
Abstract
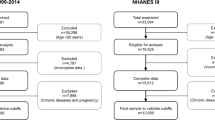
Epidemiological studies have shown that mid-arm circumference (MAC) can be used to predict death risk and malnutrition. We performed a retrospective observational study involving 11,958 US participants aged 20–90 years from the National Health and Nutrition Examination Survey III, 1988–1994, to determine the correlation between MAC and all-cause, cardiovascular, and cancer mortality risk in the obese and non-obese population. Death certificate data were obtained up to 2006. The participants were divided into three groups on the basis of body mass index: 19 ≤ BMI < 25 kg/m2 (normal weight group), 25 ≤ BMI < 30 kg/m2 (overweight group) and BMI ≥ 30 kg/m2 (obesity group); each group was then divided into three subgroups depending on their MAC level. In the non-obese population, MAC was inversely associated with all-cause mortality; specifically, in the normal weight group, the multivariate-adjusted hazard ratio of the T3 (29.6–42.0) cm subgroup was 0.72 (95% confidence interval: 0.58–0.90) when compared with the T1 (18.0–27.2) cm, while the multivariate-adjusted hazard ratio of the T2 (27.3–29.5) cm subgroup was 0.76 (95% confidence interval: 0.64–0.91) when compared with the T1 (18.0–27.2) cm subgroup. The results indicate that MAC is inversely associated with all-cause mortality in non-obese individuals in the United States.
Similar content being viewed by others


Introduction
Numerous epidemiological studies have shown that obesity is associated with a high risk of hypertension, hypercholesterolemia, type 2 diabetes mellitus, cardiovascular disease, and overall death1. Indeed, in the National Health and Nutrition Examination Survey (NHANES) 1999–2004, obesity and overweightness were highly prevalent; in fact, they have become an epidemic among older adults in the United States (US)2. Body mass index (BMI: a person’s weight in kilograms divided by the square of their height in meters) is widely used to screen for overweightness and risk of obesity-related disease3. Troiano et al. reported a U-shaped relationship between mortality and BMI, indicating that both high and low BMI are linked to a higher risk of death4. However, BMI has several limitations as a predictor of mortality: for instance, it does not distinguish between lean and fat mass, nor does it take into account relative fat distribution5,6,7.
Recently, several anthropometric parameters have been used to complement the BMI-based estimation of obesity-related risk and nutritional status; namely, mid-arm circumference (MAC), waist circumference, hip circumference, and skinfold thickness. In this regard, several studies have shown that MAC can be used to reliably estimate the risk of death, particularly in infants and children8, 9. Moreover, Mason et al.10 and Landi et al.11 reported that MAC was inversely associated with all-cause mortality in adults10, 11. However, the link between MAC and cause-specific mortality has not yet been widely explored among obese and non-obese populations in the US. In the present study, we used data from NHANES III to investigate the relationship between MAC and the risk of all-cause, cardiovascular, and cancer mortality among obese and non-obese individuals in the US.
Results
The study population comprised the 11,958 adults in the NHANES III database whose MAC measurements were available. Table 1 summarizes the clinical characteristics of each MAC tertile within the normal weight population. Participants in higher MAC tertile tended to have higher BMI, higher systolic and diastolic blood pressure, higher serum triglyceride levels, lower serum HDL levels, higher serum glucose levels, higher serum uric acid levels, higher serum AST levels, and higher serum total bilirubin levels than those in lower MAC tertile. They were also less likely to be non-Hispanic white, and more likely to be male, and to smoke than those in the lower MAC tertile. Table 2 summarizes the clinical characteristics of each MAC tertile within the overweight population. Participants in higher MAC tertile tended to have higher BMI, higher systolic and diastolic blood pressure, higher serum triglyceride levels, lower serum HDL levels, lower serum C-reactive protein levels, higher serum uric acid levels, higher serum AST levels, and higher serum total bilirubin levels than those in lower MAC tertile. They were also less likely to be non-Hispanic white, and more likely to be male and to smoke than those in the lower MAC tertile. The clinical characteristics of each MAC tertile within the obese population are summarized in Table 3. Participants with higher MAC tertile tended to have higher BMI, higher systolic and diastolic blood pressure, lower serum HDL levels, higher serum C-reactive protein levels, and higher serum uric acid levels than those in lower MAC tertile. They were also more likely to have type 2 diabetes mellitus.
In the present study, the median length of follow-up was 14.3 years. With regard to anthropometric parameters associated with all-cause mortality (shown in Table 4), the unadjusted hazard ratio (HR) for increasing MAC in Model 1 was 0.97 (95% confidence interval [CI]: 0.96–0.98). The multivariate-adjusted HRs in Models 2, 3, and 4 for increasing MAC were 0.95 (95% CI: 0.95–0.97), 0.95 (95% CI: 0.93–0.97), and 0.94 (95% CI: 0.92–0.96), respectively. This result indicates that MAC is inversely associated with all-cause mortality among the general population in the US. An inverse association between MAC and the risk of all-cause mortality was observed in non-obese subjects, with an up to 28% lower HR for all-cause mortality in normal weight participants and 24% lower HR for all-cause mortality in overweight participants, but not in obese subjects (Table 5). There were no apparent relationships between MAC and cardiovascular (Table 6) or cancer mortality (Table 7) in either the non-obese or the obese subjects after multiple-covariate adjustment.
Discussion
In the present study, conducted in the general population in the US, we determined whether there is an association between MAC and all-cause, cardiovascular, and cancer mortality risk; the link between MAC and cause-specific mortality in US obese and non-obese participants had not previously been comprehensively evaluated. The results showed an inverse association between MAC and all-cause mortality in non-obese participants, after various multiple-covariate adjustment strategies, with an up to 28% lower HR for all-cause mortality. There was no such association in obese participants. These findings may have substantial additional clinical implications for death risk prediction, whereby the benefits of MAC may be compromised by the detrimental effects of obesity on all-cause mortality.
MAC has been seen as a valuable anthropometric marker of assessing undernutrition and obesity in children and adolescents2,3,4. Several previous studies have highlighted the predictive value of MAC on all-cause, and cause-specific mortality in both Western and Asian participants12,13,14,15,16,17. Using data from the British National Diet and Nutrition Survey, which followed up 1,054 individuals aged ≥65 years for more than 15 years, Bates et al. demonstrated that each standard deviation (3.3 cm) rise in MAC was associated with a reduced overall mortality risk of 15%12. In addition, in another study involving elderly subjects, Wijnhoven and his colleagues13 reported that the HR for mortality in each lower SD of MAC was 2.26 (95% CI: 1.71–3.00) in women and 1.79 (1.48–2.16) in men. In addition, Chen et al. reported that MAC was a predictor of cause-specific mortality in a cohort study involving 19,575 adults in Bangladesh14. They reported that MAC was inversely correlated with the risk of all-cause and cardiovascular death, and with cardiovascular disease, but not with cancer mortality. These studies indicate that MAC plays a critical role in all-cause and cardiovascular mortality; our own results partially corroborate these previous reports by revealing that MAC may be a predictor of all-cause mortality in non-obese (BMI level: <30) participants in the US.
There are several mechanisms that may mediate the inverse relationship between MAC and all-cause mortality risk in non-obese individuals; for instance, deterioration of fat-free or total muscle mass, impairment of lipid and glucose metabolism, diminished nutritional status, or malnutrition. Firstly, deterioration of fat-free or total muscle mass, which may contribute to reduced MAC, has been linked to higher mortality, as well as to a number of physiological factors and underlying medical illnesses5, 6, 18. For instance, Visser et al.18 reported that higher fat infiltration within muscle tissue, as well as lower muscle mass, was linked to impaired mobility in elderly subjects. Poor muscle strength was associated with disability in activities of daily living19, and reduced physical activity predicted a higher risk of losing muscle mass and strength20, 21. Several underlying chronic conditions (e.g., type 2 diabetes mellitus, stroke, coronary heart disease, and chronic obstructive pulmonary disease) have also been associated with lower muscle mass and strength22. Illness-related muscle deterioration from physical inactivity, systemic inflammation, and nutritional depletion may be associated with higher mortality rates23,24,25,26. Secondly, impairment of lipid and glucose metabolism may play a significant role in the inverse association between MAC and the risk of all-cause mortality. In this regard, Hegarty et al. thoroughly examined the correlation between insulin resistance and intramuscular lipids27, and Olsen et al. demonstrated that arm muscles have better insulin sensitivity and higher insulin-mediated glucose clearance than leg muscles28. Thirdly, diminished nutrition or severe malnourishment, which is directly proportional to MAC, can be linked to an increase in the risk of mortality among infants and children29,30,31. Therefore, it is important to detect malnutrition early, and MAC may be an efficacious and non-invasive tool to assess nutritional status and identify subjects with a high risk of death. Such studies indicate why MAC plays such an important role in predicting all-cause mortality in non-obese individuals.
However, in the present study, the benefits of MAC-which can be used to estimate peripheral subcutaneous adipose tissue load-were compromised by the detrimental effects of obesity on all-cause mortality. There are several possible explanations for such an effect. For instance, the abdominal or visceral fat in obese individuals may cause higher rates of lipolysis, leading in turn to the release of free fatty acids into the circulation, as well as to insulin resistance, atherosclerosis, and type 2 diabetes mellitus, all of which are correlated with an elevated risk of mortality32, 33. Relatedly, recent studies34,35,36 have shown that body fat distribution is relevant to mortality risk, because subcutaneous adipose tissue releases difference levels of anti-inflammatory adipokines, circulating adiponectin, and cytokines, which may play a role in the survival benefits to non-obese individuals.
The present study, which extends the traditional application of MAC for identifying obesity or undernutrition in children and adolescents, provides evidence for an inverse association between MAC and all-cause mortality in non-obese individuals in the US. These findings emphasize the importance of MAC measurement as a substantial additional and clinical predictor of non-obese individuals who are at risk of all-cause mortality.
This study had several limitations. Firstly, the MAC was measured only once during the follow-up period, which may have led to biased results; likewise, the use of self-reported variables may have contributed to reporting bias. Secondly, the NHANES III was an observational survey that was conducted at a single time point, rather than an analysis of long-term repeated observations. Therefore, we were unable to evaluate causality in the relationship between MAC and the risk of cause-specific mortality, which would necessitate repeated MAC measurements over time. Thirdly, we cannot rule out the possibility that some confounding factors in the relationship between MAC and the risk of cause-specific mortality in obese and non-obese individuals remained unmeasured, even though we adjusted for a large number of potentially confounding variables. Several confounding factors, including different type and level of physical activity, may change the risks for mortality. We observed little overlap of MAC level between the non-obese and obese tertiles. The difference level of physical activity between these two groups could have influenced the main results.
In conclusion, we identified that MAC had good predictive ability in predicting follow-up mortality risk of non-obese population in the US. Findings from prior studies demonstrate that MAC may be an effective tool for anthropometric measure and nutritional assessment; however, our study indicated that, in non-obese participants, a significant inverse association exists between MAC and risk of all-cause mortality and higher MAC might provide a beneficial effect. These findings strengthened the importance of using anthropometric assessment tools and indicated that additional studies were warranted to clarify the mechanisms that mediate this relationship.
Materials and Methods
Study Population
Our study sample was representative of the US population and included participants aged 20–90 years, who underwent a survey and a health examination. This constituted a complex sample representing the US non-institutionalized population from NHANES III, 1988 to 1994; details of the survey design and collection procedures have been reported previously37. Demographic data collection in the NHANES III consisted of several components: a structured home interview, physical examination, blood sampling, anthropometric measurement, and body-composition assessment. All participants in the NHANES III provided written informed consent, and the study was approved by National Center for Health Statistics (NCHS) Institutional Review Board before it began; it was executed in accordance with the Declaration of Helsinki.
Mid-Arm Circumference Tertiles-based Subgroups
The participants’ MACs were measured using the standard procedures described by Lohman et al., which depend on the age of the participant38. The participants were divided into three groups on the basis of BMI: 19 ≤ BMI < 25 kg/m2 (normal weight group), 25 ≤ BMI < 30 kg/m2 (overweight group) and BMI ≥30 kg/m2 (obesity group); each group was then divided into three subgroups depending on their MAC level. The tertiles were as follows: T1 (18.0–27.2), T2 (27.3–29.5), T3 (29.6–42.0) cm in the normal weight group, T1 (20.0–31.3), T2 (31.4–33.4), T3 (33.5–52.0) cm in the overweight group and T1 (28.0–35.4), T2 (35.5–38.2), T3 (38.3–61.0) cm in the obesity group.
Follow-up Data on All-Cause, Cardiovascular, and Cancer Mortality
Follow-up data were collected regarding the all-cause, cardiovascular, and cancer mortality of the NHANES III study participants from 1988 to 2006; these data included detailed mortality information from the time of study participation39. The data were provided by the NCHS on the basis of probabilistic matching between the NHANES III participants and the National Death Index death certificate records.
Covariates
The following details were self-reported collected in the NHANES III: age, gender, race/ethnicity, medical conditions (type 2 diabetes mellitus, malignancy, stroke, and congestive heart failure), smoking status, and physical activity. Type 2 diabetes mellitus was self-reported on the basis of a physician’s diagnosis, diagnosed on the basis of random serum glucose level (≥200 mg/dL), or inferred from the participant’s use of diabetic medications (insulin injections and/or oral hypoglycemic agents). An NHANES-associated physician measured systolic and diastolic blood pressure three or four times using a mercury sphygmomanometer, and the average of these readings was used. The serum biochemical profiles were measured at the Lipoprotein Analytical Laboratory at Johns Hopkins University, Baltimore, Maryland. Specifically, serum uric acid level was measured using a Hitachi 737 automated multichannel chemistry analyzer (Boehringer Mannheim Diagnostics, Indianapolis, IN, USA). All measurements were conducted using standardized methods whose accuracy had been documented by the Centre for Disease Control and Prevention (CDC)37, 38.
Physical activity
Participants were asked the following leisure time physical activities, which and how frequently they engaged in during the past month: riding a bicycle, swimming, aerobic or other dance, jogging or running (≥1 mile), callisthenic or floor exercise, weight lifting and gardening or yard work. Duration of the physical activity was not ascertained in NHANES III.
Based on the physical activity intensity value (metabolic equivalent tasks [METs]), which represents the ratio of the energy expenditure of the activity to the basal metabolic rate, the participants classified as ideal, intermediate, and none, respectively40. For instance, the participants was classified as physically active (ideal category) if they engaged in any physical activity with 6 or more METs and 3.0 or more times per week, or any physical activity with 3 to 5.9 METs and 5 or more times per week, meaning that 150 minutes per week or more at moderate vigorous intensity, or 150 minutes per week or more at moderate + vigorous intensity, or 75 minutes per week or more at vigorous intensity. Participants were classified as intermediate category in physical activity: 1 to 149 minutes per week at moderate intensity, or 1 to 149 minutes per week at moderate + vigorous intensity, or 1 to 74 minutes per week at vigorous intensity.
Data Analysis
All statistics were analyzed using SPSS version 18 (SPSS Inc., Chicago, IL); the analyses incorporated sampling weights, and incorrect estimates of variance were prevented using the Complex Samples procedure. We conducted a complete case analysis in the present study. Quantitative variables were summarized in terms of their means and standard deviations (SD), while qualitative variables were summarized in terms of their frequency and percentages. Differences in demographic characteristics were tested using the independent t-test or Wilcoxon Rank sum test (for continuous variables), or the Chi-square test (for discrete variables). Two-sided p-values of less than 0.05 were regarded as indicating statistical significance. Multivariate Cox proportional hazard models were used to evaluate the association between the MAC tertiles in obese or non-obese subjects, and all-cause, cardiovascular, and cancer mortality. An extended-model approach was used adjust for covariates: Model 1 was not adjusted for any other variables; Model 2 was further adjusted for age, race, sex, and BMI; Model 3 was adjusted for all the additional variables that were in Model 2, as well as for serum triglycerides, serum HDL, serum glucose, serum aspartate transaminase, C-reactive protein, serum uric acid, and serum total bilirubin. Model 4 was similar to Model 3, but the following additional factors were also adjusted for: physical activity, systolic blood pressure, smoking, and type 2 diabetes mellitus.
References
Masters, R. K., Powers, D. A. & Link, B. G. Obesity and US mortality risk over the adult life course. Am J Epidemiol 177, 431–442 (2013).
Ogden, C. L. et al. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 295, 1549–1555 (2006).
Deurenberg, P., Weststrate, J. A. & Seidell, J. C. Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. Br J Nutr 65, 105–114 (1991).
Troiano, R. P., Frongillo, E. A., Sobal, J. & Levitsky, D. A. The relationship between body weight and mortality: A quantitative analysis of combined information from existing studies. Int J Obes Relat Metab Disord 20, 63–75 (1996).
Heitmann, B. L., Erikson, H., Ellsinger, B. M., Mikkelsen, K. L. & Larsson, B. Mortality associated with body fat, fat-free mass and body mass index among 60-year-old Swedish men-a 22-year follow-up. The study of men born in 1913. Int J Obes Relat Metab Disord 24, 33–37 (2000).
Allison, D. B., Zhu, S. K., Plankey, M., Faith, M. S. & Heo, M. Differential associations of body mass index and adiposity with all-cause mortality among men in the first and second National Health and Nutrition Examination Surveys (NHANES I and NHANES II) follow-up studies. Int J Obes Relat Metab Disord 26, 410–416 (2002).
Oppert, J. M. et al. Anthropometric estimates of muscle and fat mass in relation to cardiac and cancer mortality in men: the Paris Prospective Study. Am J Clin Nutr 75, 1107–1113 (2002).
Mwangome, M. K., Fegan, G. & Fulford, T. Mid-upper arm circumference at age of routine infant vaccination to identify infants at elevated risk of death: a retrospective cohort study in the Gambia. Bull World Health Organ 90, 887–894 (2012).
Rasmussen, J. et al. Mid-upper-arm-circumference and mid-upper-arm circumference z-score: the best predictor of mortality? Eur J Clin Nutr 66, 998–1003 (2012).
Mason, C., Craig, C. L. & Katzmarzyk, P. T. Influence of central and extremity circumferences on all-cause mortality in men and women. Obesity (Silver Spring) 16, 2690–2695 (2008).
Landi, F. et al. Midarm muscle circumference, physical performance and mortality: results from the aging and longevity study in the Sirente geographic area (ilSIRENTE study). Clin Nutr 29, 44–47 (2010).
Bates, C. J., Hamer, M. & Mishra, G. D. A study of relationships between bone-related vitamins and minerals, related risk markers, and subsequent mortality in older British people: the National Diet and Nutrition Survey of People Aged 65 Years and Over. Osteoporos Int 23, 457–466 (2012).
Wijnhoven, H. A. et al. Low mid-upper arm circumference, calf circumference, and body mass index and mortality in older persons. J Gerontol A Biol Sci Med Sci 65, 1107–1114 (2010).
Chen, Y. et al. A prospective study of arm circumference and risk of death in Bangladesh. Int J Epidemiol 43, 1187–1196 (2014).
Menotti, A., Puddu, P. E., Lanti, M., Maiani, G. & Fidanza, F. Cardiovascular risk factors predict survival in middle-aged men during 50 years. Eur J Intern Med 24, 67–74 (2013).
Puddu, P. E., Menotti, A., Tolonen, H., Nedeljkovic, S. & Kafatos, A. G. Determinants of 40-year all-cause mortality in the European cohorts of the Seven Countries Study. Eur J Epidemiol 26, 595–608 (2011).
Dontas, A. S., Menotti, A., Aravanis, C., Ioannidis, P. & Seccareccia, F. Comparative total mortality in 25 years in Italian and Greek middle aged rural men. J Epidemiol Community Health 52, 638–644 (1998).
Visser, M. et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J Gerontol A Biol Sci Med Sci 60, 324–333 (2005).
Rantanen, T. et al. Disability, physical activity, and muscle strength in older women: The Women’s Health and Aging Study. Arch Phys Med Rehabil 80, 130–155 (1999).
Rantanen, T., Era, P. & Heikkinen, E. Physical activity and the changes in maximal isometric strength in men and women from the age of 75 to 80 years. J Am Geriatr Soc 45, 1439–1445 (1997).
Roubenoff, R. Sarcopenia and its implications for the elderly. Eur J Clin Nutrition 54(Suppl 3), S40–S47 (2000).
Rantanen, T. et al. Grip strength changes over 27 yr in Japanese-American men. J Appl Physiol 85, 2047–2053 (1998).
Gosker, H. R., Wouters, E. F., van der Vusse, G. J. & Schols, A. M. Skeletal muscle dysfunction in chronic obstructive pulmonary disease and chronic heart failure: underlying mechanisms and therapy perspectives. Am J Clin Nutr 71, 1033–1047 (2000).
Corti, M. C., Guralnik, J. M., Salive, M. E. & Sorkin, J. D. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 272, 1036–1042 (1994).
Harris, T. B. et al. Associations of elevated interleukin-6 and C-reactive protein levels with mortality in the elderly. Am J Med 106, 506–512 (1999).
Hakim, A. A. et al. Effects of walking on mortality among nonsmoking retired men. N Engl J Med 338, 94–99 (1998).
Hegarty, B. D., Furler, S. M., Ye, J., Cooney, G. J. & Kraegen, E. W. The role of intramuscular lipid in insulin resistance. Acta Physiol Scand 178, 373–383 (2003).
Olsen, D. B., Sacchetti, M., Dela, F., Ploug, T. & Saltin, B. Glucose clearance is higher in arm than leg muscle in type 2 diabetes. J Physiol 565(Pt 2), 555–562 (2005).
Sachdeva, S., Dewan, P., Shah, D., Malhotra, R. K. & Gupta, P. Mid-upper arm circumference v. weight-for-height Z-score for predicting mortality in hospitalized children under 5 years of age. Public Health Nutr 6, 1–8 (2016).
Fiorentino M. et al. Current MUAC Cut-Offs to Screen for Acute Malnutrition Need to Be Adapted to Gender and Age: The Example of Cambodia. PLoS One 11, e0146442, doi:10.1371/journal.pone.0146442. eCollection 2016 (2016).
Aguayo, V. M., Aneja, S., Badgaiyan, N. & Singh, K. Mid upper-arm circumference is an effective tool to identify infants and young children with severe acute malnutrition in India. Public Health Nutr 18, 3244–3248 (2015).
Arner, P. Differences in lipolysis between human subcutaneous and omental adipose tissues. Ann Med 27, 435–438 (1995).
Debette, S. et al. Calf circumference is inversely associated with carotid plaques. Stroke 39, 2958–2965 (2008).
Kalantar-Zadeh, K., Abbott, K. C., Salahudeen, A. K., Kilpatrick, R. D. & Horwich, T. B. Survival advantages of obesity in dialysis patients. Am J Clin Nutr 81, 543–554 (2005).
Kalantar-Zadeh, K. & Ahmadi, S. F. Carrying a heavier weight is healthy: Obesity-reinforced fitness hypothesis in metabolically healthy obesity. Obesity (Silver Spring) 24, 281–282 (2016).
Deng, Y. & Scherer, P. E. Adipokines as novel biomarkers and regulators of the metabolic syndrome. Ann N Y Acad Sci 1212, E1–E19 (2010).
National Center for Health Statistics, Hyattsville. Plan and operation of the Third National Health and Nutrition Examination Survey, 1988-94. Series 1: programs and collection procedures. Vital Health Stat 1 32, 1–407 (1994).
Lohman T. G., Roche A. F. & Martorell R. Anthropometric Standardization Reference Manual. Abridged ed. Champaign, IL: Human Kinetics Books (1988).
The National Center for Health Statistics. Office of Analysis and Epidemiology, Third National Health and Nutrition Examination Survey (NHANES III), Linked Mortality File, Mortality follow-up through 2006: Matching Methodology; 2009 [cited 2014 May 21] Available from: http://www.cdc.gov/nchs/data/datalinkage/matching_methodology_nhanes3_final.pdf.
Yang, Q. et al. Trends in cardiovascular health metrics and associations with all-cause and CVD mortality among US adults. JAMA 307, 1273–1283 (2012).
Author information
Authors and Affiliations
Contributions
Li-Wei Wu contributed to the design of the study, was responsible for the management and retrieval of data, contributed to initial data analysis and interpretation, and drafted the initial manuscript. Li-Wei Wu, Yuan-Yung Lin, Tung-Wei Kao, Chien-Ming Lin, Chung-Ching Wang, Gia-Chi Wang, Tao-Chun Peng, Wei-Liang Chen decided upon the data collection methods. Li-Wei Wu and Wei-Liang Chen were also responsible for the data analysis decisions. Wei-Liang Chen conceptualized and designed the study, supervised all aspects of the study, critically reviewed and revised the manuscript, and approved the final manuscript as submitted. All authors meet the ICMJE criteria for authorship.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wu, LW., Lin, YY., Kao, TW. et al. Mid-Arm Circumference and All-Cause, Cardiovascular, and Cancer Mortality among Obese and Non-Obese US Adults: the National Health and Nutrition Examination Survey III. Sci Rep 7, 2302 (2017). https://doi.org/10.1038/s41598-017-02663-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-02663-7
This article is cited by
-
Association between complementary anthropometric measures and all-cause mortality risk in adults: NHANES 2011–2016
European Journal of Clinical Nutrition (2024)
-
Trajectory of mid-arm subcutaneous fat, muscle mass predicts mortality in hemodialysis patients independent of body mass index
Scientific Reports (2024)
-
Prevalence of hypertension and its associations with body composition across Chinese and American children and adolescents
World Journal of Pediatrics (2024)
-
The L-shaped association of mid-upper arm circumference with all-cause and cause-specific mortality in US adults: a population-based prospective cohort study
BMC Public Health (2023)
-
Association between segmental body composition and bone mineral density in US adults: results from the NHANES (2011–2018)
BMC Endocrine Disorders (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
