
Abstract
Periodontal biotype is used to describe the morphological characteristics of periodontal tissues and is closely related to periodontal health and prognosis of many dental treatments. This study was undertaken to explore the periodontal biotype distribution in a young Chinese population and to evaluate the accuracy of different methods for gingival thickness (GT) measurement. A total of 372 teeth from 31 periodontally healthy subjects were included. GT was measured simultaneously by probe transparency, transgingival probing and cone-beam computed tomography (CBCT). Some other anatomic parameters, including crown width/crown length ratio, attached gingival width, labial bone thickness and papilla volume were recorded for periodontal biotype classification. As found by probe transparency, the gingivae of 222 teeth (59.68%) were thick, while those of 150 teeth (40.32%) were thin. The mean GT of included subjects was 1.03 ± 0.31 mm as measured by transgingival probing and 1.03 ± 0.24 mm as measured by CBCT. Four groups were identified by cluster analysis. Thick-flap biotype, average-scalloped biotype, average-flap biotype and thin-scalloped biotype comprised 137 teeth (36.83%), 96 teeth (25.81%), 39 teeth (10.48%) and 100 teeth (26.88%), respectively. These results demonstrate that the most common periodontal biotype in this young Chinese population was the thick-flap type with low aesthetic risk.
Similar content being viewed by others


Introduction
Clinical appearance of gingiva differs from subject to subject and even among different teeth. It is closely related to periodontal health and the prognosis of many dental treatments. To describe the variation in gingival contour, “gingival biotype” was first proposed by Ochsenbein and Ross1. Then, Seibert and Lindhe introduced the term “periodontal biotype”, which classified the gingival contour into two categories, the “thick” and “thin” biotype, based on simple visual appearance of gingivae2. In 1997, Muller included some new parameters, such as tooth shape and gingival width, in his analysis of periodontal biotype3. De Rouck developed a new method for the classification of gingival biotype based on the following four clinical parameters: gingival thickness (GT), crown width/crown length ratio (CW/CL), gingival width and papilla height (PH). Then, three biotypes were identified: the thin-scalloped, thick-scalloped and thick-flat biotype4. Unfortunately, until now, there has been no unified criterion for periodontal biotype classification, although GT is undoubtedly the most important indicator of all for evaluation.
Many invasive and non-invasive methods have been employed to assess periodontal biotype. However, the most accurate method for periodontal biotype assessment and GT measurement has not yet been confirmed. Simple visual inspection was the first method developed to evaluate periodontal biotype, but it was not considered to be a reliable method by many researchers5,6. Transgingival probing is a traditional invasive method with limited application in clinic. Instead, another evaluation that is based on the transparency of the periodontal probe through the gingival margin is widely used and is taken as a simple method with excellent repeatability. Ultrasonic measurement and cone beam computerized tomography (CBCT) are also non-invasive methods, but special devices are needed for these assessments. Moreover, it was reported that the accuracy of GT measurement by ultrasonic instruments was worse than that by direct puncture7. Comparisons of different measurement methods based on the same sample are limited.
Some anatomic parameters, such as CW/CL, attached gingival width (AGW), PH, bone thickness (BT) and tooth site, were reported to be related to GT4,8,9. Different results of GT assessment and periodontal biotype exploration in different studies were also due to the included samples with different age, sex and racial characteristics3,4,8,10,11,12. Until recently, most research on periodontal biotype has been about Caucasians. In contrast, explorations in Chinese populations are limited.
The aim of the present study was to explore the periodontal biotype distribution in a young Chinese population and to evaluate the accuracy of different methods for GT measurement, including probe transparency, transgingival probing and CBCT.
Method and Materials
Subjects
This study was performed in compliance with the revised Helsinki Declaration and was approved by the Ethical Committee of Nanjing Medical University (Permit Number: 20160206). Written informed consent was obtained from all recruits.
A total of 31 periodontally healthy students in the College of Stomatology, Nanjing Medical University (aged between 18 and 27 years, mean age 22.2 years, 15 males and 16 females) were enrolled in this study from October 2016 to February 2017. Inclusion criteria were: (1) 18–30 years old; (2) no site with gingival index (GI) ≥1, probing depth (PD) >3 mm or clinical attachment loss (CAL) ≥1 mm and no radiographic evidence of alveolar bone loss; and (3) no malocclusion, crowding, missing or supernumerary anterior teeth. Exclusion criteria were: (1) crown restorations or fillings in anterior teeth; (2) previous orthodontic treatment; (3) previous periodontal surgery, including gingivectomy, flap surgery, guided tissue regeneration or periodontal plastic surgery; (4) systemic disease; (5) pregnancy and lactation; (6) use of any drugs that might lead to gingival enlargement during the past 6 months; (7) smoking; and (8) bruxism. All volunteers received oral hygiene instructions and a full-mouth supragingival scaling 1 week before clinical examination to control any possible gingival inflammation.
Clinical measurement
A total of 372 anterior teeth from 31 subjects, including upper and inferior anterior teeth, were involved in this study. Clinical periodontal parameters, including plaque index (PLI), GI, PD and CAL were recorded at six sites (mesial labial, midlabial, distal labial, mesial palatal, midpalatal and distal palatal) per tooth. All measurements were performed by a calibrated examiner.
For transgingival probing, local anesthesia (4% articaine) was applied over the gingiva of anterior teeth. To avoid mucous swelling due to local anesthesia, clinical measurements were taken 20 min after anesthesia. GT by transgingival probing (GTp) was determined at the level of the cementoenamel junction (CEJ) by piercing midfacial gingival with a #15 endodontic K-file (MANI, Tochigi, Japan), which had a rubber stop. Gingivae thicker than 0.8 mm were defined as thick, while others were categorized as thin13.
The following anatomic parameters were measured by a Williams probe (Hu-Friedy, IL, USA) to the nearest 0.5 mm:
-
(1)
CW/CL. Crown length was recorded as the distance between the incisal edge of the tooth and the free gingival margin, or if discernible, the CEJ. Crown width was the distance between the approximal tooth surfaces, which was measured at the border between the middle and the cervical third of the crown.
-
(2)
AGW was evaluated at the midfacial point by subtracting PD from keratinized gingival width, which was the distance from the free gingival margin to the mucogingival junction.
-
(3)
PH was defined as the distance from the tip of the papilla to a line connecting the midfacial soft tissue margin of two adjacent teeth.
Moreover, the visibility of a probe inserted through the gingival margin at the midfacial site of the tooth was also determined to assess periodontal biotype. If the outline of the probe could be seen through the gingiva, it was defined as thin. Otherwise, it was regarded as thick.
Radiographic measurement
To avoid the interference of surrounding soft tissues (lip and tongue), acrylic plates of maxillary and mandibular arches extending beyond the mucogingival junction were made, and zinc oxide–eugenol cement was loaded into it. Then, the plates were allowed to set intraorally during the process of CBCT examination.
CBCT scanning was performed using NewTom 5G (version FP, Verona, Italy). Exposure was performed at 110 kV in 4–5 mA for 3.6 s. Reconstructed images were generated, and digital measurements were taken using Mimics software (Materialise NV, Leuven, Belgium) with an accuracy of 0.01 mm. The following parameters were recorded: (1) GT in CBCT scanning (GTCT) was measured at the level of CEJ; (2) labial bone thickness (BT) was assessed at the midpoint of the root. The above-mentioned thickness measurements were conducted perpendicular to the midfacial surface of the tooth, as shown in Fig. 1; and (3) after 3D imaging reconstruction, gingival papilla volume (PV), which was defined by 14 points, was calculated automatically by Mimics software (Fig. 2).

Measurements of GTCT and BT in a cross-sectional image. GTCT and BT were measured perpendicular to the long axis of the tooth (a). GTCT at CEJ and BT at the midpoint of the root were measured at the midfacial surface in a cross-sectional image that passed through the long axis of the tooth (b).

3D imaging reconstruction and the measurements of PV. After CBCT scanning and 3D imaging reconstruction, interdental papilla was defined as a quadrangular pyramid outlined by 14 points (a). Points 1–6 were located in the mid-cross-sectional plane perpendicular to the connecting line of two neighbouring teeth (b). Points 7–10 were located at the free gingival margin in the proximal surfaces of the teeth (c). Points 11–14 were located in the cross-sectional image that passed through the long axis of the tooth and was perpendicular to labial surfaces (d).
Intra-examiner repeatability
All measurements were performed by one examiner (YMS). 10 volunteers randomly extracted from the total samples were reevaluated after1 month by the same clinician.
Statistical analysis
Statistical analysis of clinical and radiologic parameters, including GT, CW/CL, AGW, PH and BT, was performed using Student’s t-test. Spearman’s correlation coefficient was used to analyze the consistency of GT obtained by transgingival probing and CBCT, as well as the correlations of CW/CL, AGW, PH, BT, PV and GT. Agreement of probe transparency and GT measurements was analyzed by kappa test. Hierarchical cluster analysis (HCA) based on Euclidian distances of four parameters, including GTP, CW/CL, AGW and PV, was conducted to develop periodontal tissues typology more objectively. Before the parameters were put into HCA, they were standardized in order to ensure the same weight in the analysis. Differences in morphometric variables of the resultant clusters were analyzed by ANOVA, and the LSD test was used to compare differences between groups.
Data availability
The data generated and analyzed in this present study are available from the corresponding author upon reasonable request.
Results
Intra-examiner accuracy control
The accuracy and repeatability of the measurements were repeatedly evaluated in 10 volunteers. Pearson correlation coefficients were 0.92 (p < 0.001), 0.84 (p < 0.001), 0.94 (p < 0.001), 0.85 (p < 0.001), 0.76 (p < 0.001) and 0.72 (p < 0.001) for CW/CL, AGW, PH, GTP, GTCT and BT, respectively. Probe transparency also proved to be highly reproducible, with 86% agreement between duplicate measurements (k = 0.80, p < 0.05).
Clinical and radiographic parameters
Descriptive characteristics of 4 clinical parameters (CW/CL, AGW, PH and GTP) and 3 radiographic parameters (GTCT, BT and PV) are presented in Table 1. The mean CW/CL, AGW, PH, GTP, GTCT, BT and PV were 0.77, 5.37 mm, 4.34 mm, 1.03 mm, 1.03 mm, 0.67 mm and 75.21 mm3, respectively. Significant differences between males and females were found in CW/CL, GTP and BT (p < 0.05) and differences between maxillary and mandibular teeth were found in all of the 7 variables (p < 0.05) (Table 2).
Comparisons of GT measured by different methods
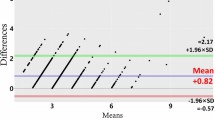
In this present research, GT was measured by transgingival probing, probe transparency and CBCT in each subject at the same time. Distribution of thick/thin gingiva as assessed by different methods is shown in Table 3. The Spearman’s correlation coefficient of GTP and GTCT was 0.40 (p < 0.001), which revealed a moderate correlation between these two methods. The kappa value of probe transparency and transgingival probing was 0.24 (p < 0.001), which indicated an unsatisfactory consistency. Moreover, no consistency was discovered between probe transparency and CBCT (k = 0.09, p = 0.051).
Correlation analysis of clinical and radiographic parameters
Correlation analysis was carried out to explore the factors closely related to periodontal biotype. A strong correlation between CW/CL and PV was revealed (p < 0.01, r = 0.554), while moderate correlations between CW/CL-AGW, CW/CL-GTP, AGW-GTP, AGW-GTCT, CTCT-GTP, PV-GTP, GTCT-PV and PV-PH were also found (p < 0.01, 0.3 < r ≤ 0.5). In addition, weak correlations existed between CW/CL-PH, CW/CL-GTCT, CW/CL-BT, AGW-BT, AGW-PV, PH-GTP, PH-BT, GTP-BT, GTCT-BT and BT-PV (p < 0.01, 0 < r ≤ 0.3). There was no significant correlation between AGW-PH and PH-GTCT (p > 0.05) (Table 4).
Cluster analysis
By HCA, four clusters of periodontal biotype were identified based on GTP, CW/CL, AGW and BT. Cluster A (thick-flap type), cluster B1 (average-scalloped type), cluster B2 (average-flap type) and cluster C (thin-scalloped type) included 137 teeth (36.83%), 96 teeth (25.81%), 39 teeth (10.48%) and 100 teeth (26.88%), respectively. Representative photographs of these four periodontal biotypes are presented in Fig. 3.

Representative photographs of the four periodontal biotypes. 11 in (a) 11 in (b) 11 in (c) and 22 in (d) were thick-flap, average-scalloped, average-flap and thin-scalloped biotype respectively.
Among the four groups, the GTP of cluster A was the thickest (p < 0.001), while that of cluster C was the thinnest (p < 0.001). No significant differences in GTP were found between cluster B2 and B1 (p > 0.05). The CW/CL of cluster B2 was significantly larger than those of the other groups (p < 0.001), which represented a quarter tooth shape. Similarly, the PVs of clusters A and B2 were much greater than those of clusters B1 and C (p < 0.001). Furthermore, the AGWs of clusters B1 and C were significantly smaller than those of the other two groups (p < 0.001) (Table 5).
Discussion
Periodontal biotype is closely related to the prognosis of many dental treatments, especially in the anterior aesthetic area. After implantation, periodontal therapy or orthodontic treatment, severe gingival recession may develop more easily in patients with a thin biotype, while deep periodontal pockets are more likely to form in persons with a thick biotype14. Therefore, it is important to identify periodontal biotype accurately in order to predict prognosis and avoid unexpected complications.
In this present study, the GT in a young Chinese population was evaluated by different methods (probe transparency, transgingival probing and CBCT) and the periodontal biotype distribution was explored by cluster analysis. Moreover, PV was first measured by CBCT and its relationship with periodontal biotype was analyzed at the same time.
The influences of some factors, such as the position and shape of the tooth, race, gender and age, on periodontal biotype have been confirmed by some researchers3,4. Until now, most studies on periodontal biotype have been in Caucasians. In Stein’s study, 60 central maxillary incisors from 60 periodontally healthy Caucasian were involved, and the mean GT was 1.25 mm11. In Nikiforidou’s research, 42 periodontally healthy subjects were recruited, and the mean GT of 186 maxillary anterior teeth was found to be 1.20 mm12. Le’s study included 84 maxillary teeth from 14 periodontally healthy Chinese individuals, and revealed that subjects with thin biotypes were only 9% of that population15. In addition, in most studies, only maxillary anterior teeth were involved. Differences in GT between maxillary and mandibular anterior teeth were reported by La Rocca and Muller16,17. Although the aesthetic appearance of mandibular anterior teeth does exist, studies concerning mandibular teeth are still limited. Therefore, both maxillary and mandible teeth were included in this study and the sample size was expanded to 372 teeth.
In the past ten years, periodontal biotype distribution was explored in numerous studies. Among them, the periodontal biotypes of subjects, but not their teeth, were confirmed by most researchers4,10,11,18,19,20. However, the effects of tooth sites on GT were revealed by Müller and Vandana17,21. Therefore, differences in periodontal biotype/GT from tooth to tooth in the same subject do exist. It is imprecise to classify a mandibular tooth with thin gingiva as a thick biotype based on the data from a maxillary tooth with thick gingiva. De Rouck noticed that the results of transgingival probing in two maxillary incisors might be different4. In this present study, differences in GTP, AGW, PH and BT between maxillary and mandibular teeth were also observed, which further confirmed that the periodontal biotype of upper anterior teeth might not represent the biotype of all anterior teeth, let alone the whole dentition. To avoid unsatisfactory prognosis, it is still very important to explore the biotype of inferior teeth accurately before some dental treatments, such as orthodontic treatment and implantation22,23. Therefore, we tried to assess periodontal biotype tooth by tooth in this study.
Many invasive and non-invasive methods have been employed to assess periodontal biotype, such as transgingival probing, probe transparency and CBCT4,12,24,25. Transgingival probing is an invasive direct measurement performed by inserting an injection needle, periodontal probe or endodontic file through gingiva under local anesthesia. Infusion of the anesthetic agent, angulations of probing and distortion of tissues might affect the precision of this measurement. In addition, excessive puncture strength might lead to the penetration of periosteum and even lamina dura. Probe transparency is a non-invasive method based on the transparency of a periodontal probe through the gingival margin. A clinical trial involving 100 periodontally healthy subjects indicated that probe transparency was highly reproducible, with 85% agreement between duplicate recordings4. However, it is also a subjective method, and its accuracy depends on the examiner’s experience. Stein found that the prognostic value of probe transparency for GT and BT was limited11. CBCT, a three-dimensional radiographic technique, is a routine examination for hard tissues. In a CBCT scan, similar radiographic densities of gingivae, lips, cheeks and tongue prevents the identification of gingivae, and a contrast agent, plastic lip retractor or cotton rolls are then needed to make soft tissues visible26,27. Moreover, gingivae are too thin to be measured accurately, and a high-resolution screen and easily operated measurement software are therefore necessary.
So far, there has been no comparison of the consistency of these three methods. In this study, an excellent consistency of transgingival probing and CBCT was confirmed, while similar consistency between transgingival probing/CBCT and probe transparency was not found in the same samples. Untill now, there has been no accurate, reliable and simple measurement method widely accepted by researchers all over the world. Dentists should choose the appropriate method according to their experiences and actual cases. For example, CBCT measurements might be included in orthodontic treatment and implantation. For these patients, it might be an excellent choice for periodontal biotype assessment.
During the past ten years, the correlation between periodontal anatomic parameters has always been focus of attention, while no consensus has been reached. Multi-parameter correlations were observed in this study, including CW/CL-GTP, PV-GTP and AGW-GTP, which implied that GT was highly correlated with the tooth and its surrounding tissues. Stein11 and Nikiforidou12 also found a close relationship between CW/CL and GT at CEJ, which was similar to our results, while Fischer did not8. For convenience of measurement, crown length was recorded as the distance between incisal edge of the teeth and free gingival margin in this study. However, it is important to point out that, to some degree, clinical crown length (from incisal edge to free gingival margin) is different from anatomical crown length (from incisal edge to CEJ), which might affect the results. Moreover, Nikiforidou indicated that GT at the CEJ was related to labial BT at a point 3 mm apical to the CEJ12. However, La Rocca pointed out that BT was related to AGW, but not to GT16. As far as BT was concerned, different results might be due to different samples and measurement sites. Nikiforidou confirmed a moderate association between GT and BT, while it was Mallikarjun’s conclusion that there was no significant correlation between them12,28. Our study indicated that the correlations between BT at the midpoint of the root and some other parameters (GTP, CW/CL, AGW and PV) were weak. In addition, there were no differences in BT among the four groups created by cluster analysis, which suggested that BT might be less associated with periodontal biotypes.
Gingival papilla in the anterior aesthetic area is not only an important biological barrier to protect the teeth and surrounding tissues but also an artificial factor in aesthetics29. During treatment in the aesthetic area, attention needs to be paid not only to the health of gingivae but also to their beauty and harmony. The appearance of interdental papilla, especially its height, is important for aesthetics in implantation30. De Rouck reported that the mean PH in Caucasians was 3.96 mm4. Cao found that the mean height and width of papilla were 3.67 mm and 4.35 mm in Chinese, which was different from our results31. Compared with the height and width of papilla, PV is a parameter in three-dimensional space and may represent the quantity of soft tissue more accurately. It is almost impossible to measure PV without CBCT scanning and three-dimensional reconstruction. Therefore, until now, there have been no studies exploring PV. Our study first found that PV was highly correlated with CW/CL and GTP, which implied the underlying relationship between PV and the appearance of tooth and periodontal soft tissues. In this present study, smaller PV was found to be more common in teeth characterized by average-scalloped and thin-scalloped biotypes. Black triangles caused by the destruction of papilla are a major cosmetic deficiency for patients who expect aesthetically pleasing restorative or orthodontic treatments. Some researchers found that black triangles developed more easily in patients with scalloped teeth32. It is unclear that whether PV is a risk factor for black triangles, and the relationship between PV and black triangles needs to be further explored.
Exploration of periodontal biotype distribution by cluster analysis was undertaken by some researchers. K-mean clustering algorithm, which classified samples according to categories specified by investigators, was employed by Müller, De Rouck and Gobbato, who artificially classified the included subjects into three periodontal biotypes4,24,25. Nikiforidou found four periodontal types by HCA12. During this statistical analysis, numbers of categories were decided by the characteristics of the data themselves, not artificially imposed by researchers. When a small sample is analyzed, the results by HCA may be scattered and difficult to generalize, while k-mean clustering may be efficient and easy to derive results. However, when larger samples are analyzed, HCA can reflect the characteristics of the data themselves as much as possible. Therefore, owing to the quantity of teeth included in this study, HCA was employed.
In papers that employed cluster analysis, different variables were analyzed in different studies, and their weights were also different. In general, GT and the shape of teeth have been the most important and frequently employed parameters to distinguish periodontal biotypes11. Gobbato even paid so much attention to tooth morphology that he did not consider GT and BT as parameters for cluster analysis24. Some other variables, including AGW, keratinized gingiva width and PH, were also taken into consideration by some studies4,25. Due to the strong correlations of PV-CW/CL and PV-GTP, we included PV in cluster analysis for the first time.
As a result of the variety of included samples, measurement means and statistical methods, different categories and proportional distribution were obtained in different papers. In Stein’s study, 46.7% of Caucasians were classified as having the thin biotype, and the others were classified as having the thick biotype11. De Rouck included 100 Caucasians and thin-scalloped, thick-flat and thick-scalloped biotypes were found to be 37%, 29% and 34% of the sample, respectively4. Le’s study identified that the thin, compromised and thick biotypes in Chinese individuals were 9%, 50% and 41%, respectively15. Four periodontal biotypes were reported by Nikiforidou: thin, average, mixed and thick type, which comprised 31.9%, 31.3%, 16.6% and 20.2% of the sample, respectively12. In our results, the most and the least common types were thick-flat (36.8%) and average-flat type (10.5%), while the rest were average-scalloped and thin-scalloped type (each approximately 1/4 of the total samples). Our present study also revealed an effectively equal distribution of slender and square teeth in a young Chinese population (slender 52.69% and square 47.31%). Moreover; there were more slender teeth in subjects with average/thin gingival and more square teeth in persons with thick/average gingiva.
In summary, a possible diversity of periodontal biotypes beyond thick and thin might exist in the young Chinese population. The most common periodontal biotype was the thick-flat biotype, which displayed a square tooth, average AGW, thick BT and large gingival papilla. Meanwhile, the second-largest biotype, the thin-scalloped biotype, which displayed a slender tooth, narrow AGW, thin BT and small gingival papilla, was the one with the highest aesthetic risk. In clinical practice, more attention should be paid to these teeth, especially in the aesthetic zone.
References
Ochsenbein, C. & Ross, S. A reevaluation of osseous surgery. Dent Clin North Am. 13, 87–102 (1969).
Seibert, J. & Lindhe, J. Esthetics and periodontal therapy. In Textbook of Clinical Periodontology (ed. Lindhe, J.) 477–514 (Munksgaard, 1989).
Müller, H. P. & Eger, T. Gingival phenotypes in young male adults. J ClinPeriodontol. 24, 65–71 (1997).
De Rouck, T., Eghbali, R., Collys, K., De Bruyn, H. & Cosyn, J. The gingival biotype revisited: transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J ClinPeriodontol. 36, 428–433 (2009).
Cuny-Houchmand, M. et al. Gingival biotype assessment: visual inspection relevance and maxillary versus mandibular comparison. Open Dent J. 7, 1–6 (2013).
Eghbali, A., De Rouck, T., De Bruyn, H. & Cosyn, J. The gingival biotype assessed by experienced and inexperienced clinicians. J ClinPeriodontol. 36, 958–963 (2009).
Savitha, B. & Vandana, K. L. Comparative assessment of gingival thickness using transgingival probing and ultrasonographic method. Indian J Dent Res. 16, 135–139 (2005).
Fischer, K. R. et al. On the relationship between gingival biotypes and supracrestal gingival height, crown form and papilla height. Clin Oral Implants Res. 25, 894–898 (2014).
Fischer, K. R., Richter, T., Kebschull, M., Petersen, N. & Fickl, S. On the relationship between gingival biotypes and gingival thickness in young Caucasians. Clin Oral Implants Res. 26, 865–869 (2015).
Kim, J. H., Cho, Y. J., Lee, J. Y., Kim, S. J. & Choi, J. I. An analysis on the factors responsible for relative position of interproximal papilla in healthy subjects. J Periodontal Implant Sci. 43, 160–167 (2013).
Stein, J. M. et al. The gingival biotype: measurement of soft and hard tissue dimensions - a radiographic morphometric study. J Clin Periodontol. 40, 1132–1139 (2013).
Nikiforidou, M. et al. Classification of periodontal biotypes with the use of CBCT. A cross-sectional study. Clin Oral Investig. 20, 2061–2071 (2016).
Frost, N. A., Mealey, B. L., Jones, A. A. & Huynh-Ba, G. Periodontal biotype: Gingival thickness as it relates to probe visibility and buccal plate thickness. J Periodontol. 86, 1141–1149 (2015).
Lee, A., Fu, J. H. & Wang, H. L. Soft tissue biotype affects implant success. Implant Dent. 20, 38–47 (2011).
Le, D., Zhang, H., Hu, W. J. & Liu, D. G. Preliminary study on gingival biotype by periodontal probing by periodontal probing. Zhonghua Kou Qiang Yi Xue Za Zhi. 47, 81–84 (2012).
La Rocca, A. P. et al. Anterior maxillary and mandibular biotype: relationship between gingival thickness and width with respect to underlying bone thickness. Implant Dent. 21, 507–515 (2012).
Müller, H. P., Schaller, N., Eger, T. & Heinecke, A. Thickness of masticatory mucosa. J Clin Periodontol. 27, 431–436 (2000).
Lazos, J. P., Senn, L. F. & Brunotto, M. N. Characterization of maxillary central incisor: novel crown–root relationships. Clin Oral Investig. 18, 1561–1567 (2014).
Montevecchi, M., Checchi, V., Piana, L. & Checchi, L. Variables Affecting the Gingival Embrasure Space in Aesthetically Important Regions: Differences between Central and Lateral Papillae. Open Dent J. 5, 126–135 (2011).
Stellini, E., Comuzzi, L., Mazzocco, F., Parente, N. & Gobbato, L. Relationships between different tooth shapes and patient’s periodontal phenotype. J Periodontal Res. 48, 657–662 (2013).
Vandana, K. L. & Savitha, B. Thickness of gingiva in association with age, gender and dental arch location. J Clin Periodontol. 32, 828–830 (2005).
Joss‐Vassalli, I., Grebenstein, C., Topouzelis, N., Sculean, A. & Katsaros, C. Orthodontic therapy and gingival recession: a systematic review. Orthod Craniofac Res. 13, 127–141 (2010).
Malhotra, R., Grover, V., Bhardwaj, A. & Mohindra, K. Analysis of the gingival biotype based on the measurement of the dentopapillary complex. J Indian SocPeriodontol. 18, 43–47 (2014).
Gobbato, L., Tsukiyama, T., Levi, P. A., Griffin, T. J. & Weisgold, A. S. Analysis of the shapes of maxillary central incisors in a Caucasian population. Int J Periodontics Restorative Dent. 32, 69–78 (2012).
Müller, H. P., Heinecke, A., Schaller, N. & Eger, T. Masticatory mucosa in subjects with different periodontal phenotypes. J Clin Periodontol. 27, 621–626 (2000).
Silva, J. N. N. et al. Influence of lip retraction on the cone beam computed tomography assessment of bone and gingival tissues of the anterior maxilla. Oral Surg Oral Med Oral Pathol Oral Radiol. 123, 714–720 (2017).
Kim, Y. J. et al. New method of assessing the relationship between buccal bone thickness and gingival thickness. J Periodontal Implant Sci. 46, 372–381 (2016).
Mallikarjun, S. et al. Comparative evaluation of soft and hard tissue dimensions in the anterior maxilla using radiovisiography and cone beam computed tomography: A pilot study. J Indian SocPeriodontol. 20, 174–177 (2016).
Zetu, L. & Wang, H. L. Management of inter‐dental/inter‐implant papilla. J Clin Periodontol. 32, 831–839 (2005).
Thoma, D. S., Buranawat, B., Hämmerle, C. H., Held, U. & Jung, R. E. Efficacy of soft tissue augmentation around dental implants and in partially edentulous areas: a systematic review. J Clin Periodontol. 41, 77–91 (2014).
Cao, J., Hu, W. J., Zhang, H., Liu, D. G. & Le, D. Preliminary study on measuring interdental papilla height and thickness of the maxillary anterior teeth based on cone-beam computed tomography. Zhonghua Kou Qiang Yi Xue Za Zhi. 48, 581–585 (2013).
Chow, Y. C., Eber, R. M., Tsao, Y. P., Shotwell, J. L. & Wang, H. L. Factors associated with the appearance of gingival papillae. J Clin Periodontol. 37, 719–727 (2010).
Acknowledgements
This work was supported by Natural Science Foundation of China through project 81771075, Natural Science Foundation of Jiangsu Province through project BK20161565 and Science and Technology Development Fund of Nanjing Medical University through project 2016NJMU052.
Author information
Authors and Affiliations
Contributions
Y.S. conceived and designed the experiments. Y.M.S., L.L.Y. and J.Y.G. performed the experiments. D.M.W. analyzed the data. Y.M.S. and L.L.Y. contributed to the drafting. W.L. prepared figures and tables. Y.S. revised the paper and supervised the whole study. All authors approved the final manuscript as submitted and agree to be accountable for the work.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shao, Y., Yin, L., Gu, J. et al. Assessment of Periodontal Biotype in a Young Chinese Population using Different Measurement Methods. Sci Rep 8, 11212 (2018). https://doi.org/10.1038/s41598-018-29542-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-29542-z
This article is cited by
-
A novel approach for gingiva thickness measurements around lower anterior teeth by means of dental magnetic resonance imaging
Clinical Oral Investigations (2023)
-
Accuracy of cone-beam computed tomography in determining gingival thickness: a systematic review and meta-analysis
Clinical Oral Investigations (2023)
-
Thermographic examination of gingival phenotypes: correlation between morphological and thermal parameters
Clinical Oral Investigations (2023)
-
Current landmarks for gingival thickness evaluation in maxillary anterior teeth: a systematic review
Clinical Oral Investigations (2023)
-
Clinical and computed tomographic evaluations of periodontal phenotypes in a Chinese population: a cross-sectional study
Clinical Oral Investigations (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
