
Abstract
Attention deficits due to auditory distractibility are pervasive among patients with acquired brain injury (ABI). It remains unclear, however, whether attention deficits following ABI specific to auditory modality are associated with altered haemodynamic responses. Here, we examined cerebral haemodynamic changes using functional near-infrared spectroscopy combined with a topological vector-based analysis method. A total of thirty-seven participants (22 healthy adults, 15 patients with ABI) performed a melodic contour identification task (CIT) that simulates auditory distractibility. Findings demonstrated that the melodic CIT was able to detect auditory distractibility in patients with ABI. The rate-corrected score showed that the ABI group performed significantly worse than the non-ABI group in both CIT1 (target contour identification against environmental sounds) and CIT2 (target contour identification against target-like distraction). Phase-associated response intensity during the CITs was greater in the ABI group than in the non-ABI group. Moreover, there existed a significant interaction effect in the left dorsolateral prefrontal cortex (DLPFC) during CIT1 and CIT2. These findings indicated that stronger hemodynamic responses involving oxygen exchange in the left DLPFC can serve as a biomarker for evaluating and monitoring auditory distractibility, which could potentially lead to the discovery of the underlying mechanism that causes auditory attention deficits in patients with ABI.
Similar content being viewed by others

Introduction
Acquired brain injury (ABI) is damage to the brain that occurs due to certain events after birth1, including a traumatic injury to brain tissues as a result of an external mechanical force2 and/or stroke, which is an ischemic or hemorrhagic cerebrovascular accident3. These events result in permanent or temporary impairments in various functional behaviours, including movement, emotion, perception, and cognition4,5,6,7,8. Cognitive impairments are pervasive among patients with ABI with attention deficits being the most common9,10,11. Selective attention, in particular, is considerably affected in patients with ABI12,13,14 as they are more susceptible to distraction4,15,16,17.
Auditory attention seems more challenging than visual attention in patients with ABI18,19. For example, individuals with ABI are incapable of focusing their attention to relevant auditory information. They also have difficulty distinguishing target sounds from distracting sounds20, and this notion is supported by previous studies that have shown that attentional performance of ABI patients is decreased during auditory distraction21,22,23,24,25. Attenuated auditory processing is probably due to the complex nature of auditory environments, which requires the simultaneous processing of many features, such as locational, timbre, and semantic cues. This consequently affects higher cognitive functions, such as working memory and executive control26 leading to, among other things, such as difficulty with speech perception in noisy environments, which can have long-term negative socio-communicative consequences.
Various neurocognitive assessments are used to diagnose and identify cognitive impairments in patients with ABI (e.g., information processing speed, short-term, and long-term memory capacity27,28). Visual stimuli have been mostly employed in the tests, such as the Stroop Colour-Word test29, Trail Making Test A and B30 and Delis-Kaplan Executive Function System Colour-Word Interference Test31. Relatively less attention has been drawn to auditory modality. The previous studies focused on the sequential processing of auditory information32,33,34 by using auditory stimuli involving spoken words and/or numbers in their tasks [e.g., paced auditory serial addition test35, auditory Stroop test36, and digit span test37. Given that distractibility is a significant contributor to the attention deficits in patients with ABI15,16,17, the development of an auditory perception test is needed in order to simulate situations requiring selective attention against simultaneous distraction.
Musical scenes assimilate real-world auditory environments in which more than two sounds streams are present. According to Bigand et al.38 listening to two or more concurrent music streams (e.g., a melody with harmonic accompaniment or two melodies) activates different types of attention, such as selective alternating and divided attention. One of the musical features, instrumental timbres, provides a perceptual cue that aids segregating multiple streams and focusing on a relevant one, such as in speech perception in noise39,40,41,42. Moreover, multi-voice music listening tasks activate neural regions involved in different types of attention43,44,45,46. The regions include the primary sensory cortices, superior temporal sulcus, and frontal and parietal regions, which are similarly activated in attention tasks using both musical and visual stimuli43,44,47,48,49.
Several studies have employed melodic contours to specifically show cognitive decline in patients with ABI and mild cognitive impairment50,51,52,53. Jeong and colleagues51,52 have developed a music-based attention assessment to evaluate attentional function in individuals with moderate to severe traumatic brain injury (TBI). Their primary findings52 showed that the melodic contour identification task (CIT) can be used with high reliability for healthy adults and patients with TBI. A follow-up study51 demonstrated the construct validity of four different factors of attention. Recently, cognitive loads across melodic CITs were examined using functional near-infrared spectroscopy (fNIRS) and demonstrated that as CIT difficulty increased, cognitive loads increased accordingly54. Collectively, these results suggest that the melodic CIT can simulate the different types and levels of auditory attention and, thus, can be used to evaluate attention deficits following brain injury.
In this study, we employed fNIRS combined with an advanced topological method to examine cerebral hemodynamic changes involving oxygen exchange during a music-cognition task. The cerebral hemodynamic response is one of the neuropathological indicators of ABI. ABI-specific changes are characterized by an imbalance between oxygen supply and consumption, which appears as hypoxia and cerebral ischemia55,56. Cerebral ischemia and hypoxia are prevalent secondary complications of ABI that are associated with poor outcome in ABI survivors57,58,59,60. Thus, indices associated with oxygen metabolism have been considered important for making region-specific assessments and planning effective rehabilitation according to the recovery phase58,61,62,63,64,65.
Although several studies have employed fNIRS to demonstrate its applicability and efficacy in monitoring hemodynamic responses66,67,68,69,70 and to examine cognitive alteration in patients with ABI, they have yielded mixed results71,72,73. During a target detection task, Merzagora et al.74 observed significantly decreases in oxygenated hemoglobin (HbO2) in ABI patients as compared with healthy adults. Similarly, Kontos et al.75 and Hashimoto et al.76 have reported large decreases or inactivation of HbO2 in the ABI group during a series of cognitive tasks (e.g. word memory, digit-symbol substitution, and working memory tests). Conversely, Hibino et al.77 found an overall enhancement of HbO2, specifically in the lateral and medial frontal regions, in patients with ABI.
The incongruence of these studies was possibly due to the use of a single hemodynamic index, namely HbO2, as this is insufficient to accurately explain the cognitive and neuropathological changes following ABI. Therefore, it is necessary to include multiple indices, such as the difference between oxygenated and deoxygenated haemoglobin, and total amount of haemoglobin concentration in order to investigate the dynamic relationship among them. The purpose of the study was to empirically demonstrate auditory distractibility of patients with ABI as evidenced by alteration in cerebral hemodynamic changes. We employed fNIRS combined with a topological vector-based analysis method to address the existing controversies in fNIRS studies. Furthermore, novel stimuli and tasks using music, namely melodic CITs were utilized to simulate distractibility in a real-world auditory environment.
Results
Behavioral Responses
Table 1 shows the mean performances on the CIT for accuracy and reaction time for the ABI and non-ABI groups. The mean accuracy in the non-ABI group was 75% for CIT1 and was followed by CIT2 (48.4%). Accuracy was lowest (40.4%) when attention shift was required between two concurrent melodic contours (CIT3). A similar trend was found across the CITs for the ABI group (decreasing from 61.5% to 21.5%), but accuracy declined considerably more between CIT1 and CIT2 than it did in the non-ABI group. Reaction time was not sensitive enough to reveal the difference between CIT1 and CIT2 for both the ABI and non-ABI groups. The mean response time in the ABI group was highest in CIT1, which was followed by CIT2 and CIT3. CIT1 and CIT2 did not differ statistically in pairwise post hoc analysis with Bonferroni correction (p < 0.05). However, this was not the case in the non-ABI group.
To illustrate the behavioral response trend, the RCS was calculated (Fig. 1), and a two-way mixed ANOVA [i.e. Group (ABI, non-ABI) × Task (CIT1, CIT2, and CIT3)] was performed. There was a significant main effect of Group [F(1,31) = 12.671, p < 0.01] and Task [F(2,62) = 35.643, p < 0.001], indicating that the overall performance was significantly better in the non-ABI group as compared with the ABI group and that performance worsened when the CIT was more difficult. In addition, the interaction between Group and Task was significant [F(2,62) = 4.146, p < 0.05]. The pairwise post hoc comparison using a Bonferroni correction revealed that the ABI group performed significantly better in CIT1 than in CIT2 (p < 0.05), while the non-ABI group did better in CIT1 than in CIT2 (p < 0.001) and in CIT2 than in CIT3 (p < 0.05). These findings indicated that CIT1 and CIT2 were able to detect between- and within-group differences. CIT3 was thus excluded in the following hemodynamic response analysis.

Changes in the rate-corrected score across CITs.
Hemodynamic Responses
Descriptive statistics showed that HbO2 was generally less active in the ABI group, which differed from previous findings (Hibino et al., 2013) (see SI Appendix, Table 1 for details). In addition, the changes in the HbO2-HHb patterns differed between the groups. Figure 2 is examples of changes in oxygenated haemoglobin (HbO2) and deoxygenated haemoglobin (HHb) data for the ABI and non-ABI groups. The sample data set showed that decreases in HHb and increases in HbO2 were observed in the non-ABI group, while both HHb and HbO2 changed in the same direction in the ABI group (See SI Appendix, Tables 2 and 3 for details). These findings confirmed that vector-based phase analyses of both HbO2 and HHb were effective.

Examples of changes in HbO2 and HHb in the six fNIRS channels.
With the vector-based phase analyses, we calculated ΔCOE, ΔCBV, angle k and scalar L and plotted the indices in a vector plan, which allowed for more insightful and efficient inspections of whether strong (or abnormal) oxygen metabolic demands were present (please see Methods for details). Figure 3 shows the relationship between oxygen demand and oxygen supply using k and L. The overall trend showed higher ΔCOEs in the ABI group than in the non-ABI group and lower ΔCBVs in the ABI group than in the non-ABI group. Generally, angle k tended to increase to 225° (phase 5) in the ABI group, while it decreased to −135° (phase 1) in the non-ABI group. The phasic information indicated that the non-ABI group was typically in phases 1 to 2 (hyperoxia/hyperemia and hyperoxia/ischemia, respectively), which indicated that the supply of HbO2 and total amount of blood were sufficient. However, the ABI group was in phases 4 to 5 (hypoxia/ischemia), which indicated that both the supply of HbO2 and total blood flow were insufficient. Exceptions were found in CH1 and CH2 only during the post-task when the cognitive demands were no longer present.

Trajectory of the vectors in the six fNIRS Channels.
To confirm the abnormalities in the oxygen metabolic demands, the four indices were converted to a PRI analysis (see SI Appendix, Table 4 for details). To standardize the differences in the individual values, we subtracted the mean value during the pre-task from the mean values during the on-task and post-task. A two-way mixed ANOVA was performed using Group (ABI, non-ABI) × Task (pre-task, on-task, post-task) for each of the six channels. The CIT1 results indicated a significant main effect of Group on the PRI at CH13 F(1,34) = 4.320, p < 0.05] and CH15 [F(1,34) = 4.920, p < 0.05] and a significant main effect of Task on the PRI at CH1 [F(2,68) = 4.830, p < 0.05], CH14 [F(2,68) = 3.348, p < 0.05] and CH15 [F(2,68) = 3.891, p < 0.05]. In addition, an interaction effect was found between Group and Task at CH15 [F(2,68) = 3.620, p < 0.05]. A post hoc comparison revealed that the PRI was higher during the on-task than the pre-task in the ABI group (p < 0.05). The CIT2 results indicated a significant main effect of Group on the PRI at CH13 [F(1,34) = 4.909, p < 0.05] and CH15 [F(1,34) = 6.270, p < 0.05] and a significant main effect of Task on the PRI at CH1 [F(2,68) = 4.496, p < 0.05], CH14 [F(2,68) = 3.387, p < 0.05] and CH15 [F(2,68) = 4.678, p < 0.05]. Most importantly, a significant interaction effect was found between group and task at CH15 [F(2,68) = 3.520, p < 0.05]. A post hoc comparison revealed that the PRI was higher during the on-task than the pre-task in the ABI group (p < 0.01).
These findings showed that the PRI values were significantly higher in the ABI group than in the non-ABI group, indicating a greater level of oxygen exchange in the ABI group and during CIT1 and CIT2. The PRIs were significantly higher in CIT1 and CIT2 than the baseline, indicating increases in oxygen exchange during CIT performance. In particular, these changes were more prominent in the left than right DLPFC.
Discussion
The present study attempted to use fNIRS technology in conjunction with a topological vector-based analysis method to assess cerebral hemodynamic changes underlying auditory dysfunctions in patients with ABI. Behavioral and hemodynamic responses were measured while individuals with ABI and without ABI performed melodic CITs. The RCS analysis showed that ABI-specific auditory distractibility was found in CIT1 and CIT2. In addition, cerebral hemodynamic changes during CIT1 and CIT2 showed a greater level of oxygen exchange in the ABI group than in the non-ABI group in the left DLPFC (i.e. CH13, and CH15). Altogether, the current findings were consistent between behavioral and hemodynamic findings, indicating that increased distractibility in ABI was possibly due to altered brain activity involving oxygen changes. The findings suggested that CIT1 and CIT2 can effectively demonstrate increases in auditory distractibility following ABI. A greater level of oxygen exchange in the left DLPFC is possibly a feature that underlies susceptibility to auditory distractibility and attention deficits following ABI. Furthermore, greater and, therefore, potentially abnormal oxygen exchanges in the region can serve as a biomarker to specifically detect auditory distractibility.
Our behavioral results showed that overall CIT performance was lower in patients with ABI than healthy adults. As the level of difficulty increased, CIT performance decreased. This trend was similar for both groups. The current findings are in line with the previous studies reporting worse performance in ABI than healthy control groups, and inadequate performances across various types of auditory attention in both patients with ABI and healthy controls21,22,78,79,80. Also, the findings were similar with our previous study54 reporting that younger and older adults showed a gradual decrease in performance accuracy across the different levels of CITs.
Interestingly, there existed a between-group difference. RCS scores between CIT1 and CIT2 were significantly different in both ABI and non-ABI group, while those between CIT2 and CIT3 were significant in the non-ABI group alone (Fig. 1). Considering that CIT1 and CIT2 required selective listening to target contours in the presence of distraction, our findings indicated that patients with ABI were susceptible to auditory distraction and their performance declined as the level of distraction increased (note that environmental sounds were used as distraction in CIT1, while target-like distracting sounds were used in CIT2). Our findings are supported by the concept of distractibility, which is considered key for leading to attention deficits in patients with ABI15,16,17. In actual fact, the declined performance in CIT1 and CIT2 (selective attention against auditory distraction) were similar to previous studies that compared and reported deficits in selective auditory attention in patients with ABI as compared to healthy controls21,22,78,79,80. An insignificant difference between CIT2 and CIT3 can be interpreted as a cognitive threshold existing in patients with ABI. Since CIT3 requires an ability to selectively attend to target contour presented by a specific instrument timbre and to shift the focus from one to another according to the visual cue given on the screen, it seems that this task involves higher-order cognition (i.e., mental flexibility) than that required in CIT2. The current findings were similar with our previous study54 that showed CIT2 is sensitive enough to detect a cognitive decline existing in elderly group compared to young adult group.
Our vector plane analysis showed that the non-ABI group fell into phases 1 to 2, while those in the ABI group mostly fell into phases 4 to 5 (see Fig. 2), which indicated that greater and, thus, potentially abnormal oxygen exchanges were required in the ABI group. More importantly, PRI analysis confirmed the trend statistically; the PRIs increased significantly more in the ABI group than in the non-ABI group in the left DLPFC (see Fig. 2, CH13 and CH15) while they performed the CIT1 and CIT2 (selective target contour identification against different types of auditory distraction). This result appeared to be due to the following: 1) increases in angle k, which meant ∆COE with decreased ∆CBV and 2) a longer scalar L, which was mainly attributed to total amount of changes in ∆COE and ∆CBV. That is, the greater oxygen exchanges in the patients with ABI as indicated by the hypoxia/ischemia phase was reflected both by high oxygen consumption (∆HHb > ∆HbO2) and a lack of sufficient oxygen supply (∆CBV < 0).
Because no studies have examined oxygen exchange (using PRI analysis) in patients with ABI in relation to their cognitive performance, we first compared our findings to a group of studies that examined cognitive loads and oxygen demands (i.e., actual and simulated driving situations) in healthy adults. Yoshino et al.81 found that oxygen metabolic demands varied with vehicle manipulation, that is to say, greater during deceleration as opposed to acceleration, and interpreted the demands that increased as an increase in the difficulty of a given task. Oka et al.82 reported a higher PRI value in the right than left premotor cortex during left curve driving, which indicated the occurrence of frequent oxygen exchanges possibly due to greater neural activities. Both studies implied that the driving tasks involving various contexts facilitated the usage of cognitive functions and changes in oxygen metabolism in the prefrontal regions. The previous findings are therefore in line with our findings that indicated that the cognitive demands associated with CITs lead to hemodynamic changes involving oxygen level exchange.
The current findings addressed previous mixed results reporting either hypo- or hyper-activation in oxygenated hemoglobin during cognitive task performance in patients with ABI75,83,84,85,86,87. Our findings in the HbO2-HHb pattern analyses confirmed the need for both indices in examining oxygen metabolism of patients with ABI (see Fig. 2 for the different activation patterns between HbO2 and HHb, which are distinctive between groups). Additional attempts to include oxygen-related multiple indices revealed the altered hemodynamic responses are ABI-specific (hypoxia and ischemia as indicated by HHb > HbO2 and CBV < 0)55,56.
Moreover, stronger oxygen metabolic demands observed in the ABI group can be interpreted as an impairment of cerebral oxygen exchange that acts as an underlying mechanism of susceptibility to auditory distraction and auditory attention deficits in patients with ABI. That is, insufficient oxygen supply due to dysfunctions in neuronal activation and connectivity caused high oxygen demands (i.e., ΔHHb is greater than ΔHbO2. These results are similar with previous findings reporting that healthy adults showed regional increases in HbO2 accompanied by HHb decreases. However, patients with cerebral ischemia or brain tumors have been reported to exhibit HHb increases together with HbO2 increases88,89,90,91. Since increasing tissue oxygenation is considered crucial in improving cognitive function for patients with ABI26,92,93,94 and TBI95,96,97, dysfunctions in oxygen metabolism can therefore underlie auditory cognitive impairment following ABI.
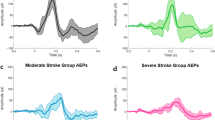
Our findings showed that the oxygen level exchange during CIT1 and CIT2 were prominent in the ABI group than in the non-ABI group in the left DLPFC (see Fig. 2, CHs 13 and 15 for PRI). This indicated that the left DLPFC was more sensitive to detect the oxygen metabolism-associated auditory dysfunction in the ABI group and, thus, can be used as a biomarker of auditory distractibility in ABI. Figure 4 shows stronger oxygen metabolic demands in the ABI than the non-ABI group and in the left than the right DLPFC. In general, the DLPFC controls higher-cognitive functions, such as working memory and executive control98,99,100. This region, also known as Brodmann area 46 (CH15 in the fNIRS data), receives information from the auditory cortex, and the stronger oxygen level exchange in the DLPFC is therefore likely to occur during the performance of a complex auditory task101,102,103,104, such as CIT1 and CIT2 that were used in our study.

Differences in oxygen metabolic demands between groups during (A) CIT1 and (B) CIT2.
In our behavioral findings, CIT2 performance significantly worsened compared with that of CIT1 indicating imposition of more cognitive loads. Although we did not find statistical significance, Fig. 4 clearly shows greater level of oxygen exchange in the left DLPFC in CIT2 than CIT1. This significant difference observed in the left DLPFC can be task specific as Jeong and Ryu (2016)105 reported prefrontal asymmetry in a timbre working memory task. Timbre is generally known as typically processed in the right hemisphere; however, when a timbre task is combined with a complex cognitive task, the left DLPFC can be dominantly activated. Timbre is one of the key factors in auditory scene analysis because it provides a perceptual clue of how one organizes perceived auditory surroundings106,107. When two people speak simultaneously, timbre cues aid in selectively attending to target information and higher-order cognitive processes, such as executive functioning that underlies goal-directed behavior, which is necessary in auditory scene analysis in concert with timbre discrimination108. In this study, we employed target melody detection utilizing timbre difference as a perceptual cue to differentiate a target during distraction. Unsurprisingly, the left DLPFC activation indicated the involvement of higher-order cognitive processing given by spatial timbre cues.
Conclusion
The present study aimed to examine cerebral hemodynamic changes in individuals with ABI during melodic contour identification task. We utilized fNIRS to monitor the hemodynamic activity in the prefrontal cortex and analysed the HbO2 and HHb related indices with a vector-based analysis method. Our behavioral findings revealed significant differences between the ABI and non-ABI groups in CIT1 and CIT2 (target contour identification against environmental sounds and target-like distraction). The level of oxygen exchange in the left DLPFC during CIT1 and CIT2 increased significantly in the patients with ABI. These findings together indicated that CIT is able to discern auditory distractibility in patients with ABI. Furthermore, more frequent oxygen exchange in the left DLPFC is a possible underlying mechanism that leads to auditory attention deficits in these patients. Our results suggest that oxygen metabolic demands during melodic CITs can provide a surrogate biomarker of auditory dysfunction in patients with ABI as a result of stroke or TBI.
The novel attempts of the current study mostly rested on the use of fNIRS combined with the vector-based analysis, which enabled to evaluate cerebral oxygen metabolism with an efficient index. This method provided a clear way to compare interrelationships among diverse indices, including ∆HbO2, ∆HHb, ΔCBV and ΔCOE on the same vector plane and to classify abnormalities in oxygen metabolism using the definitions of each of the eight phases81,82. We, however, recognize some limitations of this particular study. The fNIRS was devised to observe PFC activation alone, and therefore, connectivity with other deep brain regions or the possible influence of damaged brain areas has not been accounted for. We therefore cannot determine whether the cognitive deficits were solely associated with oxygen metabolism in the PFC. Instead, this study focused on cerebral activity involving oxygen level exchange during a non-verbal auditory assessment (note that musical non-verbal information processing is expected to be less knowledge- and culture-dependent), which could be more widely available for use.
An urgent future study would thus combine diffuse correlation spectroscopy or employ fMRI to examine a direct relationship between multiple hemodynamic indices of fNIRS combined with vector-based phase analysis and cerebral metabolic rate of oxygen (CMRO2). Future study can also consist of a scaled-up experiment that examines the relationship between music and cognitive function in real-world situations (e.g. simulated and scenario-based auditory assessments in augmented or virtual reality). Another type of future study could broaden the scope of applying CITs to more patients with cognitive impairments, including dementia and mild cognitive impairment, and compare the data with various types of neuroimaging data (e.g. fMRI) to specify the essence of music assessment.
Methods
Participants
This study was approved by the Institutional Review Board of Hanyang University (IRB No. HYUH 2013-08-017) and the National Rehabilitation Centre (IRB No. 2015-040). All participants have provided written informed consent in accordance with the Declaration of Helsinki. Thirty-seven participants (healthy adults = 22, patients with ABI = 15) participated in the study. The patients with ABI were voluntarily recruited from the National Rehabilitation Centre of South Korea. The patients were eligible if they showed cognitive impairment at least in one domain on a neuropsychological battery, the Seoul Neuropsychological Screening Battery II (SNSB-Second edition)109. Patients who had a less than three months of regular involvement in musical activities and/or professional training, who had a minimal ability to understand the spoken instruction, and who were without sensory impairments were eligible to participate in the study. The average age of the patients was 53.60 years (SD = 8.88), and an average of 19.44 months (SD = 33.28) had passed after their brain injuries. The patients’ average years of education were 14.47 years (SD = 2.28). The SI Appendix, Table 5 lists the characteristics of the patients.
The non-ABI group was voluntarily recruited by advertising on the electronic board of Hanyang University. The average age of the control group was 55.77 years (SD = 5.98), and the patients’ average years of education were 12.77 years (SD = 3.40). The control group did not have a neurological medical history and present with no sensory impairments. The groups did not differ significantly for either age or education level [t(35) = 0.8655, non-significant; t(35) = −1.644, non-significant, respectively]. All participants were right-handed according to the Edinburgh Handedness Inventory110, and no participants were regularly involved with musical activities and/or professional training.
Musical Stimuli and Task
Melodic contour identification task (CIT)54 was used in the present study. CIT was designed to measure the three types of attention: focused, selective, and alternating attention using melodic contours, including ascending, stationary, and descending. In CIT1, participants were presented with target melodic contours against environmental sounds and asked to identify the direction of contours. In CIT2, participants were presented with target melodic contours against target-like distractors (i.e., another melodic contour played by different instrument timbres) and were asked to identify a target contour presented in a predetermined instrument timbre. In CIT3, two melodic contours were presented, while participants were asked to shift their attention from one to another target contour and identify the direction of contours. For both CIT2 and CIT3, a visual cue (e.g., a picture of an instrument) was shown on the computer screen to inform about the instrument timbre of target contour.
For all CITs, melodic contours were randomly selected and presented in randomly selected instrument timbres. Two different melodic contours were simultaneously presented, and we took measures to avoid combinations being presented in the same two instrument timbres. The experiment took about 20 min to complete and behavioral and haemodynamic responses were recorded throughout the experiment. The contours were presented in one of these three synthesized instruments: piano, flute or string, and their amplitudes were identically normalized. All were generated using a musical instrument digital interface (MIDI) synthesizer that was connected to Logic Pro X, and the experimental apparatus was implemented on a computer using Visual Studio.
fNIRS measurements
We used fNIRS (16-channel Spectratech OEG-16) to record cortical tissue oxygenation (HbO2) and deoxygenation (HHb) to measure the participant’s brain activity during the CITs111,112,113. The band-type fNIRS containing an array of 12 probes was attached to each participant’s forehead to obtain hemodynamic signals in the bilateral frontal cortex (Fig. 5). The probes were connected to the main board of the fNIRS, which communicated with a computer.

Location of the probe and channels. Red and blue boxes represent the locations of detector and emitter; circled numbers represent channel information. The center of the measurement unit was placed on the frontopolar region (Fpr) according to the international 10–20 system.
Participants had a short rest period and then the pre-stimulus baseline data were obtained for 20 seconds while they fixated their eyes on the centre of the monitor. A 20-second baseline was also obtained during inter-task rest periods and post-task period. Once the baseline data were obtained, the participants were presented with instruction and examples of melodic contours. The contours were delivered via a headphone with controlled volume, while the visual cues specifying the target musical instrument were presented to the participants on a monitor. The participants underwent a practice session to become familiar with the direction identification task. When their accuracy was over 80%, the main experimental session was administered. A total of 18 test items were presented in each CIT (a blocked design) and the order of CIT was randomized across participants (Fig. 6). The experiment was performed in a sound-proof room, in which light and temperature were controlled.

The flow of the experiment.
Vector-based phase analysis for fNIRS data
The hemodynamic changes were obtained with a sampling rate of 0.65 s, and the data were converted to concentrated changes of hemoglobin using the modified Beer–Lambert law. Then, a zero-phase low- and high-pass filter with a cut-off frequency of 0.01 to 0.09 Hz was applied using matrix laboratory (MATLAB)114,115,116. The raw fNIRS data were collected and converted to concentrated changes of hemoglobin using the modified Beer–Lambert law117.
In this study, we employed a vector-based phase analysis to examine multifaceted aspects of cerebral hemodynamic changes118,119,120,121. The vector-based phase analysis devised by Kato is a method based on an orthogonal vector coordinate plane defined by four indices: ΔHbO2, ΔHHb, ΔCBV, and ΔCOE121,122,123,124. They are vector components of oxygenated hemoglobin, deoxygenated hemoglobin, total hemoglobin concentration, and oxygen level change in blood vessels, respectively82,121,125. ΔCBV and ΔCOE are obtained by rotating the vector coordinate plane defined by the ΔHbO2 and Δ HHb by 45° counterclockwise. The equations were like the following:
The four indices are subject to calculate angle k, which represents the ratio of ∆COE to ∆CBV. Since a positive ΔCOE value (HHb > HbO2) indicates the hypoxic change due to greater consumption of oxygen resulting in increases of dioxygen in blood vessels, angle k indicates the degree of oxygen exchange81,82,121,125. Angle k can be obtained by the following equation (3).
ΔCBV determines the hyperemic/ischemic state (if CBV is above zero, it is ischemia; if CBV is below zero, it is hyperemia) and ΔCOE determines the hyperoxic/hypoxic state (if COE is above zero, it is hypoxia; if COE is below zero, it is hyperoxia), together leading to changes in k value82,123,126. Hyperoxia is an increase in oxygen supply, which then increases the chances that the brain can utilize delivered oxygen and which can improve CMRO2. Hypoxia, in contrast, refers to the deprivation of an adequate oxygen supply in the brain tissues. Hyperemia is the increase in blood volume to the brain that meet the oxygen demands in the blood vessels, while ischemia means the decrease in the volume127,128,129.
Angle k, thus, can provide additional topological information concerning the various degrees of oxygen exchange (Fig. 7). Increases in k (from 0° to 225°) fall in phases 1 to 5, which reflect the increased hemodynamic activity involved in oxygen level exchange, while decreases in k (from −135° to 0°) fall into phases −1 to −3, which indicate no increases or weak changes (Please see SI Appendix, Table 6 for more details).

Polar coordinate plane of the vector-based phase.
A scalar L, the length of the vector, shows the amplitude of the vector and indicate the amounts of hemoglobin variation123. Further, the four indices (∆COE, ∆CBV, k and L) were used to calculate a phase-associated response intensity (PRI), where krad refers to the degree converted to radians. The PRI denotes the intensity of hemodynamic responses involved in oxygen exchange82. Because the four indices are visualized in the same plane, their relationships as well as the changes across time are observable and readily interpretable.
Statistical analysis
For the behavioral analysis, a two-way mixed analysis of variance (ANOVA) was performed. The independent variables were Group (ABI and non-ABI) and Task (CIT1, CIT2 and CIT3), and the dependent variable was the rate-corrected score (RCS), or the number of correct responses per second of activity. The RCS was estimated using c/ΣRT where c refers to the correct responses and RT refers to the response time130,131. For the hemodynamic analysis, a two-way mixed ANOVA was performed. The independent variables were Group (ABI and non-ABI) and task (pre-task, on-task and post-task, Note that the on-task included CIT1 and CIT2). The dependent variable was the PRIs from the vector-based phase analysis. Specifically, we focused on the hemodynamic data obtained from CHs 1, 2, 3, 13, 14 and 15 [CHs 1, 2 and 3 measured activation in the right dorsolateral prefrontal cortex (DLPFC), while CHs 13, 14 and 15 measured activation in the left DLPFC). These regions are sensitive to cognitive load113,132. All statistical analyses were performed using R.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Van Velzen, J. M., Van Bennekom, C. A., Van Dormolen, M., Sluiter, J. K. & Frings-Dresen, M. H. Factors influencing return to work experienced by people with acquired brain injury: A qualitative research study. Disabil. Rehabil. 33, 2237–2246 (2011).
Kashluba, S., Hanks, R. A., Casey, J. E. & Millis, S. R. Neuropsychologic and functional outcome after complicated mild traumatic brain injury. Arch. Phys. Med. Rehabil. 89, 904–911 (2008).
Ciuffreda, K. J. et al. Occurrence of oculomotor dysfunctions in acquired brain injury: A retrospective analysis. Optom. Am. Optom. Assoc. 78, 155–161 (2007).
Arciniegas, D. et al. Impaired auditory gating and P50 nonsuppression following traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 12, 77–85 (2000).
Barrow, I. M., Collins, J. N. & Britt, L. D. The influence of an auditory distraction on rapid naming after a mild traumatic brain injury: A longitudinal study. J. Trauma Acute Care Surg. 61, 1142–1149 (2006).
Holmqvist, K., Kamwendo, K. & Ivarsson, A.-B. Occupational therapists’ descriptions of their work with persons suffering from cognitive impairment following acquired brain injury. Scand. J. Occup. Ther. 16, 13–24 (2009).
Scheibel, R. S. et al. Altered brain activation during cognitive control in patients with moderate to severe traumatic brain injury. Neurorehabil. Neural Repair 21, 36–45 (2007).
Tsaousides, T. & Gordon, W. A. Cognitive rehabilitation following traumatic brain injury: Assessment to treatment. Mt. Sinai J. Med. A J. Transl. Pers. Med. 76, 173–181 (2009).
Hattiangadi, N. et al. Characteristics of auditory agnosia in a child with severe traumatic brain injury: A case report. Brain Lang. 92, 12–25 (2005).
Loetscher, T. & Lincoln, N. B. Cognitive rehabilitation for attention deficits following stroke. Cochrane Libr. 5 (2013).
Murakami, T. et al. Neuroanatomic pathway associated with attentional deficits after stroke. Brain Res. 1544, 25–32 (2014).
Sinclair, K. L., Ponsford, J. L., Rajaratnam, S. M. & Anderson, C. Sustained attention following traumatic brain injury: Use of the Psychomotor Vigilance Task. J. Clin. Exp. Neuropsychol. 35, 210–224 (2013).
Slovarp, L., Azuma, T. & LaPointe, L. The effect of traumatic brain injury on sustained attention and working memory. Brain Inj. 26, 48–57 (2012).
Ben-David, B. M., Nguyen, L. L. & van Lieshout, P. H. Stroop effects in persons with traumatic brain injury: Selective attention, speed of processing, or color-naming? A meta-analysis. J. Int. Neuropsychol. Soc. 17, 354–363 (2011).
Arciniegas, D. B., Held, K. & Wagner, P. Cognitive impairment following traumatic brain injury. Curr. Treat. Options Neurol. 4, 43–57 (2002).
Rinne, T., Särkkä, A., Degerman, A., Schröger, E. & Alho, K. Two separate mechanisms underlie auditory change detection and involuntary control of attention. Brain Res. 1077, 135–143 (2006).
Marsh, J. E., Vachon, F. & Jones, D. M. When does between-sequence phonological similarity promote irrelevant sound disruption? J. Exp. Psychol. Learn. Mem. Cogn. 34, 243 (2008).
Kaipio, M.-L., Cheour, M., Öhman, J., Salonen, O. & Näätänen, R. Mismatch negativity abnormality in traumatic brain injury without macroscopic lesions on conventional MRI. Neuroreport 24, 440–444 (2013).
Schaefer, M., Tewes, U., Münte, T. F. & Johannes, S. Lateralized irrelevant speech alters visuospatial selective attention mechanisms. Biol. Psychol. 72, 51–58 (2006).
Giard, M.-H., Fort, A., Mouchetant-Rostaing, Y. & Pernier, J. Neurophysiological mechanisms of auditory selective attention in humans. Front. Biosci. 5, 84–94 (2000).
Barker-Collo, S. L., Feigin, V. L., Lawes, C. M., Parag, V. & Senior, H. Attention deficits after incident stroke in the acute period: Frequency across types of attention and relationships to patient characteristics and functional outcomes. Top. Stroke Rehabil. 17, 463–476 (2010).
Kaipio, M.-L. et al. Increased distractibility in closed head injury as revealed by event-related potentials. NeuroReport Rapid Commun. Neurosci. Res. 11, 1463–1468 (2000).
Schweizer, T. A. et al. Brain activity during driving with distraction: An immersive fMRI study. Front. Hum. Neurosci. 7 (2013).
Solbakk, A.-K., Reinvang, I. & Andersson, S. Assessment of P3a and P3b after moderate to severe brain injury. Clin. Electroencephalogr. 33, 102–110 (2002).
Stapleton, T., Ashburn, A. & Stack, E. A pilot study of attention deficits, balance control and falls in the subacute stage following stroke. Clin. Rehabil. 15, 437–444 (2001).
Halterman, C. I. et al. Tracking the recovery of visuospatial attention deficits in mild traumatic brain injury. Brain 129, 747–753 (2005).
Lovell, M. R. & Fazio, V. Concussion management in the child and adolescent athlete. Curr. Sports Med. Rep. 7, 12–15 (2008).
Van Kampen, D. A., Lovell, M. R., Pardini, J. E., Collins, M. W. & Fu, F. H. The ‘value added’ of neurocognitive testing after sports-related concussion. Am. J. Sports Med. 34, 1630–1635 (2006).
Stroop, J. R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 18, 643 (1935).
Reitan, R. M. & Wolfson, D. The Halstead-Reitan neuropsychological test battery. (Neuropsychology Press, 1985).
Swanson, J. Delis-Kaplan Executive Function System: a review. Can. J. Sch. Psychol. 20, 117–28 (2005).
Madigan, N. K., DeLuca, J., Diamond, B. J., Tramontano, G. & Averill, A. Speed of information processing in traumatic brain injury: Modality‐specific factors. J. Head Trauma Rehabil. 15, 943–956 (2000).
Royan, J., Tombaugh, T. N., Rees, L. & Francis, M. The Adjusting-Paced Serial Addition Test (Adjusting-PSAT): Thresholds for speed of information processing as a function of stimulus modality and problem complexity. Arch. Clin. Neuropsychol. 19, 131–143 (2004).
Tombaugh, T. N., Stormer, P., Rees, L., Irving, S. & Francis, M. The effects of mild and severe traumatic brain injury on the auditory and visual versions of the Adjusting-Paced Serial Addition Test (Adjusting-PSAT). Arch. Clin. Neuropsychol. 21, 753–761 (2006).
Gronwall, D. M. A. Paced auditory serial-addition task: a measure of recovery from concussion. Percept. Mot. Skills 44, 367–373 (1977).
Cohen, G. & Martin, M. Hemisphere differences in an auditory Stroop test. Percept. Psychophys. 17, 79–83 (1975).
Wechsler, D. Wechsler Adult Intelligence Scale - Fourth Edition. Stat. Solut. 4, 1–3 (2008).
Bigand, E., McAdams, S. & Forêt, S. Divided attention in music. Int. J. Psychol. 35, 270–278 (2000).
Allen, K., Alais, D., Shinn-Cunningham, B. & Carlile, S. Masker location uncertainty reveals evidence for suppression of maskers in two-talker contexts. J. Acoust. Soc. Am. 130, 2043–2053 (2011).
Best, V., Carlile, S., Kopčo, N. & van Schaik, A. Localization in speech mixtures by listeners with hearing loss. J. Acoust. Soc. Am. 129, 210–215 (2011).
Luo, X., Masterson, M. E. & Wu, C.-C. Contour identification with pitch and loudness cues using cochlear implants. J. Acoust. Soc. Am. 135, 8–14 (2014).
Luo, X., Masterson, M. E. & Wu, C.-C. Melodic interval perception by normal-hearing listeners and cochlear implant users. J. Acoust. Soc. Am. 136, 1831–1844 (2014).
Janata, P., Tillmann, B. & Bharucha, J. J. Listening to polyphonic music recruits domain-general attention and working memory circuits. Cogn. Affect. Behav. Neurosci. 2, 121–140 (2002).
Janata, P. Brain networks that track musical structure. Ann. N. Y. Acad. Sci. 1060, 111–124 (2005).
Zatorre, R. J., Evans, A. C. & Meyer, E. Neural mechanisms underlying melodic perception and memory for pitch. J. Neurosci. 14, 1908–1919 (1994).
Uhlig, S., Jaschke, A. & Scherder, E. Effects of Music on Emotion Regulation: A Systematic Literature Review. In 3rd International Conference on Music & Emotion (ICME3) 11–15 (2013).
Satoh, M., Takeda, K., Nagata, K., Hatazawa, J. & Kuzuhara, S. Activated brain regions in musicians during an ensemble: A PET study. Cogn. Brain Res. 12, 101–108 (2001).
Serences, J. T. & Yantis, S. Spatially Selective Representations of Voluntary and Stimulus-Driven Attentional Priority in Human Occipital, Parietal, and Frontal Cortex. Cereb. Cortex 17, 284–293 (2007).
Talsma, D. & Kok, A. Nonspatial intermodal selective attention is mediated by sensory brain areas: evidence from event-related potentials. Psychophysiology 38, 736–751 (2001).
Belleville, S., Ménard, M.-C. & Lepage, É. Impact of novelty and type of material on recognition in healthy older adults and persons with mild cognitive impairment. Neuropsychologia 49, 2856–2865 (2011).
Jeong, E. Psychometric validation of a music-based attention assessment: Revised for patients with traumatic brain injury. J. Music Ther. 50, 66–92 (2013).
Jeong, E. & Lesiuk, T. L. Development and preliminary evaluation of a music-based attention assessment for patients with traumatic brain injury. J. Music Ther. 48, 551–572 (2011).
Rahman, T. T. A., Mohamed, S. T., Albanouby, M. H. & Bekhet, H. F. Central auditory processing in elderly with mild cognitive impairment. Geriatr. Gerontol. Int. 11, 304–308 (2011).
Jeong, E. & Ryu, H. Melodic Contour Identification Reflects the Cognitive Threshold of Aging. Front. Aging Neurosci. 8 (2016).
Kou, Z., Wiseman, N., Lu, H. & Haacke, M. Magnetic resonance imaging of brain hemodynamics and oxygen metabolism after traumatic brain injury. Proceedings of Neurosciences 1 (2016).
Ferdinand, P. & Roffe, C. Hypoxia after stroke: a review of experimental and clinical evidence. Exp. Transl. Stroke Med. 8, 9 (2016).
Heinz, U. E. & Rollnik, J. D. Outcome and prognosis of hypoxic brain damage patients undergoing neurological early rehabilitation. BMC Res. Notes 8, 243 (2015).
Nour, M., Scalzo, F. & Liebeskind, D. S. Ischemia-reperfusion injury in stroke. Interv Neurol 1, 185–199 (2013).
Veenith, T. V. et al. Pathophysiologic mechanisms of cerebral ischemia and diffusion hypoxia in traumatic brain injury. JAMA Neurol. 73, 542–550 (2016).
Vespa, P. M. Brain hypoxia and ischemia after traumatic brain injury: Is oxygen the right metabolic target? JAMA Neurol. 73, 504–505 (2016).
Bonne, O. et al. Cerebral blood flow in chronic symptomatic mild traumatic brain injury. Psychiatry Res. Neuroimaging 124, 141–152 (2003).
Grossman, E. J. et al. Cognitive impairment in mild traumatic brain injury: A longitudinal diffusional kurtosis and perfusion imaging study. Am. J. Neuroradiol. 34, 951–957 (2013).
Lu, J. et al. Histone deacetylase inhibitors are neuroprotective and preserve NGF-mediated cell survival following traumatic brain injury. Proc. Natl. Acad. Sci. 110, 10747–10752 (2013).
Mayer, A. R. et al. Investigating the properties of the hemodynamic response function after mild traumatic brain injury. J. Neurotrauma 31, 189–197 (2014).
Metting, Z., Spikman, J. M., Rödiger, L. A. & Van der Naalt, J. Cerebral perfusion and neuropsychological follow up in mild traumatic brain injury: acute versus chronic disturbances? Brain Cogn. 86, 24–31 (2014).
Wu, H.-M. et al. Selective metabolic reduction in gray matter acutely following human traumatic brain injury. J. Neurotrauma 21, 149–161 (2004).
Kou, Z., Ye, Y. & Haacke, E. M. Evaluating the role of reduced oxygen saturation and vascular damage in traumatic brain injury using magnetic resonance perfusion-weighted imaging and susceptibility-weighted imaging and mapping. Top. Magn. Reson. Imaging 24, 253–265 (2015).
Doshi, H. et al. Cerebral hemodynamic changes of mild traumatic brain injury at the acute stage. PLoS One 10 (2015).
Tichauer, K. M., Hadway, J., Lee, T.-Y. & Lawrence, K. S. Near-infrared spectroscopy measurement of cerebral oxidative metabolism: A validation study. J. Cereb. Blood Flow Metab. 25, S88–S88 (2005).
Benni, P. B., MacLeod, D., Ikeda, K. & Lin, H. M. A validation method for near-infrared spectroscopy based tissue oximeters for cerebral and somatic tissue oxygen saturation measurements. J. Clin. Monit. Comput. 32, 269–284 (2018).
Adelson, P. D., Nemoto, E., Colak, A. & Painter, M. In Intracranial Pressure and Neuromonitoring in Brain Injury 250–254 (Springer, 1998).
Haitsma, I. K. & Maas, A. I. Monitoring cerebral oxygenation in traumatic brain injury. Prog. Brain Res. 161, 207–216 (2007).
Weatherall, A., Skowno, J., Lansdown, A., Lupton, T. & Garner, A. Feasibility of cerebral near‐infrared spectroscopy monitoring in the pre‐hospital environment. Acta Anaesthesiol. Scand. 56, 172–177 (2012).
Merzagora, A. C., Schultheis, M. T., Onaral, B. & Izzetoglu, M. Functional near-infrared spectroscopy–based assessment of attention impairments after traumatic brain injury. J. Innov. Opt. Health Sci. 4, 251–260 (2011).
Kontos, A. P. et al. The effects of combat-related mild traumatic brain injury (mTBI): Does blast mTBI history matter? J. Trauma Acute Care Surg. 79, S146–S151 (2015).
Hashimoto, K., Uruma, G. & Abo, M. Activation of the prefrontal cortex during the wisconsin card sorting test (Keio Version) as measured by two-channel near-infrared spectroscopy in patients with traumatic brain injury. Eur. Neurol. 59, 24–30 (2008).
Hibino, S. et al. Oxyhemoglobin changes during cognitive rehabilitation after traumatic brain injury using near infrared spectroscopy. Neurol. Med. Chir. (Tokyo). 53, 299–303 (2013).
Hegde, S. Music-based cognitive remediation therapy for patients with traumatic brain injury. Front. Neurol. 5 (2014).
Kewman, D. G., Yanus, B. & Kirsch, N. Assessment of distractibility in auditory comprehension after traumatic brain injury. Brain Inj. 2, 131–137 (1988).
Sohlberg, M. M. & Mateer, C. A. Cognitive rehabilitation: An integrative neuropsychological approach. (Guilford Publications, 2001).
Yoshino, K., Oka, N., Yamamoto, K., Takahashi, H. & Kato, T. Correlation of prefrontal cortical activation with changing vehicle speeds in actual driving: a vector-based functional near-infrared spectroscopy study. Front. Hum. Neurosci. 7 (2013).
Oka, N. et al. Greater activity in the frontal cortex on left curves: a vector-based fNIRS study of left and right curve driving. PLoS One 10, e0127594 (2015).
Chen, J. K., Johnston, K. M., Petrides, M. & Ptito, A. Neural substrates of symptoms of depression following concussion in male athletes with persisting postconcussion symptoms. Arch. Gen. Psychiatry 65, 81–89 (2008).
Chen, J. K. et al. Functional abnormalities in symptomatic concussed athletes: An fMRI study. Neuroimage 22, 68–82 (2004).
Sánchez-Carrión, R. et al. Frontal Hypoactivation on Functional Magnetic Resonance Imaging in Working Memory after Severe Diffuse Traumatic Brain Injury. J. Neurotrauma 25, 479–494 (2008).
Slobounov, S., Gay, M., Johnson, B. & Zhang, K. Concussion in athletics: Ongoing clinical and brain imaging research controversies. Brain Imaging Behav. 6, 224–243 (2012).
Soeda, A. et al. Cognitive impairment after traumatic brain injury: A functional magnetic resonance imaging study using the Stroop task. Neuroradiology 47, 501–506 (2005).
Oehmichen, M., Woetzel, F. & Meissner, C. Hypoxic–ischemic changes in SIDS brains as demonstrated by a reduction in MAP2-reactive neurons. Acta Neuropathol. 117, 267–274 (2009).
Fujiwara, N. et al. Evoked-cerebral blood oxygenation changes in false-negative activations in BOLD contrast functional MRI of patients with brain tumors. Neuroimage 21, 1464–1471 (2004).
Murata, Y. et al. Effects of cerebral ischemia on evoked cerebral blood oxygenation responses and BOLD contrast functional MRI in stroke patients. Stroke 37, 2514–2520 (2006).
Sakatani, K. et al. Comparison of blood-oxygen-level–dependent functional magnetic resonance imaging and near-infrared spectroscopy recording during functional brain activation in patients with stroke and brain tumors. J. Biomed. Opt. 12, 62110–62118 (2007).
Li, Y., Zhou, C., Calvert, J. W., Colohan, A. R. & Zhang, J. H. Multiple effects of hyperbaric oxygen on the expression of HIF-1α and apoptotic genes in a global ischemia–hypotension rat model. Exp. Neurol. 191, 198–210 (2005).
Peng, Z., Xiao, P., Guo, H. & Liu, Q. Effect of early hyperbaric oxygen on neuronal apoptosis and learning and memory of cerebral ischemia-reperfusion injury in rats. Zhong Nan Da Xue Xue Bao Yi Xue Ban 34, 468–475 (2009).
Zhou, J. G., Liu, J. C. & Fang, Y. Q. Effect of hyperbaric oxygen on the expression of proteins Bcl-2 and Bax in the gerbil hippocampus CA1 following forebrain ischemia reperfusion. Zhongguo Ying Yong Sheng Li Xue Za Zhi 16, 298–301 (2000).
Boussi-Gross, R. et al. Hyperbaric oxygen therapy can improve post concussion syndrome years after mild traumatic brain injury-randomized prospective trial. PLoS One 8, e79995 (2013).
Liu, W. et al. Perfusion deficits in patients with mild traumatic brain injury characterized by dynamic susceptibility contrast MRI. NMR Biomed. 26, 651–663 (2013).
Wolf, E. G., Baugh, L. M., Kabban, C. M., Richards, M. F. & Prye, J. Cognitive function in a traumatic brain injury hyperbaric oxygen randomized trial. Undersea Hyperb. Med. 42, 313–332 (2015).
Fishburn, F. A., Norr, M. E., Medvedev, A. V & Vaidya, C. J. Sensitivity of fNIRS to cognitive state and load. Front. Hum. Neurosci. 8 (2014).
McKendrick, R., Ayaz, H., Olmstead, R. & Parasuraman, R. Enhancing dual-task performance with verbal and spatial working memory training: continuous monitoring of cerebral hemodynamics with NIRS. Neuroimage 85, 1014–1026 (2014).
Holper, L. & Wolf, M. Single-trial classification of motor imagery differing in task complexity: a functional near-infrared spectroscopy study. J. Neuroeng. Rehabil. 8, 34 (2011).
Hill, K. T. & Miller, L. M. Auditory attentional control and selection during cocktail party listening. Cereb. Cortex 20, 583–590 (2010).
Seydell-Greenwald, A., Greenberg, A. S. & Rauschecker, J. P. Are you listening? Brain activation associated with sustained nonspatial auditory attention in the presence and absence of stimulation. Hum. Brain Mapp. 35, 2233–2252 (2014).
Morita, A., Morishima, Y. & Rackham, D. W. Right Dorsolateral Prefrontal Cortex Activation during a Time Production Task: A Functional Near-Infrared Spectroscopy Study. Asian J. Neurosci. 2015 (2015).
Lipschutz, B., Kolinsky, R., Damhaut, P., Wikler, D. & Goldman, S. Attention-dependent changes of activation and connectivity in dichotic listening. Neuroimage 17, 643–656 (2002).
Jeong, E. & Ryu, H. Nonverbal auditory working memory: Can music indicate the capacity? Brain Cogn. 105, 9–21 (2016).
Pressnitzer, D. Auditory scene analysis: the sweet music of ambiguity. Front. Hum. Neurosci. 5 (2011).
Neuhoff, J. G. The Sonification Handbook. (Logos Publishing House, 2011).
Alain, C., McDonald, K. L., Ostroff, J. M. & Schneider, B. Age-related changes in detecting a mistuned harmonic. J. Acoust. Soc. Am. 109, 2211–2216 (2001).
Jahng, S., Na, D. L. & Kang, Y. Constructing a composite score for the Seoul Neuropsychological Screening Battery-Core. Dement Neurocogn Disord 14, 137–142 (2015).
Oldfield, R. C. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9, 97–113 (1971).
Ogawa, Y., Kotani, K. & Jimbo, Y. Relationship between working memory performance and neural activation measured using near‐infrared spectroscopy. Brain Behav. 4, 544–551 (2014).
Peck, E. M. M., Yuksel, B. F., Ottley, A., Jacob, R. J. K. & Chang, R. Using fNIRS brain sensing to evaluate information visualization interfaces. in Proceedings of the SIGCHI Conference on Human Factors in Computing Systems 473–482 (ACM, 2013).
Yasumura, A., Inagaki, M. & Hiraki, K. Relationship between neural activity and executive function: An NIRS study. ISRN Neurosci. 2014 (2014).
Akgül, C. B., Sankur, B. & Akin, A. Spectral analysis of event-related hemodynamic responses in functional near infrared spectroscopy. J. Comput. Neurosci. 18, 67–83 (2005).
Bauernfeind, G., Scherer, R., Pfurtscheller, G. & Neuper, C. Single-trial classification of antagonistic oxyhemoglobin responses during mental arithmetic. Med. Biol. Eng. Comput. 49, 979–984 (2011).
Morren, G. et al. Detection of fast neuronal signals in the motor cortex from functional near infrared spectroscopy measurements using independent component analysis. Med. Biol. Eng. Comput. 42, 92–99 (2004).
Baker, W. B. et al. Modified Beer-Lambert law for blood flow. Biomed. Opt. Express 5, 4053 (2014).
Herff, C. et al. Classification of mental tasks in the prefrontal cortex using fNIRS. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society 2160–2163, https://doi.org/10.1109/EMBC.2013.6609962 (2013).
Cui, X., Bray, S. & Reiss, A. L. Functional near infrared spectroscopy (NIRS) signal improvement based on negative correlation between oxygenated and deoxygenated hemoglobin dynamics. Neuroimage 49, 3039–3046 (2010).
Tachtsidis, I. & Scholkmann, F. False positives and false negatives in functional near-infrared spectroscopy: issues, challenges, and the way forward. Neurophotonics 3, 31405 (2016).
Yoshino, K., Oka, N., Yamamoto, K., Takahashi, H. & Kato, T. Functional brain imaging using near-infrared spectroscopy during actual driving on an expressway. Front. Hum. Neurosci. 7 (2013).
Kato, T. Apparatus for evaluating biological function. (2006).
Yoshino, K. & Kato, T. Vector-based phase classification of initial dips during word listening using near-infrared spectroscopy. Neuroreport 23, 947–951 (2012).
Akiyama, T., Ohira, T., Kawase, T. & Kato, T. TMS orientation for NIRS-functional motor mapping. Brain Topogr. 19, 1–9 (2006).
Zafar, A., Hong, K.-S. & Khan, M. J. Initial dip detection based on both HbO and HbR vector-based phase analysis. In Society of Instrument and Control Engineers of Japan (SICE), 2016 55th Annual Conference of the 543–548 (IEEE, 2016).
Zafar, A. & Hong, K.-S. Detection and classification of three-class initial dips from prefrontal cortex. Biomed. Opt. Express 8, 367–383 (2017).
Diringer, M. N. Hyperoxia–good or bad for the injured brain? Curr. Opin. Crit. Care 14, 167 (2008).
Rossi, D. J., Brady, J. D. & Mohr, C. Astrocyte metabolism and signaling during brain ischemia. Nat. Neurosci. 10, 1377 (2007).
Kelly, D. F. et al. Hyperemia following traumatic brain injury: Relationship to intracranial hypertension and outcome. J. Neurosurg. 85, 762–771 (1996).
Woltz, D. J. & Was, C. A. Availability of related long-term memory during and after attention focus in working memory. Mem. Cognit. 34, 668–684 (2006).
Vandierendonck, A. A comparison of methods to combine speed and accuracy measures of performance: A rejoinder on the binning procedure. Behav. Res. Methods 49, 653–673 (2017).
Moriguchi, Y., Sakata, Y., Ishibashi, M. & Ishikawa, Y. Teaching others rule-use improves executive function and prefrontal activations in young children. Front. Psychol. 6 (2015).
Acknowledgements
This study was supported by a National Research Foundation of Korea grant funded by the Korean government (NRF-2018R1C1B5044305).
Author information
Authors and Affiliations
Contributions
E.J. conceived and designed the experiments; J.S. recruited participants and arranged individual experiments; E.J., performed the experiments; G.J., E.J., J.L., J.S. analysed and interpreted the data; G.J. and E.J. prepared tables and figures; E.J. and G.J. wrote the manuscript; E.J., G.K., J.S., and H.R. edited the manuscript; and all authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jeong, E., Ryu, H., Shin, JH. et al. High Oxygen Exchange to Music Indicates Auditory Distractibility in Acquired Brain Injury: An fNIRS Study with a Vector-Based Phase Analysis. Sci Rep 8, 16737 (2018). https://doi.org/10.1038/s41598-018-35172-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-35172-2
Keywords
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
