inpatients. J Korean Med Sci 33, e18, https://doi.org/10.3346/jkms.2018.33.e18 (2018).
Kwon, H. L. A. J.-H. Validation for the Beck Scale for Suicide Ideation with Korean University Students. Korean Journal of Clinical Psychology 28, 1155–1172 (2009).
Roaldset, J. O., Linaker, O. M. & Bjorkly, S. Predictive validity of the MINI suicidal scale for self-harm in acute psychiatry: a prospective study of the first year after discharge. Arch Suicide Res 16, 287–302, https://doi.org/10.1080/13811118.2013.722052 (2012).
Beck, A. T., Kovacs, M. & Weissman, A. Assessment of suicidal intention: the Scale for Suicide Ideation. J Consult Clin Psychol 47, 343–352 (1979).
Hamilton, M. The assessment of anxiety states by rating. Br J Med Psychol 32, 50–55 (1959).
Hirschfeld, R. M. et al. Development and validation of a screening instrument for bipolar spectrum disorder: the Mood Disorder Questionnaire. Am J Psychiatry 157, 1873–1875, https://doi.org/10.1176/appi.ajp.157.11.1873 (2000).
Angst, J. et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord 88, 217–233, https://doi.org/10.1016/j.jad.2005.05.011 (2005).
Cho, Y., Seong, J. K., Jeong, Y., Shin, S. Y. & Alzheimer’s Disease Neuroimaging, I. Individual subject classification for Alzheimer’s disease based on incremental learning using a spatial frequency representation of cortical thickness data. Neuroimage 59, 2217–2230, https://doi.org/10.1016/j.neuroimage.2011.09.085 (2012).
Cho, H. et al. Changes in subcortical structures in early- versus late-onset Alzheimer’s disease. Neurobiol Aging 34, 1740–1747, https://doi.org/10.1016/j.neurobiolaging.2013.01.001 (2013).
Chung, S. J. et al. Subcortical shape analysis of progressive mild cognitive impairment in Parkinson’s disease. Mov Disord 32, 1447–1456, https://doi.org/10.1002/mds.27106 (2017).
Shapira, L., Shamir, A. & Cohen-Or, D. Consistent mesh partitioning and skeletonisation using the shape diameter function. The Visual Computer, 249–259, https://doi.org/10.1007/s00371-007-0197-5 (2008).
Koo, D. L., Shin, J. H., Lim, J. S., Seong, J. K. & Joo, E. Y. Changes in subcortical shape and cognitive function in patients with chronic insomnia. Sleep Med 35, 23–26, https://doi.org/10.1016/j.sleep.2017.04.002 (2017).
Boller, B., Mellah, S., Ducharme-Laliberte, G. & Belleville, S. Relationships between years of education, regional grey matter volumes, and working memory-related brain activity in healthy older adults. Brain Imaging Behav 11, 304–317, https://doi.org/10.1007/s11682-016-9621-7 (2017).
Jovicich, J. et al. MRI-derived measurements of human subcortical, ventricular and intracranial brain volumes: Reliability effects of scan sessions, acquisition sequences, data analyses, scanner upgrade, scanner vendors and field strengths. Neuroimage 46, 177–192, https://doi.org/10.1016/j.neuroimage.2009.02.010 (2009).
Han, C. E., Yoo, S. W., Seo, S. W., Na, D. L. & Seong, J. K. Cluster-based statistics for brain connectivity in correlation with behavioral measures. PLoS One 8, e72332, https://doi.org/10.1371/journal.pone.0072332 (2013).
Bielau, H. et al. Volumetric analysis of the hypothalamus, amygdala and hippocampus in non-suicidal and suicidal mood disorder patients–a post-mortem study. CNS Neurol Disord Drug Targets 12, 914–920 (2013).
Gifuni, A. J. et al. Subcortical nuclei volumes in suicidal behavior: nucleus accumbens may modulate the lethality of acts. Brain Imaging Behav 10, 96–104, https://doi.org/10.1007/s11682-015-9369-5 (2016).
Bernanke, J. A., Stanley, B. H. & Oquendo, M. A. Toward fine-grained phenotyping of suicidal behavior: the role of suicidal subtypes. Mol Psychiatry 22, 1080–1081, https://doi.org/10.1038/mp.2017.123 (2017).
Oquendo, M. A. & Baca-Garcia, E. Suicidal behavior disorder as a diagnostic entity in the DSM-5 classification system: advantages outweigh limitations. World Psychiatry 13, 128–130, https://doi.org/10.1002/wps.20116 (2014).
Oquendo, M. A., Baca-Garcia, E., Mann, J. J. & Giner, J. Issues for DSM-V: suicidal behavior as a separate diagnosis on a separate axis. Am J Psychiatry 165, 1383–1384, https://doi.org/10.1176/appi.ajp.2008.08020281 (2008).
Haber, S. N. & Knutson, B. The reward circuit: linking primate anatomy and human imaging. Neuropsychopharmacology 35, 4–26, https://doi.org/10.1038/npp.2009.129 (2010).
Witte, T. K., Fitzpatrick, K. K., Warren, K. L., Schatschneider, C. & Schmidt, N. B. Naturalistic evaluation of suicidal ideation: variability and relation to attempt status. Behav Res Ther 44, 1029–1040, https://doi.org/10.1016/j.brat.2005.08.004 (2006).
Miranda, R., Ortin, A., Scott, M. & Shaffer, D. Characteristics of suicidal ideation that predict the transition to future suicide attempts in adolescents. J Child Psychol Psychiatry 55, 1288–1296, https://doi.org/10.1111/jcpp.12245 (2014).
Board of Directors Meeting, April 1, 2016, Nashville, Tennessee. Am J Pharm Educ 80, S14, https://doi.org/10.5688/ajpe808S14 (2016).
Dombrovski, A. Y., Szanto, K., Clark, L., Reynolds, C. F. & Siegle, G. J. Reward signals, attempted suicide, and impulsivity in late-life depression. JAMA Psychiatry 70, 1, https://doi.org/10.1001/jamapsychiatry.2013.75 (2013).
Voon, V. et al. A multicentre study on suicide outcomes following subthalamic stimulation for Parkinson’s disease. Brain 131, 2720–2728, https://doi.org/10.1093/brain/awn214 (2008).
Dombrovski, A. Y. et al. The temptation of suicide: striatal gray matter, discounting of delayed rewards, and suicide attempts in late-life depression. Psychol Med 42, 1203–1215, https://doi.org/10.1017/S0033291711002133 (2012).
Bockova, M. et al. Oscillatory reactivity to effortful cognitive processing in the subthalamic nucleus and internal pallidum: a depth electrode EEG study. J Neural Transm (Vienna) 124, 841–852, https://doi.org/10.1007/s00702-017-1719-6 (2017).
Neal, L. B. & Gable, P. A. Neurophysiological markers of multiple facets of impulsivity. Biol Psychol 115, 64–68, https://doi.org/10.1016/j.biopsycho.2016.01.006 (2016).
Glenn, A. L., Raine, A., Yaralian, P. S. & Yang, Y. Increased volume of the striatum in psychopathic individuals. Biol Psychiatry 67, 52–58, https://doi.org/10.1016/j.biopsych.2009.06.018 (2010).
Shackman, A. J. et al. The integration of negative affect, pain and cognitive control in the cingulate cortex. Nat Rev Neurosci 12, 154–167, https://doi.org/10.1038/nrn2994 (2011).
Onnink, A. M. et al. Brain alterations in adult ADHD: effects of gender, treatment and comorbid depression. Eur Neuropsychopharmacol 24, 397–409, https://doi.org/10.1016/j.euroneuro.2013.11.011 (2014).
Panwar, K. et al. Differential associations between impulsivity and risk-taking and brain activations underlying working memory in adolescents. Addict Behav 39, 1606–1621, https://doi.org/10.1016/j.addbeh.2013.12.007 (2014).
Ahmadi, A. et al. Influence of alcohol use on neural response to Go/No-Go task in college drinkers. Neuropsychopharmacology 38, 2197–2208, https://doi.org/10.1038/npp.2013.119 (2013).
Markovic, V. et al. Role of habenula and amygdala dysfunction in Parkinson disease patients with punding. Neurology 88, 2207–2215, https://doi.org/10.1212/WNL.0000000000004012 (2017).
Miguel, P. M. et al. Neonatal hypoxia-ischemia induces attention-deficit hyperactivity disorder-like behavior in rats. Behav Neurosci 129, 309–320, https://doi.org/10.1037/bne0000063 (2015).
van Heeringen, K., Bijttebier, S., Desmyter, S., Vervaet, M. & Baeken, C. Is there a neuroanatomical basis of the vulnerability to suicidal behavior? A coordinate-based meta-analysis of structural and functional MRI studies. Front Hum Neurosci 8, 824, https://doi.org/10.3389/fnhum.2014.00824 (2014).
Choi, M. J. et al. Disease burden of hospitalized community-acquired pneumonia in South Korea: Analysis based on age and underlying medical conditions. Medicine (Baltimore) 96, e8429, https://doi.org/10.1097/MD.0000000000008429 (2017).
Ordaz, S. J., Goyer, M. S., Ho, T. C., Singh, M. K. & Gotlib, I. H. Network basis of suicidal ideation in depressed adolescents. J Affect Disord 226, 92–99, https://doi.org/10.1016/j.jad.2017.09.021 (2018).
Sexton, C. E., Mackay, C. E. & Ebmeier, K. P. A systematic review and meta-analysis of magnetic resonance imaging studies in late-life depression. Am J Geriatr Psychiatry 21, 184–195, https://doi.org/10.1016/j.jagp.2012.10.019 (2013).
Sachs-Ericsson, N. J. et al. Putamen Volume Differences Among Older Adults: Depression Status, Melancholia, and Age. J Geriatr Psychiatry Neurol 31, 39–49, https://doi.org/10.1177/0891988717747049 (2018).
Nestler, E. J. Role of the Brain’s Reward Circuitry in Depression: Transcriptional Mechanisms. Int Rev Neurobiol 124, 151–170, https://doi.org/10.1016/bs.irn.2015.07.003 (2015).
Russo, S. J. & Nestler, E. J. The brain reward circuitry in mood disorders. Nat Rev Neurosci 14, 609–625, https://doi.org/10.1038/nrn3381 (2013).
Lu, Y. et al. The volumetric and shape changes of the putamen and thalamus in first episode, untreated major depressive disorder. Neuroimage Clin 11, 658–666, https://doi.org/10.1016/j.nicl.2016.04.008 (2016).
Hannestad, J. et al. White matter lesion volumes and caudate volumes in late-life depression. Int J Geriatr Psychiatry 21, 1193–1198, https://doi.org/10.1002/gps.1640 (2006).
Schmaal, L. et al. Subcortical brain alterations in major depressive disorder: findings from the ENIGMA Major Depressive Disorder working group. Mol Psychiatry 21, 806–812, https://doi.org/10.1038/mp.2015.69 (2016).
Bauer, E., Toepper, M., Gebhardt, H., Gallhofer, B. & Sammer, G. The significance of caudate volume for age-related associative memory decline. Brain Res 1622, 137–148, https://doi.org/10.1016/j.brainres.2015.06.026 (2015).
Turecki, G. The molecular bases of the suicidal brain. Nat Rev Neurosci 15, 802–816, https://doi.org/10.1038/nrn3839 (2014).
Ducasse, D. et al. Acceptance and Commitment Therapy for the Management of Suicidal Patients: A Randomized Controlled Trial. Psychother Psychosom 87, 211–222, https://doi.org/10.1159/000488715 (2018).
Acknowledgements
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (No. 2011-0013064), by the Original Technology Research Program for Brain Science through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (No. NRF-2016M3C7A1947307; PI HJJ), by the Bio & Medical Technology Development Program of the NRF funded by the Korean government, MSIP (No. NRF-2017M3A9F1027323; PI HJJ), and by the Original Technology Research Program for Brain Science through the National Research Foundation of Korea(NRF) funded by the Ministry of Science and ICT, and Future Planning (2015M3C7A1029034). The Korean Ministry of Health & Welfare and the National Research Foundation of Korea had no role in study design; in the collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
J.H.J. and S.J.K. had full access to all study data and take responsibility for its integrity and the accuracy of the data analysis. J.H.J. was the principal investigator of this study. Study concept and design: J.H.J., S.J.K., K.K.W., S.J.H., and M.W.J. Data acquisition: J.H.J., S.S.W., and K.K.W. Analysis of imaging data and interpretation: S.J.K. and S.J.H. Statistical analysis: K.K.W., S.J.H., C.K.W., and M.W.J. Preparation of the manuscript: J.H.J., S.J.K., K.K.W., S.J.H., and M.W.J. Interpretation of the data and critical revision of the manuscript for important intellectual content: M.F., D.M., G.P., S.S.W., and N.E.J.
Corresponding authors
Ethics declarations
Competing Interests
Dr. Mischoulon has received research support from Nordic Naturals. He has served as an unpaid consultant for Pharmavite LLC and Gnosis USA, Inc. He has received honoraria for speaking at the Massachusetts General Hospital Psychiatry Academy, Blackmores, and PeerPoint Medical Education Institute, LLC. He has received royalties from Lippincott Williams & Wilkins for the published book “Natural Medications for Psychiatric Disorders: Considering the Alternatives”. The other authors declare no potential competing interests with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, K., Shin, JH., Myung, W. et al. Deformities of the Globus Pallidus are Associated with Severity of Suicidal Ideation and Impulsivity in Patients with Major Depressive Disorder. Sci Rep 9, 7462 (2019). https://doi.org/10.1038/s41598-019-43882-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43882-4
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
