
Abstract
Carboxylesterase 1 (CES1) hydrolyzes the prodrug clopidogrel to an inactive carboxylic acid metabolite. The effects of CES1 S75N (rs2307240,C>T) on clopidogrel response among 851 acute coronary syndrome patients who came from the north, central and south of China were studied. The occurrence ratios of each endpoint in the CC group were significantly higher than in the CT + TT group for cerebrovascular events (14% vs 4.8%, p < 0.001, OR = 0.31), acute myocardial infarction (15.1% vs 6.1%, p < 0.001, OR = 0.37) and unstable angina (62.8% vs 37.7%, p < 0.001, OR = 0.36). The results showed that there was a significant association between CES1 S75N (rs2307240) and the outcome of clopidogrel therapy. Moreover, the frequency of the T allele of rs2307240 in acute coronary syndrome patients (MAF = 0.22) was more than four times higher than that in the general public (MAF = 0.05).
Similar content being viewed by others
Introduction
Dual antiplatelet therapy (DAPT), a combination treatment of clopidogrel and aspirin, is the standard therapy for preventing recurrent cardiovascular events in patients who have coronary heart disease (CHD), who undergo a percutaneous coronary intervention (PCI) and who have acute coronary syndrome (ACS)1. It has been reported that the efficacy of clopidogrel treatment varies from person to person; 5–40% of patients do not receive therapeutic benefit and instead have an increased risk of adverse outcomes2. Some patients experience acute myocardial infarction, unstable angina, stent thrombosis (ST) and/or cerebrovascular events. Clinical, genetic, and cellular factors might contribute to the variability in clopidogrel response, and genetic factors have been estimated to explain approximately 70% of the inter-individual variance in clopidogrel pharmacokinetics and pharmacodynamics acute myocardial infarctions3.
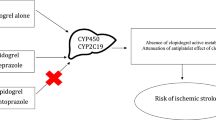
Clopidogrel is a thienopyridine prodrug that is converted to a pharmacologically active thiol metabolite through the inactive intermediate 2-oxo-clopidogrel. This reaction is catalyzed by cytochrome P450 (CYP) enzymes, including CYP2C19, CYP3A, CYP2B6, CYP1A2, and CYP2C9. However, only 15% of a clopidogrel dose is available from this pathway. The 5-thiol clopidogrel active metabolite inhibits ADP-induced platelet activation and aggregation by irreversibly binding to the P2Y12 receptor on the surface of platelets4, 5. Approximately 85% of the parent clopidogrel is rapidly hydrolyzed to the inactive metabolite, clopidogrel carboxylic acid, which is further metabolized by glucuronidation6. This hydrolysis is catalyzed by hepatic carboxylesterase 1 (CES1)7, which is primarily expressed in the liver8. In addition, CES1 can hydrolyze 2-oxo-clopidogrel and 5-thiol clopidogrel active metabolites to 2-oxo-clopidogrel carboxylate9, an inactive metabolite, and the 5-thiol carboxylic acid metabolite. Ultimately, only a small proportion of clopidogrel is converted to the active metabolite10.
In humans, CES1 is a widely expressed serine esterase, catalyzing the hydrolysis of multiple amide and ester-containing endogenous compounds, toxins, and medications to their respective free acids11. CES1 is involved in most hydrolytic activities in the human liver. Significant inter-individual variability of CES1 expression and/or activity has been consistently reported in the bio-medical literature. This variability is likely the result of both genetic and environmental factors12, 13. The genetic variants involved in the pharmacokinetics of clopidogrel have been investigated extensively; A previous study documented that the CES1 single nucleotide polymorphisms (SNPs) G143E14, 15 (rs71647871) and D260fs16 (rs71647872) exhibited markedly decreased enzymatic activity in the hydrolysis of the CES1 substrate methylphenidate and CES1A2 −816C was associated with attenuated platelet reactivity to clopidogrel17. According to a previous report, the metabolic activity of CES1A1 can differ up to 31-fold between individuals18. Therefore, it has been hypothesized that CES1 genetic variants could serve as biomarkers to predict clopidogrel response and individualize clopidogrel dosing regimens in clinical practice19.
In this study, we investigated whether CES1 S75N could significantly influence the efficacy of clopidogrel and alter the patients’ response.
Results
Genotyping and frequencies of CES1 S75N in Chinese acute coronary syndrome patients
Patients with acute coronary syndrome who were taking a standard loading or maintenance clopidogrel regime were recruited. The characteristics of the study participants can be summarized as follows. Generally, the patients were older (mean age = 63.25 ± 11.79 years) and had a high prevalence of hypertension (69.1%), hyperlipemia (49.6%), planting stents (81.9%), diabetes (31.4%) and smokers (47.8%). Additionally, many patients were taking proton pump inhibitors (PPI) (25.2%) and calcium channel blockers (CCB) (46.8%). Records revealed that 84 (9.9%) participants experienced cerebrovascular events, 94 (11%) participants underwent an acute myocardial infarction and 438 (51.5%) participants suffered unstable angina.
The S75N SNP genotype distributions for CC, CT and TT were 55.4% (n = 471), 43.7% (n = 372) and 0.2% (n = 2), respectively. Additionally, 0.7% (n = 6) patients failed genotyping. The allelic frequencies of the C and T alleles were 77.8% and 22.2%, respectively. The incidence of the C allele (11.4%, 12.6% and 55.8% in cerebrovascular events, acute myocardial infarction and unstable angina, respectively) was significantly higher than that of the T allele (4.8%, 6.1% and 37.5% in cerebrovascular events, acute myocardial infarction and unstable angina, respectively) (p < 0.001) among patients with endpoints. Additionally, the risk allele frequency of patients with endpoints was approximately half of that of patients without endpoints, as shown in Table 1. The CT and TT genotypes (CT + TT group) were combined in the subsequent analysis to elucidate the effect of the T allele (the dominant model for the T allele).
Clinical characteristics and outcomes in the S75N genotype groups
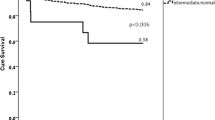
The clinical factors, such as hypertension (p = 0.003), hyperlipemia (p < 0.001), stent (p = 0.003), CCB (p = 0.026) and PPI (p < 0.001), as well as the clinical outcomes of cerebrovascular event, acute myocardial infarction and unstable angina (p < 0.001) were significantly different between the CC and CT + TT genotype groups (Table 2). Figure 1 illustrates the occurrence ratios of three endpoints among the CES1 S75N genotype groups. The occurrence ratios for each endpoint in the CC group were relatively higher for cerebrovascular events, acute myocardial infarction and unstable angina than that in the CT + TT group (14% vs 4.8%, 15.1% vs 6.1% and 62.8% vs 37.7, respectively). A logistic analysis with a CC group as a reference (odds ratio = 1.0) yielded an odds ratio of 0.31 (95% CI: 0.18 to 0.53), 0.37 (95% CI: 0.23 to 0.60) and 0.36 (95% CI: 0.27 to 0.47) for the likelihood of CT + TT genotype patients who had experienced cerebrovascular events, acute myocardial infarction and unstable angina, respectively.

Occurrence ratios in the CES1 S75N genotype group. Fourteen percent of CC group patients and 4.8% of CT + TT group patients had cerebrovascular events after clopidogrel treatment (p < 0.001). 15.1% vs 6.1% of patients suffered acute myocardial infarction and 62.8% vs 37.7% suffered unstable angina after treatment, respectively (p < 0.001). The total number of patients in the CC and CT + TT groups was 471 and 374, respectively.
Association between genetic polymorphisms and three outcomes among acute coronary syndrome patients
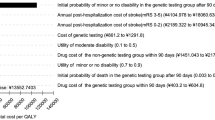
To further explore the relationship between CES1 S75N and the outcome of clopidogrel therapy, patients were stratified according to nine factors including age, gender, smoking state, stent, hypertension, hyperlipemia, diabetes, BBC and PPI, as shown in Fig. 2. In additive and dominant models, CES1 S75N correlates with cerebrovascular events in ACS patients with any of the following qualities: <75 years old, male, no smoking, stent, hypertension, hyperlipemia, no diabetes, no BBC and no PPI. In additive and dominant models, CES1 S75N also correlates with acute myocardial infarction in ACS patients with any of the following qualities: <75 years old, male, stent, hypertension, hyperlipemia, and no PPI. Smoking state, diabetes and BBC does not affect the relationship between S75N and acute myocardial infarction. Additionally, S75N also correlated to unstable angina in all ACS patients except those who took PPI and/or did not have a stent implantation in additive or dominant models, although a marginal significant difference existed in patients ≥75 and/or with diabetes.

Association between genetic polymorphisms and clinical outcomes in acute coronary syndrome patients. Each box and horizontal line represents the odds ratio (OR) and 95% confidence interval (CI); each analysis used the C allele for reference. Eight factors were included in the analysis and all factors were adjusted for the other factors. For example, when analyzing age, the factors, including gender, smoke state, plant stent, hypertension, hyperlipemia, diabetes, BBC and PPI were adjusted.
Discussion
A cohort of 851 Chinese patients with acute coronary syndrome was investigated to determine individual responses to clopidogrel. The rates of occurrence for cerebrovascular events, acute myocardial infarction and unstable angina were 9.9%, 11% and 51.5%, respectively. Our results showed that CES1 S75N enhanced the clopidogrel efficacy, leading to a greater clopidogrel response. Moreover, the frequency of the T allele of rs2307240 in ACS patients was significantly higher than that in the general population.
Clopidogrel plays a key role in the treatment of ACS. Clopidogrel is biotransformed into 2-oxo-clopidogrel in hepatic tissue, followed by subsequent hydrolysis into its active thiol metabolite. This is a two-step oxidation reaction catalyzed by cytochrome P450 enzymes. Previous research reported that CES1 was the major enzyme responsible for eliminating clopidogrel, 2-oxo-clopidogrel and the active metabolite20, 21. Additionally, recent investigations have shown that hydrolysis of clopidogrel by CES1 leads to a more than 1,000-fold increase in plasma exposure of clopidogrel carboxylic acid compared to the exposure of the parent clopidogrel and its active metabolite22. Therefore, the production of inactive metabolites occurs at a considerably higher rate compared to the formation of the active metabolite20. Additionally, an increasing number of data suggest that the genetic variation which affects the activity and expression of CES1 may also play an important role in clinical treatment23,24,25.
The remarkably higher incidence of the C allele in the study endpoint group led us to hypothesize that this SNP has a physiological function. In theory, the occurrence of cerebrovascular events, acute myocardial infarction and unstable angina are higher in subjects with the CC genotype than those with the CT + TT genotype due to enhanced formation of active metabolites or reduced elimination of parent clopidogrel in the T allele carriers. The variation of CES1 at position 75 results in a serine-to-asparagine substitution, which may influence protein phosphorylation and affect the catalytic function of CES1. S75N may alter the secondary structure of CES1 protein and influence the interaction between the CES1 protein and ligand. This finding resembles a previous result, in which the 143E substitution resulted in a complete loss of catalytic function26. Altermatively, this variation may also alter CES1 expression by affecting exon skipping, but requires further verification.
Genetic polymorphism plays an important role in the efficacy of clopidogrel treatment. However, clinical factors may influence treatment, such as age, gender, smoking state, stent, hypertension, hyperlipemia, diabetes, BBC and PPI. These variables have been eliminated by stratification analyses in our experiment. However, the association between CES1 S75N and the clopidogrel response persisted after the stratification analysis. Additionally, the relationship between S75N and three clinical outcomes was evident in each subgroup. These results suggest that CES1 S75N may independently affect clopidogrel therapy.
This is the first report on CES1 S75N and it shows the effect of the CES1 S75N variation on clopidogrel therapy. Our results provide important insight into the use of CES1 genotypes in prescribing the most effective anti-platelet therapy. Given that the frequency of the T allele within the general population is relatively low (approximately 5%), we found a much higher incidence in the study endpoint group (11–16%) and in the nonoccurrence group (24–29%). These data indicate that the mutation is a risk factor for acute coronary syndrome. Further research is required to elucidate this hypothesis and demonstrate how this SNP affects clopidogrel therapy and leads to an improved clinical response.
Methods
Study populations
A large cohort of 851 Chinese ACS patients from the Shi-jing-shan Institute of Hypertension (n = 315), Zhengzhou Central Hospital (n = 286) and Xiangya Hospital (n = 250) were eligible for this study, during the period of February 2007 to October 2015. The clinical diagnosis was based on the 2007 ACC/AHA guideline for the diagnosis and treatment of ACS, including acute ST-segment elevation myocardial infarction (STEMI), acute non-ST-segment elevation myocardial infarction (NSTEMI) and unstable angina (UA). All patients took the antiplatelet drug (clopidogrel) at a dose of 75 mg/d for more than one year. Exclusion criteria included contraindications to clopidogrel, noncompliance for more than 12 months, simultaneous anticoagulant treatment and severe hepatic or renal dysfunction. After patients underwent clopidogrel treatment for at least 12 months, a follow-up was performed by clinical visits or telephone interviews.
End-point collection was completed by an independent group that was unaware of genotype information. The primary outcome was the composite of cerebrovascular events (MACCE) and acute myocardial infarction (AMI). The secondary outcome was unstable angina (UA). Patients’ clinical outcomes consisted of cerebrovascular events (MACCE), acute myocardial infarction (AMI) and unstable angina (UA). Among them, acute myocardial infarction included STEMI and NSTEMI, which are defined as recent ischemic symptoms with electrocardiographic abnormalities in the ST segment (depression or elevation of at least 0.1 mV) and a positive troponin concentration as defined locally. UA and recurrent angina (in the hospital) are defined similarly, although electrocardiographic changes are not required. Cerebrovascular events include cerebral hemorrhage and cerebral infarction, which are diagnosed as a focal neurological deficit that persist for more than 24 hours with ischemic or hemorrhage cerebral lesions confirmed by computed tomography (CT) or magnetic resonance imaging (MRI).
This research complied with the Declaration of Helsinki, approval to conduct the research was obtained from the Chinese Clinical Trial Registry, and all participants provided written informed consent (registration number: ChiCTR-OPN-15006260).
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes using standard procedures (Puregene DNA isolation kit, Merck Eurolab). The SNP that potentially affected CES1 activity was chosen by UCSC. As a result, CES1 S75N (rs2307240) was investigated and genotyping was performed by Sequenom MassArray (Sequenom; BioMiao Biological Technology, Beijing, China). The genotype call rate of CES1 S75N was 99.3%.
Statistical analysis
SPSS 18.0 (SPSS, Inc., Somers, NY, USA) was used to calculate summary statistics, distributions, and frequencies in all patients. Three different outcomes, including cerebrovascular events, acute myocardial infarction and unstable angina, were used to investigate the response of clopidogrel. Chi-square tests and Student’s t-tests were used to determine the differences in sex, age, stent (percutaneous coronary intervention with stent implantation), hypertension and smoking among the genotypes. Continuous data are described as the mean ± standard deviation (SD) in the text and tables. Measurement data are expressed as numbers (percentage). The stratified analysis of 851 subjects was performed using PLINK and the association analyses were conducted using two models after adjusting for covariates via Chi-square tests. The additive model accounted for the additive effects of SNPs. Dominant models were tested for the minor allele with two pooled classes. For example, if A is a minor allele, then a is the major allele. The dominant model indicates a genotype of AA or Aa versus aa. The stratified analysis was performed by Stata software.
References
Levine, G. N. et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients with Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. CIRCULATION (2016).
Karazniewicz-Lada, M., Danielak, D. & Glowka, F. Genetic and Non-Genetic Factors Affecting the Response to Clopidogrel Therapy. Expert Opin Pharmacother. 13, 663–683 (2012).
Shuldiner, A. R. et al. Association of Cytochrome P450 2C19 Genotype with the Antiplatelet Effect and Clinical Efficacy of Clopidogrel Therapy. JAMA. 302, 849–857 (2009).
Dansette, P. M., Rosi, J., Bertho, G. & Mansuy, D. Cytochromes P450 Catalyze Both Steps of the Major Pathway of Clopidogrel Bioactivation, Whereas Paraoxonase Catalyzes the Formation of a Minor Thiol Metabolite Isomer. Chem Res Toxicol. 25, 348–356 (2012).
Jiang, X. L., Samant, S., Lesko, L. J. & Schmidt, S. Clinical Pharmacokinetics and Pharmacodynamics of Clopidogrel. Clin Pharmacokinet. 54, 147–166 (2015).
Silvestro, L. et al. Development and Validation of an HPLC-MS/MS Method to Quantify Clopidogrel Acyl Glucuronide, Clopidogrel Acid Metabolite, and Clopidogrel in Plasma Samples Avoiding Analyte Back-Conversion. Anal Bioanal Chem. 401, 1023–1034 (2011).
Tang, M. et al. Antiplatelet Agents Aspirin and Clopidogrel are Hydrolyzed by Distinct Carboxylesterases, and Clopidogrel is Transesterificated in the Presence of Ethyl Alcohol. J Pharmacol Exp Ther. 319, 1467–1476 (2006).
Laizure, S. C., Herring, V., Hu, Z., Witbrodt, K. & Parker, R. B. The Role of Human Carboxylesterases in Drug Metabolism: Have we Overlooked their Importance? Pharmacotherapy. 33, 210–222 (2013).
Hagihara, K. et al. A Possible Mechanism for the Differences in Efficiency and Variability of Active Metabolite Formation From Thienopyridine Antiplatelet Agents, Prasugrel and Clopidogrel. Drug Metab Dispos. 37, 2145–2152 (2009).
Farid, N. A., Kurihara, A. & Wrighton, S. A. Metabolism and Disposition of the Thienopyridine Antiplatelet Drugs Ticlopidine, Clopidogrel, and Prasugrel in Humans. J Clin Pharmacol. 50, 126–142 (2010).
Hosokawa, M. Structure and Catalytic Properties of Carboxylesterase Isozymes Involved in Metabolic Activation of Prodrugs. Molecules. 13, 412–431 (2008).
Shi, D., Yang, D., Prinssen, E. P., Davies, B. E. & Yan, B. Surge in Expression of Carboxylesterase 1 During the Post-Neonatal Stage Enables a Rapid Gain of the Capacity to Activate the Anti-Influenza Prodrug Oseltamivir. J Infect Dis. 203, 937–942 (2011).
Ross, M. K., Borazjani, A., Wang, R., Crow, J. A. & Xie, S. Examination of the Carboxylesterase Phenotype in Human Liver. Arch Biochem Biophys. 522, 44–56 (2012).
Tarkiainen, E. K. et al. Carboxylesterase 1 Polymorphism Impairs Oseltamivir Bioactivation in Humans. Clin Pharmacol Ther. 92, 68–71 (2012).
Lewis, J. P. et al. The Functional G143E Variant of Carboxylesterase 1 is Associated with Increased Clopidogrel Active Metabolite Levels and Greater Clopidogrel Response. Pharmacogenet Genomics. 23, 1–8 (2013).
Zhu, H. J. & Markowitz, J. S. Activation of the Antiviral Prodrug Oseltamivir is Impaired by Two Newly Identified Carboxylesterase 1 Variants. Drug Metab Dispos. 37, 264–267 (2009).
Xie, C. et al. The Effects of CES1A2 A(−816)C and CYP2C19 Loss-Of-Function Polymorphisms On Clopidogrel Response Variability Among Chinese Patients with Coronary Heart Disease. Pharmacogenet Genomics. 24, 204–210 (2014).
Takahashi, S., Katoh, M., Saitoh, T., Nakajima, M. & Yokoi, T. Allosteric Kinetics of Human Carboxylesterase 1: Species Differences and Interindividual Variability. J Pharm Sci. 97, 5434–5445 (2008).
Zhu, H. J. et al. Carboxylesterase 1 as a Determinant of Clopidogrel Metabolism and Activation. J Pharmacol Exp Ther. 344, 665–672 (2013).
Bouman, H. J. et al. Paraoxonase-1 is a Major Determinant of Clopidogrel Efficacy. NAT MED. 17, 110–116 (2011).
Yang, J., Shi, D., Yang, D., Song, X. & Yan, B. Interleukin-6 Alters the Cellular Responsiveness to Clopidogrel, Irinotecan, and Oseltamivir by Suppressing the Expression of Carboxylesterases HCE1 and HCE2. Mol Pharmacol. 72, 686–694 (2007).
Tarkiainen, E. K. et al. Carboxylesterase 1 C.428G > a Single Nucleotide Variation Increases the Antiplatelet Effects of Clopidogrel by Reducing its Hydrolysis in Humans. Clin Pharmacol Ther. 97, 650–658 (2015).
Merali, Z., Ross, S. & Pare, G. The Pharmacogenetics of Carboxylesterases: CES1 and CES2 Genetic Variants and their Clinical Effect. Drug Metabol Drug Interact. 29, 143–151 (2014).
Wang, X. et al. CES1 Genetic Variation Affects the Activation of Angiotensin-Converting Enzyme Inhibitors. PHARMACOGE-NOMICS J. (2015).
Shi, J. et al. Sacubitril is Selectively Activated by Carboxylesterase 1 (CES1) in the Liver and the Activation is Affected by CES1 Genetic Variation. Drug Metab Dispos. 44, 554–559 (2016).
Zhu, H. J. et al. Two CES1 Gene Mutations Lead to Dysfunctional Carboxylesterase 1 Activity in Man: Clinical Significance and Molecular Basis. Am J Hum Genet. 82, 1241–1248 (2008).
Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 81522048, No. 81573511, No. 81273595 and No. 8150131088) and The National High Technology Research and Development Program of China (863 Program) (No. 2012AA02A518 and No. 2012AA02A517).
Author information
Authors and Affiliations
Contributions
All the authors contributed substantially to the manuscript. Wei Zhang and Gan Zhou designed the study; Fei-Yan Xiao, Jian-Quan Luo, Min Liu, Lian-Bi Chen, Shan Cao, Zhao-Qian Liu, Hong-Hao Zhou, Wei Zhang and Gan Zhou performed the research; Fei-Yan Xiao analyzed the data and wrote the manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xiao, FY., Luo, JQ., Liu, M. et al. Effect of carboxylesterase 1 S75N on clopidogrel therapy among acute coronary syndrome patients. Sci Rep 7, 7244 (2017). https://doi.org/10.1038/s41598-017-07736-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-07736-1
This article is cited by
-
Pharmacogenetic study of CES1 gene and enalapril efficacy
Journal of Applied Genetics (2024)
-
Global distribution of CYP2C19 risk phenotypes affecting safety and effectiveness of medications
The Pharmacogenomics Journal (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
