
Abstract
Our aim was investigating variability in spatiotemporal parameters and kinetics of obstacle avoidance steps of different height obstacles in people with Parkinson’s disease (PD) and healthy older people. Twenty-eight participants have included (15 PD – stage disease: 2.1 ± 0.4 pts) and 13 healthy older people (control group). Each subject performed 10 trials of the following tasks: low obstacle, intermediate obstacle and high obstacle. The presentation order was randomized by block for each condition and participant. The spatiotemporal parameters was collected by GAITRite. An optoelectronic system (Optotrak Northern Digital Inc.) with 100 Hz of frequency was used to collect obstacle parameters. The kinect parameters (propulsion impulse and braking impulse) were acquire through two force plates (AccuGait), with a frequency of acquisition 200 Hz. Intersteps variability was calculated throughout mean values, standard deviation and coefficient of variation of two obstacle avoidance steps for each trial. PD group presented greater variability than control group on vertical and horizontal distances to the obstacle. Obstacle height did not change kinect’s parameters for both groups. The combination of task complexity (obstacle height) and disease impairments (gait alteration, loss of balance, etc) contributing for greater variability of Parkinson’s group. Besides, low obstacle and high obstacle seem to exacerbate variability of distance between obstacle and foot.
Similar content being viewed by others


Introduction
Dealing with obstacle and complex environments are a challenging daily life tasks and represents the most cause of falls in older1. We have found in our previous study that both people with PD and neurological healthy individuals increased their step-to-step and walking variability in the steps preceding low obstacle avoidance compared to other obstacle heights (intermediate and high obstacles), mainly in last step (n-1) before obstacle avoidance2. However, this study was not focused on how obstacle height could affect obstacle avoidance itself. Vitório et al.3 observed that during approach phase, PD presented a shorter step length (considered a bad behavior) but, during high obstacle crossing, they could increase toe-clearance. This behavior could indicate a different behavior and brain control for these two parts of obstacle avoidance (approaching phase and obstacle crossing). Moreover, obstacle crossing is a crucial point that happens daily with different height and shapes. Foot positioning in the last step before obstacle avoidance and after obstacle avoidance (distance between foot and obstacle and toe clearance), the impulse to cross the obstacle and toe clearance could be an important information to avoid trips during obstacle avoidance in people with PD1. Low variability in these parameters during obstacle avoidance could indicate accuracy and security of the system that controls gait4,5. The present study is the first study that investigated the variability of different parameters of the avoidance step in people with PD, especially considering obstacle height manipulations.
The obstacle height seems an important aspect in the strategy (adjustments) to avoid an obstacle. When the obstacle height is manipulated there is an increased in the motor requirement and planning, which demands more of the corporal and navigational system6,7. However, during approaching phase, our previous study2 showed, as expected, different behavior according obstacle height. During approaching phase for low obstacles, people with PD and their healthy-matched control increase the variability for the last foot positioning before obstacle avoidance. In other words, for the lowest one, they changed their gait very closer to the obstacle2. Thus, due to different heights of obstacle that are facing daily, obstacle crossing could be considered a very dangerous situation that could leading to fall. For example, higher obstacle requires conservative strategy in people with PD, which increase the toe clearance of both limb (leading and trailing limbs) and the step duration of the crossing step3,8. Probably the deficits in the spatial-temporal3,9 and neuromuscular10 adjustments, executive function11, attention11,12 and perceptual system10 presented by people with PD require more time-to-time adjustments13 to avoid an obstacle. Impairments on basal ganglia connections like pedunculopontine nucleus, that is related with control and voluntary movements11, may explain the deficits on postural control instability, walking deficits (slower steps, shorter steps, greater step duration), deficits on attention and learning problems, correction of movements (variability))14,15 in older people with PD. In addition, people with PD have difficult to synchronize visual and kinesthetic stimulus16,17, impairing the ability to adjust themselves when the context is manipulated. Therefore, the influence of obstacle height on variability of crossing step parameters could help to understand the pathology of gait in people with PD.
The aim of this study, therefore, was to investigate the effects of obstacle height (low, intermediate and high obstacle) on variability of spatial–temporal of trailing and leading limb and impulses of crossing step in people with PD and neurological healthy individuals. According our previous study2, we expected that the variability of gait parameters will be greater in the low obstacle avoidance in people with PD since this condition present a greater adjustment range than higher obstacle.
Methods
Participants
Data for this study were obtained in the same experiment as those published previously in Simieli et al.2. Older people with PD were selected from the Physical Activity Program for Patients with PD (PROPARKI Group - UNESP – Rio Claro – Brazil) database (more than one hundred individuals). Older neurologically healthy individuals were selected from the database of the Physical Activity Program for Older People (PROFIT - UNESP - Rio Claro). Therefore, the following exclusion criteria were analyzed previously for both groups: age under 60, cognitive decline, history of orthopedic problems (if the participant use any walking aid, we excluded from the sample), vision (glaucoma, cataract) and vestibular (dizziness, labyrinthitis) that prevented performance of the experimental protocol. Participants with diabetes mellitus were also excluded, since plantar sensitivity may be altered and thereby, impair gait2. Any visual problems that could be corrected with glasses, were included on the sample. In addition, for older people with PD, the individual was required to be under dopaminergic medication treatment and in a stage of PD up to III according to the Hoehn & Yahr disability Scale18,19. Furthermore, an experienced neurologist evaluated and diagnosed the older people with PD according to the London Brain Bank – a guideline for diagnosis20.
Clinical and walking with obstacle crossing evaluations
Both clinical and gait evaluations of the PD group were performed in an “ON” state of medication, about an hour after taking the dopaminergic medication. The following clinical scale were applied in older people with PD: Unified Parkinson’s Disease Rating Scale – UPDRS19; the Hoehn and Yahr score18; and Mini Mental State Examination21 (performed by both groups). The analysis with G*Power software showed that a sample size of at least 14 individuals (7 in each group) was needed for an 95% probability to detect a difference of 20% between the groups for the primary outcome with a type I error of 0.05, based on previously published data (Hausdorff and colleagues22).
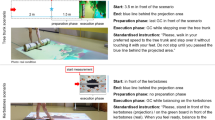
Participants were instructed to walk at their preferred speed until the end of the walkway (8 m). Ten trials of following walking conditions were performed by participants: low obstacle avoidance, intermediate obstacle avoidance and high obstacle avoidance. Thus, each participant performed 30 trials in total. The trials were performed in blocks in a randomized order for all participants. The obstacle was positioned in the center of the walkway (4 m from the start position), which height was customized for each individual. High obstacle was height equal to half the knee height (if the half knee was greater than 48.5 cm, the obstacle height was 25 cm, if lower than 48.5 cm, the obstacle height was 20 cm). Low obstacle was height equal to the ankle height (if the ankle height was greater than 7 cm, the obstacle height was 10 cm; if lower than 7 cm, the obstacle height was 5 cm). Intermediate obstacle was height equal to half the sum of the high obstacle height and low obstacle height. The obstacle width and length were 60 cm and 3 cm, respectively, independent of obstacle height. The start point was adjusted to ensure comfortable crossing with the right leg. In addition, the participants were instructed to avoid contact with the obstacle in trials where the obstacle was present (see Fig. 1).

Schematic of steps analyzed during the task. (a) Illustrate the obstacle crossing parameters3. (b) Illustrates all steps performed and steps analyzed.
The spatial-temporal parameters were acquired through GAITRite® (CIR System, Clifton, NJ, USA) and three-dimensional optoelectronic system (OPTOTRAK Certus), positioned orthogonal to the plane of progression to the right of the walkway, both with frequency of 100 samples/s. Four infrared emitters were placed over the following anatomical points: lateral face of calcaneus and head of the fifth metatarsus of the right limb, and medial face of calcaneus and head of the first metatarsus of the left limb. The data were filtered with a fifth order low-pass Butterworth filter with a cut-off frequency of 6 Hz). Two force plates (200 samples/s) – 50 × 50 cm (AccuGait, Advanced Mechanical Technologies, Boston, MA) were used to collect ground force reaction. The first force plate was placed before obstacle avoidance (force plate was stepped with trailing limb – left limb) and the second force plate was placed after obstacle (force plate was stepped with leading limb – right limb). Force plate data were filtered with a 4th order filter with a cutoff frequency of 16 Hz and the magnitude of the ground reaction force was normalized by body weight.
Data analysis
The parameters were calculated in Matlab (Version 7.0 – Math Works, Inc.). The following parameters were analyzed: step length, step duration, step velocity, step width, double support time (expressed by percentage of step duration), single support time (expressed by percentage of step duration), toe clearance of the leading and trailing limbs (vertical distance from foot to obstacle), horizontal distance from the leading and trailing limb to the obstacle before and after obstacle crossing, and braking and propulsive vertical impulses. These parameters were calculated during obstacle avoidance steps from leading limb (right limb) and trailing limb (left limb).
The variability of these parameters was calculated by the average values and standard deviations for each step for each participant, followed by the coefficient of variation of each step in each condition2,4,23,24. We calculated the variability of step of leading limb and trailing limb (2 steps).
Statistical analysis
The data of interest was statistically analyzed using SPSS 15.0 software for Windows with a significance level maintained at 0.05. The Shapiro-Wilk and Levene’s tests were used to verify the normal distribution of data and homogeneity of variance, respectively. The variability of parameters was compared through two-way ANOVAs for group (PD group x control group) and condition (low obstacle x intermediate obstacle x high obstacle), with repeated measures for condition. We also compared the trials to verify if they have a learning effect. Bonferroni post-hoc tests were performed to identify differences when the ANOVA revealed significant interactions.
Results
Twenty-eight participated in this study, who were distributed in two groups: 15 older people with PD (70.66 ± 6.55 years old; 1.63 ± 0.07 m; 70.61 ± 9.82 kg; Hoehn & Yahr = 2.1 ± 0.4 pts; UPDRS-motor = 24.75 ± 11.25 pts; 8 men) – PD group; and 13 older neurologically healthy individuals (71.53 ± 5.42 years old; 1.59 ± 0.08 m; 70.50 ± 15.49 kg; 7 men) – control group. Individuals of both group have no cognitive deficits, which was analyzed by the Mini Mental State Examination (PD group – 28.26 ± 1.66 pts; control group – 28.46 ± 1.63 pts). There are no different between groups for age (p = 0.76), body weight (p = 0.98), height (p = 0.20) and Mini Mental State Examination (p = 0.76). We also performed a chi-square for sex frequencies in each group, and there were no differences (PD group Χ2 = 0.067, p = 0.796; Control group Χ2 = 0.077, p = 0.782). Moreover, we have did an analysis to verify if they had any learning effect among trials. For this, we compared the values of first trial, second, third until the last one. We did not find any difference between the trials and, consequently, no learning effects for each group (we compared (ANOVA factor for group and trial sequence) first trial to second trial, third, fourth, until tenth (p > 0.05.). There were no freezing episodes during the experiment.
The means values of parameters for each group and according each condition are presented in Table 1.
Variability of gait parameters
ANOVA did not indicate main effects of group and group*condition interaction for kinetic parameters of force plate placed after the obstacle (F4,23 = 0.342, p = 0.323). The ANOVA indicated a condition effect for force plate placed before obstacle for propulsion impulse (F4,23 = 4,720, p = 0.006). In addition, high obstacle presented greater variability of propulsive impulse compared to intermediate obstacle (p = 0.003 – Fig. 2).

Variability of kinects parameters for each group in each condition.
The ANOVA indicated group*condition interaction. PD group presented greater variability of horizontal distance from the trailing limb to the obstacle before obstacle crossing (F2,52 = 1.169, p < 0.001) compared to control group in all obstacle height. In addition, PD group increased variability of horizontal distance from the leading limb to the obstacle after obstacle crossing and decreased variability of horizontal distance from the trailing limb to the obstacle after obstacle crossing compared to control group during low (F2,52 = 7.753, p < 0.001) and intermediate (F2,52 = 7.753, p < 0.01) obstacle avoidance. Furthermore, during low obstacle avoidance, PD group revealed greater variability of leading limb toe-clearance compared to control group (F2,52 = 6.345, p < 0.001). Finally, PD group increased variability of leading limb toe-clearance during low (F2,52 = 6.345, p < 0.002) and high (F2,52 = 6,345 p < 0.004) obstacle avoidance compared to intermediate obstacle avoidance while control group increased variability of leading limb toe-clearance during high obstacle avoidance compared to low and intermediate obstacle avoidance (F2,52 = 6.345, p < 0.001).
For group (Fig. 3), older people with PD presented greater variability of horizontal distance from the trailing limb to the obstacle before obstacle crossing (F4,23 = 10.201, p < 0.001) and horizontal distance from the leading limb to the obstacle after obstacle crossing (F4,23 = 10.201, p < 0.04) and lesser variability of horizontal distance from the trailing limb to the obstacle after obstacle crossing compared to control group (p < 0.01).

Group*obstacle variability for horizontal and vertical foot-obstacle distance before and after obstacle avoidance for leading and trailing limb. (a) Difference between low and high obstacle avoidance; (b) Difference between intermediate and high obstacle avoidance; (c) difference between low and intermediate obstacle. *Difference between people with PD and control group.
Regarding condition (Table 2), low obstacle showed lesser variability of step velocity compared to other obstacle height (F2,52 = 4,646, p < 0.001). High obstacle exhibited greater variability of leading limb toe-clearance (low obstacle – F2,52 = 13.381, p < 0.007 and intermediate obstacle – F2,52 = 13.381, p < 0.001) and lesser variability of trailing limb toe-clearance (F2,52 = 13.381, p < 0.001 for both obstacle height) compared to other obstacle height.
Discussion
The aim was to investigate the variability of spatiotemporal and kinect parameters during obstacle avoidance with different obstacle heights in people with PD and healthy neurological older people (control group). PD people showed higher values of variability than control group, mainly for horizontal distance to the obstacle and toe-clearance, corroborating with other researches4,25. However, the main findings discussed below are against our initial hypothesis: (i) the absence of effect in kinect parameters between groups and obstacle heights; (ii) increasing variability of step velocity during intermediate and high obstacle avoidance compared with low obstacle; (iii) the great variability of horizontal distance of trailing limb after obstacle avoidance for the control group.
Control group and people with PD seem to not variate during obstacle avoidance for kinect parameters. Both groups maintain their kinect characteristics during obstacle avoidance for all heights. A possible explanation is the robustness (hardiness) of these parameters. During aging, occurs neuromotor and muscular deteriotation26. This fact could be useful to understand that both group decreases muscle control and, under complexes situation (like obstacle avoidance), adopt an robustness strategy, maintaining their pattern looking for safe. Moreover, the trailing limb crossing occurs without visual information, once this member is behind participant view8,27 and contribute in this robustness. If we extrapolated our results and compare it with the results of Patla (1998)28, in which they found no difference for trailing limb during no-vision condition (regarding that they had no kinect analysis), it is possible to supposed that PD people and older people adopt this robustness strategy to keep safer. Furthermore, it is possible to link the conservation of kinect parameters before obstacle avoidance with toe-clearance (elevation of leading limb) in the three different obstacle heights. The participants maintain a safe elevation (~30 cm - the sum of obstacle height with toe clearance). In this way, it seems easier keep limb elevation height by muscle force than by the resultant of ground reaction force.
Higher and intermediate obstacles increase step velocity variability for both groups. Low obstacle avoidance showed lower values for step velocity variability than other two conditions (intermediate and high obstacle). Increase step velocity variability during obstacle avoidance could be a dangerous strategy. The physical limitation caused by higher obstacle needs a great time for preparation and attention8. Changing constantly the step velocity could increase fall risk, once older people did not showed muscular and motor system fully intact to react for any perturbation of the task26. In this form, if the planning was made on a wrong way, there will no enough time to correction and could occurring a stumbling and, consequently, a fall. Furthermore, higher obstacles generate a challenge, making more difficult to find a pattern to avoid these obstacles, increasing the variability. In other hand, low obstacles allow this pattern once it did not represent a great challenge. However, maintain the pattern could be deceptive, once both group miscalculated when they need to avoid low obstacle, let the adjustments for the last two steps before the obstacle2.
Horizontal foot placement to obstacle and toe-clearance are more variable in people with PD. This finding could be explained by follow arguments: (i) obstacle avoidance need higher complexity and execution of the movement3. People with PD present sensorial deficits7,11 which impair the correct environment perception. In this way, people with PD needs to perform constantly adjustments to correct errors and perform the task with successful. This situation becomes more severe in extreme situations, like low and high obstacle, increasing toe-clearance variability. The incapacity of this population to perceive the environment correctly in these situations17 become obstacle avoidance more challenging; (ii) obstacle avoidance relays on visual information of the relationship of the body segments with the obstacle, in the way to keep a safe distance29. For this, it is necessary a visuospatial attention to identify the obstacle and integrate visual and somatosensory information to elevate the foot in a safe distance to the obstacle29. Due to sensorial deficits of people with PD7, obstacle presence needs a complex interpretation, which needs more cortical areas to process the gait11, increasing modulation before and during obstacle avoidance; (iii) intermediate obstacle (~15 cm) is a commonly height faced off daily by participants (in Brazil, almost all curbs need to have this height, according techniques rules) and could not be so challenging as others.
Regarding our findings, the present study has some limitations. A bigger sample could be interest to reinforce our results. However, the sample size analysis indicated that the number of the actual sample is enough to present significant findings. Moreover, could be interesting to personalize the obstacle’s height according to subject’s height.
Conclusion
People with PD present great variability than control group for horizontal distance to the obstacle and toe-clearance. The combination of task complexity and disease impairments contributing for greater variability of this group. Besides, low obstacles and high obstacle seem to exacerbate variability of horizontal distance and toe-clearance for people with PD. However, obstacle height did not interfere on kinect parameters variability during obstacle avoidance. Future studies could analyze the behavior of fallers during this task, once obstacle avoidance is the most common cause of fall among older adults.
Ethics Committee
Older people gave informed consent by signing the informed consent form approved by the local Ethics Committee at UNESP – Campus Rio Claro/Brazil (CAAE #580.665/2013). All protocol was approved by the same Committee and was in accordance with Ethical guidelines (Brazilian Resolution #196/96 – National Health Council – National Council in Research Ethics).
Change history
16 April 2019
A correction to this article has been published and is linked from the HTML and PDF versions of this paper. The error has not been fixed in the paper.
References
Stolze, H. et al. Falls in frequent neurological diseases: Prevalence, risk factors and aetiology. J. Neurol. 251, 79–84 (2004).
Simieli, L. et al. The variability of the steps preceding obstacle avoidance (approach phase) is dependent on the height of the obstacle in people with Parkinson’s disease. PLoS One 12, 1–15 (2017).
Vitório, R., Pieruccini-Faria, F., Stella, F., Gobbi, S. & Gobbi, L. T. B. Effects of obstacle height on obstacle crossing in mild Parkinson’s disease. Gait Posture 31, 143–146 (2010).
Hausdorff, J. M., Cudkowicz, M. E. & Firtion, R. Gait Variability and Basal Ganglia Disorders: Stride-to-S tride Variations of Gait Cycle Timing in Parkinson’ s Disease and Huntington’ s Disease. Mov. Disord. 13, 428–437 (1998).
Terrier, P. & Schutz, Y. Variability of gait patterns during unconstrained walking assessed by satellite positioning (GPS). Eur. J. Appl. Physiol. 90, 554–561 (2003).
Maidan, I. et al. Altered brain activation in complex walking conditions in patients with Parkinson’s disease. Park. Relat. Disord. 25, 91–96 (2016).
Almeida, Q. J., Frank, J. S., Roy, E. A., Patla, A. E. & Jog, M. S. Dopaminergic modulation of timing control and variability in the gait of Parkinson’s disease. Mov. Disord. 22, 1735–1742 (2007).
Pieruccini-Faria, F. et al. Evaluating the acute contributions of dopaminergic replacement to gait with obstacles in parkinson’s disease. J. Mot. Behav. 45, 369–380 (2013).
Vitório, R. et al. Visual cues and gait improvement in Parkinson’s disease: Which piece of information is really important? Neuroscience 277, 273–280 (2014).
Stegemller, E. L. et al. Postural instability and gait impairment during obstacle crossing in parkinson’s disease. Arch. Phys. Med. Rehabil. 93, 703–709 (2012).
Dirnberger, G. & Jahanshahi, M. Executive dysfunction in Parkinson’s disease: A review. J. Neuropsychol. 7, 193–224 (2013).
Sheridan, P. L., Solomont, J., Kowall, N. & Hausdorff, J. M. Influence of Executive Function on Locomotor Function: Divided Attention Increases Gait Variability in Alzheimer’s Disease. J. Am. Geriatr. Soc. 51, 1633–1637 (2003).
Nemanich, S. T. et al. Predictors of gait speeds and the relationship of gait speeds to falls in men and women with parkinson disease. Parkinsons. Dis. 2013, (2013).
Mori, F., Okada, K., Nomura, T. & Kobayashi, Y. The Pedunculopontine Tegmental Nucleus as a Motor and Cognitive Interface between the Cerebellum and Basal Ganglia. Front. Neuroanat. 10, 1–8 (2016).
Fytagoridis, A., Silburn, P. A., Coyne, T. J. & Thevathasan, W. Understanding the human pedunculopontine nucleus in Parkinson’s disease. J. Neural Transm. 123, 769–774 (2016).
Demirci, M., Grill, S., Mcshane, L. & Hallett, M. A Mismatch Between Kinesthetic and Visual Perception in Parkinson’ s Disease. Ann. Neurol. 41, 781–788 (1996).
Chen, H.-C., Ashton-Miller, J. A., Alexander, N. B. & Schultz, A. B. Stepping Over Obstacles: Gait Patterns of Healthy Young and Old Adults. J. Gerontol. 46, M196–M203 (1991).
Hoehn, M. M. & Yahr, M. D. Parkinsonism: onset, progression, and mortality. 17 (1967).
Mds, T., Goetz, C. G., Poewe, W., Rascol, O. & Christina, S. State of the Art Review The Unified Parkinson’ s Disease Rating Scale (UPDRS): Status and Recommendations. Society 18, 738–750 (2003).
Hughes, A. J., Daniel, S. E., Ben‐Shlomo, Y. & Lees, A. J. The accuracy of diagnosis of parkinsonian syndromes in a specialist movement disorder service. Brain 125, 861–870 (2002).
Brucki, S. M. D., Nitrin, R., Caramelli, P., Bertolucci, P. H. F. & Okamoto, I. H. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq. Neuropsiquiatr. 61, 777–781 (2003).
Hausdorff, J. M. et al. Rhythmic auditory stimulation modulates gait variability in Parkinson’s disease. Eur. J. Neurosci. 26, 2369–2375 (2007).
Camicioli, R., Bouchard, T. & Licis, L. Dual-tasks and walking fast: Relationship to extra-pyramidal signs in advanced Alzheimer disease. J. Neurol. Sci. 248, 205–209 (2006).
Simieli, L. et al. Obstacle crossing with dual tasking is a danger for individuals with Alzheimer’s disease and for healthy older people. J. Alzheimer’s Dis. 43, 435–441 (2015).
Roemmich, R. T. et al. Spatiotemporal variability during gait initiation in Parkinson’s disease. Gait Posture 36, 340–343 (2012).
Kang, H. G. & Dingwell, J. B. Dynamics and stability of muscle activations during walking in healthy young and older adults. J. Biomech. 42, 2231–2237 (2009).
Mohagheghi, A. A., Moraes, R. & Patla, A. E. The effects of distant and on-line visual information on the control of approach phase and step over an obstacle during locomotion. Exp. Brain Res. 155, 459–468 (2004).
Patla, A. E. How Is Human Gait Controlled by Vision. Ecol. Psychol. 10, 287–302 (1998).
Lo, O. Y., van Donkelaar, P. & Chou, L. S. Distracting visuospatial attention while approaching an obstacle reduces the toe-obstacle clearance. Exp. Brain Res. 233, 1137–1144 (2015).
Acknowledgements
The author thanks to FAPESP #2014/20549-0 – Fundação de Amparo à Pesquisa do Estado de São Paulo.
Author information
Authors and Affiliations
Contributions
L.S. Conception of the manuscript rationale, acquisition of all gait parameters and analysis of data, preparation and correction of the manuscript; F.A.B. Guidance about the acquisition and analysis of data, preparation and correction of the manuscript; D.O.S. Acquisition of Kinematics and clinical parameters; assistance in the preparation of the figure and tables and correction of the manuscript; E.L.S. Assistance in the acquisition of data and correction of the manuscript; V.S.B. Assistance in the acquisition of data and correction of the manuscript; P.C.R.S. Assistance in the acquisition of data and correction of the manuscript; L.T.B.G. Preparation and correction of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Simieli, L., Barbieri, F.A., Orcioli-Silva, D. et al. Variability of crossing phase in older people with Parkinson’s disease is dependent of obstacle height. Sci Rep 8, 14852 (2018). https://doi.org/10.1038/s41598-018-33312-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-33312-2
Keywords
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
