
Abstract
Real-world data regarding the effectiveness and safety of generic sofosbuvir (SOF)-based interferon-free direct acting antiviral agents (DAAs) for patients with chronic hepatitis C virus (HCV) infection remain limited. A total of 517 chronic HCV-infected patients receiving 12 or 24 weeks of SOF-based therapies were retrospectively enrolled in 4 academic centers in Taiwan. The rate of sustained virologic response at week 12 off-therapy (SVR12) and that of treatment completion were assessed. The baseline characteristics and on-treatment HCV viral kinetics to predict SVR12 were analyzed. By evaluable population (EP) analysis, the SVR12 rate was 95.4% (95% confidence interval [CI]: 93.2–96.9%). The SVR12 was achieved in 29 of 34 patients (85.3%, 95% CI: 69.6–93.6%), 130 of 139 patients (93.5%, 95% CI: 88.2–96.6%), 119 of 124 patients (96.0%, 95% CI: 90.9–98.3%) and 215 of 220 patients (97.7%, 95% CI: 94.8–99.0%) who received SOF in combination with ribavirin (RBV), ledipasvir (LDV), daclatasvir (DCV) and velpatasvir (VEL), respectively. Of 517 patients, 514 (99.4%) completed the scheduled treatment. All 15 patients with true virologic failures were relapsers. Two decompensated cirrhotic patients had on-treatment deaths which were not related to DAAs. All 7 patients who were lost to follow-up had undetectable HCV RNA level at the last visit. The SVR12 rates were comparable in terms of baseline patient characteristics and viral decline at week 4 of treatment. In conclusion, generic SOF-based regimens are well tolerated and provide high SVR12 rates in patients with chronic HCV infection.
Similar content being viewed by others

Introduction
Hepatitis C virus (HCV) infection remains a challenging health problem in the world. It is estimated that approximately 71.1 million people, which account for 1.0% of the world’s population, are HCV carriers1. Among patients with chronic HCV infection, about 20% of them will evolve to cirrhosis over a period of 20–30 years. Once cirrhosis is established, the annual rates of developing hepatic decompensation and hepatocellular carcinoma (HCC) are 3–6% and 1–4%, respectively2,3. In addition to increasing the risks of liver-related morbidity and mortality, HCV infection is also associated with various extra-hepatic manifestations which further compromised the patients’ health outcome and quality of life4. On the other hand, the morbidity and mortality are significantly reduced once these patients achieve sustained virologic response (SVR) by anti-HCV agents5,6,7,8,9.
The use of interferon (IFN)-free direct acting antiviral agents (DAAs) has made a paradigm shift and become the standard of care for HCV infection. Sofosbuvir (SOF) is a pyrimidine nucleotide analogue that inhibits the HCV non-structural protein 5B (NS5B) ribonucleic acid (RNA)-dependent RNA polymerase, which is essential for viral replication. After intra-hepatic metabolism to active uridine triphosphate form, the GS-461203, it is incorporated to HCV RNA by NS5B polymerase and acts as the chain terminator10. Clinically, SOF is administered once-daily with pangenotypic potency, well tolerability, a high genetic barrier to drug resistance, and low rates of drug-drug interactions (DDIs). Furthermore, SOF can be used in combination with various kinds of NS3/4 A protease inhibitors (PIs), NS5A inhibitors, and/or ribavirin (RBV) to achieve high SVR rates11,12,13,14,15,16,17,18,19,20,21,22,23. Because of the excellent therapeutic profiles, treatment of HCV by SOF-based regimens is appealing to most health care providers.
Although SOF-based IFN-free DAAs are highly efficacious and well tolerated, many HCV-infected individuals have limited governmental reimbursement or private insurance support for brand-name agents24,25,26. Allowing generic SOF-based DAAs through voluntary or compulsory licensing can scale up the HCV treatment to facilitate more efficient HCV control, particularly for patients in resource-constrained countries. Regarding the effectiveness and safety of generic SOF in combination with ledipasvir (LDV), daclatasvir (DCV), and/or RBV, several reports from China, India, Egypt and Argentina indicated that the SVR rates were >90% and most patients tolerated the treatment well27,28,29,30,31. On the basis of these encouraging results, we aimed to evaluate the performance of generic SOF-based DAAs for HCV and factors potentially affecting the treatment response in a multicenter cohort in Taiwan.
Materials and Methods
Patients
Between May 2016 and June 2017, HCV-infected patients who received generic SOF-based IFN-free therapies for 12 or 24 weeks at the National Taiwan University Hospital (NTUH), NTUH Yun-Lin Branch, Taichung Veterans General Hospital, and Cathay General Hospital Medical Center were retrospectively enrolled. All patients were aged ≥20 years and had chronic HCV infection, defined as detectable HCV antibody (anti-HCV; Abbott HCV EIA 2.0, Abbott Laboratories, Abbott Park, Illinois, USA) and quantifiable serum HCV RNA (Cobas TaqMan HCV Test v2.0, Roche Diagnostics GmbH, Mannheim, Germany, lower limit of detection [LLOD]: 15 IU/mL) for ≥6 months. Patients were excluded from the study if they had a history of DAA exposure, had estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2, had active HCC, received antiviral regimens not recommended by American Association for the Study of Liver Diseases/Infectious Diseases Society of America (AASLD/IDSA), European Association for the Study of the Liver (EASL) or Asian Pacific Association for the Study of the Liver (APASL) guidelines, or refused to provide written informed consent32,33,34. The study was approved by the Research Ethics Committee of National Taiwan University Hospital, Taichung Veterans Hospital and Cathay General Hospital and was conducted in accordance with the principles of Declaration of Helsinki and the International Conference on Harmonization for Good Clinical Practice. All patients provided written informed consent before the study.
Study design
Baseline demographic data, hemogram, serum biochemical profiles (albumin, total bilirubin, aspartate aminotransferase [AST], alanine aminotransferase [ALT], creatinine, eGFR, as calculated by modification of diet in renal disease equation (MDRD), anti-HCV, hepatitis B virus (HBV) surface antigen (Abbott Architect HBsAg qualitative assay, Abbott Laboratories, Abbott Park, Illinois, USA), HCV RNA, HCV genotype (Abbott RealTime HCV Genotype II, Abbott Laboratories, Abbott Park, Illinois, USA) and anti-HIV (Abbott Architect HIV Ag/Ab Combo, Abbott Laboratories, Abbott Park, Illinois, USA) were collected for all patients35. The cirrhosis status was determined by liver biopsy, clinical signs of portal hypertension, imaging studies, AST-to-platelet ratio index (ARPI) at a cutoff value of >2.0 or liver stiffness measurement (LSM, FibroScan®, Echosens, Paris, France) at a cutoff value of >12.5 kPa when appropriate36. In cirrhotic patients, the severity was graded by Child-Pugh score. Baseline serum HBV DNA (Cobas AmpliPrep/Cobas Taqman HBV test v.2.0, Roche Diagnostics GmbH, Mannheim, Germany, LLOD: 20 IU/mL) or HIV RNA (Cobas AmpliPrep/Cobas Taqman HIV-1 test v.2.0, Roche Diagnostics GmbH, Mannheim, Germany, LLOD: 20 copies/mL) level was determined for patients with HBV or HIV coinfection.
Patients received SOF in combination with RBV, LDV, DCV or velpatasvir (VEL) for 12 or 24 weeks. For SOF/RBV regimen, they received a generic version of SOF (400 mg/tablet; Hepcinat®, Natco Pharma Ltd., Hyderabad, India; Sofovir®, Hetero Corporate Ltd., Hyderabad, India) 1 tablet per day in combination with weight-based RBV (Robatrol®, 200 mg capsule, Genovate Biotechnology Co. Ltd., Hsinchu, Taiwan; 1,200 mg per day if the body weight ≥75 kg; 1,000 mg per day if the body weight <75 kg). For SOF/NS5A inhibitor regimens, they received a generic version of fixed-dose combination SOF/LDV (400/90 mg tablet; Hepcinat-LP®, Natco Pharma Ltd., Hyderabad, India; Ledifos®, Hetero Corporate Ltd., Hyderabad, India), SOF/DCV (400/60 mg tablet; Darvoni®, Beacon Pharmaceuticals Ltd. Mymensingh, Bangladesh) or SOF/VEL, (400/100 mg tablet; Velpanat®, Natco Pharma Ltd., Hyderabad, India; Velasof®, Hetero Corporate Ltd., Hyderabad, India; MyHep All®, Mylan Laboratories Ltd., Hyderabad, India; Sofosvel®, Beacon Pharmaceuticals Ltd. Mymensingh, Bangladesh) 1 tablet per day with or without weight-based RBV.
Effectiveness
Patients received on-treatment serum HCV RNA testing at weeks 4 and 12. For patients receiving 12 and 24 weeks of treatment, serum HCV RNA levels were assessed at treatment weeks 12 and 24 to determine antiviral responses at end-of-treatment (EOT). Furthermore, they received off-therapy serum HCV RNA testing at week 12 to assess SVR12. If patients prematurely discontinued treatment, the antiviral response at EOT was assessed at the time of last visit. Patients were considered failure to achieve SVR12 if they lacked SVR12 data. We adopted two different endpoints for effectiveness: the evaluable population (EP) which assessed the SVR12 for patients who received at least one dosage of treatment were included in the analysis, and the per-protocol population (PP) which assessed the SVR12 by excluding non-SVR12 patients due to non-virologic failure.
Safety
The rate of treatment completion was assessed for each regimen. The reasons for patients who were lost to follow-up were recorded by the treating physicians. In patients who were seropositive for HBsAg, serum HBV DNA levels were evaluated after the initiation of DAA treatment. HBV reactivation was defined as the presence of HBV DNA level ≥LLOD in patients with baseline HBV DNA level <LLOD, or increase of HBV DNA level >1 log10 IU/mL in patients with baseline HBV DNA level ≥LLOD37. HBV-associated hepatitis was defined as HBV reactivation and hepatitis flare presenting with ALT increase ≥3 times baseline and >100 U/L38.
Statistical analysis
All analyses were performed using Statistical Program for Social Sciences (SPSS Statistics Version 23.0, IBM Corp., Armonk, New York, USA). The baseline characteristics were shown in median (range) and percentages when appropriate. The viral responses during and after treatment were shown in number and percentages with 95% confidence interval (CI). The stratified analysis of SVR12 by baseline characteristics and week 4 viral decline were assessed and shown in percentages with 95% CI.
Results
Patient characteristics
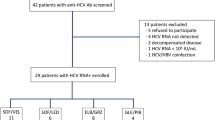
Of 593 HCV-infected patients receiving SOF-based IFN-free DAAs, 76 were excluded from the study because of prior DAA exposure, eGFR < 30 mL/min/1.73 m2, receiving antiviral regimens not recommended by guidelines, or refusal to provide informed consent. The remaining 517 patients were eligible for the analysis (Fig. 1). Table 1 shows the baseline patient characteristics. Thirty-four (6.6%), 139 (26.9%), 124 (24.0%) and 220 (42.6%) patients receiving SOF in combination with RBV, LDV, DCV and VEL, respectively. Patients receiving SOF/VEL tended to be younger, have a higher percentage of HIV-coinfected patients and a lower percentage of cirrhosis, compared to those receiving other SOF-based regimens. Among patients receiving SOF in combination with NS5A inhibitor, those receiving SOF/LDV tended to have a higher percentage of combining RBV usage, compared to those receiving SOF/DCV or SOF/VEL. All patients receiving SOF/RBV were infected with HCV genotype 2 (HCV-2) and were treated for 12 weeks, whereas all receiving SOF/LDV were infected with HCV-1a, HCV-1b or HCV-6. Sixty-nine (55.6%), one (0.8%), two (1.6%) and two (1.6%) receiving SOF/DCV had HCV-2, HCV-3, HCV-6, and mixed HCV genotype 1b + 2 and 2 + 6 infections. Patients receiving SOF/VEL had HCV-1 to 6 infection. One HCV viremic patient with indeterminate genotyping received SOF/VEL. No patients receiving SOF/RBV had decompensated cirrhosis. Among patients with HBV or HIV coinfection, 60–75% and 94.4–100% of them had baseline undetectable HBV DNA or HIV RNA levels.

Study flow.
Effectiveness
At week 4 of treatment, 30 of 34 (88.2%; 95% CI: 73.4–95.3%), 125 of 138 (90.6%; 95% CI: 84.6–94.4%), 112 of 114 (90.3%; 95% CI: 83.8–94.4%) and 196 of 220 (89.1%; 95% CI: 84.3–92.6%) patient receiving SOF in combination with RBV, LDV, DCV and VEL had undetectable serum HCV RNA level, respectively. Overall, 463 of 516 (89.7%; 95% CI: 86.8–92.1%) patients and 516 of 517 (99.8%; 95% CI: 98.9–100%) patients had undetectable serum HCV RNA levels at week 4 of treatment and at the end-of-treatment. One Child-Pugh C cirrhotic patient receiving SOF/LDV plus RBV died at treatment day 12 and the HCV RNA level at treatment week 1 was 1,047 IU/mL. The overall SVR12 rates were 95.4% (493 of 517 patients; 95% CI: 93.2–96.9%) by EP analysis, and 97.1% (493 of 508 patients; 95% CI: 95.2–98.2%) by PP analysis. The SVR12 rates for patients receiving SOF in combination with RBV, LDV, DCV, and VEL were 85.3% (95% CI: 69.9–93.6%), 93.5% (95% CI: 88.2–96.6%), 96.0% (95% CI: 90.9–98.3%) and 97.7% (95% CI: 94.8–99.0%) by EP analysis, and were 87.9% (95% CI: 72.7–95.2%), 96.3% (95% CI: 91.6–98.4%), 96.8% (95% CI: 91.9–98.7%) and 99.1% (95% CI: 96.7–99.8%) by PP analysis, respectively (Table 2).
Among patients who failed to achieved SVR12, 15 (2.9%) were relapsers and 9 (1.7%) were lost to follow-up. Among the 15 relapsers, 7 (46.7%) were male, 9 (60%) were treatment-naïve, and 10 (66.7%) had cirrhosis. Eight of the 9 (88.9%) patients who were lost to follow-up had HCV RNA level < LLOD at the last visit (Table 3).
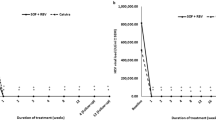
Among the 41 decompensated cirrhotic patients with available baseline and end of follow-up data, 32 (78%) and 9 (22%) of them had baseline Child-Pugh B and C. At the end of follow-up, 27 (66%), 12 (29%) and 2 (5%) of them had Child-Pugh A, B, and C, respectively (Fig. 2A). Regarding the scores for model for end-stage liver disease (MELD), 8 (20%), 3 (7%) and 30 (73%) of them had worsened, stable, and improved scores at the end of follow-up, as compared to the baseline status (Fig. 2B).

(A) Child-Pugh class shift in cirrhotic patients with baseline Child-Pugh B and C, (B) Changes of MELD scores from baseline. *Two patients who died during treatment were excluded from the analysis. MELD: model for end-stage liver disease.
Stratified analysis of baseline characteristics predictive of SVR12
Table 4 shows the stratified SVR12 rates of SOF-based DAA regimens by baseline characteristics and week 4 treatment response. The SVR12 rates were comparable with regard to age at a cut-off value of 55 years, sex, prior IFN exposure, HBV or HIV coinfection, prior history of HCC, scheduled 12 or 24 weeks of treatment, use of RBV, BMI at a cut-off value of 25 kg/m2, ALT quotient at a cut-off of 2, eGFR at a cut-off value of 60 mL/min/1.73 m2, baseline HCV viral load at a cut-off value of 6,000,000 IU/mL, HCV genotype, cirrhosis and week 4 viral decline in patients receiving SOF-based regimens. The SVR12 rates for compensated cirrhotic and decompensated cirrhotic patients were 95.5% (95% CI: 84.9–98.7%) and 80.0% (95% CI: 58.4–91.9%) receiving SOF/LDV, 89.7% (95% CI: 76.4–95.9%) and 100% (95% CI: 74.1–100%) receiving SOF/DCV, and 93.2% (95% CI: 81.8–97.7%) and 100% (95% CI: 75.8–100%) receiving SOF/VEL. In addition, the SVR12 was achieved in 42 of 45 (93.3%; 95% CI: 82.1–97.7%) patients with a prior history of HCC and in 451 of 472 (95.6%; 95% CI: 93.3–97.1%) patients without a prior history of HCC.
Safety
Five hundred fourteen of 517 (99.4%) patients completed the scheduled treatment. One Child-Pugh C and one Child-Pugh B cirrhotic patients receiving SOF/LDV plus RBV died at treatment day 12 and week 11 due to spontaneous bacterial peritonitis, respectively. One Child-Pugh A cirrhotic patient receiving SOF/VEL declined treatment after week 8 and another 6 patients declined off-therapy follow-ups. The reasons for lost to follow-up in the 7 patients were not related to DAA treatment (Table 3). Among the 41 HCV-infected patients with HBV coinfection, 9 (22.0%) also had HIV coinfection. All the 9 patients received tenofovir (TDF)-based antiretroviral agents (ARTs) and none had baseline detectable serum HBV DNA level or had HBV reactivation after DAA treatment. Nineteen of 32 (59.4%) HBV/HCV-coinfected patients without HIV infection had baseline undetectable serum HBV DNA level; 13 (40.6%) had detectable serum HBV DNA levels (range: 25 to 1,820 IU/mL). All the 32 patients did not receive oral nucleos(t)ide analogues or peginterferon for HBV prior to DAA treatment. Eighteen (56.3%) patients met the virologic criteria for HBV reactivation after the initiation of DAA treatment. One (3.1%) patient receiving SOF/LDV developed HBV-associated hepatitis at week 8 of treatment. The baseline HBV DNA level was 1,540 IU/mL, which peaked to 54,200 IU/mL at week 8 of treatment. The ALT level was 192 U/L and the serum HCV RNA level was <LLOD at the time of HBV reactivation. No concomitant serum total bilirubin level elevation or signs of hepatic decompensation was present. The patient received entecavir at week 9 and the ALT level normalized after 7 weeks of treatment.
Discussion
Compared to PI-containing HCV DAA regimens such as paritaprevir/ritonavir, ombitasvir plus dasabuvir (PrOD), elbasvir/grazoprevir (EBR/GZR), or daclatasvir/asunaprevir (DCV/ASV), PI-free SOF-based regimens have relatively lower pill burden, broader genotype/subtype coverage, fewer drug-drug interactions (DDIs), and can be applied to patients with decompensated cirrhosis11,12,13,14,15,16,17,18,19,39. Although the newly developed glecaprevir/pibrentasvir (GLE/PIB) and voxilaprevir (VOX)/SOF/VEL are potent regimens with pangenotypic activity, they are contraindicated for decompensated cirrhotic patients. Therefore, PI-free SOF-based regimens are appealing choices to health care providers for treating HCV infection.
Our study showed that the overall SVR12 rate in patients receiving generic SOF in combination with RBV or NS5A inhibitors was excellent (95.4%) and was comparable to the response rates in patients receiving brand-name agents12,13,14,15,16,17,18,19,20,21,22,23. The per-protocol SVR12 rate was 97.1% after excluding patients with non-virologic failure. Regarding safety, >99% of our patients completed the scheduled treatment. Only 2 decompensated cirrhotic patients prematurely discontinued treatment due to spontaneous bacterial peritonitis, which were considered not related to DAA usage.
In our patients receiving SOF/RBV, all were infected with HCV-2, which reflected the potential suboptimal response rates in patients infected with other genotypes. The SVR12 rate for SOF/RBV in our study was 85.3%, which was comparable to the response rates in clinical trials12,13. Although there were no statistical differences for SVR12 rates by baseline patient characteristics, our data were in line with VALENCE study that the CIs of the response rates varied widely, probably due to the small case numbers in both studies13. In HCV-2 cirrhotic patients receiving SOF/RBV for 12 weeks, the SVR12 rates in FUSION and VALENCE trials as well as Western real-world practice were 60–82%12,13,40. However, the SVR12 rate in our HCV-2 cirrhotic patients was higher (88.2%) than Western reports and was comparable to the response rates in East-Asian trials41,42,43. The factors attributed to the superior response rates in East-Asian patients to Western patients are still unknown. Furthermore, whether extending the treatment to 16 weeks could achieve better response rates in our HCV-2 cirrhotic patients needs further evaluation12,44.
The SVR12 rate of our patients receiving generic SOF/LDV-based therapies was 93.5%, which was comparable to the response rates in patients receiving brand-name agents14,15,16,17. Further analysis showed that our patients had similar SVR12 rates to the phase II and III clinical trials by cirrhosis or genotype/subtype status14,15,16,17,45. Furthermore, the SVR12 rates in our patients receiving SOF/LDV-based therapy were comparable irrespective of baseline patient characteristics, implying the use of generic SOF/LDV can also achieve excellent effectiveness.
About 66.5% of our patients were treated by generic SOF/DCV or SOF/VEL, probably due to the pangenotypic potency and relatively low pill burden compared to SOF/RBV or SOF/LDV46. The SVR12 rates in our patients receiving generic SOF/DCV and SOF/VEL-based therapies were excellent and were comparable to the phase III clinical trials and real-world reports18,19,20,21,47. Of 23 decompensated cirrhotic patients receiving generic SOF/DCV or SOF/VEL with RBV for 12 weeks, or SOF/DCV or SOF/VEL without RBV for 24 weeks, all achieved SVR12, indicating these agents still had good therapeutic effects in critically ill patients. Furthermore, the response rates remained excellent in patients with unfavorable baseline characteristics. Our data indicated that generic SOF/DCV or SOF/VEL also had similar effectiveness to brand-name agents.
Regarding our 43 decompensated cirrhotic patients, 39 (90.7%) of them achieved SVR12 by generic SOF-based DAA therapies. Most patients had improving Child-Pugh class and MELD scores following treatment, implying that the mortality and morbidity can potentially be reduced in these very sick patients.
Among our 32 HBV/HCV coinfected patients not receiving antiviral agents for HBV, the risk of HBV reactivation and the HBV-related hepatitis after generic SOF-based therapies were similar to a recent prospective cohort enrolling 101 HBV/HCV coinfected patients receiving brand-name SOF/LDV, indicating that applying generic DAAs may not increase the risk of HBV reactivation and its associated complication48. However, watchful surveillance of HBV activity is still needed to detect and treat HBV-related hepatitis and hepatic decompensation earlier.
Our data showed that the rates of HCV RNA level < LLOD at week 4 of treatment were 88.2–90.3% in patients receiving SOF-based regimens. Although about 10% of our patients remained viremic at week 4 of treatment, the SVR12 rates were comparable to those who were aviremic at week 4 of treatment. Therefore, the early virokinetics plays a minor role in predicting SVR12 in patients receiving generic SOF-based therapies49,50. Furthermore, our data was also in accordance with a recent meta-analysis that the SVR12 rates of SOF-based therapies were comparable in Asian patients with or without history of HCC51.
In addition to the excellent safety profiles and effectiveness, the prices of generic SOF-based DAA therapies are about 1–2% of the brand-name agents52. Based on these advantages, the use of generic SOF-based IFN-free DAA regimens may facilitate the mass treatment and play an important role in the elimination of HCV infection in the world, particularly in resource-constrained countries53. However, prudential assessment of severity of hepatic fibrosis, particularly for hepatic decompensation, and HCV genotype are still needed to optimize the treatment strategies.
Although generic SOF-based IFN-free DAAs had excellent safety and effectiveness, several limitations existed in our study. First, we included patients with different characteristics and the direct comparison of effectiveness and safety for each SOF-based regimen was not feasible. Second, the generic DAAs were made by various pharmaceutical companies and the direct comparison of effectiveness and safety was difficult. Third, data regarding the on-treatment constitutional or laboratory adverse events were not available in our retrospective study, making the detailed safety analysis impossible.
In summary, generic SOF-based IFN-free regimens achieved comparably excellent effectiveness and safety to the brand-name agents. These regimens may improve the care of HCV for patients with limited access to the expensive brand-name agents.
References
Polaris Observatory HCV Collaborators Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. Lancet. Gastroenterol. Hepatol. 2, 161–176 (2017).
Kao, J. H. Hepatitis C virus infection in Taiwan: Past, present, and future. J. Formos. Med. Assoc. 115, 65–66 (2016).
Liu, C. H. & Kao, J. H. Nanomedicines in the treatment of hepatitis C virus infection in Asian patients: optimizing use of peginterferon alfa. Int. J. Nanomedicine. 9, 2051–2067 (2014).
Lee, M. H. et al. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. J. Infect. Dis. 206, 469–477 (2012).
van der Meer, A. J. et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 308, 2584–2593 (2012).
Morgan, R. L. et al. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann. Intern. Med. 158, 329–337 (2013).
Nahon, P. et al. Eradication of hepatitis C virus infection in patients with cirrhosis reduces risk of liver and non-liver complications. Gastroenterology. 152, 142–156.e2 (2017).
Hsu, Y. C. et al. Association between antiviral treatment and extrahepatic outcomes in patients with hepatitis C virus infection. Gut. 64, 495–503 (2015).
Mahale, P. et al. The effect of sustained virological response on the risk of extrahepatic manifestations of hepatitis C virus infection. Gut. 67, 553–561 (2018).
Keating, G. M. Sofosbuvir: a review of its use in patients with chronic hepatitis C. Drugs. 74, 1127–1146 (2014).
Lawitz, E. et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N. Engl. J. Med. 368, 1878–1887 (2013).
Jacobson, I. M. et al. Sofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment options. N. Engl. J. Med. 368, 1867–1877 (2013).
Zeuzem, S. et al. Sofosbuvir and ribavirin in HCV genotypes 2 and 3. N. Engl. J. Med. 370, 1993–2001 (2014).
Afdhal, N. et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N. Engl. J. Med. 370, 1889–1898 (2014).
Afdhal, N. et al. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N. Engl. J. Med. 370, 1483–1493 (2014).
Charlton, M. et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology. 149, 649–659 (2015).
Manns, M. et al. Ledipasvir and sofosbuvir plus ribavirin in patients with genotype 1 or 4 hepatitis C virus infection and advanced liver disease: a multicentre, open-label, randomised, phase 2 trial. Lancet. Infect. Dis. 16, 685–697 (2016).
Sulkowski, M. S. et al. Daclatasvir plus sofosbuvir for previously treated or untreated chronic HCV infection. N. Engl. J. Med. 370, 211–221 (2014).
Feld, J. J. et al. Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. N. Engl. J. Med. 373, 2599–2607 (2015).
Foster, G. R. et al. Sofosbuvir and velpatasvir for HCV genotype 2 and 3 infection. N. Engl. J. Med. 373, 2608–2617 (2015).
Curry, M. P. et al. Sofosbuvir and velpatasvir for HCV in patients with decompensated cirrhosis. N. Engl. J. Med. 373, 2618–2628 (2015).
Jacobson, I. M. et al. Efficacy of 8 weeks of sofosbuvir, velpatasvir, and voxilaprevir in patients with chronic HCV infection: 2 phase 3 randomized trials. Gastroenterology. 153, 113–122 (2017).
Bourlière, M. et al. Sofosbuvir, velpatasvir, and voxilaprevir for previously treated HCV infection. N. Engl. J. Med. 376, 2134–2146 (2017).
Freeman, J. A. & Hill, A. The use of generic medications for hepatitis C. Liver. Int. 36, 929–932 (2016).
Ghinea, N. et al. Importation of generic hepatitis C therapies: bridging the gap between price and access in high-income countries. Lancet. 389, 1268–1272 (2017).
Lim, S. G. HCV management in resource-constrained countries. Hepatol. Int. 11, 245–254 (2017).
Zeng, Q. L. et al. Generic ledipasvir-sofosbuvir for patients with chronic hepatitis C: A real-life observational study. J. Hepatol. 66, 1123–1129 (2017).
Hill, A. et al. High sustained virological response rates using imported generic direct acting antiviral treatment for hepatitis C. J. Virus. Erad. 3, 200–203 (2017).
Omar, H. et al. Generic daclatasvir plus sofosbuvir, with or without ribavirin, in treatment of chronic hepatitis C: real-world results from 18 378 patients in Egypt. Aliment. Pharmacol. Ther. 47, 421–431 (2018).
Marciano, S. et al. Effectiveness and safety of original and generic sofosbuvir for the treatment of chronic hepatitis C: A real world study. J. Med. Virol. 90, 951–958 (2018).
Gupta, S. et al. Efficacy of generic oral directly acting agents in patients with hepatitis C virus infection. J. Viral. Hepat. 25, 771–778 (2018).
AASLD/IDSA HCV Guidance Panel Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 62, 932–954 (2015).
European Association for Study of Liver. EASL Clinical Practice Guidelines: management of hepatitis C virus infection. J. Hepatol. 60, 392–420 (2014).
Omata, M. et al. APASL consensus statements and recommendation on treatment of hepatitis C. Hepatol. Int. 10, 702–726 (2016).
Liu, C. H. et al. Comparison of Abbott RealTime HCV Genotype II with Versant Line Probe Assay 2.0 for hepatitis C virus genotyping. J. Clin. Microbiol. 53, 1754–1757 (2015).
Liu, C. H. et al. A noninvasive diagnosis of hepatic fibrosis by BioFibroScore® in chronic hepatitis C patients. J. Gastroenterol. Hepatol. 33, 291–297 (2018).
Liu, C. H. et al. Hepatitis B virus reactivation in patients receiving interferon-free direct-acting antiviral agents for chronic hepatitis C virus infection. Open. Forum. Infect. Dis. 4, ofx028 (2017).
Terrault, N. A. et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 67, 1560–1599 (2018).
Liu, C. H. et al. Real-world effectiveness and safety of paritaprevir/ritonavir, ombitasvir, and dasabuvir with or without ribavirin for patients with chronic hepatitis C virus genotype 1b infection in Taiwan. J. Gastroenterol. Hepatol. 33, 710–717 (2018).
Welzel, T. M. et al. Effectiveness and safety of sofosbuvir plus ribavirin for the treatment of HCV genotype 2 infection: results of the real-world, clinical practice HCV-TARGET study. Gut. 66, 1844–1852 (2017).
Omata, M. et al. Sofosbuvir plus ribavirin in Japanese patients with chronic genotype 2 HCV infection: an open-label, phase 3 trial. J. Viral. Hepat. 21, 762–768 (2014).
Kao, J. H. et al. A phase 3b study of sofosbuvir plus ribavirin in Taiwanese patients with chronic genotype 2 hepatitis C virus infection. Liver. Int. 36, 1101–1107 (2016).
Ahn, S. H. et al. A phase 3b study of sofosbuvir plus ribavirin in treatment-naive and treatment-experienced Korean patients chronically infected with genotype 2 hepatitis C virus. J. Viral. Hepat. 23, 358–365 (2016).
Mangia, A. et al. Sofosbuvir and ribavirin for genotype 2 HCV infected patients with cirrhosis: A real life experience. J. Hepatol. 66, 711–717 (2017).
Gane, E. J. et al. Efficacy of ledipasvir and sofosbuvir, with or without ribavirin, for 12 weeks in patients with HCV genotype 3 or 6 infection. Gastroenterology. 149, 1454–1461.e1 (2015).
Liu, C. H. et al. Generic velpatasvir plus sofosbuvir for hepatitis C virus infection in patients with or without human immunodeficiency virus coinfection. Aliment. Pharmacol. Ther. 47, 1690–1698 (2018).
Welzel, T. M. et al. Daclatasvir plus sofosbuvir, with or without ribavirin, achieved high sustained virological response rates in patients with HCV infection and advanced liver disease in a real-world cohort. Gut. 65, 1861–1870 (2016).
Liu, C. J. et al. Efficacy of ledipasvir and sofosbuvir treatment of HCV infection in patients coinfected with HBV. Gastroenterology. 154, 989–997 (2018).
Maasoumy, B. et al. Clinical value of on-treatment HCV RNA levels during different sofosbuvir-based antiviral regimens. J. Hepatol. 65, 473–482 (2016).
Fourati, S. et al. Viral kinetics analysis and virological characterization of treatment failures in patients with chronic hepatitis C treated with sofosbuvir and an NS5A inhibitor. Aliment. Pharmacol. Ther. 47, 665–673 (2018).
Ji, F. et al. Systematic review with meta-analysis: effectiveness and tolerability of interferon-free direct-acting antiviral regimens for chronic hepatitis C genotype 1 in routine clinical practice in Asia. Aliment. Pharmacol. Ther. 47, 550–562 (2018).
van de Ven, N. et al. Minimum target prices for production of direct-acting antivirals and associated diagnostics to combat hepatitis C virus. Hepatology. 61, 1174–1182 (2015).
Elsharkawy, A. et al. Planning and prioritizing direct-acting antivirals treatment for HCV patients in countries with limited resources: Lessons from the Egyptian experience. J. Hepatol. 68, 691–698 (2018).
Acknowledgements
The authors thank Hui-Ju Lin and Po-Chung Liu for clinical data management; the 7th Core Lab of National Taiwan University Hospital and the 1st Common Laboratory of National Taiwan University Hospital, Yun-Lin Branch for instrumental and technical support. This work was supported by Ministry of Science and Technology, Taiwan (106-2314-B-002-138-MY3).
Author information
Authors and Affiliations
Contributions
Conception and design: C.H. Liu, S.S. Yang, J.H. Kao. Analysis and interpretation of data: C.H. Liu. Drafting of the article: C.H. Liu, J.H. Kao. Critical revision of the article for important intellectual content: C.H. Liu, Y.J. Huang, S.S. Yang, C.H. Chang, S.S. Yang, H.Y. Sun, C.J. Liu, W.C. Liu, T.H. Su, H.C. Yang, C.M. Hong, T.C. Tseng, P.J. Chen, D.S. Chen, C.C. Hung, J.H. Kao. Final approval of the article: C.H. Liu, Y.J. Huang, S.S. Yang, C.H. Chang, S.S. Yang, H.Y. Sun, C.J. Liu, W.C. Liu, T.H. Su, H.C. Yang, C.M. Hong, T.C. Tseng, P.J. Chen, D.S. Chen, C.C. Hung, J.H. Kao. Provision of study materials or patients: C.H. Liu, Y.J. Huang, S.S. Yang, C.H. Chang, S.S. Yang, H.Y. Sun, C.J. Liu, W.C. Liu, T.H. Su, H.C. Yang, C.M. Hong, T.C. Tseng, P.J. Chen, D.S. Chen, C.C. Hung, J.H. Kao. Statistical expertise: C.H. Liu Administrative, technical, or logistic support: J.H. Kao. Collection and assembly of data: C.H. Liu.
Corresponding author
Ethics declarations
Competing Interests
Chen-Hua Liu: advisory board for Abbvie, Gilead Science, Merck Sharp & Dohme; speaker’s bureau for Abbott, Abbvie, Gilead Science, Merck Sharp & Dohme; research grant from Abbvie, Gilead Science, Merck Sharp & Dohme. Jia- Horng Kao: advisory board for Abbott, Abbvie, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, Roche; speaker’s bureau for Abbott, Abbvie, Bayer, Bristol-Myers Squibb, Gilead Science, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, Roche; Ding-Shinn Chen: advisory board for Abbvie, Gilead Science, GlaxoSmithKline, Merck Sharp & Dohme, Novartis; Pei-Jer Chen: advisory board for Abbvie, Novartis, Roche; Chien-Ching Hung: advisory boards for Abbvie, Gilead Sciences, Janssen, ViiV;. Speaker’s bureau for Abbvie, Bristol-Myers Squibb, Gilead Sciences, ViiV; research grant from Gilead Sciences, Janssen, Merck, ViiV. All other authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, CH., Huang, YJ., Yang, SS. et al. Generic sofosbuvir-based interferon-free direct acting antiviral agents for patients with chronic hepatitis C virus infection: a real-world multicenter observational study. Sci Rep 8, 13699 (2018). https://doi.org/10.1038/s41598-018-32060-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-32060-7
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
