
Abstract
This case-control study aimed to investigate differences in the sagittal spinal parameters between the symptomatic spondylolisthesis patients and the general population. Twenty-nine adolescent patients with symptomatic lumbar isthmic spondylolisthesis were included. For each patient, two age-matched, gender-matched and BMI-matched controls were enrolled. Comparison analyses detected higher values in the case group for the following parameters: CL (−22.06 ± 7.552° versus −20.36 ± 7.016°, P < 0.001), T1 Slope (19.84 ± 8.708° versus 13.99 ± 6.537°, P = 0.001), PT (21.54 ± 9.082° versus 8.87 ± 7.863°, P < 0.001), PI (64.45 ± 13.957° versus 43.60 ± 9.669°, P < 0.001), SS (42.90 ± 9.183° versus 34.73 ± 8.265°, P < 0.001), LL (−50.82 ± 21.596° versus −43.78 ± 10.356°, P = 0.042), SVA (16.99 ± 14.625 mm versus 0.32 ± 31.824 mm, P = 0.009), L5 Slope (33.95 ± 13.567° versus 19.03 ± 6.809°, P < 0.001), and L5I (8.90 ± 6.556° versus 1.29 ± 6.726°, P < 0.001). Conversely, TS-CL (6.56 ± 6.716° versus 11.04 ± 7.085°, P = 0.006), cSVA (11.31 ± 6.867 mm versus 17.92 ± 11.832 mm, P = 0.007), and TLK (−2.66 ± 10.101° versus 2.71 ± 7.708°, P = 0.007) were smaller in the case group. Slippage percentage was most correlated with PI (r = 0.530, P = 0.003), followed by PT (r = 0.465, P = 0.011) and L5I (r = 0.433, P = 0.019). Results of binary logistic regression showed that the main risk factor of isthmic spondylolisthesis was PI (OR = 1.145, 95%CI = 1.083–1.210, P < 0.001). Further subgroup analysis also showed that PI was the main risk factor of isthmic spondylolisthesis in the female adolescents (OR = 1.237, 95%CI = 1.086–1.493, P = 0.003) and in the male adolescents (OR = 1.523, 95%CI = 1.093–2.123, P = 0.013). PI was the main risk factor for adolescent symptomatic isthmic spondylolisthesis in the Chinese Han adolescents. The greater PI indicated the higher the progressive risk of spondylolisthesis. In these isthmic spondylolisthesis adolescents, the body always inclined forward and lumbar and cervical lordosis increased.
Similar content being viewed by others



Introduction
Adolescents suffering from lumbar isthmic spondylolisthesis or spondylolysis always complain of low back pain1. Isthmic spondylolysis is defined as a unilateral or bilateral defect in the pars interarticularis, which frequently occurs at L4 or L5 vertebrae2. Based on different populations, the incidence of spondylolysis varied from 4.4% to 39.7%3,4. Adolescent athletes were more susceptible to isthmic spondylolysis5. Several factors were associated with the susceptibility to spondylolysis, including ethnic heterogeneity6, genetic background7, occupation5, and sagittal balance8. Spondylolisthesis is defined as the forward slippage of vertebrae with respect to the underlying vertebrae, which frequently occurs in patients with bilateral pars defects. This abnormality usually occurred after walking age, and the adaptation both in the sagittal balance of the spine and lumbar-pelvic-femoral complex was associated with spondylolisthesis. Furthermore, it was assumed that the acquisition of bipedalism coupled with vertical stance was the prerequisite to spondylolisthesis8.
In adults, several studies have investigated the sagittal alignment in different populations9. Sagittal spine alignment was associated with Health-related quality of life (HRQoL)10, especially in elderly individuals11,12. Based on 492 consecutive Caucasian patients, aged on average 51.9 ± 16.8 years, Schwab et al.12 observed that threshold values for severe disability (Oswestry Disability Index, ODI > 40) were comprised of (pelvic tilt, PT ≥ 22°), (sagittal vertical alignment, SVA ≥ 47 mm), and (pelvic incidence minus lumbar lordosis, PI-LL ≥ 11°). It is well-known that sagittal spinal alignment changes with age, and pelvic-spine parameters vary in different populations. For example, a relatively smaller pelvic incidence (PI) was observed in the Chinese Han population than in Caucasian populations13,14.
In adolescents where no aforementioned clinical evidence was observed, previous radiographic studies proposed that the average values of PT, PI, sacral slope(SS), and other sagittal parameters should be slightly smaller when compared with normal adults15,16. Insufficient information was reported regarding the normal sagittal alignment range in adolescents, especially concerning the association of abnormal sagittal alignment with lumbar diseases such as lumbar isthmic spondylolisthesis. Therefore, this study aimed to detect the difference of sagittal alignment between adolescent symptomatic lumbar isthmic spondylolisthesis patients and general adolescents in the Chinese Han population.
Result
General information
There were 13 male and 16 female adolescents in the case group. The control group comprised of 26 males and 32 females. The averaged slip percentage was 36.97 ± 8.95%. No difference was observed in terms of age (P = 0.780), height (P = 0.332), weight (P = 0.256), BMI (P = 0.798), and gender distribution (P = 0.589). The average age in the case and control groups was 14.03 ± 1.50 years and 14.14 ± 1.68 years, respectively. The average height was 155.10 ± 11.95 cm and 157.57 ± 10.69 cm, the average weight was 53.38 ± 7.55 kg and 55.33 ± 7.36 kg, and the average BMI was 22.15 ± 1.52 kg/m2 and 22.34 ± 1.45 kg/m2, respectively. Table 1 demonstrates the details on demographic characteristics.
Univariate Analysis
Comparison analyses detected higher values in the case group for the following parameters cervical lordosis (CL: −22.06 ± 7.552° versus −20.36 ± 7.016°, P < 0.001), T1 Slope (19.84 ± 8.708° versus 13.99 ± 6.537°, P = 0.001), PT (21.54 ± 9.082° versus 8.87 ± 7.863°, P < 0.001), PI (64.45 ± 13.957° versus 43.60 ± 9.669°, P < 0.001), SS (42.90 ± 9.183° versus 34.73 ± 8.265°, P < 0.001), LL (−50.82 ± 21.596° versus −43.78 ± 10.356°, P = 0.042), SVA (16.99 ± 14.625 mm versus 0.32 ± 31.824 mm, P = 0.009), L5 Slope (33.95 ± 13.567° versus 19.03 ± 6.809°, P < 0.001), and L5 Incidence (L5I: 8.90 ± 6.556° versus 1.29 ± 6.726°, P < 0.001). Conversely, T1 Slope minus Cervical Lordosis (TS-CL: 6.56 ± 6.716° versus 11.04 ± 7.085°, P = 0.006), C2-C7 plumbline (cSVA: 11.31 ± 6.867 mm versus 17.92 ± 11.832 mm, P = 0.007), and thoracolumbar kyphosis (TLK: −2.66 ± 10.101° versus 2.71 ± 7.708°, P = 0.007) were smaller in the case group. There was no difference in C1-C2 cervical lordosis (C1-C2, P = 0.301), or thoracic kyphosis (TK, P = 0.844). Table 2 demonstrates the details on the comparison analyses.
For the male group, comparison analyses detected higher values in the case group for the following parameters including CL (−11.73 ± 8.608° versus −2.17 ± 11.056°, P = 0.010), PT (27.70 ± 6.589° versus 12.36 ± 7.874°, P = < 0.001), PI (76.75 ± 7.925° versus 51.32 ± 9.289°, P < 0.001), SS (49.06 ± 6.089° versus 38.96 ± 8.984°, P = 0.001), L5 Slope (42.78 ± 7.153° versus 21.83 ± 6.977°, P < 0.001), and L5I (−13.32 ± 5.501° versus −3.03 ± 7.032°, P < 0.001). Conversely, TS-CL (4.55 ± 6.688° versus 11.85 ± 8.359°, P = 0.010) and TLK (−10.48 ± 6.377° versus 2.40 ± 8.228°, P < 0.001) were smaller in the case group. While there was no difference in C1-C2 (P = 0.890), T1 Slope (P = 0.397), cSVA (P = 0.216), LL (P = 0.749), and SVA (P = 0.215) (Table 2).
For the female group, comparison analyses detected higher values in the case group for the following parameters including CL (−14.54 ± 10.314° versus −3.28 ± 9.417°, P < 0.001), T1 Slope (22.72 ± 9.189° versus 13.66 ± 6.734°, P < 0.001), PT (16.54 ± 7.728°, versus 6.03 ± 6.719°, P < 0.001), PI (54.46 ± 8.706° versus 37.33 ± 3.425°, P = 0.002), LL (−51.99 ± 12.347° versus −41.00 ± 7.371°, P < 0.001), TK (26.44 ± 8.462° versus 20.65 ± 8.467°, P = 0.030), SVA (12.43 ± 10.521 mm versus −6.69 ± 25.537 mm, P = 0.006), L5 Slope (26.78 ± 13.421°, versus 16.75 ± 5.834°, P = 0.001), and L5I (−5.31 ± 5.033°, versus 0.13 ± 6.219°, P = 0.004). Conversely, cSVA (7.89 ± 3.979 mm versus 15.70 ± 9.830 mm, P = 0.004) was smaller in the case group. While there was no difference in C1-C2 (P = 0.240), and TLK (P = 0.754) (Table 2).
Correlations between Slippage percentage and other sagittal spinal parameters
For the whole case and control groups, slippage percentage was most correlated with PI (r = 0.530, P = 0.003), followed by PT (r = 0.465, P = 0.011) and L5I (r = 0.433, P = 0.019). In the male group, slippage percentage was correlated with SVA (r = 0.568, P = 0.022). However, no significant correlation was observed in the female group (Table 3).
Multivariate Analysis
Results of binary logistic regression showed that the main risk factor of isthmic spondylolisthesis was PI (OR = 1.145, 95%CI = 1.083–1.210, P < 0.001) with the following parameters excluded (PT, SS, SVA, LL, L5I and L5 Slope, P > 0.05) (Table 4).
In the male group, the main risk factor of isthmic spondylolisthesis was PI (OR = 1.237, 95%CI = 1.086–1.493, P = 0.003) with the following parameters excluded (PT, SS, TLK, TK, L5 Incidence and L5 Slope, P > 0.05) (Table 5).
In the female group, the main risk factor for isthmic spondylolisthesis was PI (OR = 1.523, 95%CI = 1.093–2.123, P = 0.013) with the following parameters excluded (PT, SS, LL, SVA, TK, L5 Incidence and L5 Slope, P > 0.05) (Table 6).
Discussion
To the best of our knowledge, no report has been focused on the sagittal spinal alignment in isthmic adolescent lumbar spondylolisthesis patients in the Chinese Han population. Comparison analyses detected higher values in our case group for the following parameters: CL (P < 0.001); T1 Slope (P = 0.001); PT (P < 0.001); PI (P < 0.001); SS (P < 0.001); LL (P = 0.042); SVA (P = 0.009); L5 Slope (P < 0.001); and L5I (P < 0.001). Correlation analysis detected that slippage percentage was most correlated with PI (r = 0.530, P = 0.003), followed by PT (r = 0.465, P = 0.011) and L5I (r = 0.433, P = 0.019). Binary logistic regression showed that the main risk factor of isthmic spondylolisthesis was PI (OR = 1.145, 95%CI = 1.083–1.210, P < 0.001).
It is commonly accepted that the sagittal spine misalignment plays a vital role in the mechanisms of several spine disorders. For example, it has been reported that young lumbar disc herniation patients demonstrated smaller LL, TK, and SS in the Chinese Han population13. In adults, Yin et al.17 reported that elevated PI and small sacral table angle (STA) played vital roles in lumbar spondylolysis in the Chinese Han population. In our study, the increased PI was also observed in adolescents with lumbar isthmic spondylolisthesis (64.45 ± 13.957° versus 43.60 ± 9.669°, P < 0.001). Previous studies reported that the PI in the Chinese Han population ranged from 40 to 50 degrees18, which was smaller than that found in Caucasian15 as well as in Korean populations19. Our study also detected a similar PI (43.60 ± 9.669°) in normal adolescents. In addition, this study also observed higher PT (21.54 ± 9.082° versus 8.87 ± 7.863°, P < 0.001) and SS (42.90 ± 9.183° versus 34.73 ± 8.265°, P < 0.001) in the case group, which was in accordance with the previous findings in adult spondylolisthesis patients17. In both the female and male group, the greater values of PI, PT, and SS also presented in lumbar isthmic spondylolisthesis patients.
Moreover, logistic regression analysis indicated that the main risk factor of isthmic spondylolisthesis was PI (OR = 1.145 95%CI = 1.083–1.210, P < 0.001), which was similar to findings in previous reports15,17. There was a significant correlation between PI and other sagittal parameters, including SS, PT and LL. PI increase was accompanied by an increase in both SS and PT, with a greater increase in SS than in PT. For those individuals of higher PI, larger LL always occurred to guarantee C7 plumb line behind the femoral head and to maintain the posture balance20. However, the larger LL and SS could exert relatively higher forward shear force on an isthmic of L5, which, coupled with the defect of pars interarticularis, would lead to lumbar spondylolisthesis. Moreover, the increased shear force also led to a larger L5 slope in the control group. Further subgroup analysis also detected that PI was the main risk factor of isthmic spondylolisthesis, both in female adolescents (OR = 1.237, 95%CI = 1.086–1.493, P = 0.003) and in male adolescents (OR = 1.523, 95%CI = 1.093–2.123, P = 0.013).
As for the LL, increased LL was observed in the case groups (−50.82° ± 21.596° versus −43.78° ± 10.356°, P = 0.042). Further subgroup analysis also detected higher LL in the female isthmic spondylolisthesis (−51.99 ± 12.347° versus −41.00 ± 7.371°, P < 0.001). Similarly, a greater degree of LL was also observed in isthmic spondylolisthesis patients (−55° ± 6°) than in degenerative spondylolisthesis patients (−43° ± 13°), as well as in the controls (−48° ± 12°) in Koreans (P = 0.004)21. LL is essential to maintain an upright posture in human being. Reports have shown that the lumbar lordosis angle increased until 14 or 16 years of age, and that the increased disc wedging angle resulted in the increase of LL22. Therefore, the relatively young average age might explain the smaller LL than previously reported LL values17,18. Similarly, the small TK and TLK values were also observed when compared with the corresponding values in adults.
Initially, Roussouly et al.23 introduced the L5I. It was inferred that L5I was significantly associated with isthmic spondylolisthesis. Based on 138 healthy volunteers, Zhu et al.24 reported mean values of L5I in adolescents (17.63 ± 8.65°) and adults (16.43 ± 7.64°). They also reported that there was a positive correlation between L5I and PI (r = 0.818), and established a linear formula to evaluate an ideal L5I based on PI (L5I = 0.725PI-12.757). Thus, the larger the PI, the larger also the L5I. Therefore, the greater L5I (8.90 ± 6.556° versus 1.29 ± 6.726°, P < 0.001) in the case group might result from the greater PI (64.45 ± 13.957° versus 43.60 ± 9.669°, P < 0.001). Additionally, the further subgroup analysis also demonstrated higher L5I values both in the male and female isthmic spondylolisthesis patients.
This study also compared the cervical sagittal alignment between the two groups. In the case group, we observed a greater T1 Slope (19.84 ± 8.708° versus 13.99 ± 6.537°, P = 0.001), and a greater CL (−22.06 ± 7.552° versus −20.36 ± 7.016°, P < 0.001). However, there was no difference in C1-C2 (P = 0.301). Smaller cSVA (11.31 ± 6.867 mm versus 17.92 ± 11.832 mm, P = 0.007) and smaller TS-CL (6.56 ± 6.716° versus 11.04 ± 7.085°, P = 0.006) were demonstrated in the case group. Recently, an increased number of studies was focused on cervical sagittal alignment. Hiyama et al.25 proposed that cervical sagittal alignment could be affected by thoracic deformity. Similarly, Hwang et al.26 demonstrated that there was a significant association between TK and cervical sagittal alignment. Moreover, another study suggested that the cervical sagittal alignment was correlated with the global sagittal spine alignment rather than regional thoracic kyphosis27. Given the larger SVA (16.99 ± 14.625 mm versus 0.32 ± 31.824 mm, P = 0.009) and T1 slope (19.84 ± 8.708° versus 13.99 ± 6.537°, P = 0.001) in the case group, we also inferred that the increased lordosis in cervical sagittal plane might compensate for the forward inclined trunk. So, the horizontal gaze can be guaranteed. In addition, the further subgroup analysis also demonstrated greater cervical lordosis in both the male and the female isthmic spondylolisthesis patients.
As for slippage percentage, correlation analysis detected that it was most correlated with PI (r = 0.530, P = 0.003), followed by PT (r = 0.465, P = 0.011) and L5I (r = 0.433, P = 0.019) (Table 3). Previously, Rajnics et al.28 reported a similar correlation coefficient (r = 0.660) between slip percentage and PI. Another study also reported that slip percentage was correlated with PI (r = 0.293, p = 0.023)29. Therefore, we inferred that progression of isthmic lumbar spondylolisthesis in adolescents was associated with a greater PI. Positive correlations were also detected in PT (r = 0.465, P = 0.011), L5I (r = 0.433, P = 0.019) and cSVA (r = 0.418, P = 0.024), which presumably results from the compensation for the forward inclined body to maintain sagittal balance. However, slippage percentage was only correlated with SVA (r = 0.568, P = 0.022) in the male population. In the female population, no significant correlation was observed. It should be noticed that the small sample size might have failed to reflect the correlation when subgroup analysis was performed based on gender difference.
Even though this study investigated the sagittal spinal alignment difference between the adolescent isthmic spondylolisthesis patients and the general population in China, several limitations should be taken into consideration. First, only 29 adolescent isthmic spondylolisthesis patients were included, thus the statistical power may be dwarfed. Second, it was understood that different ethnicities demonstrated different values of sagittal spinal parameters; therefore, further studies should be performed in additional ethnic populations. Third, spinal and pelvic parameters have been verified to be significantly associated with HRQoL, which may change with increasing age. This was not evaluated in our study, since no symptoms were observed in the controls.
Conclusion
PI was the main risk factor for adolescent symptomatic isthmic spondylolisthesis in the Chinese Han adolescent population. The greater PI indicated the higher the progressive risk of spondylolisthesis. In isthmic spondylolisthesis adolescents, the body always inclined forward. With pelvic retroversion essential to maintaining sagittal balance, lumbar and cervical lordosis was always increased.
Methods and Materials
From August 2009 to August 2017, a consecutive group of 29 adolescent patients with lumbar spondylolistheses was reviewed. All patients complained repeatedly of low back pain and were admitted to our department for surgical treatment. Oblique X-ray films or CT images were used to confirm the defects in the pars interarticularis (Fig. 1). For each patient, we selected 2 age-matched, gender-matched, Body Mass Index(BMI)-matched controls who attended the Outpatient Department for scoliosis screening, and were eventually excluded via full spine X-ray films. None of the controls had a history of spinal disorders or spine surgery, nor any history of low back pain and radiologic abnormalities. Moreover, all cases and controls were less than 18 years old. This study was approved by the Institutional Review Board of ChangHai hospital. This study was approved by the Institutional Review Board of ChangHai hospital. Given the fact that all participants were under the age of 18, informed consents were obtained from their legal guardians. We confirmed that all experiments were performed in accordance with relevant guidelines and regulations.

Demonstrated an adolescent lumbar isthmic spondylolisthesis patient.
Data collection
Demographic details on age, height, weight, BMI, and gender were collected. The radiographic films were measured independently by two researchers. The parameters measured were as follows:
-
(1)
Cervical sagittal alignment parameters: C1-C2 (C1-C2 cervical lordosis, the angle between C1 and the caudal endplate of C2), CL (C2-C7 cervical lordosis is the angle between the caudal endplate of C2 and the caudal endplate of C7), cSVA(cSVA is the horizontal offset from the plumbline dropped from C2 to the posterosuperior corner of C7), TS-CL (T1 Slope minus CL is the difference between T1 Slope and CL) (Fig. 2).
Figure 2 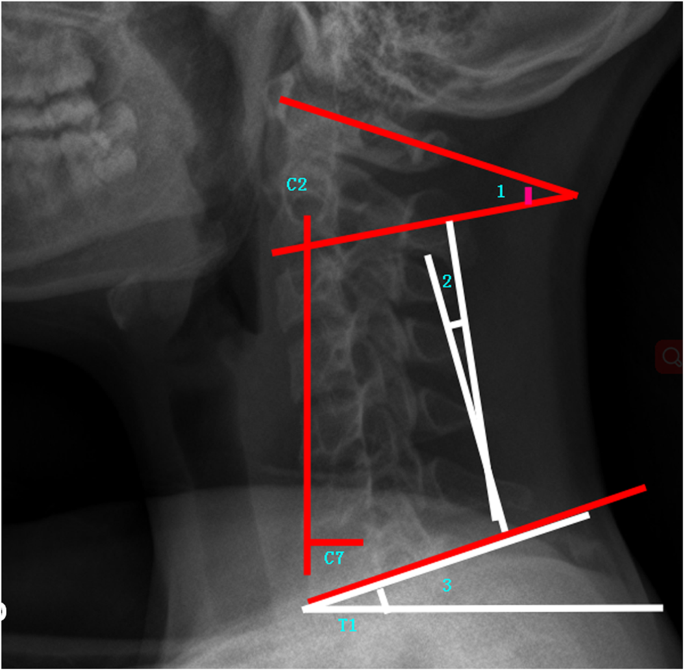
Demonstrated cervical sagittal alignment parameters (1:C1-C2, 2:C2-C7, and 3: T1 Slope).
-
(2)
Thoracic kyphosis and Lumbar lordosis parameters: TK (thoracic kyphosis)30,31, LL (lumbar lordosis)30,31, TLK (thoracolumbar kyphosis).
-
(3)
Sagittal lumbosacral parameters: SS, PT, PI, L5 Slope(the angle between a horizontal line and the superior end plate of L5), and L5I (L5 Incidence, the angle between the vertical line and the line connecting the center of the femoral heads axis to the center of the upper endplate of L523) (Fig. 3).
Figure 3 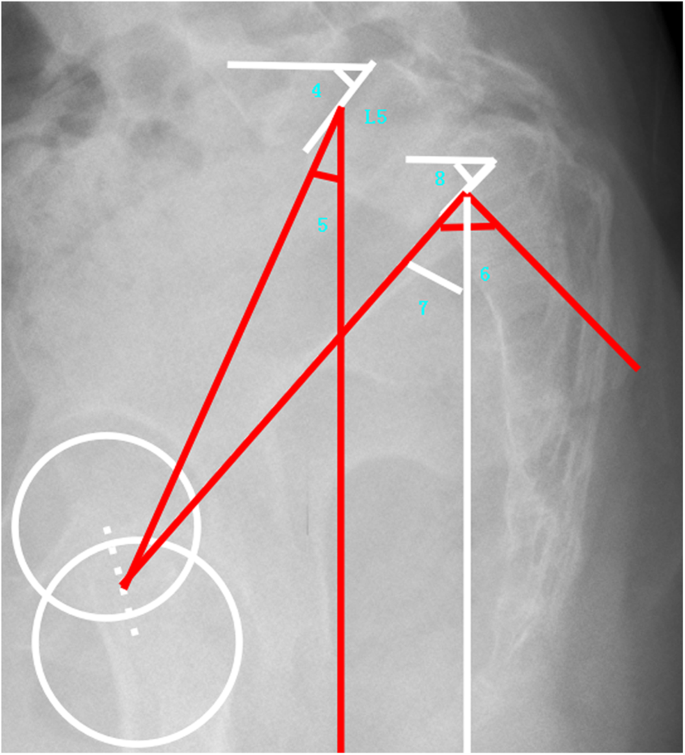
Demonstrated sagittal lumbosacral parameters (4: L5 Slope, 5: L5 Incidence, 6: Pelvic Incidence, 7: Pelvic Tilt, and 8: Sacral Slope).
-
(4)
Global sagittal alignment parameters: SVA (the horizontal offset from the posterosuperior corner of S1 to the vertebral body of C7), and T1 Slope (the angle between a horizontal line and the superior end plate of T1).
-
(5)
Slip percentage was assessed in those lumbar isthmic spondylolisthesis patients32. Figure 4 demonstrated the measurement of slip percentage.
Figure 4 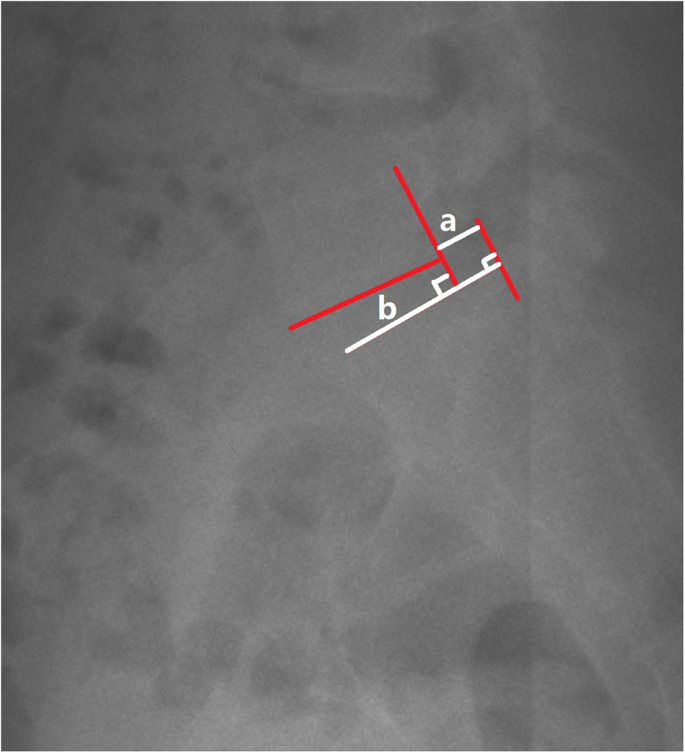
Demonstrated the measurement of slip percentage.



Statistical analysis
Statistical analyses were performed using SPSS 19.0 statistics software (SPSS Inc., Chicago, IL). Descriptive statistics were listed in the form of mean ± SD (standard deviation). An independent-sample t test was employed to assess the difference between groups. Count data distribution was assessed by Chi-square test. Correlation analysis was performed to assess the associations between slip percentage and other parameters in the case group.
To identify the main risk factors of adolescent symptomatic isthmic spondylolisthesis, multiple logistic regression models were constructed using sagittal lumbosacral parameter variables and global sagittal alignment parameters that were of significance in univariate analysis. P < 0.05 was considered as the significant level.
In addition, there are gender differences in several aspects, such as growing speed, and skeletal structure. Subgroup analysis was also performed based on gender differences.
Data availability statement
The data sets generated during the current study are available from the first author (Jian Zhao) on request.
References
Altaf, F., Heran, M. K. & Wilson, L. F. Back pain in children and adolescents. The bone & joint journal 96-b, 717–723, https://doi.org/10.1302/0301-620x.96b6.33075 (2014).
Cavalier, R., Herman, M. J., Cheung, E. V. & Pizzutillo, P. D. Spondylolysis and spondylolisthesis in children and adolescents: I. Diagnosis, natural history, and nonsurgical management. The Journal of the American Academy of Orthopaedic Surgeons 14, 417–424 (2006).
Nitta, A. et al. Prevalence of Symptomatic Lumbar Spondylolysis in Pediatric Patients. Orthopedics 39, e434–437, https://doi.org/10.3928/01477447-20160404-07 (2016).
Roche, M. B. & Rowe, G. G. The incidence of separate neural arch and coincident bone variations; a survey of 4,200 skeletons. The Anatomical record 109, 233–252 (1951).
Selhorst, M., Fischer, A. & MacDonald, J. Prevalence of Spondylolysis in Symptomatic Adolescent Athletes: An Assessment of Sport Risk in Nonelite Athletes. Clinical journal of sport medicine: official journal of the Canadian Academy of Sport Medicine, https://doi.org/10.1097/jsm.0000000000000546 (2017).
Lonstein, J. E. Spondylolisthesis in children. Cause, natural history, and management. Spine (Phila Pa 1976) 24, 2640–2648 (1999).
Matsui, Y. et al. The association of lumbar spondylolisthesis with collagen IX tryptophan alleles. The Journal of bone and joint surgery. British volume 86, 1021–1026 (2004).
Violas, P. & Lucas, G. L5S1 spondylolisthesis in children and adolescents. Orthopaedics & traumatology, surgery & research: OTSR 102, S141–147, https://doi.org/10.1016/j.otsr.2015.03.021 (2016).
Chen, H. et al. The Height-Width-Depth Ratios of the Intervertebral Discs and Vertebral Bodies in Adolescent Idiopathic Scoliosis vs Controls in a Chinese Population. Scientific Reports 7, 46448, https://doi.org/10.1038/srep46448 (2017).
Benli, I. T. et al. Minimum 10 years follow-up surgical results of adolescent idiopathic scoliosis patients treated with TSRH instrumentation. European Spine Journal 16, 381–391, https://doi.org/10.1007/s00586-006-0147-3 (2007).
Hasegawa, K. et al. Normative values of spino-pelvic sagittal alignment, balance, age, and health-related quality of life in a cohort of healthy adult subjects. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 25, 3675–3686, https://doi.org/10.1007/s00586-016-4702-2 (2016).
Schwab, F. J. et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976) 38, E803–812, https://doi.org/10.1097/BRS.0b013e318292b7b9 (2013).
Fei, H., Li, W. S., Sun, Z. R., Ma, Q. W. & Chen, Z. Q. Analysis of Spino-pelvic Sagittal Alignment in Young Chinese Patients with Lumbar Disc Herniation. Orthopaedic surgery 9, 271–276, https://doi.org/10.1111/os.12340 (2017).
Zhu, Z. et al. Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine (Phila Pa 1976) 39, E1–6, https://doi.org/10.1097/brs.0000000000000022 (2014).
Mac-Thiong, J. M., Labelle, H., Berthonnaud, E., Betz, R. R. & Roussouly, P. Sagittal spinopelvic balance in normal children and adolescents. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 16, 227–234, https://doi.org/10.1007/s00586-005-0013-8 (2007).
Ghandhari, H., Hesarikia, H., Ameri, E. & Noori, A. Assessment of normal sagittal alignment of the spine and pelvis in children and adolescents. BioMed research international 2013, 842624, https://doi.org/10.1155/2013/842624 (2013).
Yin, J. et al. Differences of Sagittal Lumbosacral Parameters between Patients with Lumbar Spondylolysis and Normal Adults. Chinese medical journal 129, 1166–1170, https://doi.org/10.4103/0366-6999.181972 (2016).
Li, W. S., Li, G., Chen, Z. Q. & Wood, K. B. Sagittal plane analysis of the spine and pelvis in adult idiopathic scoliosis. Chinese medical journal 123, 2978–2982 (2010).
Lee, C. S., Chung, S. S., Kang, K. C., Park, S. J. & Shin, S. K. Normal patterns of sagittal alignment of the spine in young adults radiological analysis in a Korean population. Spine (Phila Pa 1976) 36, E1648–1654, https://doi.org/10.1097/BRS.0b013e318216b0fd (2011).
Labelle, H., Mac-Thiong, J. M. & Roussouly, P. Spino-pelvic sagittal balance of spondylolisthesis: a review and classification. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 20(Suppl 5), 641–646, https://doi.org/10.1007/s00586-011-1932-1 (2011).
Lim, J. K. & Kim, S. M. Difference of Sagittal Spinopelvic Alignments between Degenerative Spondylolisthesis and Isthmic Spondylolisthesis. Journal of Korean Neurosurgical Society 53, 96–101, https://doi.org/10.3340/jkns.2013.53.2.96 (2013).
Shefi, S., Soudack, M., Konen, E. & Been, E. Development of the lumbar lordotic curvature in children from age 2 to 20 years. Spine (Phila Pa 1976) 38, E602–608, https://doi.org/10.1097/BRS.0b013e31828b666b (2013).
Roussouly, P., Gollogly, S., Berthonnaud, E., Labelle, H. & Weidenbaum, M. Sagittal alignment of the spine and pelvis in the presence of L5-s1 isthmic lysis and low-grade spondylolisthesis. Spine (Phila Pa 1976) 31, 2484–2490, https://doi.org/10.1097/01.brs.0000239155.37261.69 (2006).
Zhu, F. et al. Analysis of L5 incidence in normal population use of L5 incidence as a guide in reconstruction of lumbosacral alignment. Spine (Phila Pa 1976) 39, E140–146, https://doi.org/10.1097/brs.0000000000000069 (2014).
Hiyama, A. et al. Sagittal alignment of the cervical spine in adolescent idiopathic scoliosis: a comparative study of 42 adolescents with idiopathic scoliosis and 24 normal adolescents. European Spine Journal 25, 3226–3233, https://doi.org/10.1007/s00586-016-4701-3 (2016).
Hwang, S. W. et al. Cervical sagittal plane decompensation after surgery for adolescent idiopathic scoliosis: an effect imparted by postoperative thoracic hypokyphosis. Journal of Neurosurgery-Spine 15, 491–496, https://doi.org/10.3171/2011.6.spine1012 (2011).
Yagi, M. et al. Sagittal Cervical Alignment in Adolescent Idiopathic Scoliosis. Spine deformity 2, 122–130, https://doi.org/10.1016/j.jspd.2013.11.002 (2014).
Rajnics, P., Templier, A., Skalli, W., Lavaste, F. & Illes, T. The association of sagittal spinal and pelvic parameters in asymptomatic persons and patients with isthmic spondylolisthesis. Journal of spinal disorders & techniques 15, 24–30 (2002).
Oh, S.-K., Chung, S.-S. & Lee, C.-S. Correlation of Pelvic Parameters with Isthmic Spondylolisthesis. Asian Spine Journal 3, 21–26, https://doi.org/10.4184/asj.2009.3.1.21 (2009).
Lafage, V., Schwab, F., Patel, A., Hawkinson, N. & Farcy, J. P. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine 34, E599–606, https://doi.org/10.1097/BRS.0b013e3181aad219 (2009).
Vialle, R. et al. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. The Journal of bone and joint surgery. American volume 87, 260–267, https://doi.org/10.2106/jbjs.d.02043 (2005).
Harroud, A., Labelle, H., Joncas, J. & Mac-Thiong, J. M. Global sagittal alignment and health-related quality of life in lumbosacral spondylolisthesis. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 22, 849–856, https://doi.org/10.1007/s00586-012-2591-6 (2013).
Acknowledgements
This study was supported by National Natural Science Fund of China (81372012) and Natural Science Fund of Shanghai (17441900500). We are very grateful for the help of Charlotte Isler in polishing the English text in this article.
Author information
Authors and Affiliations
Contributions
M.L. and Z.Q.C.: conceived and designed the experiments. J.Z., and Y.Q.X.: performed the experiments. X.Z: analyzed the data. X.Z., J.Z. and Y.Q.X.: wrote the paper. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhao, J., Xiao, Y., Zhai, X. et al. Difference of Sagittal Alignment between Adolescents with Symptomatic Lumbar Isthmic Spondylolisthesis and the General Population. Sci Rep 8, 10956 (2018). https://doi.org/10.1038/s41598-018-29260-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-29260-6
This article is cited by
-
Lumbar degenerative disease after oblique lateral interbody fusion: sagittal spinopelvic alignment and its impact on low back pain
Journal of Orthopaedic Surgery and Research (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
