
Abstract
The association between nutritional status and gait speed remains unclear. This study described gait speed in older adults and quantified the association between overweight, obesity, undernutrition risk and gait speed. Gait speed as potential indicator of nutritional outcomes was also explored. A cross-sectional analysis was conducted in a population-based sample of 1,500 older adults ≥65 years old. Compared to “normal body mass index” women, odds ratio for a slow gait speed was approximately 2-fold higher in“overweight”, 4-fold higher in “obese” and 6-fold higher in women at “undernutrition risk”. “Undernutrition risk” category resulted from joining “undernutrition risk/undernutrition”. For men, these associations were in the same direction, but the odds ratio estimates halved. In women, identified gait speed cut-offs were 0.87 m/s for “obesity” and 0.79 m/s for “undernutrition risk”. In men, 0.94 m/s is the cut-off in which most older adults were correctly classified relative to “undernutrition risk”. About half of Portuguese older adults presented a gait speed ≤0.8 m/s. Overweight, obesity and undernutrition risk were directly and increasingly associated with slow gait speed, but approximately twice as high in women compared to men. Gait speed revealed potential utility in marking nutritional problems, but further investigation is recommended.
Similar content being viewed by others

Introduction
Older adults have a higher risk of age-related decline in functional performance and gait speed is used for functional assessment as it is a reliable, easy, quick, non-expensive and informative measurement1,2.
A poor nutritional status is also prevalent in the elderly3,4. In the oldest European population, overweight and obesity constitute a growing public health challenge3. In turn, undernutrition risk and undernutrition were observed in 60% of institutionalized older adults and in 11% of those living in the community4. Particularly in this age group, undernutrition can coexist with overweight and obesity5.
Functional performance is closely associated with nutritional well-being in older populations3,6. Handgrip strength is used to assess functional status for identification of undernutrition, but it is not appropriate for use in some populations with upper limb deformities and it cannot replace evaluation of lower extremity strength7. Gait speed could be a very informative measure in situations where it is not appropriate to measure handgrip strength. Misu et al. recently studied the association between undernutrition and gait speed among 204 community-dwelling older adults, and their results suggested that undernutrition status affects lateral trunk control during walking8. However, the association between undernutrition and gait speed has been scarcely investigated. Moreover, the association between overweight and gait speed remains to be explored and gait speed cut-offs associated with poor nutritional status are not yet defined.
This study aimed to describe gait speed in a nationwide sample of older adults and to quantify the association between overweight, obesity, undernutrition risk and gait speed. Furthermore, the usefulness of gait speed as a potential indicator of poor nutritional outcomes in older adults was also explored.
Methods
Study and sample design
A cross-sectional observational study was conducted in Portugal, in a cluster sample of 1,500 older adults ≥65 years old, between December 2015 and June 2016, in accordance with “The Nutrition UP 65 Study Protocol”9.
Data from the 2011 Census was used to obtain a nationally representative sample of Portuguese older adults in terms of sex, age, educational level and residence area defined in the Nomenclature of Territorial Units for Statistical purposes9. A random, stratified and cluster sampling method was applied. Three or more town councils with >250 inhabitants were randomly selected by each regional area. The potential participants were contacted directly at home by door knocking, through telephone or institutions, such as town councils and parish centres. Individuals were considered eligible if they had Portuguese nationality with current tax residence in Portugal, and if they were aged ≥65 years9. The initial sample was composed of 5% of older adults in nursing homes, a proportion similar to that of the Portuguese population9. The participant was considered a community-dwelling individual if he slept in his own house or in the house of a family member or a friend more than half of the days in the preceding month9. Written informed consent was obtained from older adults or their legally authorized representatives, depending on cognitive status.
Data collection and variable definition
Eight interviewers worked on data collection during this period. All interviewers were previously trained, in order to improve intra and inter interviewer agreement, and the corresponding errors were obtained for anthropometric values. Intra-interviewer error ranged from 0.05% to 0.34% and inter-interviewer error varied between 0.19% and 1.48%. These values are considered acceptable for trained anthropometrists9.
Demographic data included information on sex, date of birth and education level determined by the number of completed school years.
Cognitive performance was assessed by the version of Mini Mental State Examination validated for the Portuguese population9,10. The cut-off scores for cognitive impairment were as follows: individuals with no education, <15 points; 1 to 11 years of years of school completed, <22 points; and >11 years of school completed, <27 points9,10. For individuals identified as presenting cognitive impairment, reported data was provided by a person close to the participant, such as a family member or caregiver.
Self-reported sitting time, data on chronic diseases and about self-perceived health status, as well as anthropometric and functional parameters, were measured and collected according to the standard procedures previously published in “The Nutrition UP 65 Study Protocol”9.
Poor nutritional status, namely overweight and obesity were identified using the BMI cut-offs of the World Health Organization criteria11. Undernutrition was identified using the Portuguese version of the Mini-Nutritional Assessment® - Short Form (MNA-SF)9,12. It is a valid nutritional screening tool for free-living and clinically relevant older populations, recommended by the European Society for Clinical Nutrition and Metabolism (ESPEN)13. The MNA-SF contains geriatric-specific assessment questions related to nutritional and health status, namely questions about possible food intake decline, weight loss during the previous three months, mobility, possible psychological stress or acute disease in the previous three months and neuropsychological problems12. Participants were considered undernourished if the final MNA-SF score was ≤7 points and they were considered at risk of undernutrition if the final MNA-SF score was between 8 and 11 points. Participants with a score ≥12 points were classified without undernutrition risk/undernutrition12,13. Considering the small proportion of participants classified as undernourished in the initial sample (n = 19, 1.3%), both undernourished and participants at risk of undernutrition were grouped together in a single category of “undernutrition risk/undernutrition”. From now on, for simplicity, “undernutrition risk/undernutrition” will be cited as “undernutrition risk”.
Categories of nutritional status
In the initial sample, there were 37 (2.5%) cases of missing gait speed records and gait speed was not evaluated in 27 (1.8%) individuals due to mobility restrictions. In 11 (0.7%) cases, there were missing variables related to self-reported chronic diseases. The following categories of nutritional status were considered for 1,425 participants, corresponding to 95% of the total original dataset:
-
“normal BMI”, which included participants with a BMI between 18.5 and 24.9 kg/m2 and without undernutrition risk according to a MNA-SF ≥ 12 points. This category was used as reference;
-
“overweight”, which included participants with a BMI between 25.0 and 29.9 kg/m2 and without undernutrition risk according to a MNA-SF ≥ 12 points;
-
“obesity”, which included participants with a BMI ≥ 30.0 kg/m2 and without undernutrition risk according to a MNA-SF ≥ 12 points;
-
“undernutrition risk”, a category for participants with a MNA-SF score < 12 points. This category included participants with normal BMI, overweight and obesity.
Gait speed
Gait speed was calculated for each participant using distance in meters and time in seconds9,14. It was obtained by dividing the distance travelled 4.6 m, on a flat and unobstructed path, by the time to cover that distance. The distance was marked on the floor with a visible tape. The study incorporated an additional distance of 2 m for acceleration and a further 2 m for deceleration9,14. The following instruction was given to the participant: “I will say ready, set, go. When I say go, walk at your normal and comfortable pace until I say stop”9,14. The walking time was registered with a stopwatch with a resolution of 0.01 s (School Electronic Stopwatch, Dive049, Topgim, Portugal).
Ethics approval and consent to participate
This study was conducted according to the guidelines of the Declaration of Helsinki. Potential participants were contacted by the interviewer, who provided information about the study purposes and methodology, and invited them to participate. In cases of acceptance, cognitive performance was assessed by the version of Mini Mental State Examination validated for the Portuguese population with cut-offs depending on the educational level10. Individuals without cognitive impairment were asked to read and sign a duplicated informed consent form. If the participant was deemed to be cognitively impaired, two representatives were asked to read and sign the duplicated informed consent form. And so, in this way, written informed consent was obtained from participants or their legally authorized representatives.
The study protocol was approved by the Ethics Committee of Social Sciences and Health from Faculty of Medicine of University of Porto, Portugal (PCEDCSS – FMUP 15/2015) and by the Portuguese National Commission of Data Protection (9427/2015).
Statistical analysis
A sensitivity analysis was carried out comparing the mean values of all variables between excluded and included individuals. The purpose of this analysis was to determine if the excluded older adults differed from those included in the present study, in order to evaluate potential results bias. Excluded individuals were older (mean age of 76.7 ± 7.9 years), compared to participants in the remaining sample (mean age of 74.9 ± 7.0 years), p = 0.032. However, in relation to all other variables, including gait speed, BMI and nutritional status, significant differences were not found.
Characteristics of the sample were presented stratified by sex and by gait speed. The median of the sample distribution (0.8 m/s) was used to establish a cut-off of gait speed, because there are no validated gait speed cut-offs for nutritional outcomes. Categorical variables were presented as counts and proportions and were compared using the chi-square test. The normality of variables distribution was examined with the Kolmogorov-Smirnov test. Means and standard deviation values were calculated and compared using the Student’s t-test and Anova test.
A logistic regression model was used to estimate the probability of a gait speed ≤0.8 m/s according to poor nutritional status, stratified by sex. Chi-square test for trend was estimated. Odds ratio and 95% confidence intervals were estimated adjusting for age, height, mid-arm muscle circumference, Mini Mental State Examination score, self-reported sitting time and for the number of chronic diseases, as continuous variables.
Receiver operating characteristic (ROC) curves were constructed to evaluate the performance of gait speed adjusted for height (gait speed/height) to identify poor nutritional outcomes, particularly obesity and undernutrition. The areas under the curves (AUCs) and their 95% confidence intervals were also calculated. The AUC should be >0.5 in an effective screening test, an AUC = 0.5 indicates that the screening test is no better than chance. Sensitivities, specificities and positive likelihood ratios (LR), for describing the ability of gait speed to identify poor nutritional outcomes, were also calculated. Likelihood ratio is an alternative method for evaluating the value of a diagnostic test. It expresses “the probability that a given test result would occur in a person with the target disorder divided by the probability that the same result would occur in a person without that disorder” and positive LR is attained through the formula: LR = sensitivity/(1 − specificity)15. Values between 0 and 1 show the decrease in post-test probability of having poor nutritional outcomes according to low gait speed values15. Values higher than 1 show the increase of post-test probability of having poor nutritional outcomes according to low gait-speed values15.
Results were considered significant when p < 0.05.
Results
Participants’ age ranged from 65 to 100 years and gait speed ranged from 0.18 to 2.25 m/s, with a median of 0.84 m/s.
In this nationwide sample, 16.6% of participants were classified with normal BMI, 44.6% with overweight and 38.9% with obesity. In the total sample, 15.2% of individuals were included in the “undernutrition risk” category and among these participants, 27.2% had a normal BMI, 35.5% were overweight and 37.3% were obese.
Characteristics of the sample are summarized in Table 1. According to the gait speed cut-off (0.8 m/s), statistically significant differences in BMI were observed among women, but not in men. Women with slow gait speed had higher BMI than women with high gait speed values (p < 0.001).
Compared to women with “normal BMI”, the odds ratio for a gait speed ≤0.8 m/s was approximately 2-fold higher in women with “overweight”, 4-fold higher in women with “obesity” and 6-fold higher in women with “undernutrition risk” (p for trend: <0.001) (Table 2). For male older adults, these associations were in the same direction but the odds ratio estimates halved (p for trend: 0.001) (Table 2). These estimates were independent of factors such as age, height, mid-arm muscle circumference, Mini Mental State Examination score, self-reported sitting time and number of chronic diseases (Table 2).
Participants with “normal BMI” had a gait speed mean of 0.95 m/s (women) and 0.99 m/s (men), those with “overweight” had a mean of 0.89 m/s (women) and 1.01 m/s (men), participants with “obesity” had a mean of 0.79 m/s (women) and 0.94 m/s (men), participants at “undernutrition risk” had a mean of 0.72 m/s (women) and 0.84 m/s (men) (p < 0.001 for each sex, according to nutritional status categories). For both sexes, no statistically significant differences were found between the gait speed of participants without obesity and gait speed of obese participants in the “undernutrition risk” category.
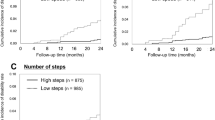
Results on the performance of gait speed adjusted for height to identify poor nutritional outcomes are displayed in Table 3 and Fig. 1. For women with “obesity” and at “undernutrition risk”, LR were >1 and AUCs of ROC curves were >0.5 and statistically significant (p < 0.001) (Table 3 and Fig. 1A,B). In women, identified gait speed cut-offs were 0.87 m/s for “obesity” and 0.79 m/s for “undernutrition risk” (Table 3).

Sex-specific ROC curves of gait speed (adjusted for height) for undernutrition risk/undernutrition (A and C) and for obesity without undernutrition risk (B and D).
For men at “undernutrition risk”, the gait speed of 0.94 m/s was the value in which most older adults were correctly classified (Table 3). A sensitivity of 0.768, a specificity of 0.460, a LR > 1 and an AUC > 0.5 were estimated (p = 0.001) (Table 3 and Fig. 1C). The ROC curve was not statistically significant for men with “obesity” (p = 0.521) (Fig. 1D).
Discussion
In the present study, the association between overweight, obesity, undernutrition risk and gait speed in older adults was explored and results have shown that they are directly and increasingly associated with slow gait speed.
According to the literature, mobility impairment is defined as a usual gait speed ≤0.8 m/s, because this cut-off predicts disability and reduced overall survival16. This value coincides approximately with the median of gait speed in our sample and was used to establish a cut-off. Consequently, it is worrying that such a large proportion of older adults revealed mobility impairment. Changes related to the aging process and poor nutritional outcomes can explain the low gait speed values found among our participants. Firstly, it is known that in older populations, the general decrease in muscle strength due to loss of motor neurons, muscle fibers and aerobic capacity, is associated with a decreased gait speed and consequent adaptation17. This study sample is particularly prone to these disabilities due to the participants’ old age, with a median of 74 years. Secondly, obesity has been consistently associated with an increased risk of deterioration in physical functionality among older adults18. Therefore, the high proportion of participants with overweight and obesity can also explain gait speed results. Even among participants who were at “undernutrition risk”, more than half were also overweight or obese.
Overweight and obesity exerts an excessive load on body and knee joints leading on shorter step length that prompts slower gait speed19. Mechanisms that underlie the association between obesity and gait speed may also be mediated by several cytokines secreted from adipose tissue and consequent chronic inflammation20,21. Recently, potential obesity-related differences in neural activity during ambulation in older adults were reported22. Otherwise, a slow gait speed can also lead to obesity by decreased physical activity and increased sedentary lifestyle23. It is important to note that present analysis relies on cross-sectional data and temporal relationships could not be inferred. Therefore, we explored both possible scenarios: the association between nutritional status and gait speed, and gait speed as a potential functional marker of these problems.
In turn, undernutrition is strongly related with low muscle mass and strength which can also explain a low gait performance24,25. Recent research demonstrated that undernutrition can affect lateral trunk control during walking8. Among community-dwelling older adults, gait speed was also associated with MNA score, used to assess nutritional status26. These findings corroborate our results concerning the association between undernutrition and low gait speed. However, it is important to emphasize that the “undernutrition risk” category included overweight/obese participants.
The coexistence of undernutrition with obesity is now a reality which has been connected to higher dependence on the activities of daily living and with aggravation of mobility impairment among community-dwelling older adults5,27. Undernutrition is often associated with sarcopenia which is characterized by an age-related decline in muscular strength and functional ability27. It has been suggested that the association between low muscle mass and functional decline is explained by underlying muscle strength28. The coexistence of sarcopenia with obesity is also now a reality named sarcopenic obesity, which may carry the cumulative risk derived from each of the two individual body composition phenotypes29,30. Despite these facts, a sensitivity analysis conducted in our sample did not present statistically significant differences between gait speed of participants at undernutrition risk without obesity and gait speed of those at undernutrition risk with obesity.
According to the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition, there is no single parameter that is definitive for recognition of undernutrition in adults and older adults6. The identification of two or more of a set of six defined characteristics is recommended for undernutrition diagnosis, among which handgrip strength is included as functional measure6.
Handgrip strength has been showing a good predictive validity identifying those patients with a higher length of hospital stay31,32. However, handgrip strength cannot replace the assessment of functionality of lower limbs or the assessment of activities of daily living. This study is a first step towards knowing if gait speed may be an alternative functional measure, when the measurement of handgrip strength is not possible.
In the present sample, overweight, obesity and undernutrition were directly and increasingly associated with slower gait speed, but more strongly in women than in men. In line with our results, it was previously reported that elevations of several baseline adiposity measures were associated with a decline in gait speed, but also more strongly in women than in men33. Gender differences may be explained by the differences in body composition34,35. Body mass index use as a surrogate indicator of adiposity can be prone to errors because fat mass and fat free mass are not differentiated34, even though present results have been adjusted for the mid-arm muscle circumference. In men, the contribution of skeletal muscle mass to the total body weight is higher than in women, while in women, the proportion of fat mass/skeletal muscle mass is generally higher than in men35,36. Consequently, the association between overweight/obesity assessed through BMI and low gait speed can become more evident in women than in men.
In addition, although there is no data on the frequency of hip osteoarthritis in our sample, differences according to sex in the relation between obesity, hip damage and gait speed37,38 are also a potential explanation of why in the present study obesity was more strongly associated with low gait speed in women than in men.
Regarding the performance of gait speed to identify older adults presenting poor nutritional outcomes, although sensitivities higher than 65% were found, the specificities were relatively low. These sensitivity values are within the acceptable ranges for nutritional assessment tools39 and can be regarded as a strength because a sensitive test is more useful at an early stage of nutritional assessment, since it identifies high proportion of those older adults who present poor nutritional outcomes39. Because specific tests are useful in confirming a diagnosis that has been suggested by other procedures39 the low specificity cannot be interpreted as a major problem, however it is obviously desirable to have a test that is both highly sensitive and highly specific39.
Nevertheless, this is an exploratory study that displays preliminary results concerning the potential capacity of gait speed to identify poor nutritional outcomes. Further research should be conducted, comparing the ability of slow gait speed relative to a standard functional assessment methodology, in order to identify these poor nutritional outcomes.
This study is one of the first to explore gait speed as afunctional measure associated with poor nutritional outcomes in older adults, not only with undernutrition, but also with overweight and obesity. Imbalances in groups sizes may have been a limitation. However, in the present sample, other hypotheses of stratification according to nutritional outcomes were not feasible because of the high prevalence of overweight and obesity.
Conclusion
About half of Portuguese older adults presented a gait speed ≤0.8 m/s. Overweight, obesity and undernutrition risk were directly and increasingly associated with a slow gait speed, but this association was approximately twice as high in women compared to men. Gait speed revealed potential utility as a marker of nutritional problems, but further investigation is required to understand its ability to be part of a screening or assessment method of nutritional status dysfunctions.
References
Beaton, K., McEvoy, C. & Grimmer, K. Identifying indicators of early functional decline in community-dwelling older people: a review. Geriatr Gerontol Int. 15(2), 133–40 (2015).
Inzitari, M. et al. [Do you measure gait speed in your daily clinical practice? A review]. Rev Esp Geriatr Gerontol. 52(1), 35–43 (2017).
Asp, M., Simonsson, B., Larm, P. & Molarius, A. Physical mobility, physical activity, and obesity among elderly: findings from a large population-based Swedish survey. Public Health. 147, 84–91 (2017).
Kaiser, M. J. et al. Prospective validation of the modified mini nutritional assessment short-forms in the community, nursing home, and rehabilitation setting. J Am Geriatr Soc. 59(11), 2124–8 (2011).
Molino, S., Dossena, M., Buonocore, D. & Verri, M. Sarcopenic Obesity: An Appraisal of the Current Status of Knowledge and Management in Elderly People. J Nutr Health Aging. 20(7), 780–8 (2016).
White, J. V., Guenter, P., Jensen, G., Malone, A. & Schofield, M. Academy of Nutrition and Dietetics Malnutrition Work Group; A.S.P.E.N. Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 112(5), 730–8 (2012).
Norman, K., Stobäus, N., Gonzalez, M. C., Schulzke, J. D. & Pirlich, M. Hand grip strength: outcome predictor and marker of nutritional status. Clin Nutr. 30, 135–142 (2011).
Misu, S. et al. Association between gait abnormality and malnutrition in a community-dwelling elderly population. Geriatr Gerontol Int. 17(8), 1155–1160 (2016).
Amaral T. F. et al. Nutritional Strategies Facing an Older Demographic: The Nutrition UP 65 Study Protocol. JMIR Res Protoc. 14;5(3):e184, https://doi.org/10.2196/resprot.6037 (2016).
Guerreiro, M. Testes de rastreio de defeito cognitivo e demência: uma perspectiva prática. Rev Port Clin Geral. 26, 46–53 (2010).
World Health Organization (WHO). Body mass index classification. Copyright WHO (2006). http://apps.who.int/bmi/index.jsp?introPage=intro_3.html [accessed 2017-05-22].
Nestle Nutrition Institute. MNA-Mini Nutritional Assessment. http://www.mna-elderly.com/forms/mini/mna_mini_portuguese.pdf [accessed 2017-05-22].
Kaiser, M. J. et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging. 13(9), 782–8 (2009).
Wang, C. Y., Chen, T. R., Lin, Y. H., Liu, M. H. & Chen, Y. C. Gait speed measure: the effect of different measuring distances and the inclusion and exclusion of acceleration and deceleration. Percept Mot Skills. 114(2), 469–78 (2012).
Porta M. A Dictionary of Epidemiology, 6th edition Publisher: Oxford University Press Editor (2014).
Verghese, J. et al. Epidemiology of gait disorders in community-residing older adults. J Am Geriatr Soc. 54(2), 255–61 (2006).
Andersen, J. L. Muscle fibre type adaptation in the elderly human muscle. Scand J Med Sci Sports. 13(1), 40–7 (2003).
Wojzischke, J., Diekmann, R. & Bauer, J. M. Obesity in old age and its importance for functionality and frailty. Z Gerontol Geriatr. 49(7), 573–80 (2016).
Bindawas, S. M. Relationship between frequent knee pain o, and gait speed in older adults: data from the Osteoarthritis Initiative. Clin Interv Aging. 25(11), 237–44 (2016).
Visser, M. et al. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: the Health ABC Study. J Gerontol A Biol Sci Med Sci. 57(5), M326–32 (2002).
Addison, O. et al. Intramuscular fat and inflammation differ in older adults: the impact of frailty and inactivity. J Nutr Health Aging. 18(5), 532–8 (2014).
Osofundiya, O., Benden, M. E., Dowdy, D. & Mehta, R. K. Obesity-specific neural cost of maintaining gait performance under complex conditions in community-dwelling older adults. Clin Biomech (Bristol, Avon). 35, 42–8 (2016).
McDermott, M. M. et al. Community walking speed, sedentary or lying down time, and mortality in peripheral artery disease. Vasc Med. 21(2), 120–9 (2016).
Naseer, M., Forssell, H. & Fagerström, C. Malnutrition, functional ability and mortality among older people aged word ≥60 years: a 7-year longitudinal study. Eur J Clin Nutr. 70(3), 399–404 (2016).
Bollwein, J. et al. Nutritional status according to the mini nutritional assessment (MNA®) and frailty in community dwelling older persons: a close relationship. J Nutr Health Aging. 17(4), 351–6 (2013).
Kaburagi, T. et al. Nutritional status is strongly correlated with grip strength and depression in community-living elderly Japanese. Public Health Nutr. 14(11), 1893 (2011).
Batsis, J. A., Mackenzie, T. A., Barre, L. K., Lopez-Jimenez, F. & Bartels, S. J. Sarcopenia, sarcopenic obesity and mortality in older adults: results from the National Health and Nutrition Examination Survey III. Eur J Clin Nutr. 68(9), 1001–7 (2014).
Visser, M. et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J Gerontol A Biol Sci Med Sci. 60(3), 324–33 (2005).
Scott, D. et al. Sarcopenic obesity and dynapenicobesity: 5-year associations with falls risk in middle-aged and older adults. Obesity (Silver Spring). 22(6), 1568–74 (2014).
Prado, C. M., Wells, J. C., Smith, S. R., Stephan, B. C. & Siervo, M. Sarcopenic obesity: A Critical appraisal of the current evidence. Clin Nutr. 31(5), 583–601 (2012).
Mendes, J., Azevedo, A. & Amaral, T. F. Handgrip strength at admission and time to discharge in medical and surgical inpatients. JPEN J Parenter Enteral Nutr. 38(4), 481–8 (2014).
Guerra, R. S., Fonseca, I., Pichel, F., Restivo, M. T. & Amaral, T. F. Usefulness of six diagnostic and screening measures for undernutrition in predicting length of hospital stay: a comparative analysis. J Acad Nutr Diet. 115(6), 927–38 (2015).
Beavers, K. M. et al. Associations between body composition and gait-speed decline: results from the Health, Aging, and Body Composition study. Am J Clin Nutr. 97(3), 552–60 (2013).
Cederholm, T. et al. Diagnostic criteria for malnutrition - An ESPEN Consensus Statement. Clin Nutr. 34(3), 335–40 (2015).
López-Ortega, M. & Arroyo, P. Anthropometric characteristics and body composition in Mexican older adults: age and sex differences. Br J Nutr. 115(3), 490–9 (2016).
Lim, Y. P., Lin, Y. C. & Pandy, M. G. Muscle function during gait is invariant to age when walking speed is controlled. Gait Posture. 38(2), 253–9 (2013).
Workgroup of the American Association of Hip and Knee Surgeons Evidence Based Committee. Obesity and total joint arthroplasty: a literature based review. J Arthroplasty. 28:714–21 (2013).
Inoue, W. et al. Are there different factors affecting walking speed and gait cycle variability between men and women in community-dwelling older adults? Aging Clin Exp Res. 29(2), 215–21 (2017).
Fletcher, R. H. & Fletcher, S. W. Clinical epidemiology: The essentials. 4th edition Philadelphia: Lippincott Williams & Wilkins (2005).
Acknowledgements
The present project was 85% funded by the Public Health Initiatives Programme (PT06), financed by European Economic Area (EEA) Grants Financial Mechanism 2009 2014. The EEA Grants are managed by “Administração Central do Sistema de Saúde” through the “Programa Iniciativas em Saúde Pública”. Mendes J is receiving a scholarship from the “Fundação para a Ciência e a Tecnologia”, Portuguese Government Organization (Project SFRH/BD/115665/2016).
Author information
Authors and Affiliations
Contributions
J.M. and T.F.A. designed the research. J.M. and T.F.A. analyzed data. J.M., N.B., A.S., P.P., P.M., C.A., R.N. and T.F.A. contributed to manuscript preparation and approved the final version of the manuscript submitted for publication.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mendes, J., Borges, N., Santos, A. et al. Nutritional status and gait speed in a nationwide population-based sample of older adults. Sci Rep 8, 4227 (2018). https://doi.org/10.1038/s41598-018-22584-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-22584-3
This article is cited by
-
The mediating effect of nutrition on oral frailty and fall risk in community-dwelling elderly people
BMC Geriatrics (2024)
-
Factors associated with 10-m walking speed in outpatients undergoing hemodialysis: a multicenter cross-sectional study
Renal Replacement Therapy (2023)
-
The evaluation of the association between preoperative sarcopenia and postoperative pneumonia and factors for preoperative sarcopenia in patients undergoing thoracoscopic-laparoscopic esophagectomy for esophageal cancer
Surgery Today (2023)
-
The effect of age on the association between daily gait speed and abdominal obesity in Japanese adults
Scientific Reports (2021)
-
Nutritional Assessment in Older Adults: MNA® 25 years of a Screening Tool & a Reference Standard for Care and Research; What Next?
The Journal of nutrition, health and aging (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
