
Abstract
Human motion capture and analysis could be made easier through the use of wearable devices such as inertial sensors and/or pressure insoles. However, many steps are still needed to reach the performance of optoelectronic systems to compute kinematic parameters. The proposed dataset has been established on 10 asymptomatic adults. Participants were asked to walk at different speeds on a 10-meters walkway in a laboratory and to perform different movements such as squats or knee flexion/extension tasks. Three-dimensional trajectories of 69 reflective markers placed according to a conventional full body markerset, acceleration and angular velocity signals of 8 inertial sensors, pressure signals of 2 insoles, 3D ground reaction forces and moments obtained from 3 force plates were simultaneously recorded. Eight calculated virtual markers related to joint centers were also added to the dataset. This dataset contains a total of 337 trials including static and dynamic tasks for each participant. Its purpose is to enable comparisons between various motion capture systems and stimulate the development of new methods for gait analysis.
Similar content being viewed by others

Background & Summary
Human motion measurement and analysis represent a major topic in the medical field to understand people’s gross motor function, e.g. to identify possible risks of fall1 or to understand gait deviations2. This is usually performed with an optoelectronic system in a gait laboratory. However, this method requires qualified staff (especially for the marker placement which is done by palpation by an examiner and which is the largest source of variability3), advanced and expensive technological equipments4, and is time-consuming. These factors usually restrain such analyses to large medical institutions. In recent years, wearable systems have been trusted into the forefront of movement analysis due to their miniaturization. This is particularly the case for inertial sensors, also called Inertial Measurement Units (IMUs), that are commonly composed of a 3-axis accelerometer, a 3-axis gyroscope and eventually a 3-axis magnetometer5. By attaching these sensors to a set of body segments, they could give access to a quick, easy-to-use and less expensive gait analysis than an optoelectronic system4. Their use is increasingly popular in human movement science as evidenced by many studies in the field6.
Few datasets have been made available in the literature and can be used to validate the different steps of 3D kinematic calculations7,8. The measurements carried out in the present study provide a comprehensive dataset9 on asymptomatic participants with the 3D trajectories of 37 cutaneous markers, 32 cluster markers and 8 calculated joint centers, the signals of 8 IMUs placed on each lower-limb segment, on the pelvis and on the torso, the signals of 2 insoles, and the signals of 3 force plates installed in the middle of the walkway. The two last devices give also access to kinetic data and open comparison with other studies10. Various movements have been recorded, such as gait at different speeds (i.e. slow gait, comfortable gait, fast gait), running, squats and functional tasks.
The primary objective of this study was to provide a dataset9 allowing the comparison, validation, and improvement of different wearable motion capture systems and could lead to the development of a clinical protocol for clinical gait analysis outside the laboratory11. In particular, the resulting dataset is oriented towards the computation of lower-limb kinematics using IMUs, the computation of spatio-temporal parameters using instrumented insoles, and the development of activity detection algorithms using IMUs and insoles data, useful in many applications12,13,14,15. This work was carried out during the study of Carcreff et al.16. With the knowledge of the position and orientation of the IMU sensors in the optoelectronic camera coordinate system, the dataset was used to validate algorithms for calculating kinematics from inertial data16. This dataset9 could thus be used alone, or merged with another dataset, to validate such procedures and methods.
Methods
Participants
Ten asymptomatic participants (4 women and 6 men, 29.7 ± 6.4 years, 1.74 ± 0.06 m, 68.0 ± 13.9 kg) were recruited on a voluntary basis. The study was approved by the Ordinance on Human Research17 (project ID: CCER-2020-00358) with the exception of Clinical trials and follows the Swiss legal requirements, the current version of the World Medical Association Declaration of Helsinki and the principles of Good Clinical Practice. All participants gave their informed consent prior to their participation in the study. They were included if they were between 5 and 70 years old, asymptomatic (i.e. healthy without any disease affecting gait), with no previous surgery on lower limbs nor spine in the last two years, no allergy to hypoallergenic adhesive tape, and no known pregnancy.
Records
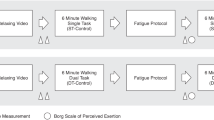
A 12-camera optoelectronic system (Oqus 7+, Qualisys, Göteborg, Sweden) sampled at 100 Hz was used to track the 3D trajectories of 69 reflective markers placed on anatomical landmarks and on clusters. Anatomical markers (14 mm diameter) of the lower body were placed according to the Conventional Gait Model 1.018 (Fig. 1) and the markers of the upper body were placed according to the Plug In Gait model (Vicon Motion Systems, Oxford, UK)19. A full description of each marker is reported in Table 1 and in Table 2.

Reflective markers of the lower body placed according to the Conventional Gait Model 1.0 + reflective markers of the upper body placed according to the Plug In Gait model + LFMH marker (red markers), cluster markers (black markers) to track inertial sensors and calculated virtual markers, i.e. joint centers (green markers).
Three force plates sampled at 1000 Hz (AMTI Accugait, Watertown, MA, USA) were used to record 3D ground reaction forces and moments. Available ground reaction forces and moments across participants and trials are accesible in Table 3. A description of force plate data is reported in Table 4.
Eight IMUs (Physilog6S, GaitUp, Renens, Switzerland) sampled at 256 Hz were strapped (SuperWrap, Qualisys, Göteborg, Sweden) on feet, shanks, thighs, pelvis and trunk (Figs. 1, 2). They recorded 3D linear accelerations with a range of ±16 g, 3D angular velocities with a range of ±2000 °/s, 3D magnetic field intensity with a range of ±50 mT, and the barometric altitude from 260 to 1260 hPa. A short description of IMUs data is presented in Table 5. The IMUs were switched on about 10 minutes before the beginning of the recordings, levelled horizontally, and all aligned. The measurement of the IMUs at rest can be found in the raw data (bin file). It is therefore possible for each user to develop its own algorithms. The “master” sensor was always switched on last, in order to have the same routine for all measurements and to have approximately the same switch-on delay. Each IMU was placed on a 3D printed cluster of four markers (9.5 mm diameter) to track its position and orientation in the global coordinate system defined by the optoelectronic system (Fig. 3). Then, IMUs were switched off after the end of recordings under the same conditions as for the switch on.

Full setup on a participant, including systems used during the measurement and fixing tools.

Definition of the coordinate systems of each device used during the measurement.
Two insoles (Insole3, Moticon ReGo AG, Munich, Germany) sampled at 100 Hz were used to measure feet plantar pressures. These insoles were composed of 16 pressure sensors, a 3D accelerometer and a 3D gyroscope, as described in Table 6 and Fig. 4. The total area covered by pressure sensors ranged from 7.6 mm2 to 16.5 mm2 depending on sensor insoles (Fig. 4). They were switched on just before the beginning of the recordings (after the participant preparation) and were switched off after the end of recordings and data transfer to the computer.

Sensor insoles outline and plantar sensor positions. Adapted from Moticon Science Sensor Insole specification.
Procedure
For each participant, the entire data collection was performed in a single session which lasted approximately one hour. All sessions were managed by two operators, one was experienced in placing the anatomical markers and the other performed data recordings. The following procedure was adopted:
Calibration of the systems
The calibration of the motion capture system was performed following the instructions available in the manufacturer’s documentation, including the definition of the global coordinate system, the dynamic calibration of the cameras, and the zeroing of the force plates. The calibration of the pressure insoles was also performed following the instructions of the manufacturer’s documentation, including the zeroing (i.e. the automatic zeroing mode is based on algorithms continuously checking sensor zero levels and compensates for sensor offsets and drifts which may occur due to lacing shoes and due to temperature changes. In addition, a manual zeroing routine can be carried out by means of a software function20) and the calibration (i.e. the calibration routine is carried out using the app and included very-slow gait and static postures20) of the insoles. No calibration was required for the IMUs following the manufacturer’s recommendations.
Introduction to the participant
The operators introduced the laboratory, and briefly explained the conduct of the session, and the material used.
Preparation of the participant
The participant was asked to change clothes to tight-fitting clothes or underwear, and was asked to be barefoot. An operator collected the participant’s anthropometric data (i.e. height, body mass, as well as pelvic, knees and ankles width). The participant was then equipped with cutaneous reflective markers attached with double-sided adhesive tape, IMUs placed in marker clusters and fixed with straps, and sensor insoles placed in sandals (participants had to walk with shoes) (Fig. 2).
Synchronization record
Systems’ synchronization tasks (i.e. IMU-to-optoelectronic and insole-to-IMU synchronizations) were performed at the beginning and at the end of each session since no hardware synchronization was available. IMU-to-optoelectronic synchronization task consisted of inducing a vertical acceleration on a rod equipped with an IMU and two reflective markers. Insole-to-IMU synchronization task consisted of a jump performed by the participant equipped with IMUs and insoles. The alignment of the systems’ timestamps was performed in post-processing using the recorded data.
Static trial
A 10-second recording was performed with the participant standing upright (T-pose) on the force plate in the middle of the walkway with straight legs, and parallel feet hip-width apart (Supplementary Table 1). This position allowed a recording with all the markers to reconstruct marker trajectories when there were marker trajectory gaps by rigid transformation21. The proper propostion of the subject was carefully controlled by the experimenter (Supplementary Table 1) before starting the acquisition since the task was to be used for IMU-to-segment calibration16,22,23. The verbal instruction was: “Spread your arms slightly and stay in a static position for 10 seconds without moving.”
Walking trials
The participant was asked to walk back and forth on the 10-m walkway at three different speeds: comfortable speed, slow speed and fast speed. No instruction was given about the force plates to ensure the most natural gait. A minimum of 8 trials were recorded for each subject for the comfortable speed to ensure a minimum of 7 validated force plate data (left and right side taken together), and 2 trials were recorded for the two other speeds whatever the force plate recordings. Details of available force plate data for each participant and for each task are reported in Table 1. The verbal instruction for the comfortable speed was: “Walk naturally to the other end of the walkway at a comfortable speed.”; The verbal instruction for the slow speed was: “Walk more slowly than before to the other end of the walkway.”; The verbal instruction for the fast speed was: “Walk quickly to the other end of the walkway but do not run.” The instructions given to the participants are detailed in Supplementary Table 1.
Running trials
The participant was asked to run at a spontaneous speed without sprinting in order to avoid too many marker occultations. Two trials were recorded whatever the force plate recordings. The verbal instruction was: “Run to the other end of the walkway without sprinting.” (Supplementary Table 1).
Calibration trials
Five different movements, being 5 independent trials stored in separate files, were performed by the participant: 1) 5 squats with a medium flexion and standing on the heels at the end of knees extension, 2) 5 hip abductions and adductions on both sides consecutively, 3) 5 hip/knee/ankle flexions on both sides consecutively, 4) 5 hip rotations on both sides consecutively, and 5) 5 pelvis rotations, 5 pelvis anteversions and retroversions, and 5 pelvis obliquities. Because of the length of all the verbal instructions, these are detailed in Supplementary Table 1. These trials can be used to perform IMU-to-segment calibration16,22,23.
Timed Up and Go trials
Two Timed Up and Go (TUG) tests24 were performed, one with a 3-m walking part and another one with 5-m walking part. The participant started out sitting on a stool, got up, walked 3 or 5 meters, turned around and returned to sit on the stool. No instruction was given to the participant to perform the task, he/she just started with his/her arms at their sides (Supplementary Table 1). The participant was seated on a stool and not a chair to avoid back marker occultations. The verbal instruction was: “Stand up and walk 3 meters to the cone, turn around and walk back to the stool, turn to sit down and sit down.”
Sit to Stand trials
This task was adapted from the standardized sit to stand test25. The participant was asked to stand up from a stool and sit down five consecutive times26 as quickly as possible. Participant’s arms were crossed on stomach or chest to avoid marker occultations (Supplementary Table 1). The verbal instruction was: “Stand up and sit down 5 times as fast as possible.”
Sitting trials
The participant began in a sitting position with an angle of 90° at hip, knee and ankle levels, and with a straight chest. A minimum of five seconds without movement were recorded. Then, the participant was asked to extend his/her legs and tilt his/her chest, and a minimum of five seconds without movement were again recorded. Finally, a passive flexion/extension of the knee and ankle was induced by the operator on both sides consecutively (Supplementary Table 1). The verbal instruction was: “Keep your arms at your sides and sit still for 5 seconds (without moving). Then, sit with your legs straight, without moving, for 5 seconds – only your heels touch the ground.”
2-minute trials
The participant was asked to walk back and forth along 20 m at comfortable speed. No instruction was given about the force plates to ensure the most natural gait. Since the field of view of the optoelectronic cameras is only 5 m and to avoid having a too long recording, several recordings were started each time the participant entered the cameras’ field of view. Thus, during the 2-minute trial, there were at least three recordings. The verbal instruction was: “Walk naturally to the other end of the walkway at a comfortable speed, and turn around and go to the other end during 2 minutes.”
Data processing
Three-dimensional marker trajectories and ground reactions were labelled with the Qualisys Tracking Manager software (QTM 2019.3, Qualisys, Göteborg, Sweden). Raw data were exported in c3d file format (https://www.c3d.org) and processed under Matlab (R2019b, The MathWorks, USA) using the Biomechanics Toolkit (BTK)27. Marker trajectories processing consisted in an interpolation to fill gaps using a reconstruction based on marker inter-correlations28.
Joint centers of the lower limbs and the center of the posterior and anterior iliac spines were calculated and added as virtual markers in each trial file. Hip joint centers were computed with Hara’s regression equations29, while other joint centers were calculated with a chord function30.
Ground reaction processing consisted in (1) a data zeroing and (2) 3D centre of pressure (CoP) recomputation. The zeroing process was required as some trials showed an offset of the force data, even if a platform reset was performed at the beginning of each session.
The CoP recomputation was required due to incompatibility of the BTK c3d parser and the type of force plate and in particular the AMTI Accugait Type 5 used in this study. A custom Matlab program was used for this purpose. No filtering was applied on both marker trajectories and force plates data.
Gait events (i.e. foot strikes and foot offs) related to slow gait, comfortable gait, fast gait and 2-min trials were automatically detected using a validated algorithm proposed by Zeni et al.31. Each file containing the events detected has been visually checked and corrected if necessary using the open-source software Mokka (http://biomechanical-toolkit.github.io/). For this process, running and TUG trials were excluded to avoid any detection problems due to marker occultations and turnaround during tests. The three force plates were not used for gait event detection because of the low number of steps. Regarding the insoles, we did not have direct access to the events detected by the software and we did not implemented/validated any code for it. It is still possible to add events manually using for instance the open-source software Mokka.
All data and metadata (description of the data organization provided in the dataset9) recorded by the optoelectronic system and force plates were stored in c3d file format (binary files, see Code Availability section for file reading and https://www.c3d.org/) by task and session.
IMUs position and orientation were tracked using the marker clusters to perform calibrations. Indeed, many studies have shown the importance of performing a IMU-to-segment calibration16,22,23 to ensure that IMUs are properly aligned with the anatomical axes. This calibration largely influences kinematics computation22. Several IMU-to-segment approaches exist; the most common being the functional calibration which consists of aligning the sensors and segments frames based on specific 2D-movements realized by the subject23. Thus, the proposed dataset9 is composed of several functional tasks performed in different anatomical planes to allow IMU-to-segment calibration (e.g. flexion/extensions, rotations, ab/adductions).
No data processing was performed on IMUs and insoles data. The IMUs data were stored in bin file format (binary files, see Code Availability section for file reading) and the insoles data in txt file format (ASCII files) by session.
Optoelectronic and IMUs data could not be synchronized with a hardware system because the version of IMUs we used did not include this function. Thus, the data were synchronized using the start and end impacts with acceleration peak detection (see Procedure 4. Synchronization record). IMUs and insoles data were synchronized using jump events. The optoelectronic and force plates data were not cut. For the IMUs and insoles files, the data were synchronized respectively with peak detection and cross-correlation functions. Then, these data were resampled to 100 Hz (optoelectronic sampling frequency), cropped according to the synchronized timestamps and stored in a csv format (ASCII file) by task and session. These files contain synchronized marker trajectories, linear accelerations and angular velocities of IMUs and all insole data.
All other data such as anthropometric data as well as non-synchronized force plate data, gait events, and IMU barometers are only stored in c3d or bin files. It should be noted that the synchronization procedure precision is approximated at 0.1 second due to the manual detection performed using a custom Matlab program. The difficulty was to be precise for the operator.
Thus, it is strongly recommended that each user resynchronizes the data for their own applications if needed. For this purpose, users can use the raw data present in the data repository.
Missing data
There was no insole data for Participant 01 because of a delay in the delivery of the devices from the start of the study. During the 2-minute trials of the Participant 03 the Qualisys Tracking Manager software crashed and recordings could not be saved. Finally, for the Participant 05, the left thigh (LT) IMU sensor stopped during the measurement and no data were recorded.
Data Records
Data description
All recorded data are described in detail in Excel files available in the dataset9. Each optoelectronic, IMUs, and insole data have their own Excel file with a detailed description of the acquired data (e.g. for the IMUs, the parameters of each electronic sensor are described as well as the location of the “master” sensor and the synchronization information data between the sensor set). Moreover, in the optoelectronic Excel file, a complete list of tasks performed or not by the participants as well as associated comments (in case of errors or problems occurred during data acquisition and post-processing) are given. Finally, each Excel file contains a “Description” sheet that summarizes the content of the other sheets present in the file.
All data files are available online on a Yareta database9: https://doi.org/10.26037/yareta:xkxgaw6ewjdhfntdhtj7upepxy.
Data are organized by participant folder (PXX_SYY, P: for Participant, S: for Session) and each folder contains two sub-folders:
-
RAW_DATA
-
One .c3d file per trial recorded during the session
-
Eight .bin files corresponding to the IMUs data recorded during the session
-
One .txt file corresponding to the insole data recorded during the session
-
-
SYNC_DATA
-
One .csv file per trial with all the optoelectronic, IMUs and insole synchronized data recorded during the session
-
C3D trial files are referenced in our dataset9 as PXX_SYY_[Trial type]_[Trial number].c3d, with the following correspondence:
-
P: for Participant
-
XX: participant number (e.g. 01)
-
S: for Session
-
YY: session number (e.g. 01)
-
[Trial type]: task performed (Table 7)
Table 7 Description of trial tasks. -
[Trial number]: trial number (e.g. 01)
IMUs are referenced as PXX_SYY_ZZ_Inertial_sensor.bin, with:
-
ZZ: sensor name including TR: torso/SA: pelvis/RT: right thigh/RS: right shank/RF: right foot/LT: left thigh/LS: left shank/LF: left foot
Insoles data are referenced as PXX_SYY_Sensor_insoles.txt.
Synchronized data are referenced with the same name as c3d files but with the file extension .csv.
Technical Validation
Calibration of the optoelectronic system
The optoelectronic system was calibrated before each session following the instruction available in the manufacturer’s documentation. The standard deviation of the calibration tool length for all the sessions was on average 1.5 mm for a calibrated volume of 5 × 2 × 2 m and the average residuals (i.e. the minimum distance between a 2D marker ray and its corresponding 3D point) of the markers were below 2.5 mm. This value of 1.5 mm could be reduced for a smaller volume, but for the volume used in this study, it was not possible to define a focal length allowing a sharpness on the whole length of 5 m.
3D trajectories of reflective markers
For all dynamic trials of all sessions, the 3D marker trajectories were fill gapped and 0% of gap is thus present in the reported trajectories, except for synchronization tasks where a gap may be present at the impact. Average residuals of the markers were below 1.3 mm. These data were not filtered.
Inertial sensors
No calibration task was recommended by the manufacturer’s documentation, as the IMUs have been calibrated in factory. The sensor noises are as follows:
-
Accelerometer: average standard deviation <7 mg (milli g-force)
-
Gyroscope: average standard deviation <1.3 dps (degree per second)
-
Magnetometer: average standard deviation <10 mG (milli-Gauss) for X- and Y-axes, <15 mG for Z-axis
-
Barometer: average standard deviation <0.06 mBar (after low frequency variation removal)
Sensor insoles
Sensor insoles were calibrated for each participant before the session according to the instruction given by the manufacturer. A zeroing of each insole was performed before the start of the acquisition as well as a calibration sequence consisting of a slow walking, a standing still and body weight shifts. Temporal drift, i.e. the total drift of the timing data over time since the start of the measurement, has been estimated by the manufacturer to be less than 1%.
Limitations
The main limitation of using this data set is the small number of participants. Indeed, only 10 participants were included and three of them had missing data.
Another limitation is the synchronization of the systems. Because of the lack of synchronization accuracy (0.1 s) and data cropping, the authors suggest that users use the synchronized data with caution or develop their own synchronization algorithms.
In addition, no information was given by the manufacturer of the IMUs, either for sensor calibration or gyro zeroing. The gains and offsets were therefore not modified during the measurement.
The use of different acquisition frequencies between the systems (256 Hz for IMUs and 100 Hz for optoelectronics) may lead to errors during resampling. The value of 100 Hz for the optoelectronic data was chosen to keep some consistency between the acquired data and the existing database of the laboratory. Regarding the 256 Hz frequency for the IMUs, it was chosen to record high speed running movements (sprint tasks). However, these tasks are not present in the dataset because the optoelectronic data were not usable.
Usage Notes
Optoelectronic data and metadata stored in c3d files can be directly read using the open-source motion analyzer software Mokka (http://biomechanical-toolkit.github.io/). It is also possible to read these data in a scripting software (e.g. Matlab) using a c3d parser like Biomechanics ToolKit (BTK) (http://biomechanical-toolkit.github.io/). Concerning IMUs data, the manufacturer provides a software to read the sensor signals stored in bin files (Research Toolkit for Physilog6S, https://research.gaitup.com/support/#1610537099987-3-1). A Matlab toolkit is also available on their website (https://physilog.com/). The raw data of sensor insoles can be read with any text editor.
Code availability
Matlab codes used to preprocess data, compute joint centers and identify gait events are shared in open access through dedicated gitlab repositories (respectively: https://gitlab.unige.ch/KLab/preprocessing_toolbox, https://gitlab.unige.ch/KLab/fusion_biplane_xrays_motion_capture and https://gitlab.unige.ch/KLab/gev).
The Biomechanics Toolkit (BTK) is freely available on the following repository: https://github.com/Biomechanical-ToolKit/BTKCore.
The IMUs data reader is freely available on the following website: https://physilog.com/).
References
Herssens, N., How, D., van de Berg, R. & McCrum, C. Falls Among People With Bilateral Vestibulopathy: A Review of Causes, Incidence, Injuries, and Methods. JAMA Otolaryngol. Neck Surg. 148, 187 (2022).
Armand, S., Decoulon, G. & Bonnefoy-Mazure, A. Gait analysis in children with cerebral palsy. EFORT Open Rev. 1, 448–460 (2016).
Gorton, G. E., Hebert, D. A. & Gannotti, M. E. Assessment of the kinematic variability among 12 motion analysis laboratories. Gait Posture 29, 398–402 (2009).
Mayagoitia, R. E., Nene, A. V. & Veltink, P. H. Accelerometer and rate gyroscope measurement of kinematics: an inexpensive alternative to optical motion analysis systems. J. Biomech. 35, 537–542 (2002).
Constant, N. et al. Chapter 13 - Data analytics for wearable IoT-based telemedicine. in Wearable Sensors (Second Edition) (ed. Sazonov, E.) 357–378 (Academic Press, 2021).
Kobsar, D. et al. Wearable Inertial Sensors for Gait Analysis in Adults with Osteoarthritis-A Scoping Review. Sensors 20, E7143 (2020).
Weygers, I. et al. Reference in-vitro dataset for inertial-sensor-to-bone alignment applied to the tibiofemoral joint. Sci. Data 8, 208 (2021).
Schreiber, C. & Moissenet, F. A multimodal dataset of human gait at different walking speeds established on injury-free adult participants. Sci. Data 6, 111 (2019).
Grouvel, G., Armand, S., Moissenet, F., & Carcreff, L. Human gait and other movements - markers / inertial sensors / pressure insoles / force plates. Université de Genève, Yareta https://doi.org/10.26037/yareta:xkxgaw6ewjdhfntdhtj7upepxy (2022).
Dorschky, E., Nitschke, M., Seifer, A.-K., van den Bogert, A. J. & Eskofier, B. M. Estimation of gait kinematics and kinetics from inertial sensor data using optimal control of musculoskeletal models. J. Biomech. 95, 109278 (2019).
Fusca, M. et al. Validation of a Wearable IMU System for Gait Analysis: Protocol and Application to a New System. Appl. Sci. 8, 1167 (2018).
Sy, L. et al. Estimating Lower Limb Kinematics Using a Reduced Wearable Sensor Count. IEEE Trans. Biomed. Eng. 68, 1293–1304 (2021).
Slade, P., Habib, A., Hicks, J. L. & Delp, S. L. An Open-Source and Wearable System for Measuring 3D Human Motion in Real-Time. IEEE Trans. Biomed. Eng. 69, 678–688 (2022).
Kim, W.-S., Choi, H., Jung, J.-W., Yoon, J. S. & Jeoung, J. H. Asymmetry and Variability Should Be Included in the Assessment of Gait Function in Poststroke Hemiplegia With Independent Ambulation During Early Rehabilitation. Arch. Phys. Med. Rehabil. 102, 611–618 (2021).
Olivares, A., Ramírez, J., Górriz, J. M., Olivares, G. & Damas, M. Detection of (in)activity periods in human body motion using inertial sensors: a comparative study. Sensors 12, 5791–5814 (2012).
Carcreff, L., Payen, G., Grouvel, G., Massé, F. & Armand, S. Three-Dimensional Lower-Limb Kinematics from Accelerometers and Gyroscopes with Simple and Minimal Functional Calibration Tasks: Validation on Asymptomatic Participants. Sensors 22, 5657 (2022).
Ordinance on Human Research: Swiss Federal Council. Ordinance on Human Research with the Exception of Clinical Trials (Human Research Ordinance, HRO) 2014.
Leboeuf, F. et al. The conventional gait model, an open-source implementation that reproduces the past but prepares for the future. Gait Posture 69, 235–241 (2019).
Gutierrez, E. M., Bartonek, Å., Haglund-Åkerlind, Y. & Saraste, H. Centre of mass motion during gait in persons with myelomeningocele. Gait Posture 18, 37–46 (2003).
Söderkvist, I. & Wedin, P. A. Determining the movements of the skeleton using well-configured markers. J. Biomech. 26, 1473–1477 (1993).
Lebleu, J. et al. Lower Limb Kinematics Using Inertial Sensors during Locomotion: Accuracy and Reproducibility of Joint Angle Calculations with Different Sensor-to-Segment Calibrations. Sensors 20, 715 (2020).
Pacher, L., Chatellier, C., Vauzelle, R. & Fradet, L. Comparison of lower limb calibration methods for movement analysis with inertial measurement unit (IMU). Comput. Methods Biomech. Biomed. Engin. 23, S215–S217 (2020).
Podsiadlo, D. & Richardson, S. The timed ‘Up & Go’: a test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 39, 142–148 (1991).
30 Second Sit to Stand Test. Shirley Ryan AbilityLab https://www.sralab.org/rehabilitation-measures/30-second-sit-stand-test.
de Melo, T. A. et al. The Five Times Sit-to-Stand Test: safety and reliability with older intensive care unit patients at discharge. Rev. Bras. Ter. Intensiva 31, 27–33 (2019).
Barre, A. & Armand, S. Biomechanical ToolKit: Open-source framework to visualize and process biomechanical data. Comput. Methods Programs Biomed. 114, 80–87 (2014).
Gløersen, Ø. & Federolf, P. Predicting Missing Marker Trajectories in Human Motion Data Using Marker Intercorrelations. PLOS ONE 11, e0152616 (2016).
Hara, R., McGinley, J., Briggs, C., Baker, R. & Sangeux, M. Predicting the location of the hip joint centres, impact of age group and sex. Sci. Rep. 6, 37707 (2016).
Zeni, J. A., Richards, J. G. & Higginson, J. S. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 27, 710–714 (2008).
Acknowledgements
This study was co-financed by Innosuisse - Swiss Innovation Agency (Bern, Switzerland) and Gait Up SA - Project number: 38215.1 IP-LS - “KINEMAGICS: 3D kinematics for clinical gait analysis using wearable sensors”.
The authors would also like to thank all the participants for their participation in the study.
Author information
Authors and Affiliations
Contributions
L.C. and G.G. designed the protocol and performed data collection to establish the presented dataset. F.M. helped in the data processing. G.G. performed data processing, checked all records and wrote the final manuscript. S.A. supervised the project and provided overall project management. S.A., L.C., F.M. and G.G. revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
Gait Up SA was not involved in the acquisition and processing of data, nor in the writing of the article.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grouvel, G., Carcreff, L., Moissenet, F. et al. A dataset of asymptomatic human gait and movements obtained from markers, IMUs, insoles and force plates. Sci Data 10, 180 (2023). https://doi.org/10.1038/s41597-023-02077-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41597-023-02077-3
