
Abstract
Fetal heart rate (FHR) monitoring is essential for fetal management during pregnancy and delivery but results in many false-positive diagnoses. Air pollution affects the uterine environment; thus, air pollution may change FHR reactivity. This study assessed the association between exposure to air pollution during pregnancy and FHR monitoring abnormalities using 2005–2010 data from the Japan Perinatal Registry Network database. Participants were 23,782 singleton pregnant women with FHR monitoring, without acidemia or fetal asphyxia. We assessed exposure to air pollutants, including particulate matter (PM), ozone, nitrogen dioxide (NO2), and sulfur dioxide (SO2). In a multi-trimester model, first-trimester PM exposure was associated with false positives in FHR monitoring (odds ratio [OR] per interquartile range (10.7 μg/m3) increase = 1.20; 95% CI: 1.05–1.37), but not second-trimester exposure (OR = 1.05; 95% CI: 0.91–1.21) and third-trimester exposure (OR = 1.06; 95% CI: 0.96-1.17). The association with first-trimester PM exposure persisted after adjustment for exposure to ozone, NO2, and SO2; however, ozone, NO2, and SO2 exposure was not associated with false positives in FHR monitoring. First-trimester PM exposure may alter fetal cardiac response and lead to false positives in FHR monitoring.
Similar content being viewed by others


Introduction
Research on fetal heart rate (FHR) monitoring has been conducted to determine the clinical significance of different morphological categories of FHR tracing. It was thought that if hypoxia and other aspects of fetal status could be understood and medical interventions administered early, the incidence of fetal death during delivery, neonatal asphyxia, and even cerebral palsy could be reduced1. However, subsequent studies reported no change in the incidence of cerebral palsy, and while the number of perinatal deaths has declined, the number of cesarean sections (C-sections) has increased2. Abnormalities in FHR monitoring can appear as late deceleration (LD), severe variable deceleration (SVD), loss of variability (LV), or bradycardia. When these occur alone or in combination, non-reassuring fetal status is diagnosed, and immediate delivery of the fetus is recommended3. However, the increase in the C-section rate has been accompanied by an increased awareness of the harm this procedure can cause. Moreover, fetuses that exhibit FHR abnormalities do not necessarily present with acidosis and do not always require immediate delivery3,4,5. In other words, there are many cases of false positives in FHR monitoring which do not actually present with acidosis. Since FHR monitoring is an essential component of fetal management, pursuing the causes of false positives in FHR monitoring is extremely important. However, these causes are not clearly understood6,7,8.
Recently, air pollution has been linked to fetal growth restriction, low birth weight9,10,11, and preterm birth12. Research in animal models has confirmed that air pollution can damage the uterine environment and affect fetal growth and development13,14. Fetuses adapt to changes in the uterine environment (e.g., undernutrition, maternal inflammation, and stress), and the results of these adaptations may manifest in adulthood as heart disease or other health problems15. Air pollution can cause uterine inflammation16, which often leads to hypoxic states17. In animal experiments, hypoxic stimulation causes changes in heart rate responses. Subsequently, the same amount of hypoxic stimulation caused greater declines in the heart rate18,19.
Therefore, we hypothesized that exposure to inflammation caused by air pollution changes the fetal heart rate responses and causes false positives in FHR monitoring. In this study, we considered cases that presented with FHR monitoring abnormalities, without acidemia or fetal asphyxia, with umbilical arterial blood pH ≥ 7.2, and Apgar score ≥7, as false positives20,21, and examined the association with exposure to air pollution during pregnancy.
Methods
Study population
This study was approved by the Institutional Review Board of Kyushu University (No. 28-153), Japan, and the Japan National Institute for Environmental Studies (No. 1-2016-005) and performed according to the Declaration of Helsinki. Analyses were performed on de-identified data from the Japan Perinatal Registry Network database, which is maintained by the Japan Society of Obstetrics and Gynecology. This database includes data on all live births and stillbirths after 22 weeks of gestation at participating hospitals (primarily university hospitals and local general hospitals). Details of this database have been published previously22.
In this study, we used perinatal data from 28 hospitals across eight prefectures (Fukuoka, Saga, Nagasaki, Kumamoto, Oita, Miyazaki, Kagoshima, and Okinawa) in the western part of Japan (Kyushu-Okinawa District), from 2005 to 2010. The data included maternal age, height, weight, parity, gestational age as determined from ultrasound findings in early pregnancy, smoking status and alcohol consumption during pregnancy, medical history, diagnoses of obstetric complications, birth weight, and infant sex.
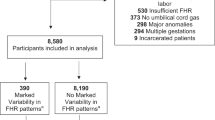
During the study period, 47,835 singleton deliveries were registered. Among these, 6,906 deliveries for which the prefecture of the mother’s residence was different from the location of the birth hospital were excluded to avoid exposure misclassification due to the Japanese satogaeri custom (some mothers go back to their parental homes, and deliver at a hospital near their parents’ homes). In addition, the following deliveries were excluded: 2,832 deliveries with gestational age <32 weeks (unsuitable for FHR assessment23,24); 9,752 deliveries with missing information on umbilical cord blood pH (n = 7,282) or umbilical blood pH < 7.2 (acidemia)20,25 (n = 2,470); 1,385 deliveries with Apgar scores <7 at 1 minute or 5 minutes after birth (to restrict the study sample to newborns in good health21); 1,726 deliveries to mothers with intrauterine infection, oligohydramnios, or placental abruption (which are causes of FHR monitoring abnormalities26,27; one delivery with fetal death (stillbirth); 1,346 deliveries with conception date ≥22 weeks before the study period began and those with conception dates ≤42 weeks before the study period ended to prevent fixed cohort bias28, and 105 deliveries with missing data on maternal age (n = 2) or exposure to pollutants (n = 103). After applying these exclusions, 23,782 singleton deliveries at gestational age ≥32 weeks were included in the analysis.
Environmental data
Concentrations of air pollutants (particulate matter [PM], nitrogen dioxide [NO2], sulfur dioxide [SO2], and ozone measured as photochemical oxidants), measured at ambient air pollution monitoring stations and whose measurements were regarded to be representative of their respective communities, were collected from the Japan National Institute for Environmental Studies’ atmospheric environment database. As an indicator of PM, we used suspended PM, defined under the Japan Air Quality Standards as airborne particles with a 100% cut-off level of 10-μm aerodynamic diameter29. Because routine measurement of PM2.5 (particles with a 50% cut-off level of 2.5 μm in aerodynamic diameter) at monitoring stations did not start in Japan until after 2010, we could not assign PM2.5 concentrations to most of the study participants.
The Japan Perinatal Registry Network database includes de-identified data; thus, we did not have the specific residential addresses or postal codes of study participants. Based on the assumption that the pregnant women reside near their delivery hospitals, which we previously validated30, we assigned pollutant concentrations measured at the closest monitoring station to each participant’s delivery hospital. Each monitoring station and the corresponding hospital were located within the same administrative area, and the median linear distance between them was 1.1 miles (1.8 km), except for one hospital in Okinawa prefecture (8.5 miles [13.6 km]). Specific locations of 24 monitoring stations and 28 hospitals have been described previously31.
We used daily mean concentrations of air pollutants (maximum 8-h mean concentrations for ozone) and calculated the average concentrations during the first trimester (0–13 weeks of gestation), second trimester (14–27 weeks of gestation), and third trimester (28-31 weeks of gestation as we included women who delivered in the preterm period).
FHR monitoring abnormality
FHR monitoring was performed at the time of hospitalization after the onset of labor or for complications such as the rupture of membranes. FHR monitoring was also performed during delivery.
The Japan Perinatal Registry Network database contains data on the following eight intrapartum FHR monitoring parameters: early deceleration (ED), LD, mild variable deceleration (MVD), SVD, LV, bradycardia, tachycardia, and others. In the present study, FHR monitoring abnormalities was defined as LD, SVD, LV, or bradycardia alone or a combination of them; ED is considered to be a normal reaction, and MVD and tachycardia are not attributable to acidosis alone32. However, if ED, MVD, tachycardia or others were recorded in addition to LD, SVD, LV, or bradycardia, the participant was still classified under the FHR monitoring abnormality category. Concerns could also be raised regarding the reliability and validity of diagnoses based on FHR monitoring. However, as assessments were performed by obstetricians at university hospitals and regional general hospitals, we expected inter-rater variability to be low33.
Statistical analysis
To measure the association between exposure to pollutants during the first trimester and FHR monitoring abnormalities, odds ratios (ORs) and 95% confidence intervals (CIs) per 10-unit increase in pollutant concentrations were estimated using multilevel logistic regression with hospital-level random effects (Supplementary figure). In this study, we assumed a linear association, since there was no evidence of a non-linear one. Regression models were adjusted for exposure to each pollutant during the first, second and third trimesters; maternal age at delivery (<25, 25–29, 30–34, ≥35 years); birth year (2005, 2006, 2007, 2008, 2009, 2010); season of conception (spring, summer, autumn, winter); smoking during pregnancy (no, yes, missing); alcohol drinking during pregnancy (no, yes, missing); parity (0, ≥1); mode of delivery (vaginal, scheduled cesarean, emergency cesarean); gestational age at birth (32,33,34,35,36, ≥37 weeks of gestation); small for gestational age (birth weight <10 percentile for gestational age) (yes, no) due to abnormal FHR based on prematurity23,24; and premature rupture of membranes (yes, no) and presence of congenital abnormalities (yes, no) as these two conditions are associated with FHR monitoring abnormalities34,35,36,37. Then, we constructed a multi-trimester model including exposure during all three trimesters. In addition, we performed several sensitivity analyses in order to avoid the possibility of residual confounding. We also constructed a multi-pollutant model including exposure to all pollutants. Statistical analyses were conducted using STATA 13 for Windows (Stata Corporation, College Station, TX, USA).
Results
The characteristics of the 23,782 deliveries included in the study are shown in Table 1. The mean maternal age at delivery was 31.0 years (standard deviation [SD] = 5.5), and 9.8% of fetuses exhibited FHR monitoring abnormalities. During the first trimester, mean concentrations of the pollutants were 27.1 μg/m3 (SD =8.0) for PM, 41.3 ppb (9.7) for ozone, 11.5 ppb (6.2) for NO2, and 3.1 ppb (1.4) for SO2 (Table 2). Pearson’s correlation coefficients for exposure to PM and NO2 were moderate (0.52 during the first trimester, 0.54 during the second trimester, and 0.47 during the third trimester).
Associations between exposure to pollutants and false positives in FHR monitoring are shown in Table 3. In a multi-trimester model, first-trimester PM exposure was positively associated with false positives in FHR monitoring (OR per interquartile range (10.7 μg/m3) increase in PM concentrations = 1.20; 95% CI: 1.05–1.37). This association was not significantly changed after exposure to ozone, NO2, or SO2 during the first trimester (OR = 1.23, 95% CI = 1.05–1.44) (Table 4). In contrast, no significant association was observed between exposure in other trimesters and false positives in FHR monitoring (OR per interquartile range (10.4 μg/m3) = 1.05, 95% CI: 0.91–1.21 for the second trimester; and OR per interquartile range (12.4 μg/m3) = 1.06, 95% CI: 0.96-1.17 for the third trimester). The results for first-trimester PM exposure were robust in all the sensitivity analyses as follows: excluding participants in the Okinawa area due to the distance between one hospital and its respective monitoring station; restricted to nulliparous women; restricted to non-smokers and non-drinkers; excluding women who delivered in the preterm period (32,33,34,35,36 weeks of gestation) or who delivered a small for gestational age infant; excluding women with premature rupture of membranes or those who delivered an infant with congenital anomalies; and excluding women with scheduled cesarean deliveries to exclude births with less delivery-related stress to the fetus. Exposure to ozone, NO2, or SO2 during the first, second, and third trimesters were not associated with false positives in FHR monitoring.
Discussion
In this study, we observed a positive association between exposure to PM in the first trimester of pregnancy and false positives in FHR monitoring. No associations were observed for ozone, NO2, or SO2. Moreover, no association was observed between PM exposure in the second- and third-trimester and false positives in FHR monitoring. To the best of our knowledge, this is the first study to report an association between first-trimester PM exposure and false positives in FHR monitoring.
False positives in FHR monitoring have been linked to congenital anomalies, infections, and maternal smoking35,36,37,38,39. FHR monitoring abnormalities have been reported at high frequencies in these cases, even when the fetus was otherwise well. Although FHR monitoring abnormalities can lead to emergency C-sections in cases of cardiac malformation, acidosis is often not observed in such cases. Moreover, bradycardia, LD, and other FHR monitoring abnormalities are frequently observed in cases of cytomegalovirus infection38. Additionally, maternal smoking can alter the regulation of heart rate and increase infant reactivity soon after birth39,40. Even in the absence of complications, maternal smoking has been linked to an elevated C-section rate due to the diagnosis of non-reassuring fetal status39. While the study reporting this association did not measure umbilical arterial blood pH, no differences in Apgar scores were reported between the smoking and non-smoking groups39. Although exposure to maternal smoking can occur throughout gestation, infections have a greater influence on the fetus early in pregnancy. FHR changes are reciprocally formed and regulated by the autonomic nervous system, the cardiovascular center in the brainstem, and the cardiac conduction system41. The first trimester is a critical period for the formation of these control mechanisms. In the present study, the association between false positives in FHR monitoring and exposure to air pollution was observed for the first-trimester but not second or third-trimester exposure. Nachman et al.16 reported a direct association between PM2.5 exposure and intrauterine inflammation using histopathological analyses of human placenta samples. On the one hand, inflammatory tissue often leads to hypoxic states17. In animal experiments, hypoxic stimulation causes changes in heart rate responses. Subsequently, the same amount of hypoxic stimulation caused greater declines in the heart rate18,19. Based on these findings, about the potential mechanism, we thought that uterine inflammation and hypoxic stimulation caused by air pollution in the first trimester might affect the cardiovascular center of the brainstem and the heart rate reactivity of the fetus. However, further research regarding the underlying mechanism is needed.
One limitation of this study is the locations at which air pollution levels were measured. Data were collected from the ambient air pollution monitoring station closest to the hospital where the study participant gave birth and thus provided imperfect measurements of women’s individual exposures. However, this exposure misclassification was likely to be non-differential; therefore, we would underestimate the effect of PM exposure on abnormal FHR. And there are also a limitation of this study. Because routine measurement of PM2.5 at monitoring stations did not start in Japan until after 2010, we could not analyze PM 2.5 separately in this study. In addition, since there were unmeasured factors, such as socioeconomic status, the possibility of residual confounding could not be excluded. Finally, the generalization of our results requires careful attention because of the exclusion of women thought to have participated in the satogaeri custom.
In 33.5% (777) of the cases that showed false positives in FHR monitoring, emergency C-sections were performed. Hence, preventing air pollution exposure in the first trimester of pregnancy could help reduce C-sections performed because of false positives in FHR monitoring. This is highly significant as it could help conserve medical resources. We recommend that future epidemiological studies be performed to verify and build on these findings.
Conclusions
We observed a positive association between exposure to PM in the first trimester and false positives in FHR monitoring. No associations were observed for ozone, NO2, or SO2. Moreover, no association was observed between PM exposure in the second- and third-trimester and false positives in FHR monitoring. Thus, first-trimester PM exposure may alter the FHR response and lead to false positives in FHR monitoring.
References
Quilligan, E. J. & Paul, R. H. Fetal monitoring: is it worth it? Obstet Gynecol. 45, 96–100 (1975).
Nelson, K. B., Dambrosia, J. M., Ting, T. Y. & Grether, J. K. Uncertain value of electronic fetal monitoring in predicting cerebral palsy. N Engl J Med 334, 613–618 (1996).
Spencer, J. A. Clinical overview of cardiotocography. Br J Obstet Gynaecol 100(Suppl. 9), 4–7 (1993).
Devoe, L. Electronic fetal monitoring: does it really lead to better outcomes? Am J Obstet Gynecol 204, 455–456 (2011).
Neilson, D. R., Freeman, R. K. & Mangan, S. Signal ambiguity resulting in unexpected outcome with external fetal heart rate monitoring. Am J Obstet Gynecol 198, 717–724 (2008).
Alfirevic, Z., Devane, D. & Gyte, G. M. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst Rev 5, CD006066 (2013).
Macones, G. A., Hankins, G. D., Spong, C. Y., Hauth, J. & Moore, T. The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Obstet Gynecol. 112, 661–666 (2008).
Pinas, A. & Chandraharan, E. Continuous cardiotocography during labour: Analysis, classification and management. Best Pract Res Clin Obstet Gynaecol 30, 33–47 (2016).
Bobak, M. Outdoor air pollution, low birth weight, and prematurity. Environ Health Perspect 108, 173–176 (2000).
Dejmek, J., Selevan, S. G., Benes, I., Solansky, I. & Sram, R. J. Fetal growth and maternal exposure to particulate matter during pregnancy. Environ Health Perspect 107, 475–480 (1999).
Lee, B. E. et al. Exposure to air pollution during different gestational phases contributes to risks of low birth weight. Hum Reprod. 18, 638–643 (2003).
Ritz, B., Yu, F., Chapa, G. & Fruin, S. Effect of air pollution on preterm birth among children born in Southern California between 1989 and 1993. Epidemiology. 11, 502–511 (2000).
Tsukue, N., Tsubone, H. & Suzuki, A. K. Diesel exhaust affects the abnormal delivery in pregnant mice and the growth of their young. Inhal Toxicol. 14, 635–651 (2002).
Veras, M. M. et al. Particulate urban air pollution affects the functional morphology of mouse placenta. Biol Reprod 79, 578–584 (2008).
Barker, D. J. Adult consequences of fetal growth restriction. Clin Obstet Gynecol 49, 270–283 (2006).
Nachman, R. M. et al. Intrauterine Inflammation and Maternal Exposure to Ambient PM2.5 during Preconception and Specific Periods of Pregnancy: The Boston Birth Cohort. Environ Health Perspect 124, 1608–1615 (2016).
Eltzschig, H. K. & Carmeliet, P. Hypoxia and inflammation. N Engl J Med 364, 656–665 (2011).
Pulgar, V. M. et al. Mild chronic hypoxemia modifies expression of brain stem angiotensin peptide receptors and reflex responses in fetal sheep. Am J Physiol Regul Integr Comp Physiol 297, R446–452 (2009).
Pulgar, V. M., Zhang, J., Massmann, G. A. & Figueroa, J. P. Mild chronic hypoxia modifies the fetal sheep neural and cardiovascular responses to repeated umbilical cord occlusion. Brain Res. 1176, 18–26 (2007).
Riley, R. J. & Johnson, J. W. Collecting and analyzing cord blood gases. Clin Obstet Gynecol 36, 13–23 (1993).
Casey, B. M., McIntire, D. D. & Leveno, K. J. The continuing value of the Apgar score for the assessment of newborn infants. N Engl J Med 344, 467–471 (2001).
Hayashi, K., Matsuda, Y., Kawamichi, Y., Shiozaki, A. & Saito, S. Smoking during pregnancy increases risks of various obstetric complications: a case-cohort study of the Japan Perinatal Registry Network database. J Epidemiol. 21, 61–66 (2011).
Pillai, M. & James, D. The development of fetal heart rate patterns during normal pregnancy. Obstet Gynecol. 76, 812–816 (1990).
Murray, H. Antenatal Foetal Heart Monitoring. Best Pract Res Clin Obstet Gynaecol 38, 2–11 (2017).
Omo-Aghoja, L. Maternal and fetal Acid-base chemistry: a major determinant of perinatal outcome. Ann Med Health Sci Res 4, 8–17 (2014).
Freeman, R. K., Garite, T. J., Nageotte, M. P. & Miller, L. A. Fetal Heart Rate Monitoring. 4th ed. (Lippincott Williams & Wilkins, 2012).
Hasegawa, J. et al. Intrapartum fetal heart rate pattern in oligohydramnios. Fetal Diagn Ther 24, 267–270 (2008).
Strand, L. B., Barnett, A. G. & Tong, S. Methodological challenges when estimating the effects of season and seasonal exposures on birth outcomes. BMC Med Res Methodol 11, 49 (2011).
Japan Ministry of the Environment. Environmental quality standards in Japan – air quality. https://www.env.go.jp/en/air/aq/aq.html (2016).
Michikawa, T., Morokuma, S., Nitta, H., Kato, K. & Yamazaki, S. Comparison between air pollution concentrations measured at the nearest monitoring station to the delivery hospital and those measured at stations nearest the residential postal code regions of pregnant women in Fukuoka. Environ Health Prev Med 22, 55 (2017).
Michikawa, T. et al. A register-based study of the association between air pollutants and hypertensive disorders in pregnancy among the Japanese population. Environ Res. 142, 644–650 (2015).
Murphy, A. A., Halamek, L. P., Lyell, D. J. & Druzin, M. L. Training and competency assessment in electronic fetal monitoring: a national survey. Obstet Gynecol. 101, 1243–1248 (2003).
Hayashi, M., Nakai, A., Sekiguchi, A. & Takeshita, T. Fetal heart rate classification proposed by the perinatology committee of the Japan Society of Obstetrics and Gynecology: reproducibility and clinical usefulness. J Nippon Med Sch 79, 60–68 (2012).
Harding, J. A. et al. Correlation of amniotic fluid index and nonstress test in patients with preterm premature rupture of membranes. Am J Obstet Gynecol 165, 1088–1094 (1991).
Garite, T. J., Linzey, E. M., Freeman, R. K. & Dorchester, W. Fetal heart rate patterns and fetal distress in fetuses with congenital anomalies. Obstet Gynecol. 53, 716–720 (1979).
Powell Phillips, W. D. & Towell, M. E. Abnormal fetal heart rate associated with congenital abnormalities. Br J Obstet Gynaecol 87, 270–274 (1980).
Ueda, K. et al. Intrapartum fetal heart rate monitoring in cases of congenital heart disease. Am J Obstet Gynecol. 201, 64.e1–64.e6 (2009).
Kaneko, M., Sameshima, H., Ikeda, T., Ikenoue, T. & Minematsu, T. Intrapartum fetal heart rate monitoring in cases of cytomegalovirus infection. Am J Obstet Gynecol 191, 1257–1262 (2004).
Lurie, S., Ribenzaft, S., Boaz, M., Golan, A. & Sadan, O. The effect of cigarette smoking during pregnancy on mode of delivery in uncomplicated term singleton pregnancies. J Matern Fetal Neonatal Med 27, 812–815 (2014).
Cohen, G., Vella, S., Jeffery, H., Lagercrantz, H. & Katz-Salamon, M. Cardiovascular stress hyperreactivity in babies of smokers and in babies born preterm. Circulation. 118, 1848–1853 (2008).
Christoffels, V. M. & Moorman, A. F. Development of the cardiac conduction system: why are some regions of the heart more arrhythmogenic than others? Circ Arrhythm Electrophysiol 2, 195–207 (2009).
Acknowledgements
We thank the many doctors who cooperated with the creation of the Japan Perinatal Registry Network database. This study was supported by a research grant from the Japan National Institute for Environmental Studies and in part by MEXT KAKENHI (grant no.: 24119004) and Japan Society for the Promotion of Science KAKENHI (grant no.: 16H01880, 16K13072). The sponsors had no involvement in the study design, collection, analysis, and interpretation of data, the writing of the report, or the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
Study concept and design: S.M. Statistical analyses: T.M. Drafting of the manuscript: S.M. and T.M. Critical revision of the manuscript for important intellectual content: all authors. Technical or material support: Y.S. Study supervision: K.K. and H.N. Manuscript review: all authors.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Morokuma, S., Michikawa, T., Yamazaki, S. et al. Association between exposure to air pollution during pregnancy and false positives in fetal heart rate monitoring. Sci Rep 7, 12421 (2017). https://doi.org/10.1038/s41598-017-12663-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-12663-2
This article is cited by
-
Associations between air pollution exposure and birth defects: a time series analysis
Environmental Geochemistry and Health (2021)
-
Non-reassuring foetal status and neonatal irritability in the Japan Environment and Children’s Study: A cohort study
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
