
Abstract
Serum uric acid level is a risk factor for cardiovascular disease (CVD). However, whether it is an independent risk factor or not remains controversial. We analyzed the association between serum uric acid level and cardiovascular risk. In total, 973 nonhypertensive and nondiabetic participants in the I-Lan Longitudinal Aging Study were eligible for this study. Subjects were divided into tertiles according to uric acid levels. The 10-year cardiovascular risk was calculated using Framingham risk score (FRS). Study subjects in the highest tertile of serum uric acid level were older, more likely to be male, and had higher systolic blood pressure, body mass index, carotid artery intima–media thickness and serum triglyceride, high-sensitivity C-reactive protein, and low-density lipoprotein cholesterol levels and lower serum high-density lipoprotein cholesterol levels (all p < 0.05). Subjects in the highest tertile had significantly higher FRS (p < 0.001). After adjusting for other risk factors, serum uric acid level remained associated significantly with the FRS (p < 0.05). In binary logistic regression analysis, the serum uric acid level was an independent predictive factor for high (≥20%) FRS (odds ratio 1.33, 95% confidence interval 1.10–1.68). These findings warrant attention to this cardiovascular risk factor in apparently healthy adults.
Similar content being viewed by others
Introduction
An increased serum uric acid level is a common finding in patients with hypertension, insulin resistance, obesity, and cardiovascular disease (CVD). Moreover, high uric acid levels have been found to be associated with higher incidences of diabetes, hypertension, and chronic kidney disease. An elevated serum uric acid level has been considered to be a risk factor for CVD. However, debate remains about whether such elevation is an independent predictor of cardiovascular risk. Uric acid elevation has been proposed to be a compensatory mechanism to counteract oxidative damage related to atherosclerosis1. Nevertheless, the hypothesis that reduction of the serum uric acid level could prevent CVD has not been tested. The serum uric acid level probably reflects and integrates different risk factors and their possible interactions.
In the current study, we investigated the association between serum uric acid concentration and cardiovascular risk in nonhypertensive and nondiabetic individuals, with the aim of minimizing potential unwanted interactions. An understanding of the clinical significance of this relationship may prompt earlier surveillance of the serum uric acid level in asymptomatic individuals, and result in the identification of populations at high risk of CVD.
Results
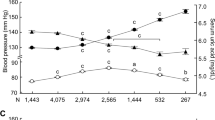
Data from 973 nonhypertensive and nondiabetic ILAS participants (46.8% men, mean age 61.7 ± 8.6 years, range 50–89 years) were analyzed. Table 1 summarizes the demographic and clinical characteristics of the study subjects. The subjects were divided into tertiles according to serum uric acid concentration (first tertile, <5.0 mg/dl; second tertile, 5.0–6.1 mg/dl; third tertile, >6.1 mg/dl).
Study participants in the third tertile of serum uric acid level were older, more likely to be male, and had higher SBP, BMI, and serum triglyceride and LDL-C levels and lower HDL-C levels (all p < 0.05). Subjects with higher serum uric acid levels also had significantly enhanced high-sensitivity C-reactive protein levels and increased cIMT (both p < 0.005).
Table 2 shows coefficients of correlation between the serum uric acid level and the FRS and other cardiovascular risk factors. The serum uric acid level was correlated positively with the FRS, age, SBP, BMI, triglyceride level, LDL-C level, high-sensitivity C-reactive protein level, smoking, and cIMT (all p < 0.01), but negatively with the HDL-C level and glomerular filtration rate (GFR) (both p < 0.01). In multivariate analysis, the correlation between the serum uric acid level and the FRS remained significant after adjustment for age, BMI, SBP, triglyceride level, LDL-C level, HDL-C level, GFR, high-sensitivity C-reactive protein level, cIMT, and smoking (p = 0.002; Table 3, model 3).
The study subjects were separated into three groups according to the FRS. Two hundred forty-three subjects were assigned to the high-risk group (FRS ≥ 20%), 256 were assigned to the intermediate-risk group (FRS 10–20%), and 474 were assigned to the low-risk group (FRS ≤ 10%). The serum uric acid level differed significantly among groups (p < 0.001); it was significantly higher in the high-risk group than in the intermediate-risk and low-risk groups [6.5 mg/dl vs. 6.1 mg/dl (p = 0.001) and 5.1 mg/dl (p < 0.001), respectively].
Binary logistic regression analysis was also performed to define the predictive value of the serum uric acid level for high (≥20%) FRS. Age, BMI, SBP, HDL-C level, triglyceride level, and GFR were included in the analysis. A high serum uric acid level was found to be associated independently with a high FRS (odds ratio 1.33, 95% confidence interval 1.10–1.68; Table 4).
Discussion
The main question addressed in this study was whether the serum uric acid level is an independent risk factor for CVD in nonhypertensive and nondiabetic individuals. Our findings demonstrate that elevated serum uric acid levels were associated independently with high FRS after adjustment for other potential confounding risk factors. Of note, the uric acid level was also associated with the high-sensitivity C-reactive protein level and cIMT, markers of systemic inflammation and preclinical atherosclerosis. These findings provide pivotal evidence that elevated uric acid concentrations may increase CVD risk and represent a potential therapeutic target in the primary prevention of CVD.
Uric acid is a major product of purine metabolism. In adults, the serum uric acid level varies with body weight, height, blood pressure, renal function, and alcohol intake2. Uric acid levels are also affected by numerous conditions, including obesity, hypertension, diabetes, hyperlipidemia, and renal disease, and by diuretic use3,4. Moreover, a previous report showed that hyperuricemia was associated with insulin resistance and metabolic syndrome in essentially health subjects5.
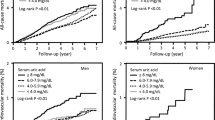
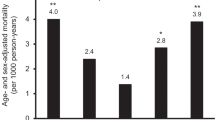
The association between uric acid and CVD has been discussed since the 1950s6. However, the clinical relevance of uric acid in CVD remains controversial. The National Health and Nutrition Examination Survey I Follow-Up Study, in which 5,926 subjects with 16.4 years of follow up were enrolled, demonstrated that increased serum uric acid levels were associated significantly with a higher risk of cardiovascular mortality7. After controlling for potential risk factors, this association persisted, even in subjects with low cardiovascular risk. Similar results were obtained in a prospective study of middle-aged Finnish men8. The uric acid concentration is a strong predictor of cardiovascular mortality in men without clinical CVD and diabetes. Data from another epidemiological longitudinal survey also showed serum uric acid is a predictor of long-term incidence of CVD events, deaths and all-cause mortality9. In addition, a gender difference in the association between serum uric acid and CVD incidence has been reported. The association was more strongly in women than in men10. Our study extends previous findings to further support the link between a high serum uric acid level and CVD.
In contrast, some epidemiological studies have indicated that the serum uric acid level is not independent of other established risk factors for CVD11,12,13 In a community-based, prospective observational study in which 6,763 Framingham Heart Study participants were followed, the positive association between the serum uric acid level and cardiovascular events was not sustained after accounting for other risk factors11. The greatest difficulty in clarifying this debate stems from the frequent association of the circulating uric acid concentration with other cardiovascular risk factors, such as hypertension, chronic kidney disease, metabolic syndrome, diabetes, and smoking. Accordingly, previous studies have been limited in their ability to elucidate the causal role of uric acid in CVD.
Several experimental and clinical studies have refueled the debate. Uric acid has been found to impair nitric oxide synthesis, resulting in vascular endothelial dysfunction14. Not surprisingly, similar effects were observed in patients with hyperuricemia. Flow-mediated vasodilation, representative of endothelial function, was significantly lower in hyperuricemic patients than in a control group15. Endothelial dysfunction, characterized by the alteration of the vascular lining, is prone to pro-thrombotic, pro-inflammatory, and pro-constrictive. Our recent data suggest an association between a previous history of gout attack and the risk of deep vein thrombosis16. Furthermore, endothelial dysfunction is associated with arterial stiffness and the development of hypertension. Emerging evidence also demonstrates links between the uric acid level and wave reflection and arterial stiffness17,18.
The findings of numerous studies support the relationship between serum uric acid and CVD. Zoppini et al.19 reported that higher uric acid levels were associated with an increased risk of cardiovascular mortality in patients with type 2 diabetes after adjustment for other risk factors, including age, sex, BMI, smoking, hypertension, dyslipidemia, diabetes duration, HbA1c level, medication use, and renal function. In this large cohort study, we demonstrated that enhanced uric acid levels were associated with increased systemic inflammation, preclinical atherosclerosis, and future cardiovascular risk. However, whether reduction of the uric acid concentration in hyperuricemic patients could have beneficial effects, reducing cardiovascular morbidity and mortality, remains unknown. Further large prospective studies are warranted to verify this hypothesis.
Some possible limitations of this study should be mentioned. First, given the cross-sectional design, we could not establish a causal relationship between uric acid elevation and CVD. The study results obtained from an observational analysis. Moreover, our participants were healthier than the general population of community-dwelling older adults because we excluded those with hypertension, diabetes, and disability. Finally, a future prospective study is needed to determine whether the serum uric acid level is an independent predictor of long-term cardiovascular outcomes, and whether its reduction could reduce the occurrence of adverse cardiovascular events.
In conclusion, the serum uric acid level was associated significantly with the FRS in nonhypertensive and nondiabetic individuals. Further prospective studies are required to determine whether reduction of the uric acid concentration has beneficial effects, reducing cardiovascular risk.
Methods
Study design and population
The I-Lan Longitudinal Aging Study (ILAS) is a community-based aging cohort study conducted in I-Lan County, Taiwan20. Community-dwelling adults aged > 50 years were randomly sampled through the household registries of the county government in Yuanshan Township. Selected residents were invited by the research team to participate, and informed consent was obtained from all participants. The inclusion criteria were: (i) residence in I-Lan County with no plan to move in the near future and (ii) age >50 years. Respondents that met any one of the following conditions were excluded from the study: (i) inability to communicate with the interviewer; (ii) poor functional status that could lead to failure of evaluation, such as inability to complete a 6-m timed walk within a reasonable period of time; (iii) limited life expectancy (<6 months) because of major illness; (iv) presence of an implant contraindicating magnetic resonance imaging; and (v) current institutionalization.
In total, 1,798 inhabitants of I-Lan County were enrolled. After the further exclusion of participants with hypertension and/or diabetes (214 had hypertension and diabetes, 526 had hypertension, and 85 had diabetes), 973 participants remained eligible for this study. The institutional review board of National Yang-Ming University approved the research as a whole. All research was performed in accordance with relevant regulations.
Demographic data collection and physical examination
Participants’ medical histories, including information about conventional cardiovascular risk factors, and current drug treatments were obtained during personal interviews and from medical files. Each participant’s weight, height, and waist circumference were measured, and the body mass index (BMI) was calculated. Brachial blood pressure was accessed with a mercury sphygmomanometer after patients sat for ≥15 min. The average of three systolic blood pressure (SBP) measurements was used for the analysis.
Framingham risk score
The Framingham risk score (FRS) is a widely accepted formulation for CVD prediction that has been validated in large population studies21. The Framingham Heart Study group provided several risk prediction equations for CVD, coronary heart disease, congestive heart failure, and atrial fibrillation. Among these equations, we adapted the equation used to calculate the 10-year risk of CVD development for this study. The suggested equation considered age, sex, high blood pressure, smoking, hyperlipidemia, and diabetes to be the major risk factors for CVD development. The equation incorporates multivariate analysis with calculation of a regression coefficient for each possible risk factor.
Carotid ultrasonography
Carotid ultrasonography was performed with an ultrasound system (GE LOGIQ 400 PRO; GE, Cleveland, OH, USA). A well-trained technician performed measurements for all participants. Images were obtained bilaterally of the proximal to distal common carotid artery (CCA), the carotid bifurcations, and the origin of the internal carotid arteries. The carotid intima–media thickness (cIMT) was measured at a site with no discrete plaque along a 10-mm-long segment of the far wall of the CCA. The average of the bilateral cIMTs was calculated for analysis22.
Laboratory measurement
All blood samples were drawn with the participant in the seated position after a 10-h overnight fast. Serum concentrations of glucose, uric acid, total cholesterol, triglycerides, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) and high-sensitivity C-reactive protein were determined using an automatic analyzer (ADVIA 1800; Siemens, Malvern, PA, USA). Whole-blood glycated hemoglobin A1c (HbA1c) was measured by an enzymatic method using the Tosoh G8 HPLC Analyzer (Tosoh Bioscience, Inc., San Francisco, CA, USA).
Statistical analysis
The complete dataset was analyzed, and results were expressed as means ± standard deviations or as frequencies and percentages. Comparisons among the three groups were made by analysis of variance, the Kruskal–Wallis test, or the chi-squared test, as appropriate. The chi-squared test was used for subgroup comparisons of categorical variables. Linear regression analysis was performed to evaluate the association between the serum uric acid level and FRS. Data were analyzed using SPSS software (version 20; SPSS Inc., Chicago, IL, USA). Two-tailed p values < 0.05 were considered to indicate statistical significance.
References
Nieto, F. J., Iribarren, C., Gross, M. D., Comstock, G. W. & Cutler, R. G. Uric acid and serum antioxidant capacity: a reaction to atherosclerosis? Atherosclerosis 148, 131–139 (2000).
Nishioka, K. & Mikanagi, K. Hereditary and environmental factors influencing on the serum uric acid throughout ten years population study in Japan. Advances in experimental medicine and biology 122A, 155–159 (1980).
Benedek, T. G. Correlations of serum uric acid and lipid concentrations in normal, gouty, and atherosclerotic men. Annals of internal medicine 66, 851–861 (1967).
Steele, T. H. & Oppenheimer, S. Factors affecting urate excretion following diuretic administration in man. The American journal of medicine 47, 564–574 (1969).
Bonora, E. et al. Relationship of uric acid concentration to cardiovascular risk factors in young men. Role of obesity and central fat distribution. The Verona Young Men Atherosclerosis Risk Factors Study. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity 20, 975–980 (1996).
Gertler, M. M., Garn, S. M. & Levine, S. A. Serum uric acid in relation to age and physique in health and in coronary heart disease. Annals of internal medicine 34, 1421–1431 (1951).
Fang, J. & Alderman, M. H. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. Jama 283, 2404–2410 (2000).
Niskanen, L. K. et al. Uric acid level as a risk factor for cardiovascular and all-cause mortality in middle-aged men: a prospective cohort study. Archives of internal medicine 164, 1546–1551, https://doi.org/10.1001/archinte.164.14.1546 (2004).
Puddu, P. E. et al. Serum uric acid and eGFR_CKDEPI differently predict long-term cardiovascular events and all causes of deaths in a residential cohort. International journal of cardiology 171, 361–367, https://doi.org/10.1016/j.ijcard.2013.12.029 (2014).
Puddu, P. E., Schiariti, M. & Torromeo, C. Gender and Cardiovascular Mortality in Northern and Southern European Populations. Current pharmaceutical design 22, 3893–3904 (2016).
Culleton, B. F., Larson, M. G., Kannel, W. B. & Levy, D. Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Annals of internal medicine 131, 7–13 (1999).
Moriarity, J. T., Folsom, A. R., Iribarren, C., Nieto, F. J. & Rosamond, W. D. Serum uric acid and risk of coronary heart disease: Atherosclerosis Risk in Communities (ARIC) Study. Annals of epidemiology 10, 136–143 (2000).
Wheeler, J. G., Juzwishin, K. D., Eiriksdottir, G., Gudnason, V. & Danesh, J. Serum uric acid and coronary heart disease in 9,458 incident cases and 155,084 controls: prospective study and meta-analysis. PLoS medicine 2, e76, https://doi.org/10.1371/journal.pmed.0020076 (2005).
Choi, Y. J. et al. Uric acid induces endothelial dysfunction by vascular insulin resistance associated with the impairment of nitric oxide synthesis. FASEB journal: official publication of the Federation of American Societies for Experimental Biology 28, 3197–3204, https://doi.org/10.1096/fj.13-247148 (2014).
Ho, W. J. et al. Association between endothelial dysfunction and hyperuricaemia. Rheumatology 49(1929–1934), 184, https://doi.org/10.1093/rheumatology/keq. (2010).
Chiu, C. C. et al. Association between previous history of gout attack and risk of deep vein thrombosis - a nationwide population-based cohort study. Scientific reports 6, 26541, https://doi.org/10.1038/srep26541 (2016).
Canepa, M. et al. Longitudinal Association Between Serum Uric Acid and Arterial Stiffness: Results From the Baltimore Longitudinal Study of Aging. Hypertension 69, 228–235, https://doi.org/10.1161/HYPERTENSIONAHA.116.08114 (2017).
Hsu, P. F. et al. Associations of serum uric acid levels with arterial wave reflections and central systolic blood pressure. International journal of cardiology 168, 2057–2063, https://doi.org/10.1016/j.ijcard.2013.01.164 (2013).
Zoppini, G. et al. Elevated serum uric acid concentrations independently predict cardiovascular mortality in type 2 diabetic patients. Diabetes care 32, 1716–1720, https://doi.org/10.2337/dc09-0625 (2009).
Liu, L. K. et al. Sarcopenia, and its association with cardiometabolic and functional characteristics in Taiwan: results from I-Lan Longitudinal Aging Study. Geriatrics & gerontology international 14(Suppl 1), 36–45, https://doi.org/10.1111/ggi.12208 (2014).
D’Agostino, R. B. Sr. et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation 117, 743–753, https://doi.org/10.1161/CIRCULATIONAHA.107.699579 (2008).
Chang, C. C. et al. Association between frailty and carotid intima media thickness and inflammatory marker in an elderly population. Geriatrics & gerontology international. https://doi.org/10.1111/ggi.13099 (2017).
Acknowledgements
This study was supported in part by research grants from the Novel Bioengineering and Technological Approaches to Solve Two Major Health Problems in Taiwan program, sponsored by the Taiwan Ministry of Science and Technology Academic Excellence Program (MOST-106-2633-B-009-003); Taipei Veterans General Hospital (VGH-V100E2-002 and VGHUST103-G7-2-1); the National Taiwan University Hospital, Hsinchu Branch (HCH104-10 and HCH105-7); and the Ministry of Science and Technology (MOST-105-2314-B-002-119, 106-2314-B-002-173-MY3, MOHW 106-TDU-B-211-113001). The funding institutions took no part in the study design, data collection or analysis, publication intent, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
Authors C.C., Chang, R.H., Chou and C.S. Kuo contributed to the conception and design of the work. Authors L.K., Liu and L.K., Chen acquired the data, and C.C. Chang performed the analysis. All authors were involved in the interpretation of data. C.C. Chang, C.H., Wu, P.H., Huang and S.J., Lin drafted the work, which was critically revised by all other authors. All authors approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chang, CC., Wu, CH., Liu, LK. et al. Association between serum uric acid and cardiovascular risk in nonhypertensive and nondiabetic individuals: The Taiwan I-Lan Longitudinal Aging Study. Sci Rep 8, 5234 (2018). https://doi.org/10.1038/s41598-018-22997-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-22997-0
This article is cited by
-
Metabolomic signatures of ideal cardiovascular health in black adults
Scientific Reports (2024)
-
High serum uric acid trajectories are associated with risk of myocardial infarction and all-cause mortality in general Chinese population
Arthritis Research & Therapy (2022)
-
Dissecting the clinical relevance of polygenic risk score for obesity—a cross-sectional, longitudinal analysis
International Journal of Obesity (2022)
-
The effects of vitamin D3 supplementation on TGF-β and IL-17 serum levels in migraineurs: post hoc analysis of a randomized clinical trial
Journal of Pharmaceutical Health Care and Sciences (2021)
-
Endothelial dysfunction in neuroprogressive disorders—causes and suggested treatments
BMC Medicine (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
